1. Introduction
In rehabilitation institutes, the anaerobic threshold is typically evaluated by the exercise tolerance test to assess the systemic aerobic capacity [
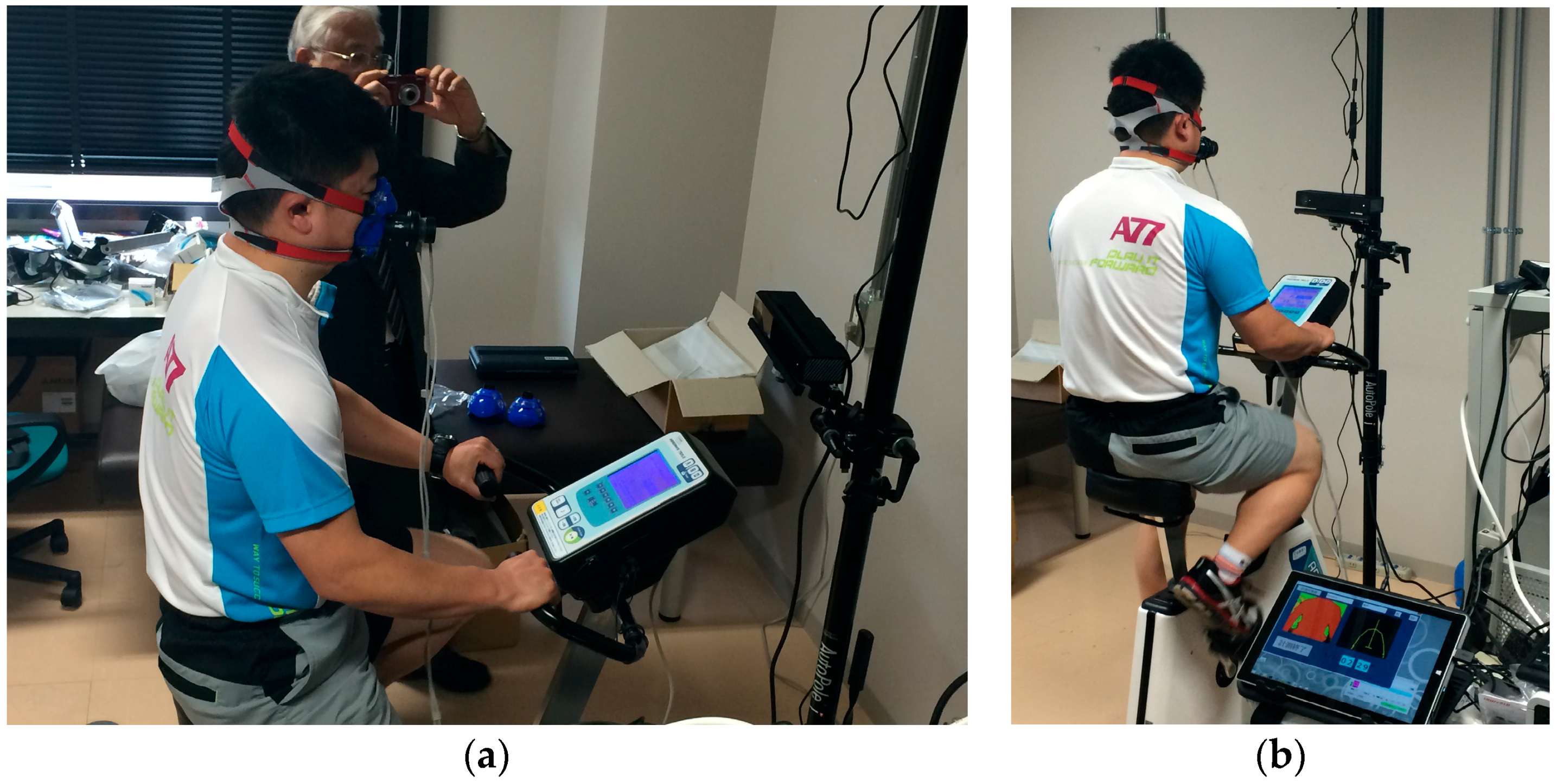
1]. Although an expiration gas analyzer is conventionally used for the assessment of the anaerobic threshold (AT), it is expensive. In addition, convenient assessment is difficult while using the expiration gas analyzer, because it requires mounting a gas mask on the face of participants, which poses significant problems, particularly in children and the elderly who usually have dfficulty wearing a mask. Thus, the development of a simple and cost-effective method to assess the AT is imperative for performing safe and effective exercise.
The VT, an equivalent index of the AT, is evaluated from the change in minute ventilation (VE) obtained by the ramp load test using a bicycle ergometer [
2]. The generation of anaerobic energy stimulates the production of the lactic acid, which when buffered with bicarbonate ion increases the ventilation volume by producing carbon dioxide [
3]. Caiozzeo [
4] demonstrated that the VT could be evaluated not only from the increased amount of carbon dioxide in expiration but also from the increased VE in the ramp load test.
Previously, we investigated a non-contact measurement with respiration in the rest position by using pattern light projection [
5], which elucidated that the volume change in the chest significantly correlated with the change in ventilation. In addition, this method established non-contact respiration measurement during pedaling with a recumbent bicycle ergometer [
2]. The application of Caiozzeo’s VT calculation by VE elucidated that the VT could be calculated even by the non-contact respiration measurement [
6]. In this method, the increase in the volume change because of the increase in the exercise intensity in the ramp load test is evaluated in the non-contact measurement, and the point at which the volume change rate increases is estimated as the VT, also referred as QVT. The result of this method suggests the feasibility of the systemic aerobic capacity assessment using the non-contact respiration measurement.
In our previous study mentioned above, although we used a recumbent bicycle ergometer, upright bicycle ergometers are more prevalent [
7]. Hence, improving the versatility of the proposed method necessitates non-contact respiration measurement using an upright bicycle ergometer. In upright bicycle ergometers, the body motion by pedaling is higher than those in the recumbent types. However, non-contact respiration measurement by pedaling using an upright bicycle ergometer is considered challenging. Hence, one study proposed a method to facilitate stable non-contact respiration measurement by reducing the impact of the pedaling motion [
8].
