A Comparative Study of Fitness Levels among Norwegian Youth in 1988 and 2001

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Equipment
2.3. Protocol
Indirect and Direct Tests of Maximal Oxygen Uptake
2.4. Sargent Jump-and-Reach Test for Jump Height
2.5. Broomstick Test for Shoulder Flexibility
2.6. Straight-Leg-Raise Test for Hamstring Flexibility
2.7. Ethical Considerations
2.8. Statistics
3. Results
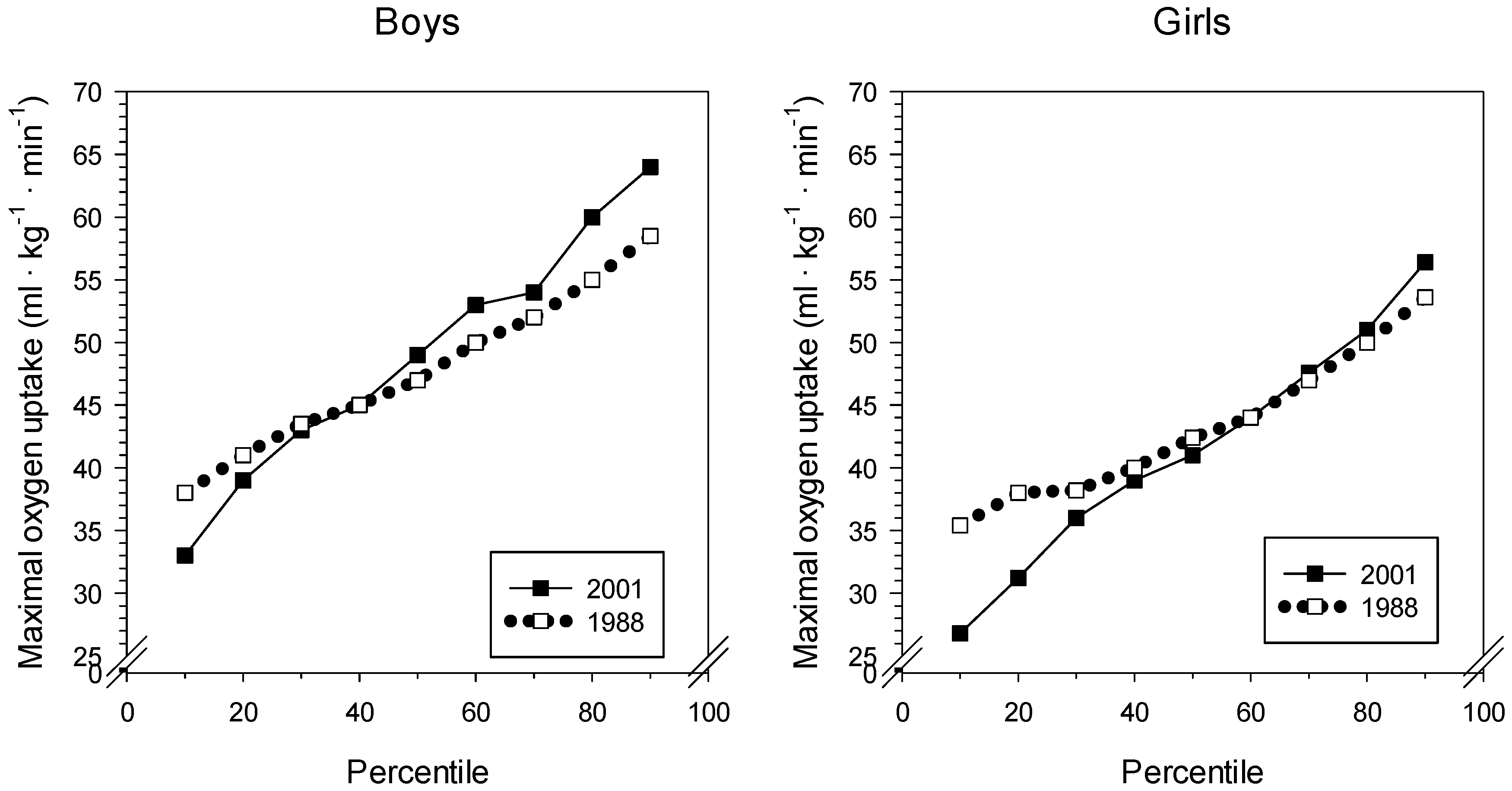
3.1. Maximal Oxygen Uptake
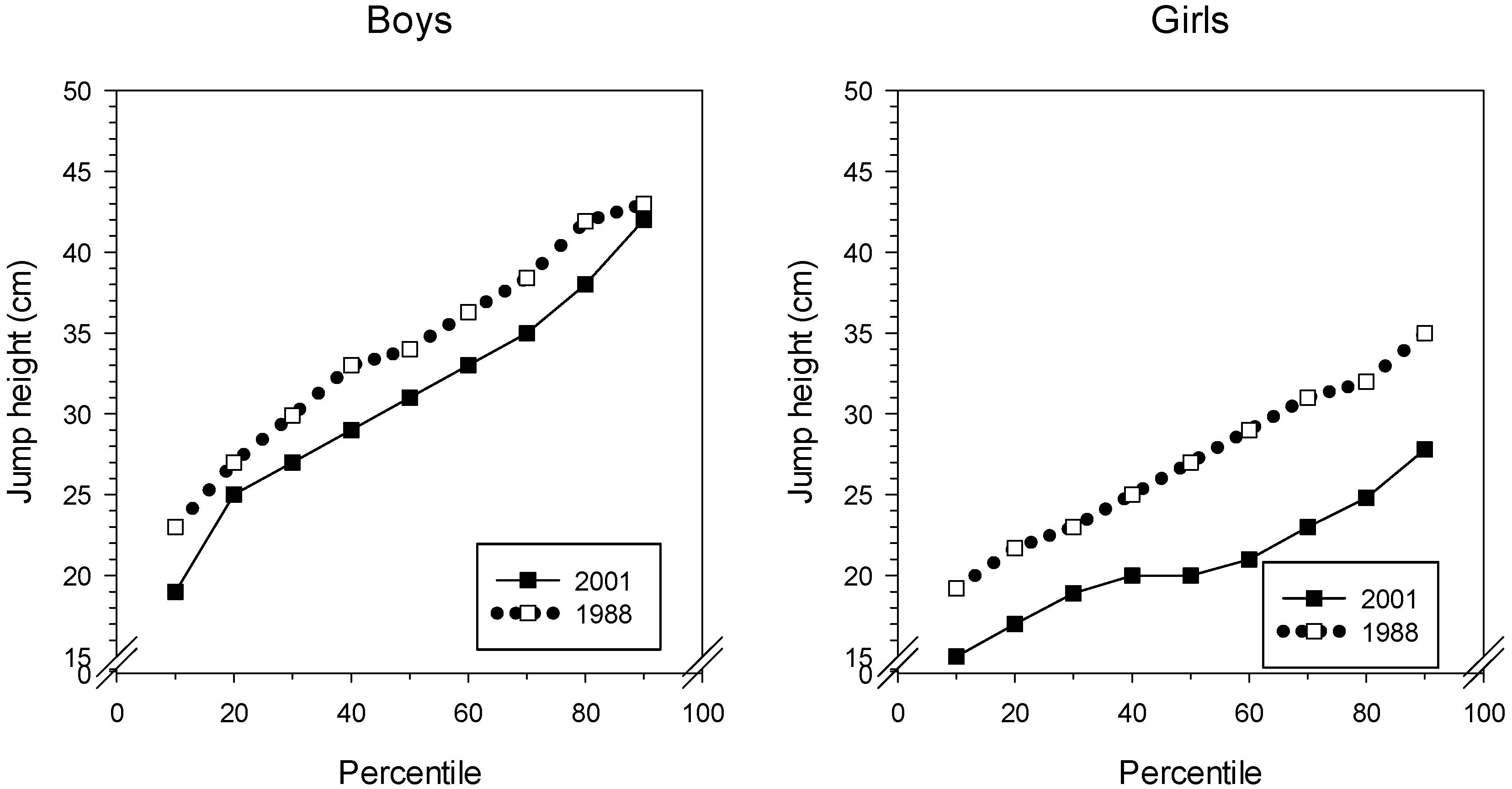
3.2. Jump Height
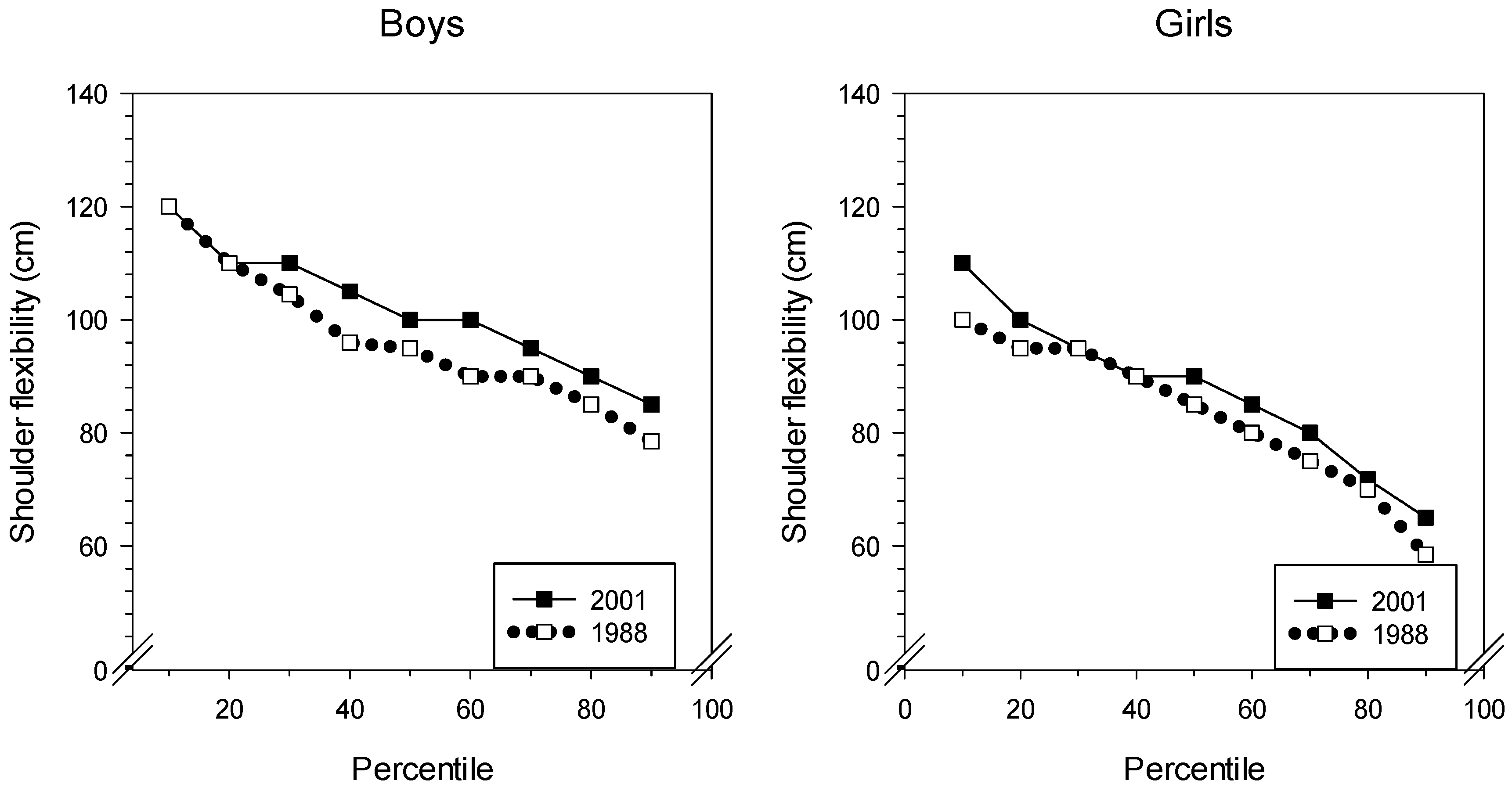
3.3. Shoulder Flexibility
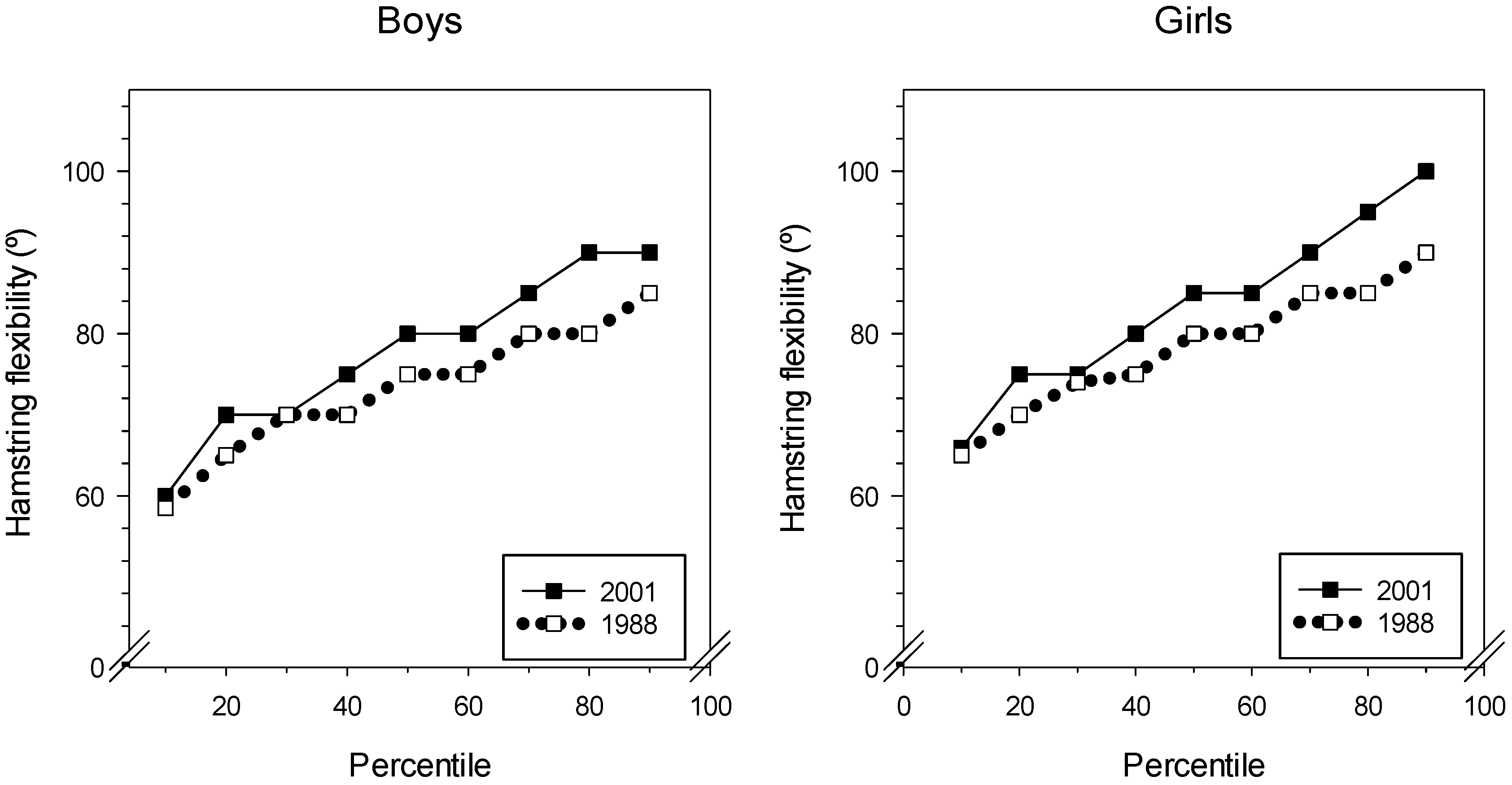
3.4. Hamstring Flexibility (Straight-Leg Raise)
3.5. Quantile Analysis
4. Discussion
4.1. Oxygen Uptake: Endurance
4.2. Jump Height
4.3. Shoulder Flexibility
4.4. Straight-Leg-Raise Test
4.5. Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tomkinson, G.R.; Léger, L.A.; Olds, T.S.; Cazorla, G. Secular trends in the performance of children and adolescents (1980–2000): An analysis of 55 studies of the 20 m shuttle run test in 11 countries. Sports Med. Auckl. NZ 2003, 33, 285–300. