Awareness and Knowledge of the Physical Activity Guidelines and Their Association with Physical Activity Levels



Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Physical Activity Assessment
2.3. Awareness and Knowledge of PA Guidelines
2.4. Statistical Analysis
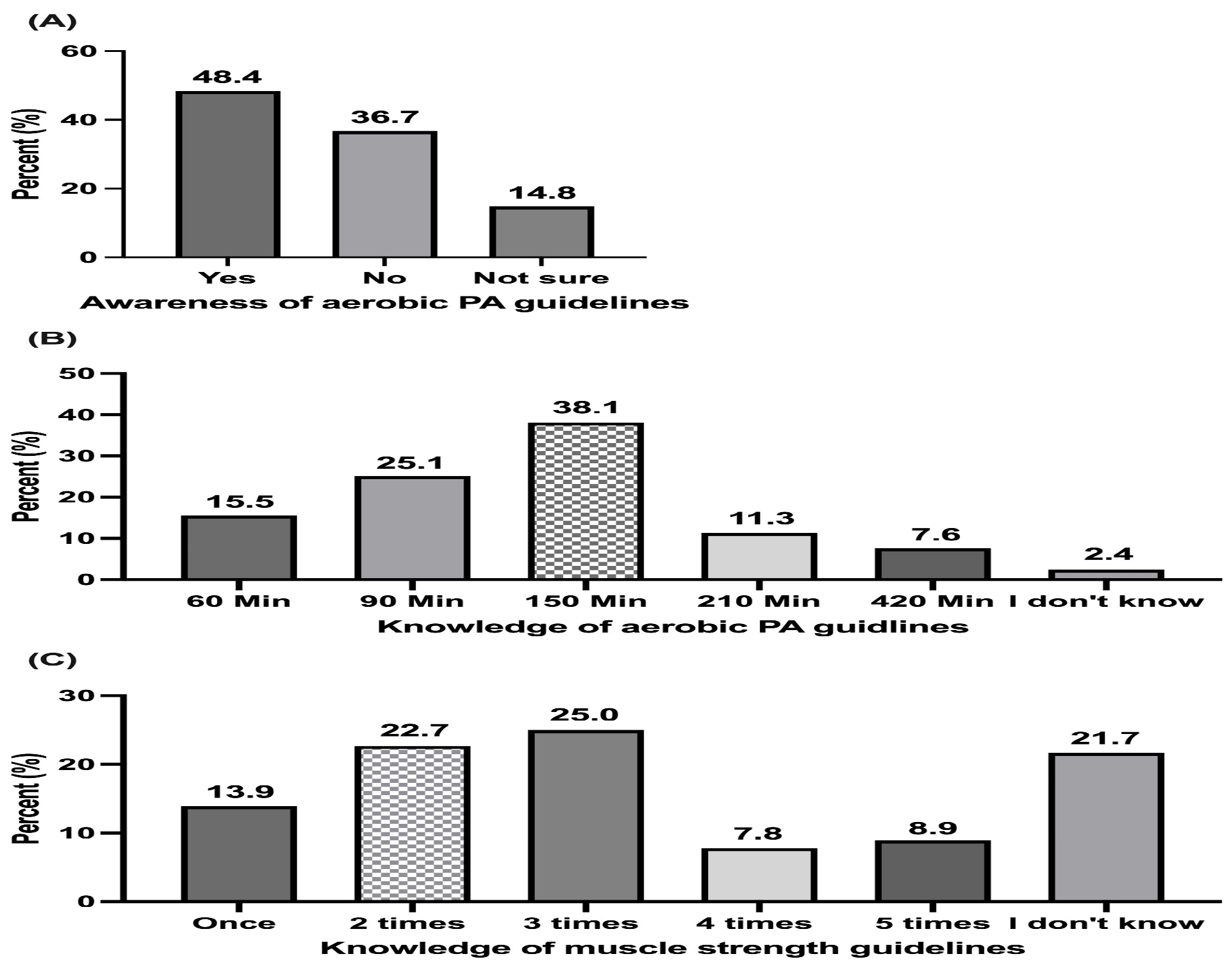
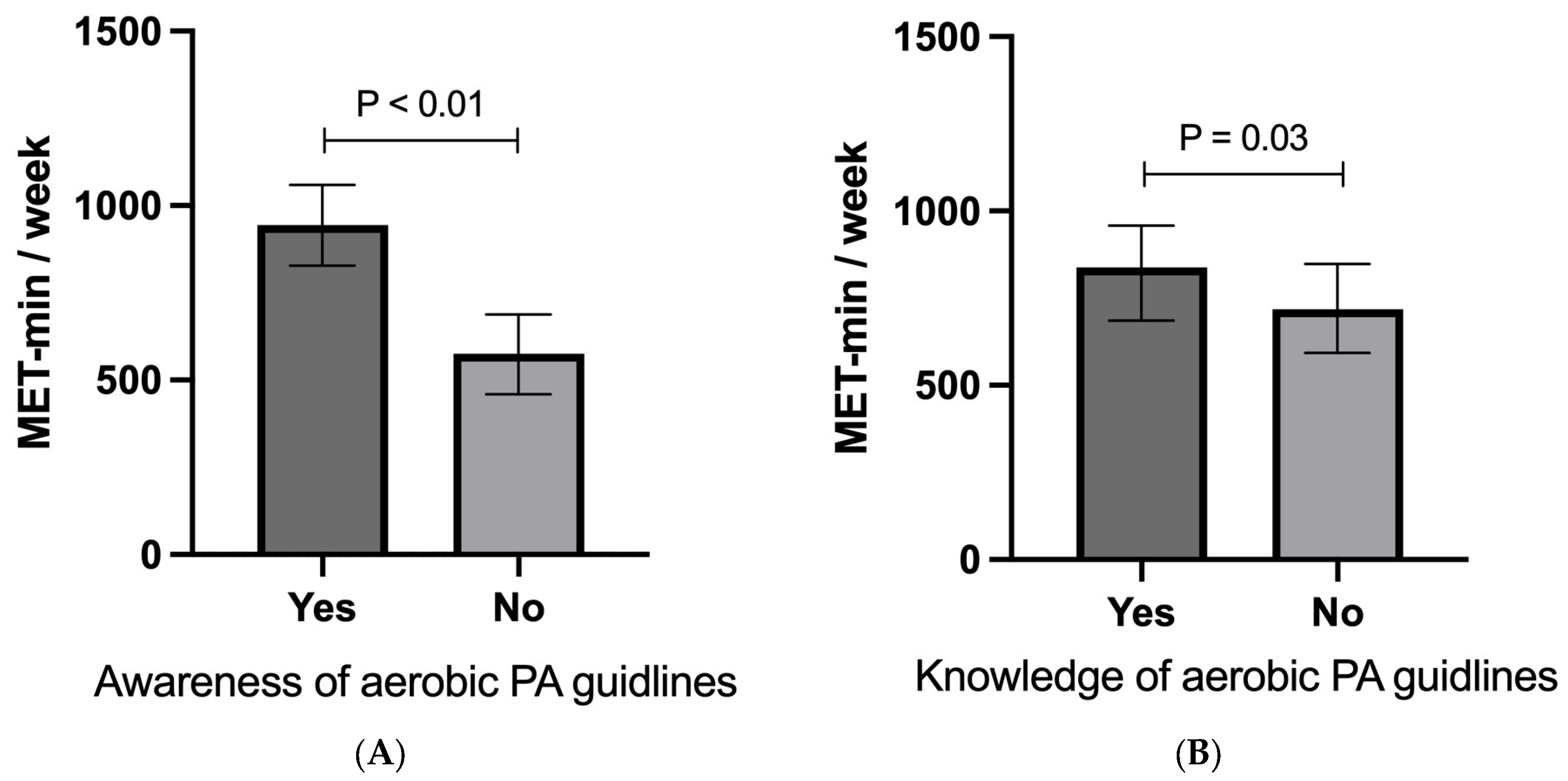
3. Results
Participants Characteristics
4. Discussion
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, G.F.; Balady, G.; Blair, S.N.; Blumenthal, J.; Caspersen, C.; Chaitman, B.; Epstein, S.; Froelicher, E.S.S.; Froelicher, V.F.; Pina, I.L.; et al. Statement on exercise: Benefits and recommendations for physical activity programs for all Americans. A statement for health professionals by the Committee on Exercise and Cardiac Rehabilitation of the Council on Clinical Cardiology, American Heart Association. Circulation 1996, 94, 857–862. [Google Scholar] [PubMed]
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S.; Lancet Physical Activity Series Working Group. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Services USDoHaH. Physical Activity Guidelines for Americans, 2nd ed. 2018. Available online: https://health.gov/our-work/nutrition-physical-activity/physical-activity-guidelines (accessed on 9 April 2024).