In our previous studies, we used a sensor based on the active stereo method, called fiber-grating vision sensor (FG sensor), which was developed independently by us and is not sold in general [
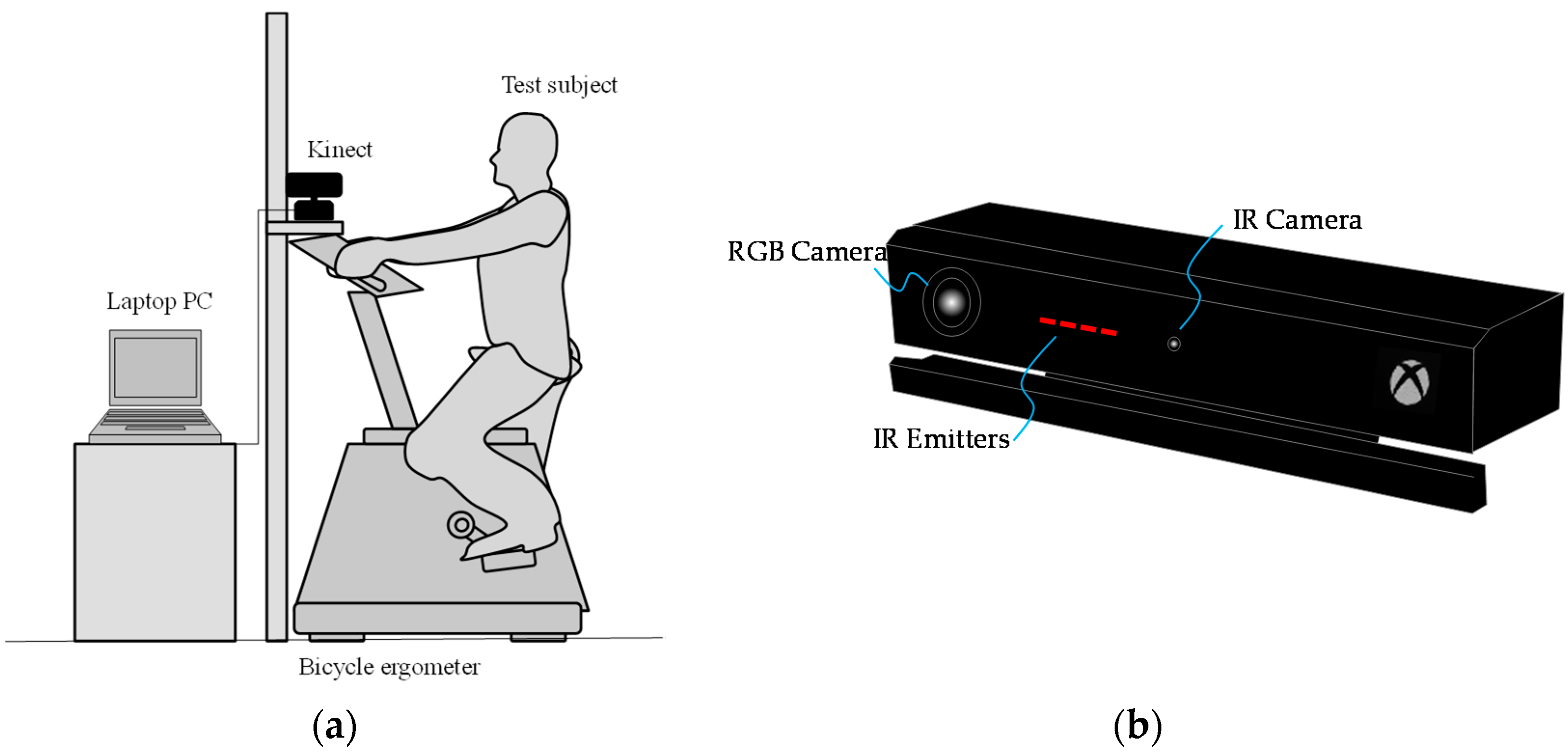
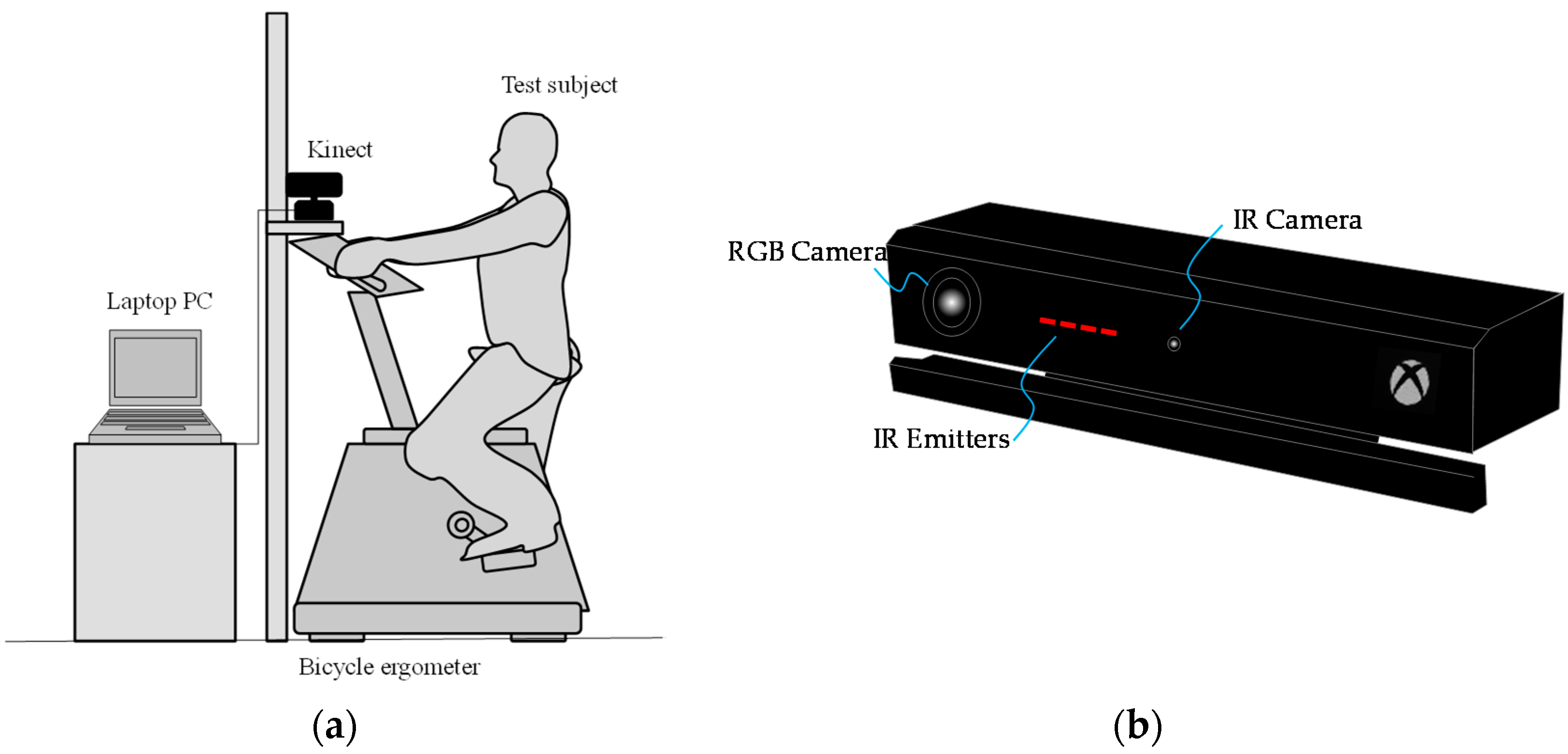
9]. In 2010, Microsoft launched the Kinect sensor as a non-contact controller of the game console. The Kinect sensor is a three-dimensional vision sensor based on the active stereo in which the pattern light—called ‘light coding’—is projected onto an object, and the three-dimensional shape of the object is reconstructed by image analysis of the pattern light distribution. The Kinect sensor is cost-effective and it facilitates real-time processing of three-dimensional data measured by our own program because it supports USB connection to a PC. For this reason, Kinect sensors are used in a wide range of research fields for various purposes.
