Acute Caffeine Supplementation Does Not Improve Performance in Trained CrossFit® Athletes



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Measures and Procedures
2.3. Analysis
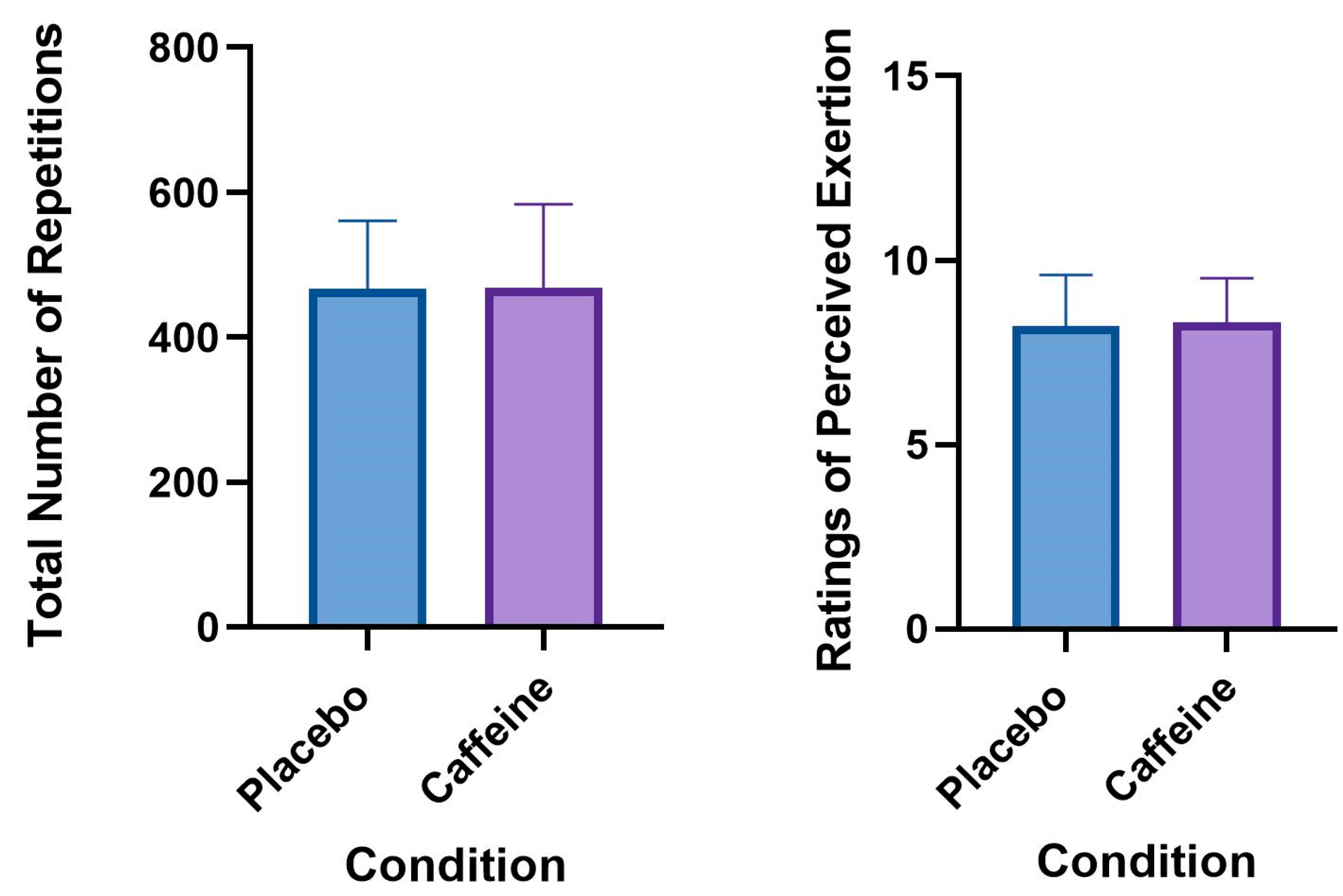
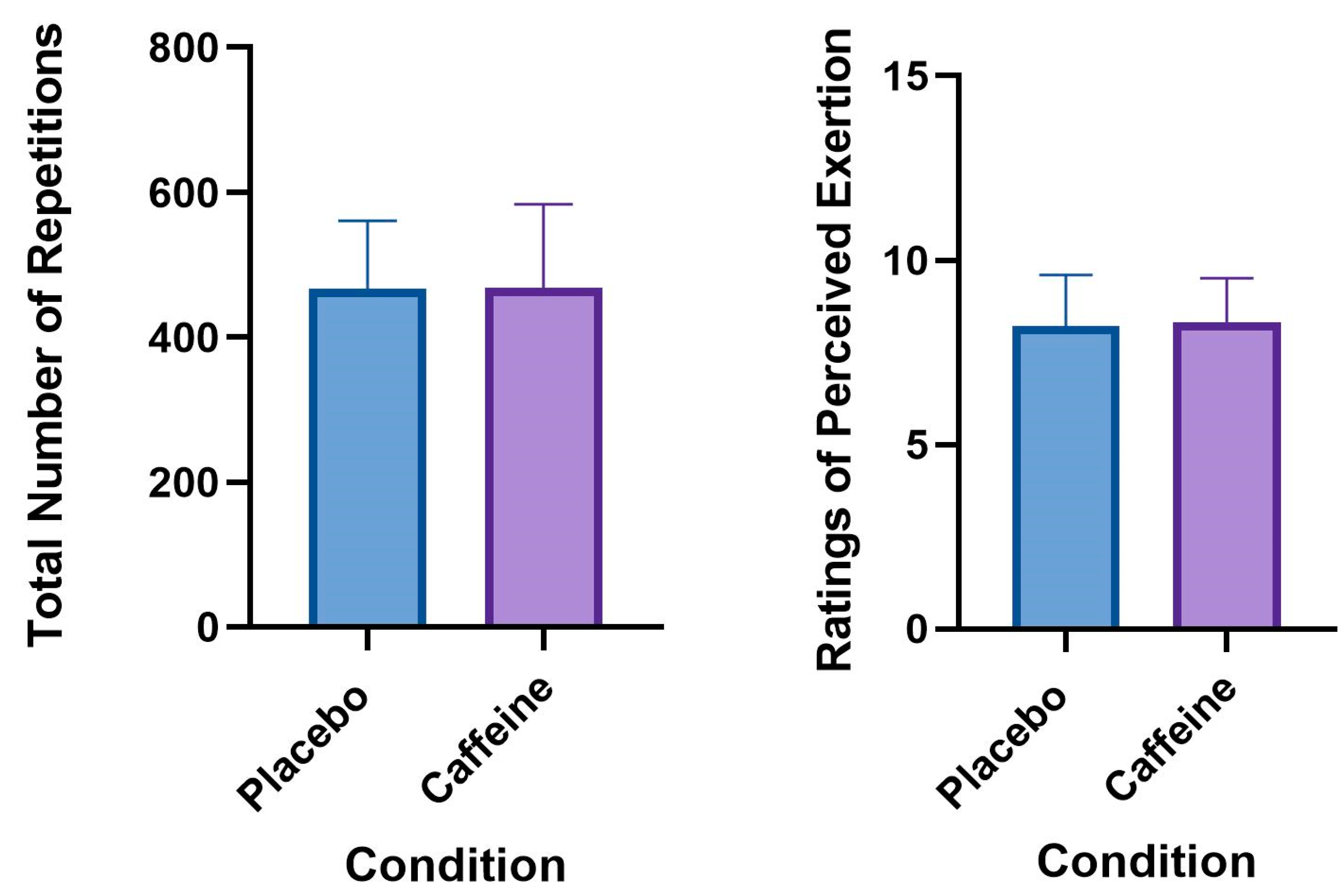
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Del Coso, J.; Muñoz, G.; Muñoz-Guerra, J. Prevalence of caffeine use in elite athletes following its removal from the World Anti-Doping Agency list of banned substances. Appl. Physiol. Nutr. Metab. 2011, 36, 555–561. [Google Scholar] [CrossRef] [Green Version]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 104–125. [Google Scholar] [CrossRef] [Green Version]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E.; et al. ISSN exercise & sports nutrition review update: Research & recommendations. J. Int. Soc. Sports Nutr. 2018, 15, 1–57. [Google Scholar]
- Evans, M.; Tierney, P.; Gray, N.; Hawe, G.; Macken, M.; Egan, B. Acute ingestion of caffeinated chewing gum improves repeated sprint performance of team sport athletes with low habitual caffeine consumption. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 221–227. [Google Scholar] [CrossRef]
- Grgic, J.; Mikulic, P.; Schoenfeld, B.J.; Bishop, D.J.; Pedisic, Z. The influence of caffeine supplementation on resistance exercise: A review. Sport Med. 2019, 49, 1–14. [Google Scholar] [CrossRef]
- Warren, G.; Park, N.; Maresca, R.; Mckibans, K.; Millard-Stafford, M. Effect of caffeine ingestion on muscular strength and endurance: A Meta-Analysis. Med. Sci. Sport Exerc. 2010, 42, 1375–1387. [Google Scholar] [CrossRef]
- Graham, T.E. Caffeine and exercise metabolism, endurance and performance. Sport Med. 2001, 31, 785–807. [Google Scholar] [CrossRef]
- Todd, A.; Daniel, W. Efficacy of caffeine ingestion for short-term high-intensity performance: A systematic review. J. Strength Cond. Res. 2010, 24, 257–265. [Google Scholar]
- Bishop, D.J.; Girard, O. Determinants of team-sport performance: Implications for altitude training by team-sport athletes. Br. J. Sports Med. 2013, 47 (Suppl. 1), i17–i21. [Google Scholar] [CrossRef] [Green Version]
- Mielgo-Ayuso, J.; Calleja-Gonzalez, J.; Del Coso, J.; Urdampilleta, A.; León-Guereño, P.; Fernández-Lázaro, D. Caffeine supplementation and physical performance, muscle damage and perception of fatigue in soccer players: A systematic review. Nutrients 2019, 11, 440. [Google Scholar] [CrossRef] [Green Version]
