Effects of Different Combinations of Concentric and Eccentric Resistance Training Programs on Traditional and Alternative Hamstrings-to-Quadriceps Ratios





Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
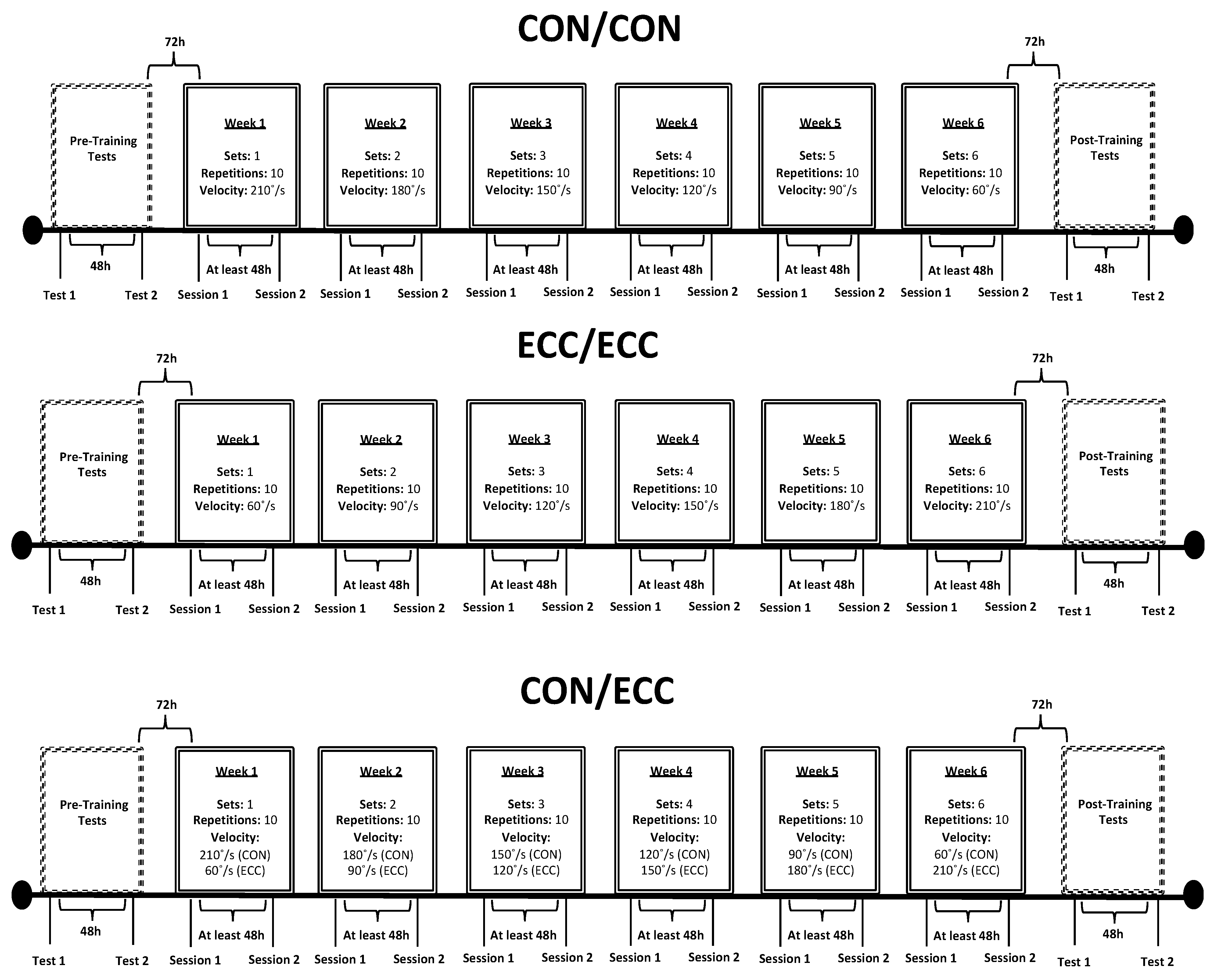
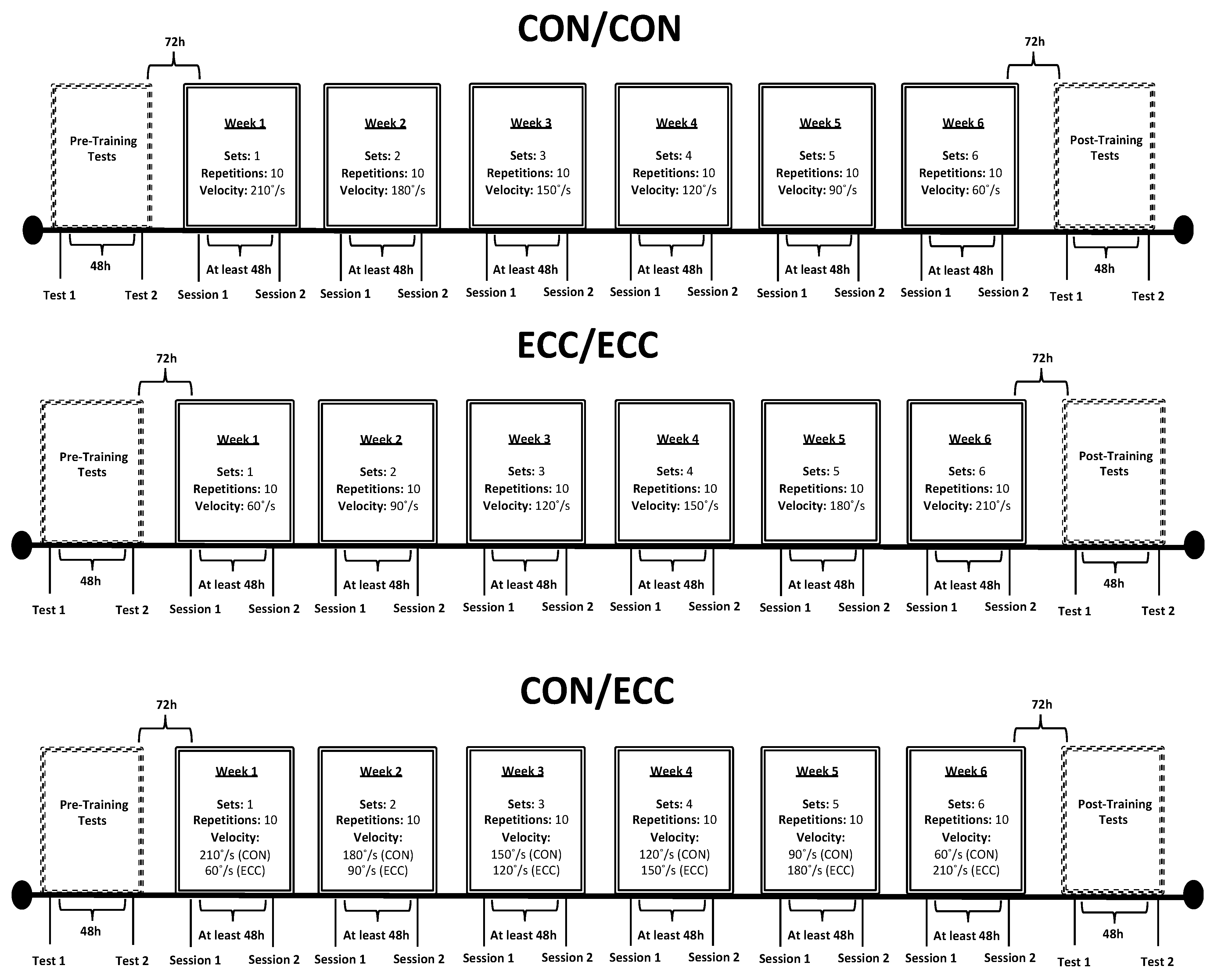
2.2. Experimental Design
2.3. Pretesting
2.3.1. Ultrasound Measurements
2.3.2. Isometric Maximal Testing, MA, and RTD
2.3.3. Isokinetic Maximal Testing
2.3.4. Traditional and Alternative H:Q Ratios
2.4. Training Sessions
2.5. Post-Testing
2.6. Statistical Analyses
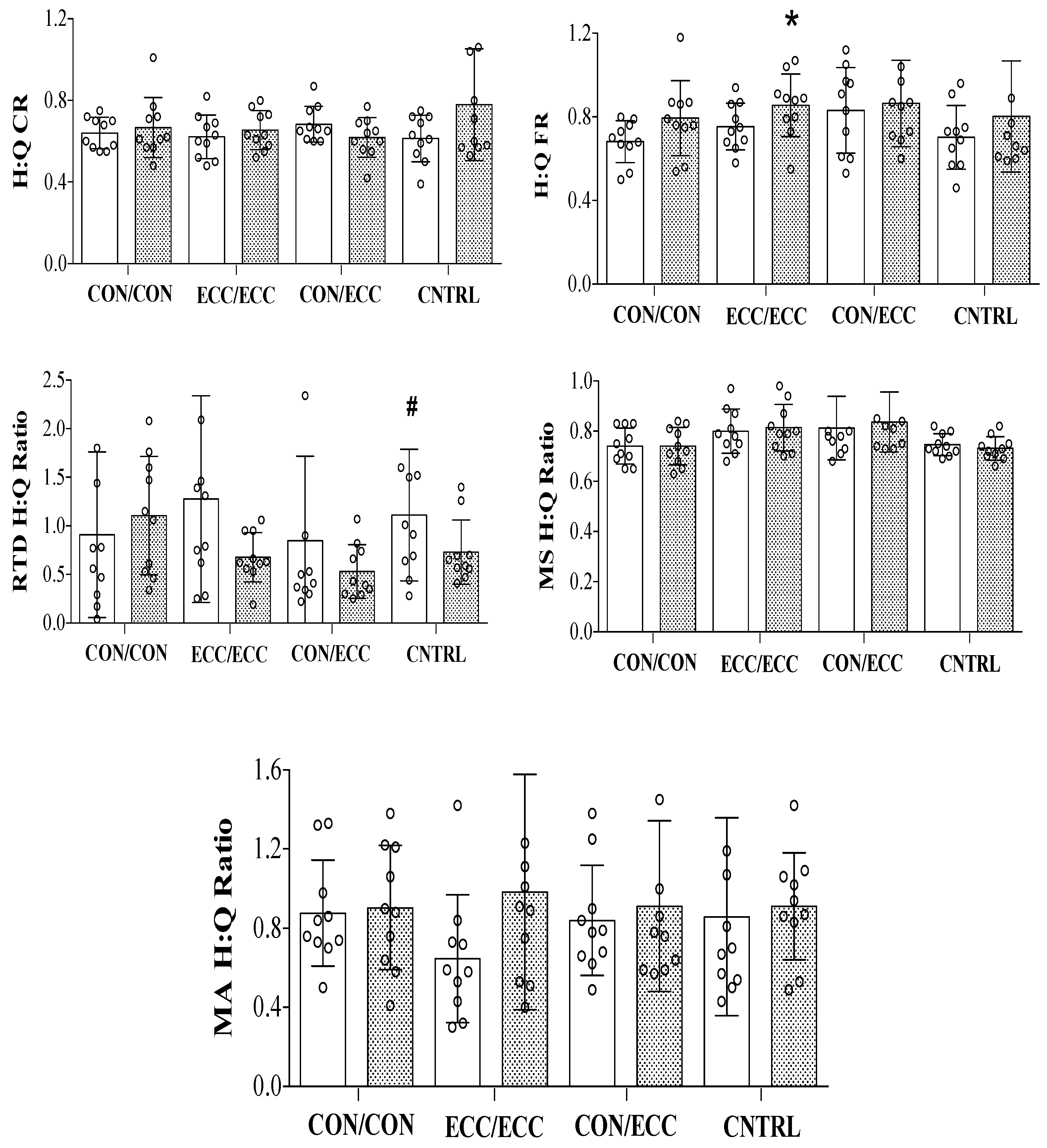
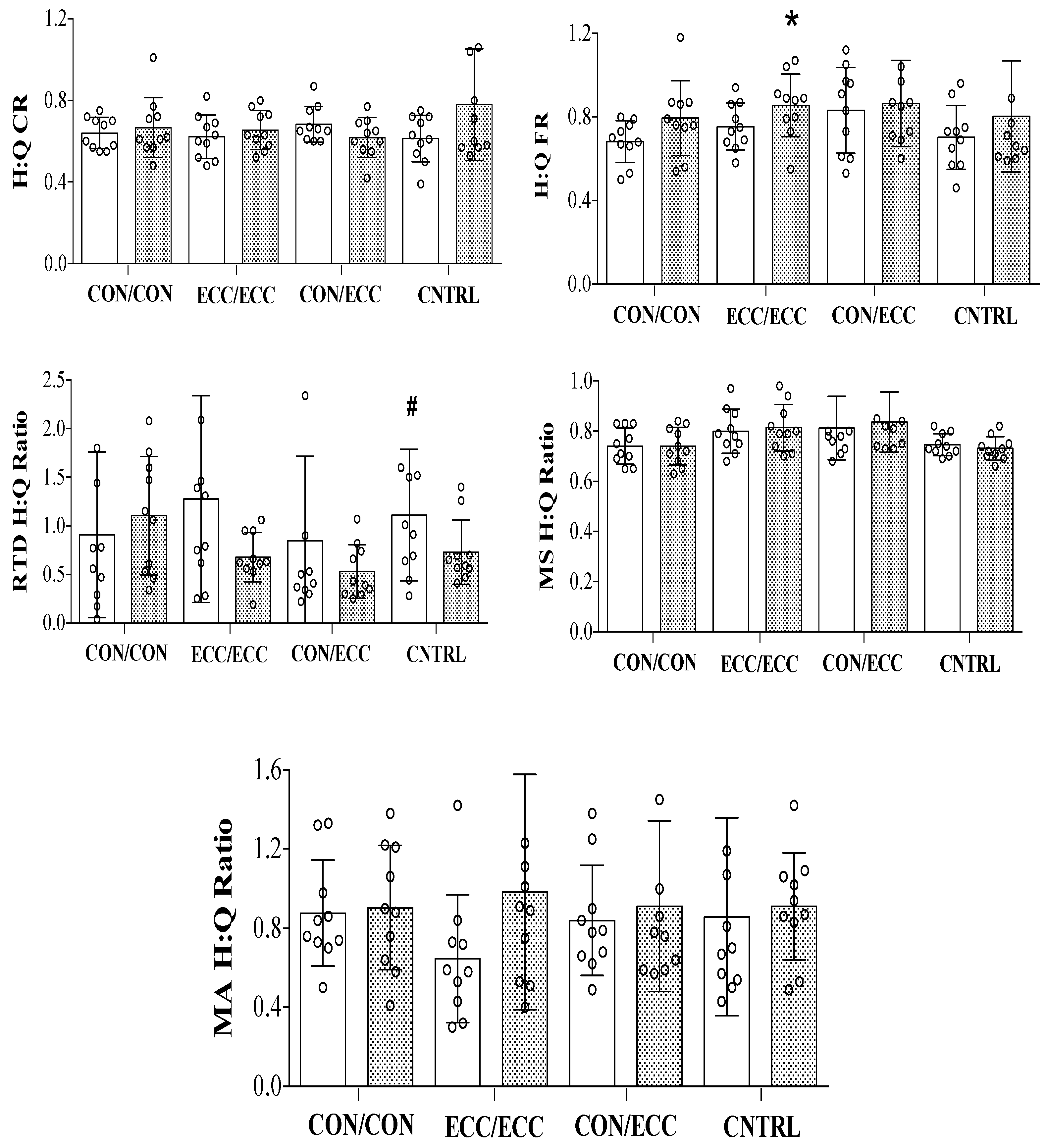
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Coombs, R.; Garbutt, G. Development in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J. Sports Sci. Med. 2002, 1, 56–62. [Google Scholar]
- Ruas, C.V.; Minozzo, F.; Pinto, M.D.; Brown, L.E.; Pinto, R.S. Lower-extremity strength ratios of professional soccer players according to field position. J. Strength Cond. Res. 2015, 29, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Ruas, C.V.; Pinto, M.D.; Brown, L.E.; Minozzo, F.; Mil-Homens, P.; Pinto, R.S. The association between conventional and dynamic control knee strength ratios in elite soccer players. Isokinet. Exerc. Sci. 2015, 23, 1–12. [Google Scholar] [CrossRef]
- Aagaard, P.; Simonsen, E.B.; Magnusson, S.P.; Larsson, B.; Dyhre-Poulsen, P. A new concept for isokinetic hamstring: Quadriceps muscle strength ratio. Am. J. Sports Med. 1998, 26, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Croisier, J.L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.; Suen, A.M.Y.; Yeung, E.W. A prospective cohort study of hamstring injuries in competitive sprinters: Preseason muscle imbalance as a possible risk factor. Br. J. Sports Med. 2009, 43, 589–594. [Google Scholar] [CrossRef]
