The Athletics Injury Prevention Programme Can Help to Reduce the Occurrence at Short Term of Participation Restriction Injury Complaints in Athletics: A Prospective Cohort Study



Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Athletics Injury Prevention Programme and Implementation
2.4. Data Collection Regarding Participation in the AIPP, Exposure and Injury Complaints
2.5. Data Analysis
3. Results
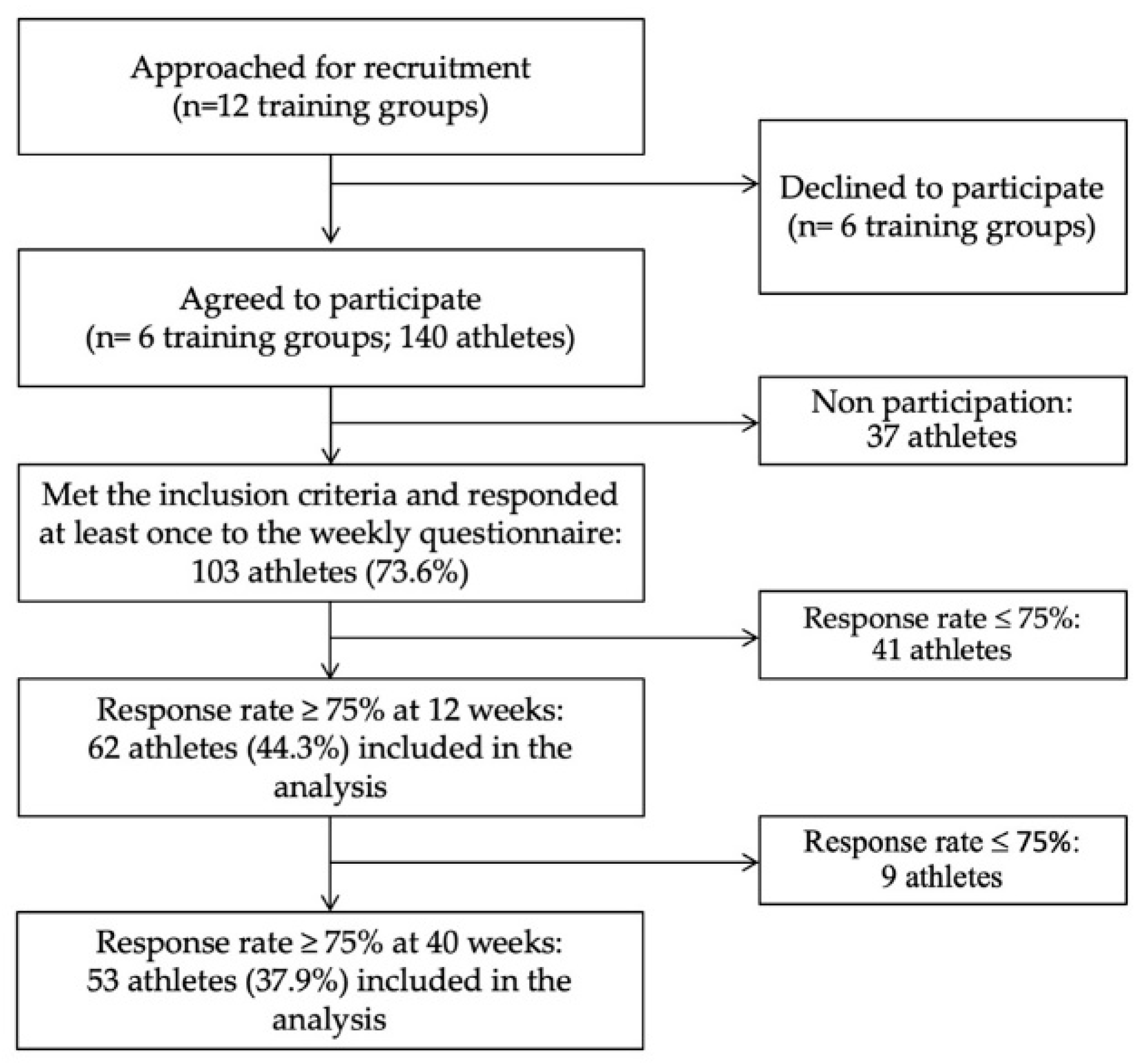
3.1. Participants
3.2. Short-Term Effect of the AIPP
3.3. Long-Term Effect of the AIPP
4. Discussion
4.1. AIPP Can Reduce Occurrence of Participation Restriction Injury Complaints
4.2. Methodological Considerations
4.3. Practical Implications for AIPP and Athlete Health
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Edouard, P.; Alonso, J.M.; Jacobsson, J.; Depiesse, F.; Branco, P.; Timpka, T. Injury Prevention in Athletics: The Race Has Started and We Are on Track! New Stud. Athl. 2015, 30, 69–78. [Google Scholar]
- D’Souza, D. Track and field athletics injuries—A one-year survey. Br. J. Sports Med. 1994, 28, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Crossley, K. Musculoskeletal injuries in track and field: Incidence, distribution and risk factors. Aust. J. Sci. Med. Sport 1996, 28, 69–75. [Google Scholar] [PubMed]
- Jacobsson, J.; Timpka, T.; Kowalski, J.; Nilsson, S.; Ekberg, J.; Dahlström, Ö.; Renström, P.A. Injury patterns in Swedish elite athletics: Annual incidence, injury types and risk factors. Br. J. Sports Med. 2013, 47, 941–952. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Navarro, L.; Branco, P.; Gremeaux, V.; Timpka, T.; Junge, A. Injury frequency and characteristics (location, type, cause and severity) differed significantly among athletics (‘track and field’) disciplines during 14 international championships (2007–2018): Implications for medical service planning. Br. J. Sports Med. 2020, 54, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Richardson, A.; Navarro, L.; Gremeaux, V.; Branco, P.; Junge, A. Relation of team size and success with injuries and illnesses during eight international outdoor athletics championships. Front. Sport. Act. Living 2019. [Google Scholar] [CrossRef]
- Raysmith, B.; Drew, M.K. Performance success or failure is influenced by weeks lost to injury and illness in elite Australian Track and Field athletes: A 5-year prospective study. J. Sci. Med. Sport 2016, 19, 778–783. [Google Scholar] [CrossRef]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C.G. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 1992, 14, 82–99. [Google Scholar] [CrossRef]