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Arabia MoHoS. Physical Activity Guidelines 2020. Available online: https://www.moh.gov.sa/Ministry/About/Health%20Policies/037.pdf (accessed on 9 April 2024).
- Evenson, K.R.; Alhusseini, N.; Moore, C.C.; Hamza, M.M.; Al-Qunaibet, A.; Rakic, S.; Alsukait, R.F.; Herbst, C.H.; AlAhmed, R.; Al-Hazzaa, H.M.; et al. Scoping Review of Population-Based Physical Activity and Sedentary Behavior in Saudi Arabia. J. Phys. Act. Health 2023, 20, 471–486. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Langlois, M.A.; Hallam, J.S. Integrating multiple health behavior theories into program planning: The PER worksheet. Health Promot. Pract. 2010, 11, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Tombor, I.; Michie, S. Methods of Health Behavior Change; Oxford Research Encyclopedias-Psychology: Oxford, UK, 2017. [Google Scholar]
- Plotnikoff, R.C.; Trinh, L. Protection Motivation Theory: Is This a Worthwhile Theory for Physical Activity Promotion? Exerc. Sport Sci. Rev. 2010, 38, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.G.; Wolin, K.Y.; Puleo, E.M.; Mâsse, L.C.; Atienza, A.A. Awareness of national physical activity recommendations for health promotion among US adults. Med. Sci. Sports Exerc. 2009, 41, 1849–1855. [Google Scholar] [CrossRef]
- Chen, T.J.; Whitfield, G.P.; Watson, K.B.; Fulton, J.E.; Ussery, E.N.; Hyde, E.T.; Rose, K. Awareness and Knowledge of the Physical Activity Guidelines for Americans, 2nd Edition. J. Phys. Act. Health 2023, 20, 742–751. [Google Scholar] [CrossRef]
- Vaara, J.P.; Vasankari, T.; Koski, H.J.; Kyröläinen, H. Awareness and Knowledge of Physical Activity Recommendations in Young Adult Men. Front. Public Health 2019, 7, 310. [Google Scholar] [CrossRef] [PubMed]
- Statistics GAO. Statistical Yearbook. 2019. Available online: https://www.stats.gov.sa/en/1006 (accessed on 9 April 2024).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Byrne, N.M.; Hills, A.P.; Hunter, G.R.; Weinsier, R.L.; Schutz, Y. Metabolic equivalent: One size does not fit all. J. Appl. Physiol. 2005, 99, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed]
- IR Committee. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)-Short and Long Forms. 2005. Available online: https://biobank.ndph.ox.ac.uk/showcase/ukb/docs/ipaq_analysis.pdf (accessed on 9 April 2024).