In another study of ours, we investigated the respiration measurement using the Kinect sensor as an alternative to the FG sensor in the ramp load test. The findings revealed that the quantitative respiration measurement in the resting posture is possible with the Kinect but not the FG sensor [
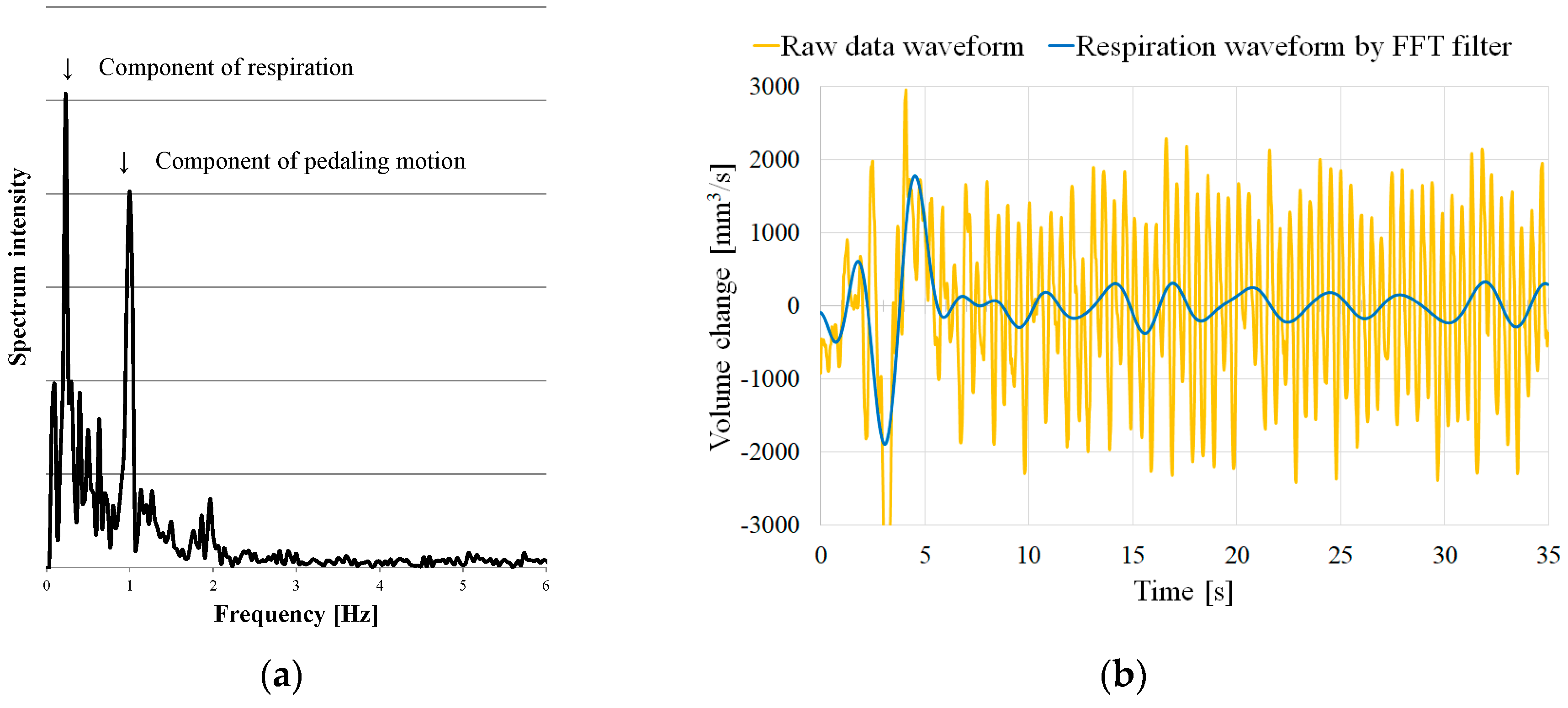
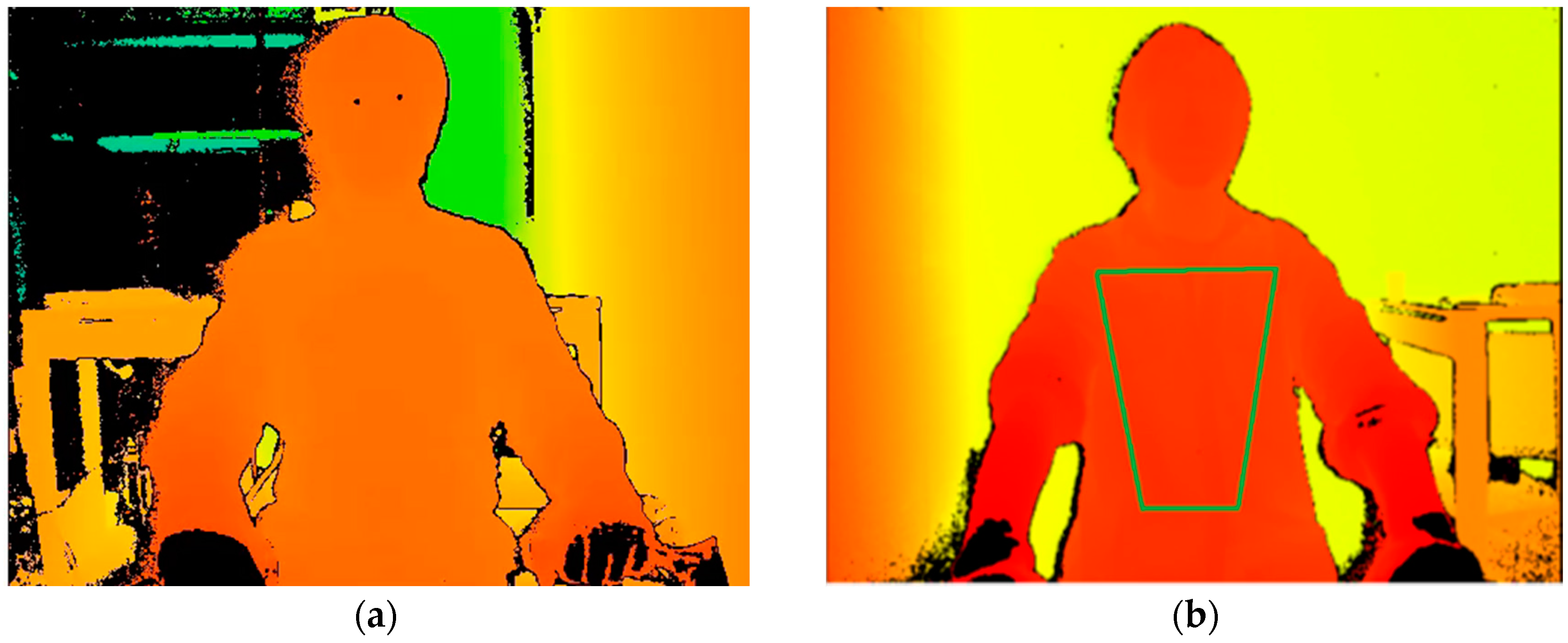
10]. As mentioned above, since the change in the posture by pedaling is significant in the test using the upright bicycle ergometer, reducing the impact of the body movement on the assessment of signal is essential. Hence, we proposed a method to consider the part of the body (i.e., chest and abdomen) where the respiratory motion was likely to appear as a region of interest (ROI). Consequently, we illustrated that the accuracy of the quasi tidal volume (QTV) fluctuation can be enhanced by filtering the three-dimensional shape change in the ROI [
11]. However, even this method did not facilitate the complete elimination of the effect of a large change in the posture and was, thus, considered difficult to apply at a high exercise intensity of ≥100 W.