- Salinero, J.J.; Lara, B.; Del Coso, J. Effects of acute ingestion of caffeine on team sports performance: A systematic review and meta-analysis. Res Sport Med. 2019, 27, 238–256. [Google Scholar] [CrossRef]
- McLellan, T.M.; Caldwell, J.A.; Lieberman, H.R. A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 2016, 71, 294–312. [Google Scholar] [CrossRef] [Green Version]
- Umemura, T.; Ueda, K.; Nishioka, K.; Hidaka, T.; Takemoto, H.; Nakamura, S.; Jitsuiki, D.; Soga, J.; Goto, C.; Chayama, K.; et al. Effects of acute administration of caffeine on vascular function. Am. J. Cardiol. 2006, 98, 1538–1541. [Google Scholar] [CrossRef]
- Ruíz-Moreno, C.; Lara, B.; Brito de Souza, D.; Gutiérrez-Hellín, J.; Romero-Moraleda, B.; Cuéllar-Rayo, Á.; Del Coso, J. Acute caffeine intake increases muscle oxygen saturation during a maximal incremental exercise test. Br. J. Clin. Pharmacol. 2019, 1–7. [Google Scholar] [CrossRef]
- Broxterman, R.M.; Ade, C.J.; Craig, J.C.; Wilcox, S.L.; Schlup, S.J.; Barstow, T.J. Influence of blood flow occlusion on muscle oxygenation characteristics and the parameters of the power-duration relationship. J. Appl. Physiol. 2015, 118, 880–889. [Google Scholar] [CrossRef] [Green Version]
- Vanhatalo, A.; Fulford, J.; DiMenna, F.J.; Jones, A.M. Influence of hyperoxia on muscle metabolic responses and the power-duration relationship during severe-intensity exercise in humans: A 31 P magnetic resonance spectroscopy study. Exp. Physiol. 2010, 95, 528–540. [Google Scholar] [CrossRef] [Green Version]
- Polito, M.D.; Souza, D.B.; Casonatto, J.; Farinatti, P. Acute effect of caffeine consumption on isotonic muscular strength and endurance: A systematic review and meta-analysis. Sci. Sports 2016, 31, 119–128. [Google Scholar] [CrossRef]
- Astorino, T.A.; Rohmann, R.L.; Firth, K. Effect of caffeine ingestion on one-repetition maximum muscular strength. Eur. J. Appl. Physiol. 2008, 102, 127–132. [Google Scholar] [CrossRef]
- Astorino, T.A.; Martin, B.J.; Schachtsiek, L.; Wong, K.; Ng, K. Minimal effect of acute caffeine ingestion on intense resistance training performance. J. Strength Cond. Res. 2011, 25, 1752–1758. [Google Scholar] [CrossRef] [Green Version]
- Duncan, M.; Oxford, S. The effect of caffeine ingestion on mood state and bench press performance to failure. J. Strength Cond. Res. 2011, 25, 178–185. [Google Scholar] [CrossRef]
- Hudson, G.M.; Green, J.M.; Bishop, P.A.; Richardson, M.T. Effects of caffeine and aspirin on light resistance training performance, perceived exertion, and pain perception. J. Strength Cond. Res. 2008, 22, 1950–1957. [Google Scholar] [CrossRef]