- Edouard, P.; Richardson, A.; Murray, A.; Duncan, J.; Glover, D.; Kiss-Polauf, M.; Depiesse, F.; Branco, P. Ten tips to hurdle the injuries and illnesses during major athletics championships: Practical recommendations and resources. Front. Sport. Act. Living 2019. [Google Scholar] [CrossRef]
- Lauersen, J.B.; Bertelsen, D.M.; Andersen, L.B. The effectiveness of exercise interventions to prevent sports injuries: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2014, 48, 871–877. [Google Scholar] [CrossRef]
- Junge, A.; Rösch, D.; Peterson, L.; Graf-Baumann, T.; Dvorak, J. Prevention of soccer injuries: A prospective intervention study in youth amateur players. Am. J. Sports Med. 2002, 30, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Soligard, T.; Myklebust, G.; Steffen, K.; Holme, I.; Silvers, H.; Bizzini, M.; Junge, A.; Dvorak, J.; Bahr, R.; Andersen, T.E. Comprehensive warm-up programme to prevent injuries in young female footballers: Cluster randomised controlled trial. BMJ 2008, 337, a2469. [Google Scholar] [CrossRef] [PubMed]
- Walden, M.; Atroshi, I.; Magnusson, H.; Wagner, P.; Hagglund, M. Prevention of acute knee injuries in adolescent female football players: Cluster randomised controlled trial. BMJ 2012, 344, e3042. [Google Scholar] [CrossRef] [PubMed]
- Myklebust, G.; Engebretsen, L.; Braekken, I.H.; Skjølberg, A.; Olsen, O.-E.; Bahr, R. Prevention of anterior cruciate ligament injuries in female team handball players: A prospective intervention study over three seasons. Clin. J. Sport Med. 2003, 13, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Olsen, O.E.; Myklebust, G.; Engebretsen, L.; Holme, I.; Bahr, R. Exercises to prevent lower limb injuries in youth sports: Cluster randomised controlled trial. BMJ 2005, 330, 449. [Google Scholar] [CrossRef]
- Andersson, S.H.; Bahr, R.; Clarsen, B.; Myklebust, G. Preventing overuse shoulder injuries among throwing athletes: A cluster-randomised controlled trial in 660 elite handball players. Br. J. Sports Med. 2017, 51, 1073–1080. [Google Scholar] [CrossRef]
- Carragher, P.; Rankin, A.; Edouard, P. A One-Season Prospective Study of Illnesses, Acute, and Overuse Injuries in Elite Youth and Junior Track and Field Athletes. Front. Sport. Act. Living 2019, 1, 1–12. [Google Scholar] [CrossRef]
- Arnason, A.; Andersen, T.E.; Holme, I.; Engebretsen, L.; Bahr, R. Prevention of hamstring strains in elite soccer: An intervention study. Scand. J. Med. Sci. Sport. 2008, 18, 40–48. [Google Scholar] [CrossRef]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmich, P. Preventive Effect of Eccentric Training on Acute Hamstring Injuries in Men’s Soccer: A cluster-randomised controlled trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef]