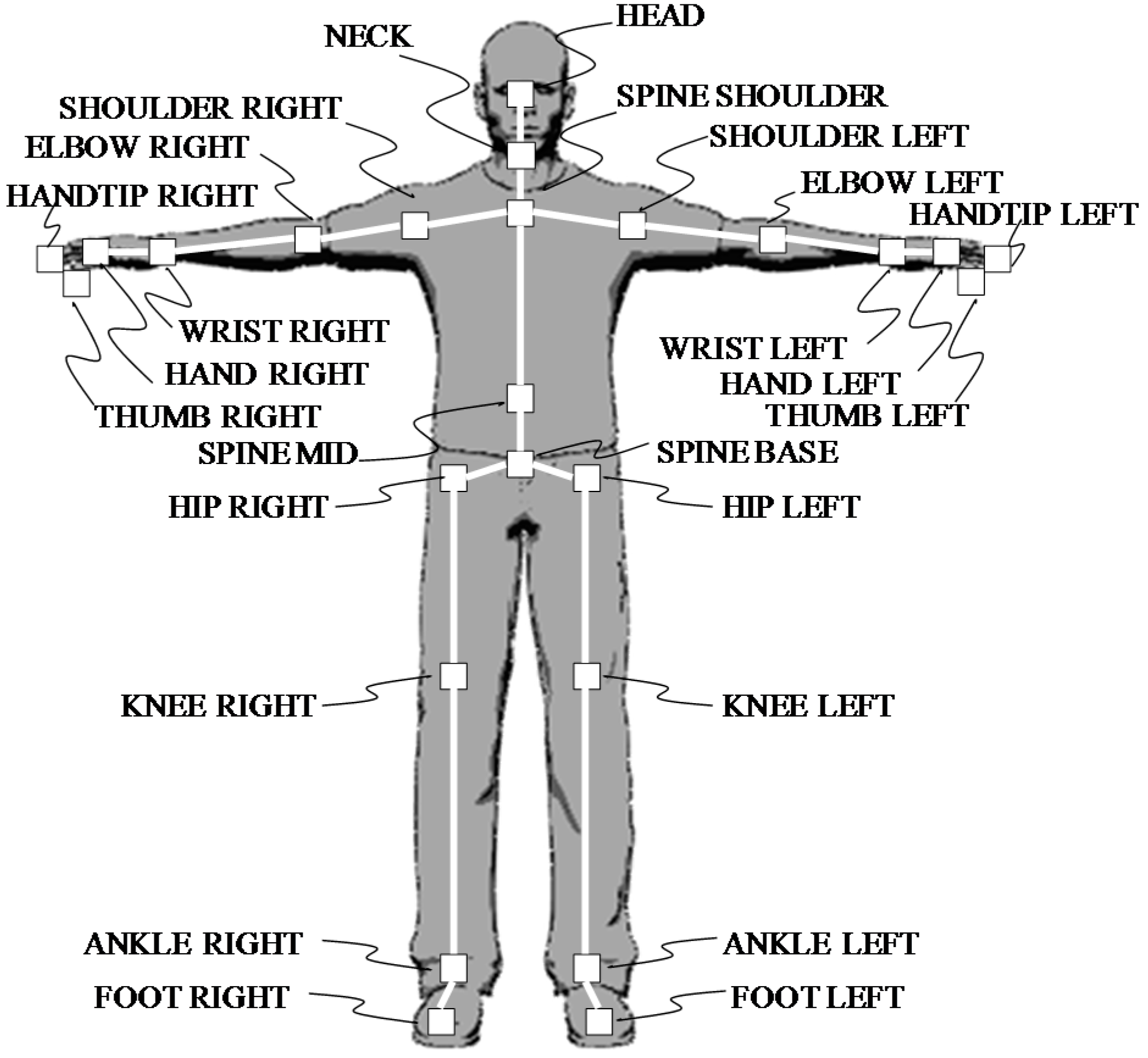
In 2014, a new version of the Kinect sensor (Kinect v2 sensor) was released, in which the measurement method was revised from active stereo to time-of-flight (TOF). The principle of TOF states that the distance is calculated from the time until the light projected from the light source is reflected by an object and reaches a light-receiving sensor. Typically, light-receiving sensors are distributed in a two-dimensional array and the distance distribution, in which the distance image can be acquired. Apparently, data obtained from the distance image facilitates three-dimensional shape reconstruction of the object. Although the measurement accuracy of the Kinect v2 sensor is almost equal to that of the previous version, its motion capture function has been enhanced for its easy use.