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R.; Olds, T.S. Secular changes in pediatric aerobic fitness test performance: The global picture. Med. Sport Sci. 2007, 50, 46–66. [Google Scholar] [PubMed]
- Westerstahl, M.; Barnekow-Bergkvist, M.; Hedberg, G.; Jansson, E. Secular trends in body dimensions and physical fitness among adolescents in Sweden from 1974 to 1995. Scand. J. Med. Sci. Sports 2003, 13, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, J.C.; Malina, R.M. Secular trend in peak oxygen consumption among United States youth in the 20th century. Am. J. Hum. Biol. 2002, 14, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Fredriksen, P.M.; Thaulow, E.; Nystad, W.; Ingjer, F. Aerobic capacity in children and adolescents--Nordic results over the past 45 years. Tidsskr. Den Nor. Lægeforen. 1998, 118, 3106–3110. [Google Scholar]
- Dyrstad, S.M.; Berg, T.; Tjelta, L.I. Secular trends in aerobic fitness performance in a cohort of Norwegian adolescents. Scand. J. Med. Sci. Sports 2012, 22, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Dyrstad, S.M.; Aandstad, A.; Hallén, J. Aerobic fitness in young Norwegian men: a comparison between 1980 and 2002. Scand. J. Med. Sci. Sports 2005, 15, 298–303. [Google Scholar] [CrossRef]
- Dos Santos, F.K.; Prista, A.; Gomes, T.N.Q.F.; Daca, T.; Madeira, A.; Katzmarzyk, P.T.; Maia, J.A.R. Secular trends in physical fitness of Mozambican school-aged children and adolescents. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2015, 27, 201–206. [Google Scholar] [CrossRef]
- Ellingsen, F. Kartlegging av Styrke, Bevegelighet, Koordinasjon og Utholdenhet: Skoleelever i Akershus 1968 og 1997. In Mapping of Strength, Flexibility, Coordination and Endurance: School Children in Akershus County 1968 and 1997; Landslaget Fysisk Fostring i Skolen: Tønsberg, Norway, 1998. [Google Scholar]
- Huotari, P.R.T.; Nupponen, H.; Laakso, L.; Kujala, U.M. Secular trends in muscular fitness among Finnish adolescents. Scand. J. Public Health 2010, 38, 739–747. [Google Scholar] [CrossRef]