- Li, R.C.; Maffulli, N.; Hsu, Y.C.; Chan, K.M. Isokinetic strength of the quadriceps and hamstrings and functional ability of anterior cruciate deficient knees in recreational athletes. Br. J. Sports Med. 1996, 30, 161–164. [Google Scholar] [CrossRef]
- Van Dyk, N.; Bahr, R.; Whiteley, R.; Tol, J.L.; Kumar, B.D.; Hamilton, B.; Farooq, A.; Witvrouw, E. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: A 4-year cohort study. Am. J. Sports Med. 2016, 44, 1789–1795. [Google Scholar] [CrossRef]
- Ruas, C.V.; Pinto, R.S.; Haff, G.G.; Lima, C.D.; Pinto, M.D.; Brown, L.E. Alternative methods of determining hamstrings-to-quadriceps ratios: A comprehensive review. Sports Med. Open 2019, 5, 11. [Google Scholar] [CrossRef]
- Grygorowicz, M.; Michalowska, M.; Walczak, T.; Owen, A.; Grabski, J.K.; Pyda, A.; Piontek, T.; Kotwicki, T. Discussion about different cut-off values of conventional hamstring-to-quadriceps ratio used in hamstring injury prediction among professional male football players. PLoS ONE 2017, 12, e0188974. [Google Scholar] [CrossRef]
- Greco, C.C.; Da Silva, W.L.; Camarda, S.R.; Denadai, B.S. Rapid hamstrings/quadriceps strength capacity in professional soccer players with different conventional isokinetic muscle strength ratios. J. Sports Sci. Med. 2012, 11, 418–422. [Google Scholar] [PubMed]
- Hannah, R.; Minshull, C.; Smith, S.L.; Folland, J.P. Longer electromechanical delay impairs hamstrings explosive force versus quadriceps. Med. Sci. Sports Exerc. 2014, 46, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Grazioli, R.; Lopez, P.; Andersen, L.L.; Machado, C.L.F.; Pinto, M.D.; Cadore, E.L.; Pinto, R.S. Hamstring rate of torque development is more affected than maximal voluntary contraction after a professional soccer match. Eur. J. Sport. Sci. 2019, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jordan, M.J.; Aagaard, P.; Herzog, W. Rapid hamstrings/quadriceps strength in acl-reconstructed elite alpine ski racers. Med. Sci. Sports Exerc. 2015, 47, 109–119. [Google Scholar] [CrossRef]