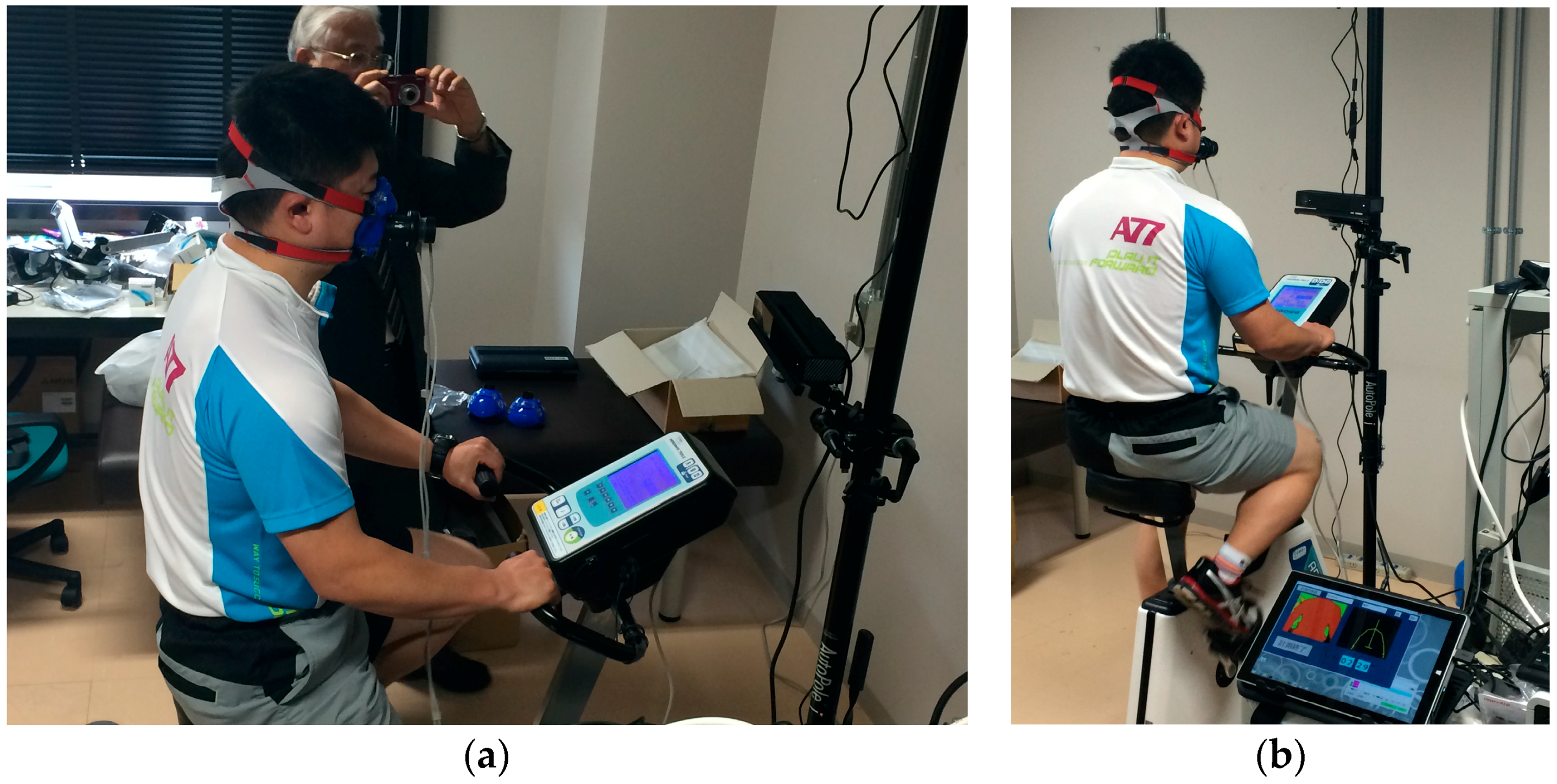
By tracking the thoracoabdominal activity using the motion capture function of the Kinect v2 sensor, this study aims to propose a non-contact respiration measurement during the exercise tolerance test corresponding to an increase in the body movement with an increasing exercise intensity. Additionally, it assesses the validity of the proposed method by comparative experiment using the expiratory gas analyzer.
3. Results
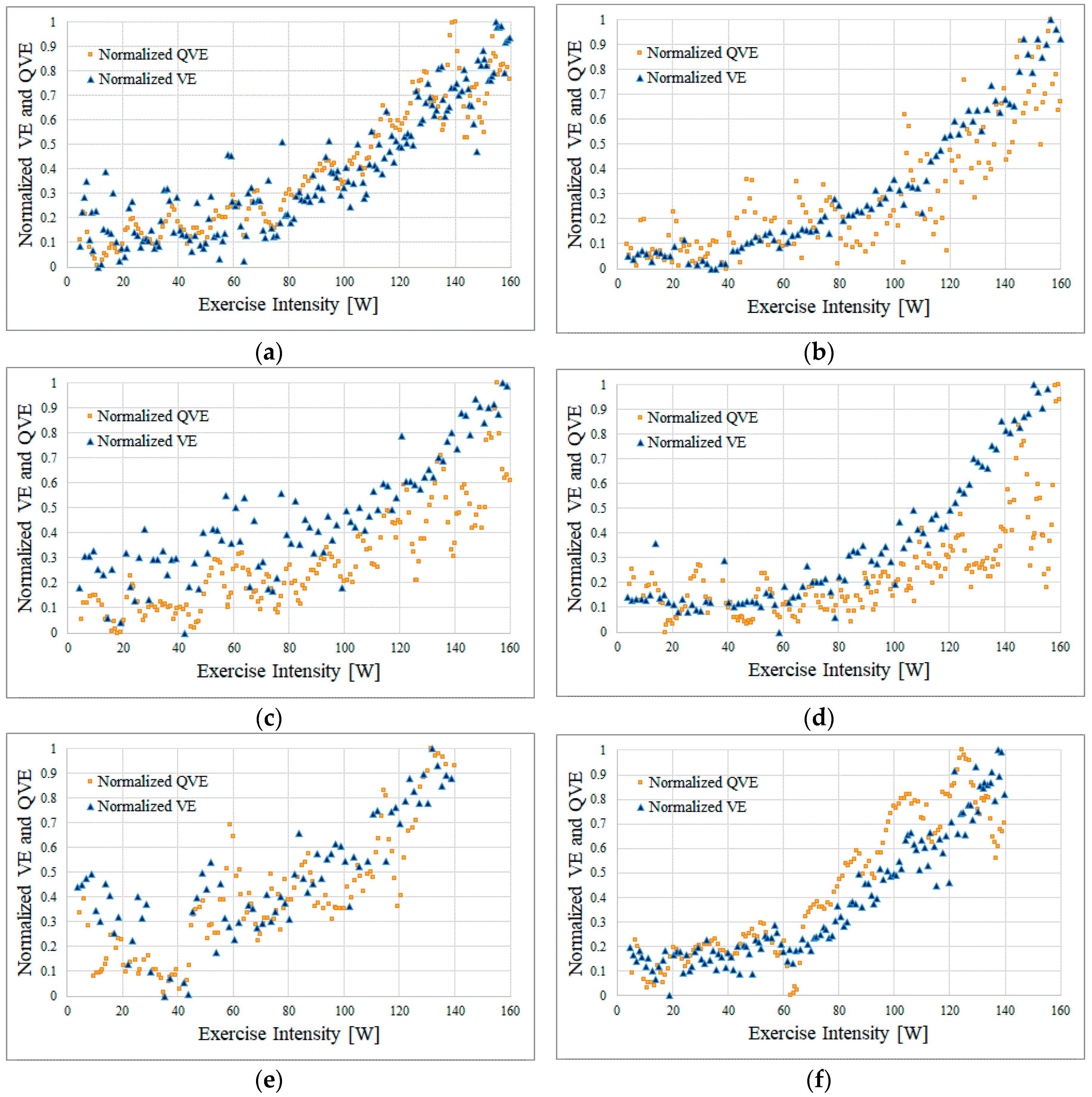
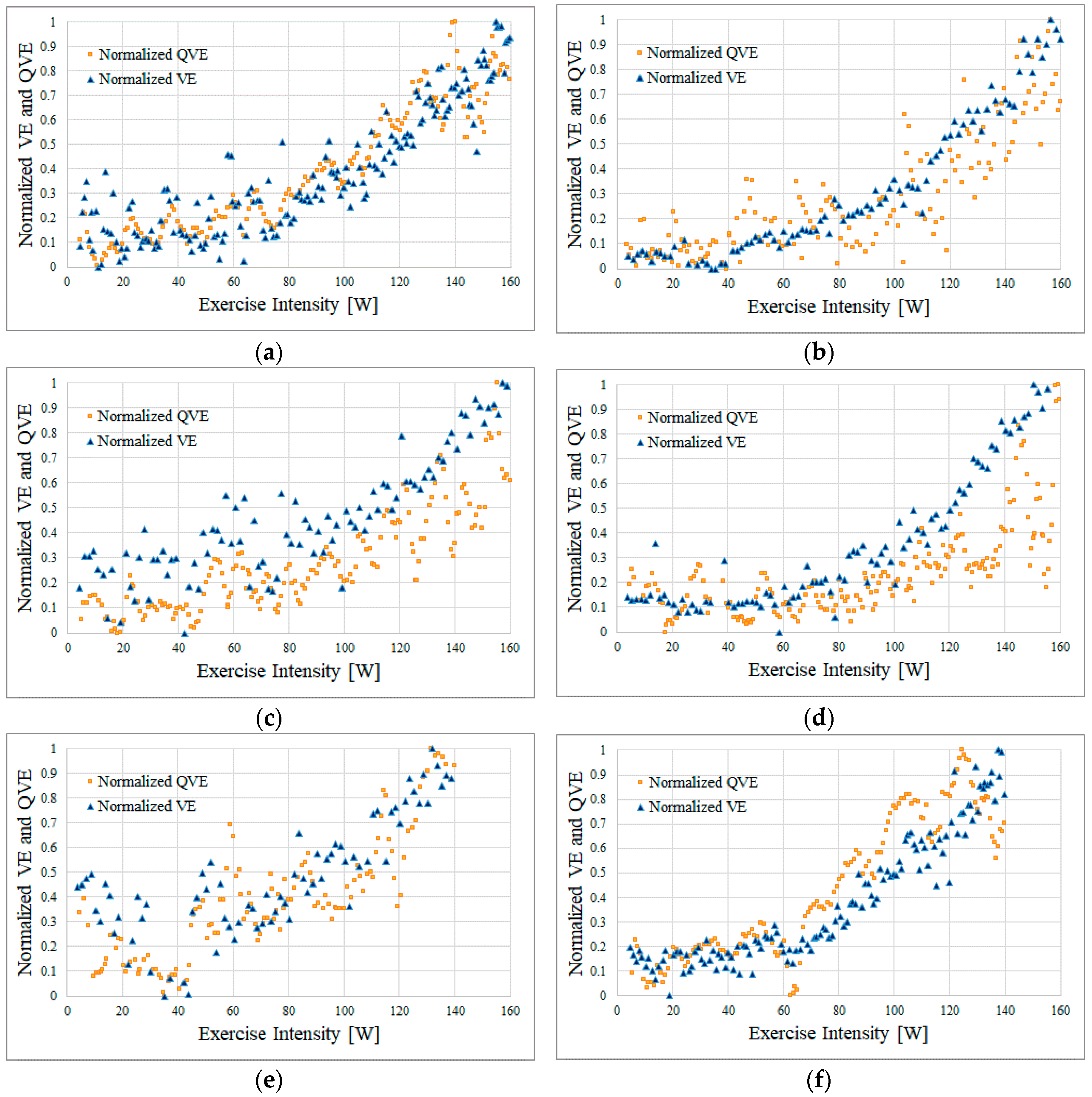
Figure 7 shows the results of the simultaneous measurement as follows: yellow squares, the QVE obtained by the proposed method; blue triangles, the VE obtained by the expiration gas analyzer; the horizontal axis, the normalized value of QVE/VE. With the minimum and the maximum as a standard, we calculated the normalized value so that the value changed from 0 to 1.
Among the six subjects, Subjects A, B, C, and D rode the bicycling ergometer up to an exercise intensity of 160 W. In contrast, Subjects E and F were unable to continue pedaling with the exercise intensity around 140 W because of fatigue and stopped exercising at 140 W.
In all results, compared to the VE, the QVE was highly variable (
Figure 7). However, we observed that the VE and QVE changed with a similar tendency in each subject.