- Moore, L.V.; Fulton, J.; Kruger, J.; McDivitt, J. Knowledge of physical activity guidelines among adults in the United States, HealthStyles 2003−2005. J. Phys. Act. Health 2010, 7, 141–149. [Google Scholar] [CrossRef] [PubMed]
- AlMarzooqi, M.A.; Alsukait, R.F.; Aljuraiban, G.S.; Alothman, S.A.; AlAhmed, R.; Rakic, S.; Herbst, C.H.; Al-Hazzaa, H.M.; Alqahtani, S.A. Comprehensive assessment of physical activity policies and initiatives in Saudi Arabia 2016–2022. Front. Public Health 2023, 11, 1236287. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; AlMarzooqi, M.A. Descriptive Analysis of Physical Activity Initiatives for Health Promotion in Saudi Arabia. Front. Public Health 2018, 6, 329. [Google Scholar] [CrossRef] [PubMed]
- Knox, E.C.L.; Esliger, D.W.; Biddle, S.J.H.; Sherar, L.B. Lack of knowledge of physical activity guidelines: Can physical activity promotion campaigns do better? BMJ Open 2013, 3, e003633. [Google Scholar] [CrossRef] [PubMed]
- Cameron, C.; Craig, C.L.; Bull, F.C.; Bauman, A. Canada’s physical activity guides: Has their release had an impact? Can. J. Public Health 2007, 98 (Suppl. S2), S161–S169. [Google Scholar]
- Gore, D.; Kothari, A. Social determinants of health in Canada: Are healthy living initiatives there yet? A policy analysis. Int. J. Equity Health 2012, 11, 41. [Google Scholar] [CrossRef]
- Abula, K.; Gröpel, P.; Chen, K.; Beckmann, J. Does knowledge of physical activity recommendations increase physical activity among Chinese college students? Empirical investigations based on the transtheoretical model. J. Sport Health Sci. 2018, 7, 77–82. [Google Scholar] [CrossRef] [PubMed]
- McQueen, A.; Vernon, S.W.; Meissner, H.I.; Rakowski, W. Risk perceptions and worry about cancer: Does gender make a difference? J. Health Commun. 2008, 13, 56–79. [Google Scholar] [CrossRef] [PubMed]
- DiLorenzo, T.A.; Schnur, J.; Montgomery, G.H.; Erblich, J.; Winkel, G.; Bovbjerg, D.H. A model of disease-specific worry in heritable disease: The influence of family history, perceived risk and worry about other illnesses. J. Behav. Med. 2006, 29, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Robb, K.A.; Miles, A.; Wardle, J. Demographic and psychosocial factors associated with perceived risk for colorectal cancer. Cancer Epidemiol. Biomark. Prev. 2004, 13, 366–372. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Abahussain, N.A.; Al-Sobayel, H.I.; Qahwaji, D.M.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 140. [Google Scholar] [CrossRef] [PubMed]
- El Bcheraoui, C.; Tuffaha, M.; Daoud, F.; Kravitz, H.; Al Mazroa, M.A.; Al Saeedi, M.; Memish, Z.A.; Basulaiman, M.; Al Rabeeah, A.A.; Mokdad, A.H. On your mark, get set, go: Levels of physical activity in the Kingdom of Saudi Arabia, 2013. J. Phys. Act. Health 2016, 13, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Hyde, E.T.; Omura, J.D.; Watson, K.B.; Fulton, J.E.; Carlson, S.A. Knowledge of the Adult and Youth 2008 Physical Activity Guidelines for Americans. J. Phys. Act. Health 2019, 16, 618–622. [Google Scholar] [CrossRef]