- Feito, Y.; Heinrich, K.; Butcher, S.; Poston, W. High-intensity functional training (HIFT): Definition and research implications for improved fitness. Sports 2018, 6, 76. [Google Scholar] [CrossRef] [Green Version]
- Box, A.G.; Feito, Y.; Petruzzello, S.J.; Mangine, G.T. Mood state changes accompanying the Crossfit Open TM competition in healthy adults. Sports 2018, 6, 67. [Google Scholar] [CrossRef] [Green Version]
- Jagim, A.R.; Rader, O.; Jones, M.T.; Oliver, J.M. The physical demands of multi-modal training competitions and their relationship to measures of performance. J. Strength Cond. Res. 2015, 31, 1212–1220. [Google Scholar] [CrossRef]
- Butcher, S.J.; Judd, T.B.; Benko, C.R.; Horvey, K.J.; Pshyk, A.D. Relative intensity of two types of CrossFit exercise: Acute circuit and high-intensity interval exercise. J. Fit. Res. 2015, 4, 3–15. [Google Scholar]
- Fernández, J.F.; Solana, R.S.; Moya, D.; Marin, J.M.S.; Ramón, M.M. Acute physiological responses during crossfit® workouts. Eur. J. Hum. Mov. 2015, 35, 114–124. [Google Scholar]
- Butcher, S.J.; Neyedly, T.J.; Horvey, K.J.; Benko, C.R. Do physiological measures predict selected CrossFit® benchmark performance? J. Sports Med. 2015, 6, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Crawford, D.A.; Drake, N.B.; Carper, M.J.; DeBlauw, J.; Heinrich, K.M. Are changes in physical work capacity induced by high-intensity functional training related to changes in associated physiologic measures? Sports 2018, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Rountree, J.A.; Krings, B.M.; Peterson, T.J.; Thigpen, A.G.; McAllister, M.J.; Holmes, M.E.; Smith, J.W. Efficacy of carbohydrate ingestion on crossfit exercise performance. Sports 2017, 5, 61. [Google Scholar] [CrossRef] [Green Version]
- Fogaça, L.J.; Santos, S.L.; Soares, R.C.; Gentil, P.; Naves, J.P.; Dos, W.S.; Pimentel, G.D.; Bottaro, M.; Mota, J.F. Effect of caffeine supplementation on exercise pndomized, erformance, power, markers of muscle damage, and perceived exertion in trained CrossFit men: A randomized double-blind, placebo-controlled crossover trial. J. Sports Med. Phys. Fit. 2020, 60, 181–188. [Google Scholar]
- Southward, K.; Rutherfurd-Markwick, K.J.; Ali, A. The effect of acute caffeine ingestion on endurance performance: A systematic review and meta–analysis. Sport Med. 2018, 48, 1913–1928. [Google Scholar] [CrossRef]