- Beyer, R.; Kongsgaard, M.; Hougs Kjaer, B.; Ohlenschlaeger, T.; Kjaer, M.; Magnusson, S.P. Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial. Am. J. Sports Med. 2015, 43, 1704–1711. [Google Scholar] [CrossRef]
- Kongsgaard, M.; Kovanen, V.; Aagaard, P.; Doessing, S.; Hansen, P.; Laursen, A.H.; Kaldau, N.C.; Kjaer, M.; Magnusson, S.P. Corticosteroid injections, eccentric decline squat training and heavy slow resistance training in patellar tendinopathy. Scand. J. Med. Sci. Sport. 2009, 19, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Kerkhoffs, G.M.; van den Bekerom, M.; Elders, L.A.; van Beek, P.A.; Hullegie, W.A.; Bloemers, G.M.; de Heus, E.M.; Loogman, M.C.; Rosenbrand, K.C.; Kuipers, T.; et al. Diagnosis, treatment and prevention of ankle sprains: An evidence-based clinical guideline. Br. J. Sport. Med. 2012, 46, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Coulombe, B.J.; Games, K.E.; Neil, E.R.; Eberman, L.E. Core stability exercise versus general exercise for chronic low back pain. J. Athl. Train. 2017, 52, 71–72. [Google Scholar] [CrossRef]
- Timpka, T.; Alonso, J.-M.; Jacobsson, J.; Junge, A.; Branco, P.; Clarsen, B.; Kowalski, J.; Mountjoy, M.; Nilsson, S.; Pluim, B.; et al. Injury and illness definitions and data collection procedures for use in epidemiological studies in Athletics (track and field): Consensus statement. Br. J. Sports Med. 2014, 48, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.-M.J.-M.; Jacobsson, J.; Timpka, T.; Ronsen, O.; Kajenienne, A.; Dahlström, Ö.; Spreco, A.; Edouard, P. Preparticipation injury complaint is a risk factor for injury: A prospective study of the Moscow 2013 IAAF Championships. Br. J. Sports Med. 2015, 49, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Rønsen, O.; Myklebust, G.; Flørenes, T.W.; Bahr, R. The Oslo Sports Trauma Research Center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. Br. J. Sports Med. 2014, 48, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Jacobsson, J.; Timpka, T.; Alonso, J.M.; Kowalski, J.; Nilsson, S.; Karlsson, D.; Depiesse, F.; Branco, P. Extending in-competition Athletics injury and illness surveillance with pre-participation risk factor screening: A pilot study. Phys. Ther. Sport 2015, 16, 98–106. [Google Scholar] [CrossRef]
- Nielsen, R.O.; Bertelsen, M.L.; Ramskov, D.; Møller, M.; Hulme, A.; Theisen, D.; Finch, C.F.; Fortington, L.V.; Mansournia, M.A.; Parner, E.T. Time-to-event analysis for sports injury research part 2: Time-varying outcomes. Br. J. Sports Med. 2019, 53, 70–78. [Google Scholar] [CrossRef]
- Edouard, P.; Branco, P.; Alonso, J.-M. Challenges in Athletics injury and illness prevention: Implementing prospective studies by standardised surveillance. Br. J. Sports Med. 2014, 48, 481–482. [Google Scholar] [CrossRef]