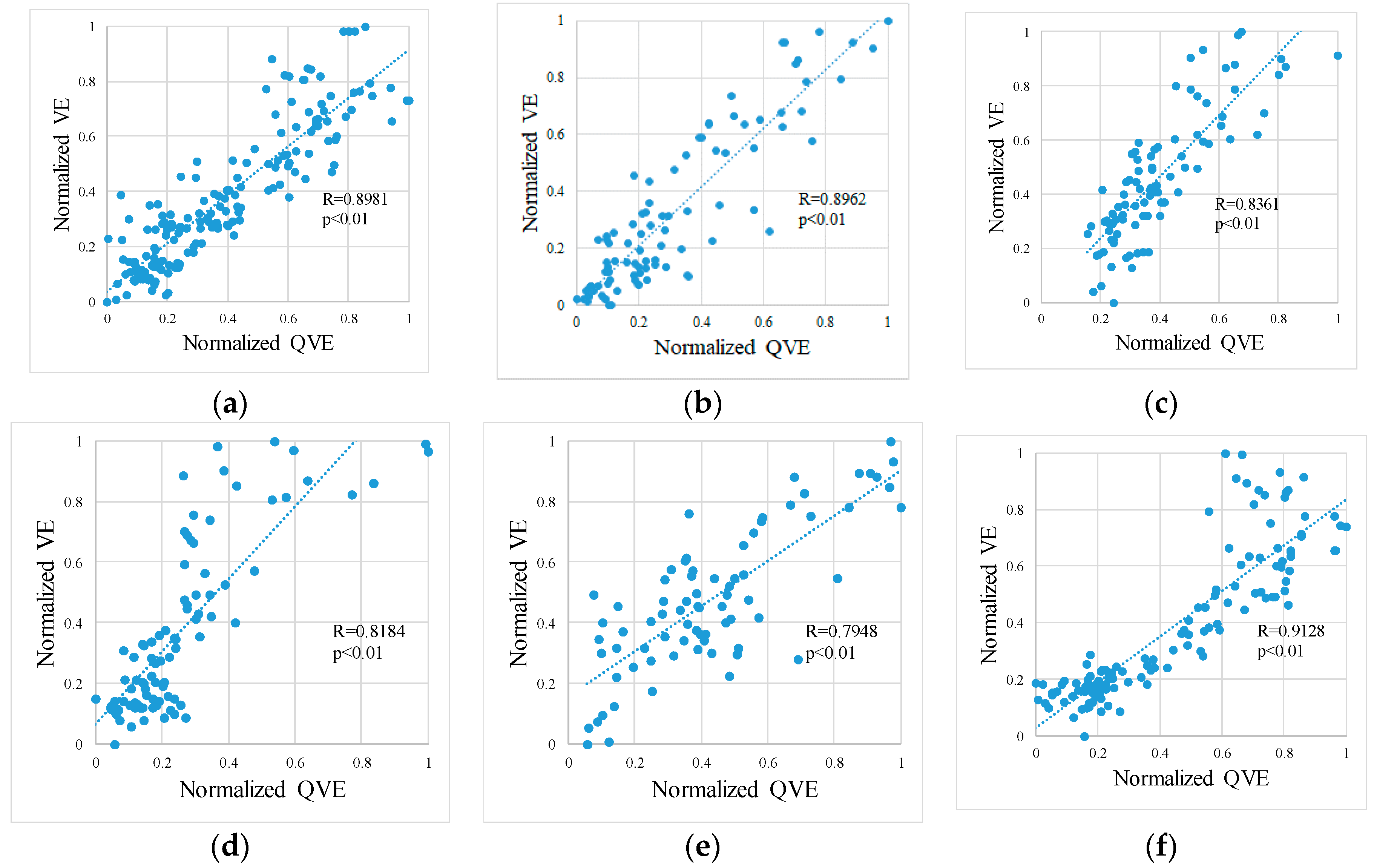
Figure 8 shows scatter diagrams of the VE and QVE. Furthermore, the linear regression analysis revealed that the correlation coefficient was ≥0.79 in any of our subjects. For each subject, the bias and the 95% confidence interval (95% CI) of the difference between VE and QVE as well as VT estimated by the expiration gas analyzer and QVT estimated by the method proposed in our previous works [
6] are shown in
Table 2.
4. Discussion
This study suggests that non-contact respiration measurement can be performed even during pedaling movements with an exercise intensity of 140–160 W per the proposed method. In the method proposed previously [
10], non-contact respiration measurement at an exercise intensity of ≥100 W was difficult; however, the proposed method in this study overcomes those limitations and proves its validity and usefulness.
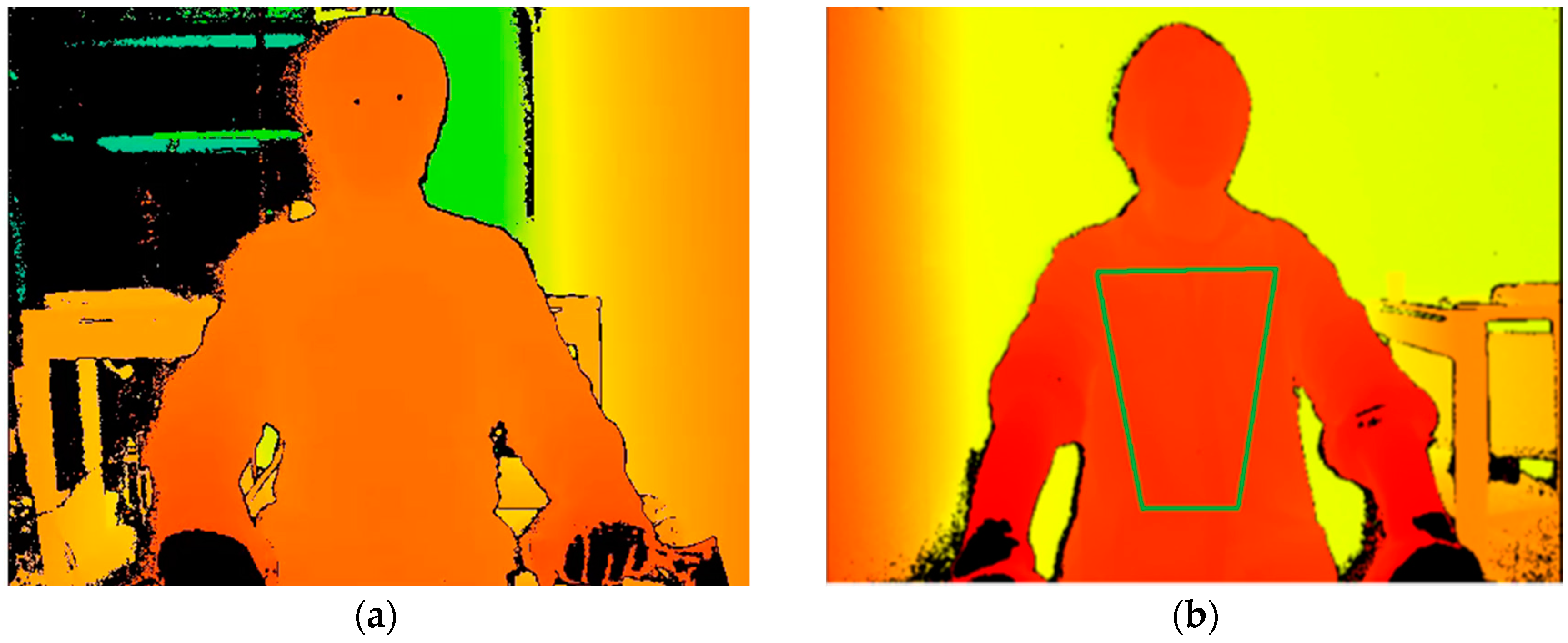
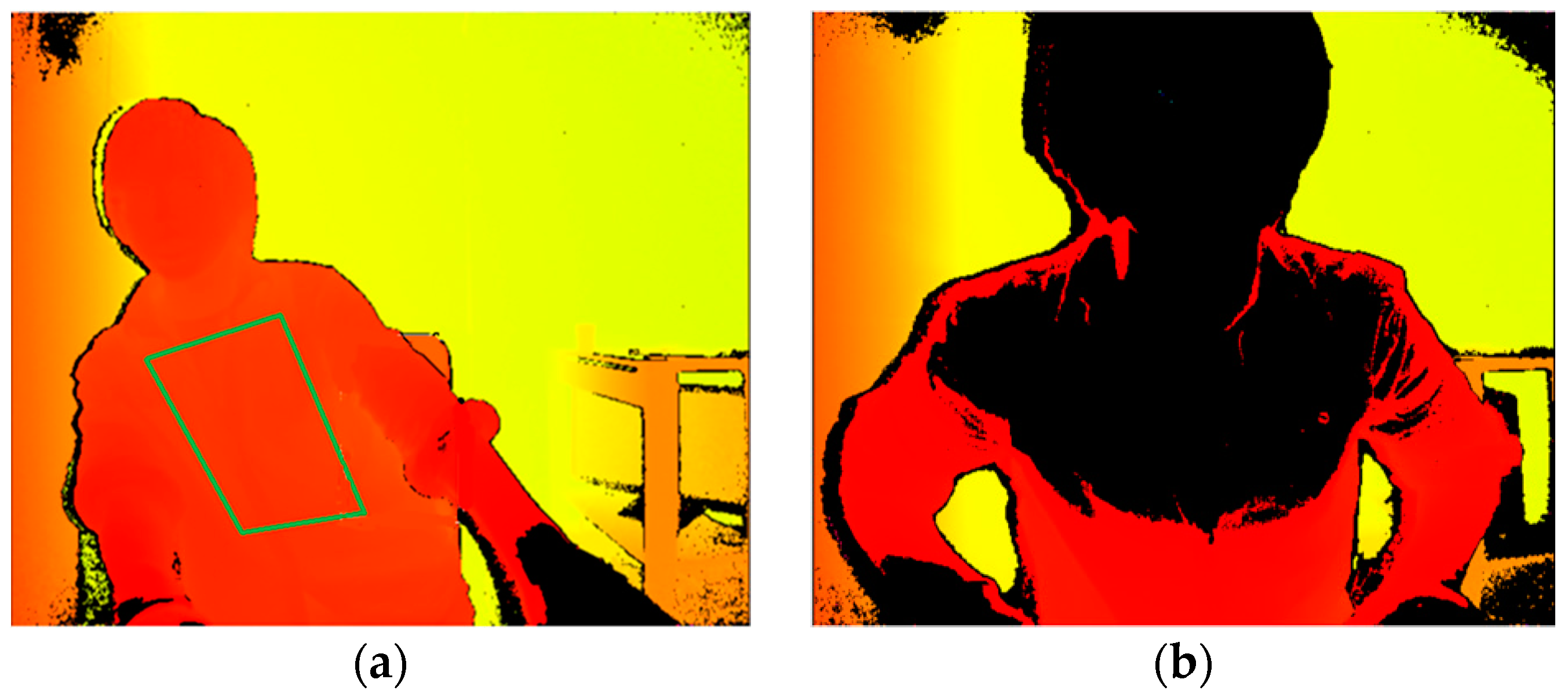
However, as the exercise intensity increased, we observed the tendency for the VE and QVE to diverge, which may warrant further investigation. For example, with Subject D, the VE and QVE started diverging at an exercise intensity of ≥120 W. At this time, Subject D was in a posture in which the left and right inclinations were significant (
Figure 9a). Although the ROI was correctly set at this time, the large left and right movements presumably hindered the detection of respiration, which is moving in the depth direction. In addition, the ROI could not be set correctly because the subject was too close to the sensor, which restricted the precise respiration measurement (
Figure 9b). This may be attributed to the fact that distance information is not measured because the upper body was set at a position closer than the lower limit (50 cm) of the sensing range of the Kinect v2. Thus, further study is necessary to elucidate the conditions at which the accuracy of non-contact respiration measurement deteriorates. As a countermeasure, two approaches are conceivable. The first approach is to set a longer distance between the subject and the sensor. Another approach is to place the backrest on the ergometer’s seat chair. When subjects pedal with their back in contact with the backrest, it is possible to prevent measurement from being impossible due to a forward-tilting posture.
The correlation coefficient between the VE and QVE in this study was ≥0.79 (
Figure 8). An investigation by optoelectronic plethysmography (OEP) is a well-known study on the correlation between the volume change in the chest and exhalation flow during exercise. Apparently, OEP is an application of motion capture using markers that enables strict volume measurement than markerless motion capture. A previous study on OEP revealed that the correlation coefficient with spirometer was >0.75, which corroborates our results [
14]. In our method, estimation of the thoracic region was not strict; however, we obtained a reasonable correlation by noise reduction processing.