- Graham-Paulson, T.; Perret, C.; Goosey-Tolfrey, V. Improvements in cycling but not handcycling 10 km time trial performance in habitual caffeine users. Nutrients 2016, 8, 393. [Google Scholar] [CrossRef] [Green Version]
- Pickering, C.; Kiely, J. What should we do about habitual caffeine use in athletes? Sport Med. 2018, 49, 833–842. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, P.J.; Motl, R.W.; Broglio, S.P.; Ely, M.R. Dose-dependent effect of caffeine on reducing leg muscle pain during cycling exercise is unrelated to systolic blood pressure. Pain 2004, 109, 291–298. [Google Scholar] [CrossRef]
- Burke, L.M. Caffeine and sports performance. Appl. Physiol. Nutr. Metab. 2008, 33, 1319–1334. [Google Scholar] [CrossRef]
- Kamimori, G.H.; Karyekar, C.S.; Otterstetter, R.; Cox, D.S.; Balkin, T.J.; Belenky, G.L.; Eddington, N.D. The rate of absorption and relative bioavailability of caffeine administered in chewing gum versus capsules to normal healthy volunteers. Int. J. Pharm. 2002, 234, 159–167. [Google Scholar] [CrossRef]
- Kliszczewicz, B.; Snarr, R.L.; Esco, M. Metabolic and cardiovascular response to the Crossfit workout “cindy”: A pilot study. J. Sport Hum. Perform. 2014, 2, 1–9. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sport Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Mora-Rodríguez, R.; Pallarés, J.G.; López-Gullón, J.M.; López-Samanes, Á.; Fernández-Elías, V.E.; Ortega, J.F. Improvements on neuromuscular performance with caffeine ingestion depend on the time-of-day. J. Sci. Med. Sport 2015, 18, 338–342. [Google Scholar] [CrossRef]
- Mora-Rodríguez, R.; Pallarés, J.G.; López-Samanes, Á.; Ortega, J.F.; Fernández-Elías, V.E. Caffeine ingestion reverses the circadian rhythm effects on neuromuscular performance in highly resistance-trained men. PLoS ONE 2012, 7, e33807. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciencess; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- San Juan, A.F.; López-Samanes, Á.; Jodra, P.; Valenzuela, P.L.; Rueda, J.; Veiga-Herreros, P.; Pérez-López, A.; Domínguez, R. caffeine supplementation improves anaerobic performance and neuromuscular efficiency and fatigue in Olympic-level boxers. Nutrients 2019, 11, 2120. [Google Scholar] [CrossRef] [Green Version]
- Schneiker, K.T.; Bishop, D.; Dawson, B.; Hackett, L.P. Effects of caffeine on prolonged intermittent- sprint ability in team-sport athletes. Med. Sci. Sport Exerc. 2006, 38, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.W.; Housh, T.J.; Schmidt, R.J.; Johnson, G.O.; Housh, D.J.; Coburn, J.W.; Malek, M.H. The acute effects of a caffeine-containing supplement on strength, muscular endurance, and anaerobic capabilities. J. Strength Cond. Res. 2006, 20, 506–520. [Google Scholar]