- Evangelidis, P.E.; Massey, G.J.; Pain, M.T.G.; Folland, J.P. Strength and size relationships of the quadriceps and hamstrings with special reference to reciprocal muscle balance. Eur. J. Appl. Physiol. 2016, 116, 593–600. [Google Scholar] [CrossRef]
- Wieschhoff, G.G.; Mandell, J.C.; Czuczman, G.J.; Nikac, V.; Shah, N.; Smith, S.E. Acute non-contact anterior cruciate ligament tears are associated with relatively increased vastus medialis to semimembranosus cross-sectional area ratio: A case-control retrospective mr study. Skeletal. Radiol. 2017, 46, 1469–1475. [Google Scholar] [CrossRef]
- Behan, F.P.; Maden-Wilkinson, T.M.; Pain, M.T.G.; Folland, J.P. Sex differences in muscle morphology of the knee flexors and knee extensors. PLoS ONE 2018, 13, e0190903. [Google Scholar] [CrossRef]
- Aagaard, P.; Simonsen, E.B.; Andersen, J.L.; Magnusson, S.P.; Bojsen-Moller, F.; Dyhre-Poulsen, P. Antagonist muscle coactivation during isokinetic knee extension. Scand. J. Med. Sci. Sports 2000, 10, 58–67. [Google Scholar] [CrossRef]
- Kellis, E.; Katis, A. Quantification of functional knee flexor to extensor moment ratio using isokinetics and electromyography. J. Athl. Train. 2007, 42, 477–485. [Google Scholar]
- Ruas, C.V.; McManus, R.T.; Bentes, C.M.; Costa, P.B. Acute effects of proprioceptive neuromuscular facilitation on peak torque and muscle imbalance. J. Funct. Morphol. Kinesiol. 2018, 3, 63. [Google Scholar] [CrossRef]
- Costa, P.B.; Ruas, C.V.; Smith, C.M. Effects of stretching and fatigue on peak torque, muscle imbalance and stability. J. Sports Med. Phys. Fitness 2018, 58, 957–965. [Google Scholar] [PubMed]