- Loprinzi, P.D. An initial assessment of secular trends in muscular strength among children, adolescents, and adults across the lifespan: National sample of Americans. Am. J. Health Promot. AJHP 2018, 32, 705–707. [Google Scholar] [CrossRef]
- Huotari, P.; Heikinaro-Johansson, P.; Watt, A.; Jaakkola, T. Fundamental movement skills in adolescents: Secular trends from 2003 to 2010 and associations with physical activity and BMI. Scand. J. Med. Sci. Sports 2018, 28, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Sahin, F.N.; Kiziyalli, M.; Genchi, R.; Basile, M.; Silva, C.; Loureiro, N.; Demetriou, Y.; Beckmann, J.; Pajaujiene, S.; et al. Physical fitness and motor coordination monitoring during enriched sport activities in a sample of children living in Europe. The ESA program. Acta Medica Mediterr. 2018, 34, 11–12. [Google Scholar]
- Åstrand, P.-O.; Ryhming, I. A nomogram for calculation of aerobic capacity (physical fitness) from pulse rate during sub-maximal work. J. Appl. Physiol. 1954, 7, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Åstrand, I. Aerobic work capacity in men and women with special reference to age. Acta Physiol. Scand. Suppl. 1960, 49, 1–92. [Google Scholar]
- Sargent, D.D.A. The physical test of a man. Am. Phys. Educ. Rev. 1921, 26, 188–194. [Google Scholar] [CrossRef]
- Haag, H.; Dassel, H. Fitness-Tests: Lehrhilfen Zum Testen im Sportunterricht für Schule und Verein [Teaching Aids for Testing in Physical Education for Schools and Clubs]; Verlag K. Hofmann: Schorndorf, Germany, 1975. [Google Scholar]
- De Salles, P.G.; Vasconcellos, F.V.; de Salles, G.F.; Fonseca, R.T.; Dantas, E.H. Validity and reproducibility of the Sargent jump test in the assessment of explosive strength in soccer players. J. Hum. Kinet. 2012, 33, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Aaberge, K. Prosjektrapport for utveljing av testbatteri og resultat for fysisk test og re-test av 240 6-klassingar. [Project Report for Selection of Test Battery and Results of Physical Test and Re-test of 240 6th Graders]; Songdal lærarhøgskule: Sogndal, Norway, 1988. [Google Scholar]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br. J. Sports Med. 2017. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Olds, T.S. Secular changes in aerobic fitness test performance of Australasian children and adolescents. Med. Sport Sci. 2007, 50, 168–182. [Google Scholar]
- Keren, G.; Magazanik, A.; Epstein, Y. A comparison of various methods for the determination of VO2max. Eur. J. Appl. Physiol. 1980, 45, 117–124. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef]
- Andersen, L.B.; Froberg, K.; Kristensen, P.L.; Moller, N.C.; Resaland, G.K.; Anderssen, S.A. Secular trends in physical fitness in Danish adolescents. Scand. J. Med. Sci. Sports 2010, 20, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Kasch, F.W. The validity of the Astrand and Sjostrand submaximal tests. Phys. Sportsmed. 1984, 12, 47–54. [Google Scholar] [CrossRef]
- Teräslinna, P.; Ismail, A.H.; MacLeod, D.F. Nomogram by Astrand and Ryhming as a predictor of maximum oxygen intake. J. Appl. Physiol. 1966, 21, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, B. Static Flexibility Test for the Shoulder. Available online: https://www.brianmac.co.uk/flextest4.htm#ref (accessed on 22 August 2018).