- Woolf, K.; Bidwell, W.K.; Carlson, A.G. The effect of caffeine as an ergogenic aid in anaerobic exercise. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 412–429. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.C.; Hawley, J.A.; Desbrow, B.; Jones, A.M.; Blackwell, J.R.; Ross, M.L.; Zemski, A.J.; Burke, L.M. Single and combined effects of beetroot juice and caffeine supplementation on cycling time trial performance. Appl. Physiol. Nutr. Metab. 2013, 39, 1050–1057. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, V.L.; Messias, F.R.; Zanchi, N.E.; Gerlinger-Romero, F.; Duncan, M.J.; Guimarães-Ferreira, L. Effects of acute caffeine ingestion on resistance training performance and perceptual responses during repeated sets to failure Effects of acute caffeine ingestion on resistance training performance and perceptual responses during repeated sets. J. Sports Med. Phys. Fit. 2015, 55, 383–389. [Google Scholar]
- Glaister, M; Multiple-sprint work: methodological physiological, and experimental issues. Int. J. Sports Physiol. 2008, 3, 107–112. [CrossRef]
- Guest, N.; Corey, P.; Vescovi, J.; El-Sohemy, A. Caffeine, CYP1A2 genotype, and endurance performance in athletes. Med. Sci. Sports Exerc. 2018, 50, 1570–1578. [Google Scholar] [CrossRef]
- Puente, C.; Abian-Vicen, J.; Del Coso, J.; Lara, B.; Salinero, J.J. The CYP1A2-163C>A polymorphism does not alter the effects of caffeine on basketball performance. PLoS ONE 2018, 13, e0195943. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.; O’Donnell, J.; Foskett, A.; Rutherfurd-Markwick, K. The influence of caffeine ingestion on strength and power performance in female team-sport players. J. Int. Soc. Sports Nutr. 2016, 13, 46. [Google Scholar] [CrossRef] [Green Version]
- Irwin, B.C.; Scorniaenchi, J.; Kerr, N.L.; Eisenmann, J.C.; Feltz, D.L. Aerobic exercise is promoted when individual performance affects the group: A test of the kohler motivation gain effect. Ann. Behav. Med. 2012, 44, 151–159. [Google Scholar] [CrossRef]
- Brupbacher, G.; Harder, J.; Faude, O.; Zahner, L.; Donath, L. Music in CrossFit®—Influence on performance, physiological, and psychological parameters. Sports 2014, 2, 14–23. [Google Scholar] [CrossRef]