- Nielsen, R.O.; Bertelsen, M.L.; Ramskov, D.; Damsted, C.; Verhagen, E.; Bredeweg, S.W.; Theisen, D.; Malisoux, L. Randomised controlled trials (RCTs) in sports injury research: Authors-Please report the compliance with the intervention. Br. J. Sports Med. 2020, 54, 51–57. [Google Scholar] [CrossRef]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition—Narrative review and new concept. Br. J. Sports Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Mendiguchia, J.; Martinez-Ruiz, E.; Edouard, P.; Morin, J.-B.; Martinez-Martinez, F.; Idoate, F.; Mendez-Villanueva, A. A Multifactorial, Criteria-based Progressive Algorithm for Hamstring Injury Treatment. Med. Sci. Sports Exerc. 2017, 49, 1482–1492. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Berton, A.; Marinozzi, A.; Maffulli, N.; Denaro, V. The FIFA 11+ Program Is Effective in Preventing Injuries in Elite Male Basketball Players: A Cluster Randomized Controlled Trial. Am. J. Sports Med. 2012, 40, 996–1005. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: A cluster randomised trial. Br. J. Sports Med. 2013, 47, 794–802. [Google Scholar] [CrossRef]
- Fuller, C.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hagglund, M.; McCrory, P.; Meeuwisse, W. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand. J. Med. Sci. Sport. 2006, 16, 83–92. [Google Scholar] [CrossRef]
- Junge, A.; Engebretsen, L.; Alonso, J.M.; Renström, P.; Mountjoy, M.; Aubry, M.; Dvorak, J. Injury surveillance in multi-sport events: The International Olympic Committee approach. Br. J. Sports Med. 2008, 42, 413–421. [Google Scholar] [CrossRef]
- Mountjoy, M.; Junge, A.; Alonso, J.M.; Clarsen, B.; Pluim, B.M.; Shrier, I.; van den Hoogenband, C.; Marks, S.; Gerrard, D.; Heyns, P.; et al. Consensus statement on the methodology of injury and illness surveillance in FINA (aquatic sports). Br. J. Sports Med. 2016, 50, 590–596. [Google Scholar] [CrossRef]
- Clarsen, B.; Myklebust, G.; Bahr, R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) overuse injury questionnaire. Br. J. Sports Med. 2013, 47, 495–502. [Google Scholar] [CrossRef]


{kind=link}
| Exercises | Repetitions | Bonus (If It is too Easy, Athlete can Increase Difficulty) |
|---|---|---|
| Core stability—the plank (4 sides: prone position, lateral, supine position, lateral): | ||
| Level 1: both legs | 15 s per side for 3 min | 4 × 30 s for 6 min, then for 12 min |
| Level 2: alternate legs | ||
| Level 3: unstable support | ||
| Single leg balance: | ||
| Level 1: static | 3 × 15 s (each side) | 3 × 30 s each side |
| Level 2: unstable support | ||
| Level 3: throwing ball with partner, then on unstable support | ||
| Pelvis strengthening: | ||
| Lunges | 3 × 10 rep. | 6 × 10 rep., then 6 × 10 rep. with medicine ball |