- Taylor, M.J.D.; Cohen, D.; Voss, C.; Sandercock, G.R.H. Vertical jumping and leg power normative data for English school children aged 10–15 years. J. Sports Sci. 2010, 28, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Bovet, P.; Auguste, R.; Burdette, H. Strong inverse association between physical fitness and overweight in adolescents: A large school-based survey. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Temfemo, A.; Hugues, J.; Chardon, K.; Mandengue, S.-H.; Ahmaidi, S. Relationship between vertical jumping performance and anthropometric characteristics during growth in boys and girls. Eur. J. Pediatr. 2009, 168, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R. Global changes in anaerobic fitness test performance of children and adolescents (1958–2003). Scand. J. Med. Sci. Sports 2007, 17, 497–507. [Google Scholar] [CrossRef]
- Júlíusson, P.B.; Roelants, M.; Eide, G.E.; Hauspie, R.; Waaler, P.E.; Bjerknes, R. Overweight and obesity in Norwegian children: secular trends in weight-for-height and skinfolds. Acta Paediatr. Oslo Nor. 2007, 96, 1333–1337. [Google Scholar] [CrossRef]
- Andersen, L.F.; Lillegaard, I.T.L.; Øverby, N.; Lytle, L.; Klepp, K.-I.; Johansson, L. Overweight and obesity among Norwegian schoolchildren: Changes from 1993 to 2000. Scand. J. Public Health 2005, 33, 99–106. [Google Scholar] [CrossRef]
- Hartig, D.E.; Henderson, J.M. Increasing hamstring flexibility decreases lower extremity overuse injuries in military basic trainees. Am. J. Sports Med. 1999, 27, 173–176. [Google Scholar] [CrossRef]
- Shacklock, M. Clinical Neurodynamics. A New System of Musculoskeletal Treatment; Elsevier: Amsterdam, The Netherlands, 2005; ISBN 0-7506-5456-2. [Google Scholar]
- López-Miñarro, P.Á.; Muyor, J.M.; Alacid, F.; Vaquero-Cristóbal, R.; López-Plaza, D.; Isorna, M. Comparison of hamstring extensibility and spinal posture between kayakers and canoeists. Kinesiology 2013, 45, 163–170. [Google Scholar]
- Devillé, W.L.; van der Windt, D.A.; Dzaferagić, A.; Bezemer, P.D.; Bouter, L.M. The test of Lasègue: systematic review of the accuracy in diagnosing herniated discs. Spine 2000, 25, 1140–1147. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort | n | Mean | SD | p | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|---|
| Boys 2001 | 99 | 49.0 | 12.0 | 0.332 | 42.0 | 56.0 |
| Boys 1988 | 104 | 47.7 | 8.3 | 42.0 | 53.5 | |
| Girls 2001 | 77 | 42.0 | 11.3 | 0.374 | 35.0 | 49.0 |
| Girls 1988 | 83 | 43.4 | 8.2 | 38.0 | 48.0 |
| Cohort | n | Mean | SD | p | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|---|
| Boys 2001 | 99 | 31.1 | 8.4 | 0.001 | 26.0 | 36.0 |
| Boys 1988 | 106 | 35.0 | 7.9 | 30.0 | 41.5 | |
| Girls 2001 | 91 | 20.1 | 5.5 | <0.001 | 16.0 | 24.0 |
| Girls 1988 | 81 | 27.1 | 6.1 | 23.0 | 31.0 |
| Cohort | n | Mean | SD | p | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|---|
| Boys 2001 | 99 | 100.0 | 14.6 | 0.039 | 110.0 | 90.0 |
| Boys 1988 | 106 | 95.8 | 14.4 | 105.0 | 85.0 | |
| Girls 2001 | 92 | 87.2 | 17.2 | <0.01 | 100.0 | 80.0 |