- Krajnc, Z.; Vogrin, M.; Recnik, G.; Crnjac, A.; Drobnic, M.; Antolic, V. Increased risk of knee injuries and osteoarthritis in the non-dominant leg of former professional football players. Wien. Klin. Wochenschr 2010, 122 (Suppl. 2), 40–43. [Google Scholar] [CrossRef]
- Ruas, C.V.; Brown, L.E.; Pinto, R.S. Lower-extremity side-to-side strength asymmetry of professional soccer players according to playing position. Kinesiology 2015, 47, 188–192. [Google Scholar]
- Rech, A.; Radaelli, R.; Goltz, F.R.; da Rosa, L.H.T.; Schneider, C.D.; Pinto, R.S. Echo intensity is negatively associated with functional capacity in older women. Age 2014, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ruas, C.V.; Pinto, R.S.; Lima, C.D.; Costa, P.B.; Brown, L.E. Test-retest reliability of muscle thickness, echo-intensity and cross sectional area of quadriceps and hamstrings muscle groups using b-mode ultrasound. Int. J. Kinesiol. Sports Sci. 2017, 5, 35–41. [Google Scholar] [CrossRef]
- Ruas, C.V.; Brown, L.E.; Lima, C.D.; Gregory Haff, G.; Pinto, R.S. Different muscle action training protocols on quadriceps-hamstrings neuromuscular adaptations. Int. J. Sports Med. 2018, 39, 355–365. [Google Scholar] [CrossRef]
- Munro, B.H. Statistical Methods for Health Care Research, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; Volume 1. [Google Scholar]
- Jenkins, N.D.; Miller, J.M.; Buckner, S.L.; Cochrane, K.C.; Bergstrom, H.C.; Hill, E.C.; Smith, C.M.; Housh, T.J.; Cramer, J.T. Test-retest reliability of single transverse versus panoramic ultrasound imaging for muscle size and echo intensity of the biceps brachii. Ultrasound Med. Biol. 2015, 41, 1584–1591. [Google Scholar] [CrossRef]
- Pinto, R.S.; Correa, C.S.; Radaelli, R.; Cadore, E.L.; Brown, L.E.; Bottaro, M. Short-term strength training improves muscle quality and functional capacity of elderly women. Age 2014, 36, 365–372. [Google Scholar] [CrossRef]