- Morton, R.H. Deception by manipulating the clock calibration influences cycle ergometer endurance time in males. J. Sci. Med. Sport 2009, 12, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.A.; Drake, N.B.; Carper, M.J.; DeBlauw, J.; Heinrich, K.M. Validity, reliability, and application of the session-RPE method for quantifying training loads during high intensity functional training. Sports 2018, 6, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, B.; de Oliveira, L.F.; da Silva, R.P.; de Salles Painelli, V.; Gonçalves, L.S.; Yamaguchi, G.; Mutti, T.; Maciel, E.; Roschel, H.; Artioli, G.G.; et al. Placebo in sports nutrition: A proof-of-principle study involving caffeine supplementation. Scand. J. Med. Sci. Sport 2017, 27, 1240–1247. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Subject ID | Session 1 Treatment | Session 1 Total Repetitions | Session 2 Total Repetitions | Percent Change between Sessions | Percent Change between Conditions |
|---|---|---|---|---|---|
| 1 | Placebo | 214 | 240 | 12.1 | 12.1 |
| 2 | Caffeine | 300 | 339 | 13.0 | −11.5 |
| 3 | Caffeine | 372 | 373 | 0.3 | −0.3 |
| 4 | Placebo | 581 | 611 | 5.2 | 5.2 |
| 5 | Placebo | 458 | 485 | 5.9 | 5.9 |
| 6 | Placebo | 431 | 456 | 5.8 | 5.8 |
| 7 | Placebo | 510 | 611 | 19.8 | 19.8 |
| 8 | Caffeine | 467 | 512 | 9.6 | −8.8 |
| 9 | Caffeine | 461 | 486 | 5.4 | −5.1 |
| 10 | Caffeine | 374 | 473 | 2.0 | −20.9 |
| 11 | Placebo | 460 | 458 | −0.4 | −0.4 |
| 12 | Placebo | 423 | 421 | −0.5 | −0.5 |
| 13 | Caffeine | 533 | 474 | −11.1 | 12.4 |
| 14 | Placebo | 519 | 551 | 6.2 | 6.2 |
| 15 | Caffeine | 585 | 607 | 3.8 | −3.6 |
| 16 | Placebo | 534 | 541 | 1.3 | 1.3 |
| 17 | Caffeine | 379 | 410 | 3.8 | −7.6 |
| 18 | Placebo | 630 | 711 | 8.2 | 12.9 |
| 19 | Caffeine | 366 | 420 | 14.8 | −12.9 |
| 20 | Caffeine | 450 | 480 | 6.7 | −6.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stein, J.A.; Ramirez, M.; Heinrich, K.M. Acute Caffeine Supplementation Does Not Improve Performance in Trained CrossFit® Athletes. Sports 2020, 8, 54. https://doi.org/10.3390/sports8040054
Stein JA, Ramirez M, Heinrich KM. Acute Caffeine Supplementation Does Not Improve Performance in Trained CrossFit® Athletes. Sports. 2020; 8(4):54. https://doi.org/10.3390/sports8040054
Chicago/Turabian StyleStein, Jesse A., Melitza Ramirez, and Katie M. Heinrich. 2020. "Acute Caffeine Supplementation Does Not Improve Performance in Trained CrossFit® Athletes" Sports 8, no. 4: 54. https://doi.org/10.3390/sports8040054
APA StyleStein, J. A., Ramirez, M., & Heinrich, K. M. (2020). Acute Caffeine Supplementation Does Not Improve Performance in Trained CrossFit® Athletes. Sports, 8(4), 54. https://doi.org/10.3390/sports8040054