In addition, a difference magnitude of ±10 W between the QVT estimated by the proposed method and the VT estimated by the expiratory gas analyzer suggests that the proposed method might allow VT calculation without contact in the lamp load test using a general upright bicycle ergometer. As shown in
Table 2, the difference between VE and QVE is rather large, but the trends of changes in VE and QVE are similar, as reflected by the correlation coefficient. Consequently, VT and QVT may show close values. In this experiment, because the distribution of the subjects’ VT was biased to approximately 100 W, additional tests are required for subjects with more diverse VT. However, the primary objective of this research was to construct a method to conveniently calculate the VT from an engineering perspective, which has been significantly attained in this study.
This study has some limitations. First, the sample size of this study is small, and all participants were males. Thus, it is necessary to conduct extensive studies targeting a variety of subjects from different age groups, genders, and athletic abilities. In addition, the structural and statistical examination is required for more subjects. From the perspective of motion analysis, a comparison by introducing OEP is considered to be effective for assessing the validity and reliability of the proposed method.
5. Conclusions
By tracking the thoracoabdominal region using the motion capture function of the Kinect v2 sensor, we proposed a non-contact respiration measurement during the exercise tolerance test corresponding to an increased body movement with increasing exercise intensity. In this study, we designed a digital filter for bandpass filter processing in real time. As a result of investigating the correlation between the QVE and the VE by simultaneous measurement using an expiration gas analyzer, a high correlation coefficient up to about 160 W of the exercise intensity was obtained. The study clarifies that posture during the pedaling motion affects the measurement accuracy of the proposed method. Nevertheless, elucidation of the condition that deteriorates the precise measurement warrants further study.
QVT estimated from QVE showed a difference of ±10 W from VT calculated by expiratory gas analyzer. In this experiment, the number of subjects, as well as difference in VT among these subjects, was small. Thus, the examination of the correlation between QVT and VT was impossible. Therefore, in this experiment, the feasibility of the proposed method could not be completely demonstrated. However, QVT estimated by the proposed method shows a value close to VT. In addition, our VT estimation method based on the knowledge of Caiozzeo shows a robust estimation accuracy in our previous research. Taken together, these results suggest that VT can be estimated by non-contact sensing for the unstable posture of the subject who pedals with an upright bicycle ergometer.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}