- Brown, L.E.; Weir, J.P. Asep procedures recommendation i: Accurate assessment of muscular strength and power. J. Exerc. Physiol. Online 2001, 4, 1–21. [Google Scholar]
- Ruas, C.V.; Brown, L.E.; Lima, C.D.; Costa, P.B.; Pinto, R.S. Effect of three different muscle action training protocols on knee strength ratios and performance. J. Strength Cond. Res. 2018, 32, 2154–2165. [Google Scholar] [CrossRef]
- Golik-Peric, D.; Drapsin, M.; Obradovic, B.; Drid, P. Short-term isokinetic training versus isotonic training: Effects on asymmetry in strength of thigh muscles. J. Hum. Kinet. 2011, 30, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.E. Isokinetics in Human Performance; Human Kinetics: Champaign, IL, USA, 2000. [Google Scholar]
- Rhea, M.R. Determining the magnitude of treatment effects in strength training research through the use of the effect size. J. Strength Cond. Res. 2004, 18, 918–920. [Google Scholar] [PubMed]
- Askling, C.; Karlsson, J.; Thorstensson, A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand. J. Med. Sci. Sports 2003, 13, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Mjølsnes, R.; Arnason, A.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. Concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef]
- Croisier, J.L.; Forthomme, B.; Namurois, M.H.; Vanderthommen, M.; Crielaard, J.M. Hamstring muscle strain recurrence and strength performance disorders. Am. J. Sports Med. 2002, 30, 199–203. [Google Scholar] [CrossRef]
- Roig, M.; O’Brien, K.; Kirk, G.; Murray, R.; McKinnon, P.; Shadgan, B.; Reid, W.D. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: A systematic review with meta-analysis. Br. J. Sports Med. 2009, 43, 556–568. [Google Scholar] [CrossRef]