| Hip abductor strengthening-Level 1: leg empty | 3 × 10 rep. (each side) | 6 × 10 rep. (each side), then unstable support |
| Hip abductor strengthening-Level 2: with elastic | 3 × 10 rep. (each side) | 6 × 10 rep. (each side), then unstable support |
| Hamstring exercises: | ||
| Hamstring stretching (different positions) | 3 × 15 s | |
| Hamstring strengthening: | ||
| Level 1: isometric contraction on two legs | 6 × 6 s | 10 × 10 s |
| Level 1: heel to buttock with elastic | 3 × 6 s (each side) | 5 × 10 s (each side) |
| Level 2: isometric contraction on one leg | 6 × 6 s (each side) | 10 × 10 s (each side) |
| Level 2: heel to buttock with elastic | 3 × 6 s (each side) | 5 × 10 s (each side) |
| Level 3: Nordic hamstring with help of upper arms | 1 × 5 rep., then 3 × 5 rep., then 6 × 6 rep. | |
| Level 4: Nordic hamstring | 1 × 5 rep., then 3 × 5 rep., then 6 × 6 rep. | |
| Level 5: Pliometric | 1 × 5 rep., then 3 × 5 rep., then 6 × 6 rep. | |
| Lower leg exercises: | ||
| Lower leg stretching | 3 × 15 s (each side) | |
| Lower leg strengthening: | ||
| Level 1: down to the ground | 3 × 8 rep. (each side) | 3 × 10 rep., then 5 × 10 rep. each side and then increase load |
| Level 2: down to the void | 3 × 8 rep. (each side) | 3 × 10 rep., then 5 × 10 rep. each side, and then increase loads |
| At 12 Weeks (n = 62) | At 40 Weeks (n = 53) | Comparison between 12 and 40 Weeks Groups | |||
|---|---|---|---|---|---|
| Anthropometric data (mean (SD)) | |||||
| Sex (M/F) (n) | 34/28 | 31/22 | Chi2 = 0.16; p = 0.69 | ||
| Age (years) | 21.4 | (5.3) | 23.6 | (7.1) | p = 0.97 |
| Height (cm) | 175.4 | (9.3) | 175.5 | (7.4) | p = 0.60 |
| Body mass (kg) | 64.3 | (10.8) | 64.7 | (10.0) | p = 0.73 |
| Body mass index (kg/m2) | 20.8 | (2.0) | 20.9 | (2.0) | p = 0.89 |
| History of injury complaints (n (%)) | |||||
| In the preceding season | 47 | (76.8) | 41 | (77.4) | Chi2 = 0.04; p = 0.84 |
| Disciplines (n (%)) | Chi2 = 1.13; p = 0.98 | ||||
| Sprints | 17 | (27.4) | 14 | (26.4) | |
| Hurdles | 6 | (9.7) | 3 | (5.7) | |
| Middle distances | 7 | (11.3) | 5 | (9.4) | |
| Long distances | 3 | (4.8) | 3 | (5.7) | |
| Jumps | 6 | (9.7) | 6 | (11.3) | |
| Throws | 3 | (4.8) | 2 | (3.8) | |
| Combined events | 20 | (32.3) | 20 | (37.7) | |
| Time Scale: Cumulative Weeks | Time Scale: Cumulative Training Time | |||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | Time-Independancies of Variables | HR | 95% CI | p Value | Time-Independancies of Variables | |
| At 12 weeks | ||||||||
| Main factor: AIPP | 0.36 | (0.15 to 0.86) | 0.02 | 0.95 | 0.29 | (0.12 to 0.73) | 0.009 | 0.80 |
| Adjustment variables: | ||||||||
| Sex (M) | 1.35 | (0.17 to 10.7) | 0.78 | 0.94 | 1.34 | (0.16 to 11.5) | 0.79 | 0.62 |