| Girls 1988 | 86 | 81.6 | 16.0 | 95.0 | 75.0 |
| Cohort | n | Mean | SD | p | 25th Percentile | 75th Percentile | |
|---|---|---|---|---|---|---|---|
| Right Leg | Boys 2001 | 99 | 77.5 | 11.6 | <0.001 | 70.0 | 80.0 |
| Boys 1988 | 106 | 72.2 | 9.0 | 65.0 | 85.0 | ||
| Girls 2001 | 92 | 83.1 | 13.1 | 0.004 | 75.0 | 90.0 | |
| Girls 1988 | 85 | 77.9 | 10.6 | 70.0 | 85.0 | ||
| Left Leg | Boys 2001 | 99 | 78.3 | 11.9 | <0.001 | 70.0 | 85.0 |
| Boys 1988 | 98 | 71.6 | 8.4 | 65.0 | 75.0 | ||
| Girls 2001 | 92 | 82.5 | 13.8 | 0.036 | 72.5 | 90.0 | |
| Girls 1988 | 85 | 78.6 | 10.5 | 70.0 | 85.0 | ||
| Variable | τ | p | Quantile |
|---|---|---|---|
| Boys shoulder flex | −2.12 | 0.036 | 0.1 |
| Boys straight-leg-raise test, right leg | −2.99 | 0.004 | 0.9 |
| Boys straight-leg-raise test, left leg | −7.85 | <0.001 | 0.1 |
| Boys straight-leg-raise test, left leg | −3.57 | 0.001 | 0.3 |
| Boys straight-leg-raise test, left leg | −3.07 | 0.003 | 0.4 |
| Girls maximal oxygen uptake | 2.48 | 0.015 | 0.1 |
| Girls maximal oxygen uptake | 3.02 | 0.003 | 0.3 |
| Girls maximal oxygen uptake | 3.16 | 0.002 | 0.5 |
| Girls maximal oxygen uptake | 3.62 | 0.001 | 0.6 |
| Girls jump height | −2.23 | 0.029 | 0.8 |
| Girls straight-leg-raise test, right leg | 2.00 | 0.048 | 0.7 |
| Girls straight-leg-raise test, left leg | 1.99 | 0.050 | 0.9 |
| Quantile | Variable | Boys 2001 | Boys 1988 | Girls 2001 | Girls 1988 |
|---|---|---|---|---|---|
| Qworst | VO2max (mL·kg−1·min−1) | 34 (6) | 36 (4) * | 28 (4) | 33 (3) * |
| Jump height (cm) | 20.3 (5.1) | 24.6 (4.2) * | 18.6 (5.6) | 23.9 (6.1) * | |
| Shoulder flexibility (cm) | 115.6 (5.8) | 78.4 (7.6) * | 88.2 (16.9) | 71.3 (19.7) * | |
| Right straight-leg raise (°) | 59.5 (4.1) | 56.7 (3.8) * | 64.8 (6.0) | 62.0 (4.6) n.s. | |
| Left straight-leg raise (°) | 61.9 (4.0) | 58.1 (3.3) # | 65.9 (5.6) | 62.7 (3.3) # | |
| Qbest | VO2max (mL·kg−1·min−1) | 63 (7) | 58 (4) # | 57 (6) | 54 (7) n.s. |
| Jump height (cm) | 41.1 (4.3) | 44.7 (3.6) * | 27.2 (3.2) | 34.1 (4.0) * | |
| Shoulder flexibility (cm) | 76.8 (10.3) | 73.5 (6.5) n.s. | 63.2 (18.4) | 59.3 (11.7) * | |
| Right straight-leg raise (°) | 91.0 (6.4) | 82.0 (2.5) # | 97.0 (9.5) | 90.0 (5.9) # | |
| Left straight-leg raise (°) | 90.7 (6.5) | 81.9 (3.2) # | 97.3 (9.1) | 90.4 (5.9) # |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aaberge, K.; Mamen, A. A Comparative Study of Fitness Levels among Norwegian Youth in 1988 and 2001. Sports 2019, 7, 50. https://doi.org/10.3390/sports7020050
Aaberge K, Mamen A. A Comparative Study of Fitness Levels among Norwegian Youth in 1988 and 2001. Sports. 2019; 7(2):50. https://doi.org/10.3390/sports7020050
Chicago/Turabian StyleAaberge, Kari, and Asgeir Mamen. 2019. "A Comparative Study of Fitness Levels among Norwegian Youth in 1988 and 2001" Sports 7, no. 2: 50. https://doi.org/10.3390/sports7020050
APA StyleAaberge, K., & Mamen, A. (2019). A Comparative Study of Fitness Levels among Norwegian Youth in 1988 and 2001. Sports, 7(2), 50. https://doi.org/10.3390/sports7020050