- Van Dyk, N.; Bahr, R.; Burnett, A.F.; Whiteley, R.; Bakken, A.; Mosler, A.; Farooq, A.; Witvrouw, E. A comprehensive strength testing protocol offers no clinical value in predicting risk of hamstring injury: A prospective cohort study of 413 professional football players. Br. J. Sports Med. 2017, 51, 1695–1702. [Google Scholar] [CrossRef]
- Eustace, S.J.; Page, R.M.; Greig, M. Contemporary approaches to isokinetic strength assessments in professional football players. Sci. Med. Football 2017, 1, 251–257. [Google Scholar] [CrossRef]
- Pinto, M.D.; Blazevich, A.J.; Andersen, L.L.; Mil-Homens, P.; Pinto, R.S. Hamstring-to-quadriceps fatigue ratio offers new and different muscle function information than the conventional non-fatigued ratio. Scand. J. Med. Sci. Sports 2018, 28, 282–293. [Google Scholar] [CrossRef]
- Kobayashi, H.; Kanamura, T.; Koshida, S.; Miyashita, K.; Okado, T.; Shimizu, T.; Yokoe, K. Mechanisms of the anterior cruciate ligament injury in sports activities: A twenty-year clinical research of 1700 athletes. J. Sports Sci. Med. 2010, 9, 669–675. [Google Scholar]
- Masuda, K.; Kikuhara, N.; Takahashi, H.; Yamanaka, K. The relationship between muscle cross-sectional area and strength in various isokinetic movements among soccer players. J. Sports Sci. 2003, 21, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, D.A.; Kamen, G.; Frost, G. Neural adaptations to resistive exercise: Mechanisms and recommendations for training practices. Sports Med. 2006, 36, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Colson, S.; Pousson, M.; Martin, A.; Van Hoecke, J. Isokinetic elbow flexion and coactivation following eccentric training. J. Electromyogr. Kinesiol. 1999, 9, 13–20. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| CON/CON | ECC/ECC | CON/ECC | CNTRL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | ES | Pre | Post | ES | Pre | Post | ES | Pre | Post | ES | |