| Age | 1.01 | (0.99 to 1.21) | 0.09 | 0.97 | 1.10 | (1.00 to 1.21) | 0.06 | 0.09 |
| Height | 1.91 | (1.03 to 3.53) | 0.04 | 0.98 | 2.08 | (1.09 to 3.99) | 0.03 | 0.76 |
| Body mass | 0.43 | (0.20 to 0.98) | 0.04 | 0.96 | 0.40 | (0.17 to 0.92) | 0.03 | 0.83 |
| Body mass index | 8.11 | (0.67 to 98.6) | 0.10 | 0.91 | 11.2 | (0.78 to 159.0) | 0.08 | 0.60 |
| Disciplines (reference combined events): | ||||||||
| Sprints | 0.51 | (0.13 to 2.01) | 0.33 | 0.053 | 0.64 | (0.16 to 2.56) | 0.53 | 0.33 |
| Hurdles | 0.01 | (0.01 to 0.95) | 0.05 | 0.29 | 0.01 | (0.01 to 0.96) | 0.05 | 0.82 |
| Middle distances | 0.53 | (0.09 to 3.14) | 0.48 | 0.80 | 0.54 | (0.08 to 3.41) | 0.51 | 0.24 |
| Long distances | 0.39 | (0.02 to 9.68) | 0.57 | 0.44 | 0.62 | (0.02 to 15.2) | 0.77 | 0.63 |
| Jumps | 1.29 | (0.23 to 7.32) | 0.78 | 0.26 | 1.66 | (0.31 to 8.90) | 0.56 | 0.33 |
| Throws | 0.00 | (0.00 to inf) | 1.00 | 1.00 | 0.00 | (0.00 to inf) | 1.00 | 1.00 |
| History of injury complaints in the preceding season | 1.40 | (0.33 to 6.03) | 0.65 | 0.86 | 1.53 | (0.35 to 6.67) | 0.57 | 0.30 |
| Response rate | 1.05 | (0.98 to 1.13) | 0.17 | 0.58 | 1.03 | (0.95 to 1.10) | 0.57 | 0.50 |
| Training per week | 1.14 | (0.93 to 1.39) | 0.20 | 0.25 | ||||
| Competition per week | 37.7 | (4.79 to 295.9) | 0.0006 | 0.15 | 48.3 | (6.76 to 344.3) | 0.0001 | 0.91 |
| Cox model adjustment | Concordance = 0.824 (se = 0.038); Likelihood ratio test = 39.55 on 16 df, p < 0.0001; Wald test = 29.92 on 16 df, p = 0.002; Score (logrank) test = 38.69 on 16 df, p = 0.001 | Concordance = 0.838 (se = 0.034); Likelihood ratio test = 43.63 on 15 df, p = 0.0001; Wald test = 32.92 on 15 df, p = 0.005; Score (logrank) test = 47.61 on 15 df, p < 0.0001 | ||||||
| Time-independancies of variables | chi-2 test = 14.9; p = 0.53 | chi-2 test = 15.7; p = 0.40 | ||||||
| At 40 weeks | ||||||||
| Main factor: AIPP | 0.79 | (0.47 to 1.31) | 0.36 | 0.88 | 0.87 | (0.52 to 1.44) | 0.58 | 0.99 |
| Adjustment variables: | ||||||||
| Sex (M) | 0.98 | (0.22 to 4.35) | 0.98 | 0.93 | 1.00 | (0.24 to 4.21) | 1.00 | 0.86 |
| Age | 0.97 | (0.89 to 1.06) | 0.50 | 0.43 | 1.04 | (0.95 to 1.15) | 0.38 | 0.67 |
| Height | 1.63 | (0.90 to 2.94) | 0.11 | 0.65 | 1.19 | (0.65 to 2.17) | 0.57 | 0.46 |
| Body mass | 0.50 | (0.23 to 1.09) | 0.08 | 0.63 | 0.76 | (0.35 to 1.65) | 0.49 | 0.44 |
| Body mass index | 7.27 | (0.68 to 77.7) | 0.10 | 0.64 | 2.13 | (0.19 to 23.7) | 0.54 | 0.44 |
| Disciplines: | ||||||||
| Combined events | 1.70 | (0.10 to 32.4) | 0.72 | 0.49 | 0.32 | (0.02 to 4.21) | 0.41 | 0.71 |
| Sprints | 2.31 | (0.12 to 44.2) | 0.58 | 0.30 | 0.35 | (0.03 to 4.94) | 0.44 | 0.53 |
| Hurdles | 8.68 | (0.31 to 247.1) | 0.21 | 0.57 | 0.89 | (0.05 to 16.9) | 0.94 | 0.87 |