| Q CON PT | 226.23 ± 47.05 | 231.84 ± 51.77 | 0.12 | 206.44 ± 46.84 | 240.44 ± 60.13 | 0.73 | 197.51 ± 38.28 | 222.06 ± 43.81 | 0.64 | 200.32 ± 39.00 | 202.39 ± 35.48 | 0.05 |
| Q ECC PT | 229.14 ± 63.15 | 306.83 ± 49.05 | 1.23 | 235.96 ± 64.90 | 312.67 ± 52.64 | 1.18 | 243.13 ± 50.07 | 279.90 ± 72.32 | 0.61 | 230.67 ± 58.86 | 223.62 ± 79.69 | −0.12 |
| Q PT (Collapsed, Action) | 340.80 ± 70.19 | 385.26 ± 63.77 | 0.63 | 324.42 ± 77.16 | 396.77 ± 81.95 * | 0.94 | 319.08 ± 63.59 | 362.01 ± 75.90 * | 0.68 | 315.66 ± 60.35 | 314.20 ± 62.32 | −0.024 |
| H CON PT | 143.79 ± 29.04 | 149.41 ± 23.84 | 0.19 | 127.65 ± 31.69 | 154.21 ± 26,68 | 0.84 | 135.17 ± 20.18 | 143.52 ± 21.22 | 0.41 | 124.91 ± 36.04 | 155.57 ± 61.81 | 0.85 |
| H ECC PT | 152.39 ± 31.31 | 179.86 ± 43.46 | 0.88 | 153.88 ± 31.21 | 198.31 ± 17.44 | 1.42 | 160.28 ± 35.98 | 186.67 ± 33.40 | 0.73 | 140.17 ± 37.29 | 158.55 ± 45.01 | 0.49 |
| H PT (Collapsed, Action) | 219.98 ± 42.89 | 396.76 ± 62.41 * | 4.12 | 204.58 ± 46.19 | 411.83 ± 57.60 * | 4.49 | 215.31 ± 35.43 | 373.23 ± 82.80 * | 4.46 | 195.99 ± 55.37 | 302.90 ± 88.76 * | 2.02 |
| Q RTD | 196.73 ± 144.91 | 162.53 ± 132.73 | −0.24 | 142.85 ± 149,77 | 225.91 ± 130.02 | 0.55 | 259.33 ± 128.33 | 304.99 ± 107.39 | 0.36 | 163.21 ± 67.40 | 222.85 ± 134.65 | 0.88 |
| H RTD | 102.99 ± 53.70 | 135.18 ± 49,53 | 0.60 | 111.84 ± 71.51 | 149.69 ± 88.82 | 0.53 | 157.57 ± 99.52 | 168.39 ± 101.24 | 0.11 | 170.00 ± 124.29 | 146.16 ± 78.80 | −0.19 |
| Q MT | 140.86 ± 9.80 | 149.31 ± 14.96 | 0.86 | 135.72 ± 10.84 | 154.47 ± 8.22 | 1.73 | 130.52 ± 14.96 | 138.60 ± 14.76 | 0.54 | 135.25 ± 7.51 | 131.55 ± 9.93 | −0.49 |
| H MT | 104.20 ± 8.77 | 110,48 ± 15.19 | 0.72 | 108.84 ± 16.15 | 125.62 ± 15.90 | 1.04 | 104.71 ± 12.59 | 115.39 ± 14.10 | 0.85 | 100.88 ± 7.96 | 96.32 ± 9.80 | −0.57 |
| MT (Collapsed, Muscle) | 192.86 ± 11.73 | 204.56 ± 20.78 * | 0.99 | 190.14 ± 17.42 | 217.28 ± 13.73 * | 1.56 | 182.88 ± 17.45 | 196.29 ± 18.33 * | 0.77 | 185.69 ± 10.61 # | 179.72 ± 14.22 | −0.56 |
| Q MA | 0.49 ± 0.22 | 0.57 ± 0.21 | 0.35 | 0.56 ± 0.19 | 0.45 ± 0.22 | −0.60 | 0.52 ± 0.26 | 0.41 ± 0.13 | −0.41 | 0.45 ± 0.20 | 0.45 ± 0.17 | 0.033 |
| H MA | 0.40 ± 0.15 | 0.51 ± 0.25 | 0.72 | 0.37 ± 0.26 | 0.37 ± 0.21 | 0.0097 | 0.44 ± 0.27 | 0.40 ± 0.28 | 0.00075 | 0.33 ± 0.14 | 0.39 ± 0.14 | 0.39 |
| MA (Collapsed, Muscle) | 0.65 ± 0.24 | 0.82 ± 0.30 * | 0.73 | 0.65 ± 0.32 | 0.64 ± 0.31 | −0.04 | 0.70 ± 0.38 | 0.63 ± 0.24 | −0.18 | 0.56 ± 0.20 | 0.65 ± 0.22 | 0.45 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruas, C.V.; Pinto, R.S.; Haff, G.G.; Lima, C.D.; Brown, L.E. Effects of Different Combinations of Concentric and Eccentric Resistance Training Programs on Traditional and Alternative Hamstrings-to-Quadriceps Ratios. Sports 2019, 7, 221. https://doi.org/10.3390/sports7100221
Ruas CV, Pinto RS, Haff GG, Lima CD, Brown LE. Effects of Different Combinations of Concentric and Eccentric Resistance Training Programs on Traditional and Alternative Hamstrings-to-Quadriceps Ratios. Sports. 2019; 7(10):221. https://doi.org/10.3390/sports7100221
Chicago/Turabian StyleRuas, Cassio V., Ronei S. Pinto, Guy G. Haff, Camila D. Lima, and Lee E. Brown. 2019. "Effects of Different Combinations of Concentric and Eccentric Resistance Training Programs on Traditional and Alternative Hamstrings-to-Quadriceps Ratios" Sports 7, no. 10: 221. https://doi.org/10.3390/sports7100221
APA StyleRuas, C. V., Pinto, R. S., Haff, G. G., Lima, C. D., & Brown, L. E. (2019). Effects of Different Combinations of Concentric and Eccentric Resistance Training Programs on Traditional and Alternative Hamstrings-to-Quadriceps Ratios. Sports, 7(10), 221. https://doi.org/10.3390/sports7100221