| Middle distances | 1.95 | (0.10 to 36.2) | 0.66 | 0.51 | 0.57 | (0.04 to 8.83) | 0.69 | 0.90 |
| Long distances | 4.75 | (0.16 to 144.8) | 0.37 | 0.42 | 0.94 | (0.03 to 29.6) | 0.97 | 0.23 |
| Jumps | 10.3 | (0.50 to 215.3 | 0.13 | 0.90 | 2.90 | (0.18 to 47.4) | 0.46 | 0.86 |
| Throws | 0.00 | (0.00 to inf) | 1.00 | 1.00 | 0.00 | (0.00 to inf) | 1.00 | 1.00 |
| History of injury complaints in the preceding season | 0.81 | (0.26 to 2.48) | 0.71 | 0.83 | 1.36 | (0.45 to 4.13) | 0.59 | 0.92 |
| Response rate | 1.08 | (1.01 to 1.15) | 0.03 | 0.32 | 1.03 | (0.98 to 1.09) | 0.26 | 0.66 |
| Training per week | 9.10 | (0.78 to 1.06) | 0.23 | 0.03 | ||||
| Competition per week | 0.54 | (0.43 to 0.69) | <0.0001 | 0.38 | 0.61 | (0.48 to 0.76) | <0.0001 | 0.63 |
| Cox model adjustment | Concordance = 0.876 (se = 0.026); Likelihood ratio test = 87.75 on 17 df, p < 0.0001; Wald test = 41.89 on 17 df, p < 0.0001; Score (logrank) test = 73.95 on 17 df, p < 0.0001 | Concordance = 0.84 (se = 0.033); Likelihood ratio test = 78.91 on 16 df, p < 0.0001; Wald test = 40.81 on 16 df, p < 0.0001; Score (logrank) test = 68.46 on 16 df, p < 0.0001 | ||||||
| Time-independancies of variables | chi-2 test = 10.6; p = 0.88 | chi-2 test = 85.4; p = 0.93 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edouard, P.; Cugy, E.; Dolin, R.; Morel, N.; Serra, J.-M.; Depiesse, F.; Branco, P.; Steffen, K. The Athletics Injury Prevention Programme Can Help to Reduce the Occurrence at Short Term of Participation Restriction Injury Complaints in Athletics: A Prospective Cohort Study. Sports 2020, 8, 84. https://doi.org/10.3390/sports8060084
Edouard P, Cugy E, Dolin R, Morel N, Serra J-M, Depiesse F, Branco P, Steffen K. The Athletics Injury Prevention Programme Can Help to Reduce the Occurrence at Short Term of Participation Restriction Injury Complaints in Athletics: A Prospective Cohort Study. Sports. 2020; 8(6):84. https://doi.org/10.3390/sports8060084
Chicago/Turabian StyleEdouard, Pascal, Emmanuelle Cugy, Romain Dolin, Nicolas Morel, Jean-Michel Serra, Frédéric Depiesse, Pedro Branco, and Kathrin Steffen. 2020. "The Athletics Injury Prevention Programme Can Help to Reduce the Occurrence at Short Term of Participation Restriction Injury Complaints in Athletics: A Prospective Cohort Study" Sports 8, no. 6: 84. https://doi.org/10.3390/sports8060084
APA StyleEdouard, P., Cugy, E., Dolin, R., Morel, N., Serra, J.-M., Depiesse, F., Branco, P., & Steffen, K. (2020). The Athletics Injury Prevention Programme Can Help to Reduce the Occurrence at Short Term of Participation Restriction Injury Complaints in Athletics: A Prospective Cohort Study. Sports, 8(6), 84. https://doi.org/10.3390/sports8060084