- Piercy, K.L.; Bevington, F.; Vaux-Bjerke, A.; Hilfiker, S.W.; Arayasirikul, S.; Barnett, E.Y. Understanding Contemplators’ Knowledge and Awareness of the Physical Activity Guidelines. J. Phys. Act. Health 2020, 17, 404–411. [Google Scholar] [CrossRef]
- Park, J.-H.; Nam, S.-J.; Kim, J.-E.; Kim, N.-C. Application of the extended parallel process model and risk perception attitude framework to obesity knowledge and obesity prevention behaviors among Korean adults. BMC Public Health 2024, 24, 748. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | n | % | |
|---|---|---|---|
| Gender | |||
| Male | 469 | 46.1 | |
| Female | 549 | 53.9 | |
| Age | |||
| 17–34 | 631 | 62.0 | |
| 35–49 | 295 | 29.0 | |
| 50–64 | 92 | 9.0 | |
| BMI | |||
| Underweight | 91 | 8.9 | |
| Normal weight | 434 | 42.6 | |
| Overweight | 305 | 30.0 | |
| Obese | 188 | 18.5 | |
| Education | |||
| Bachelor’s degree and above | 559 | 54.9 | |
| Some college | 212 | 20.8 | |
| Secondary school and lower | 247 | 24.3 | |
| Marital status | |||
| Single | 580 | 57.0 | |
| Married | 401 | 39.4 | |
| Divorced/widowed | 37 | 3.6 | |
| Job | |||
| Employed | 413 | 40.6 | |
| Unemployed | 159 | 15.6 | |
| Student | 418 | 41.1 | |
| Retired | 28 | 2.8 | |
| Smoking | |||
| Smoker | 92 | 9.0 | |
| Non-smoker | 880 | 86.4 | |
| Ex-smoker | 46 | 4.5 | |
| Income (SAR) | |||
| ≤5000 | 554 | 54.4 | |
| 5000–9999 | 157 | 15.4 | |
| 10,000–14,999 | 130 | 12.8 | |
| 15,000–19,999 | 120 | 11.8 | |
| ≥20,000 | 57 | 5.6 | |
| Living environment | |||
| Urban | 776 | 76.2 | |
| Rural | 242 | 23.8 | |
| PA level | |||
| Low | 451 | 44.3 | |
| Moderate | 443 | 43.5 | |
| High | 124 | 12.2 |
| Characteristics | Awareness of PA Guidelines | Knowledge of Aerobic PA Guidelines | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes n = 493 (48.4%) | No n = 525 (51.6%) | ES | p | Yes n = 388 (38.1) | No n = 630 (61.9) | ES | p | ||||||
| n | % | n | % | n | % | n | % | ||||||
| Gender | Male | 195 | 41.6 | 274 | 58.4 | 0.13 | <0.01 | 196 | 41.8 | 273 | 58.2 | 0.07 | 0.02 |
| Female | 298 | 54.3 | 251 | 45.7 | 192 | 35.0 | 357 | 65.0 | |||||
| Age | 17–34 | 290 | 46.0 | 341 | 54.0 | 0.074 | 0.06 | 257 | 40.7 | 374 | 59.3 | 0.08 | 0.04 |
| 35–49 | 160 | 54.2 | 135 | 45.8 | 105 | 35.6 | 190 | 64.4 | |||||
| 50–64 | 43 | 46.7 | 49 | 53.3 | 26 | 28.3 | 66 | 71.7 | |||||
| BMI | Underweight | 41 | 45.1 | 50 | 54.9 | 0.11 | 0.01 | 33 | 36.3 | 58 | 63.7 | 0.07 | 0.21 |
| Normal weight | 197 | 45.4 | 237 | 54.6 | 164 | 37.8 | 270 | 62.2 | |||||
| Overweight | 172 | 56.4 | 133 | 43.6 | 129 | 42.3 | 176 | 57.7 | |||||
| Obese | 83 | 44.1 | 105 | 55.9 | 62 | 33.0 | 126 | 67.0 | |||||
| Education | Bachelor’s degree and above | 261 | 46.7 | 298 | 53.3 | 0.06 | 0.19 | 207 | 37.0 | 352 | 63.0 | 0.04 | 0.51 |
| Some college | 100 | 47.2 | 112 | 52.8 | 88 | 41.5 | 124 | 58.5 | |||||
| Secondary school and lower | 111 | 51.4 | 105 | 48.6 | 93 | 37.7 | 154 | 62.3 | |||||
| Marital status | Single | 264 | 45.5 | 316 | 54.5 | 0.07 | 0.10 | 239 | 41.2 | 341 | 58.8 | 0.07 | 0.06 |
| Married | 210 | 52.4 | 191 | 47.6 | 136 | 33.9 | 265 | 66.1 | |||||
| Divorced/widowed | 19 | 51.4 | 18 | 48.6 | 13 | 35.1 | 24 | 64.9 | |||||
| Job | Employed | 210 | 50.8 | 203 | 49.2 | 0.09 | 0.03 | 148 | 35.8 | 265 | 64.2 | 0.08 | 0.09 |
| Unemployed | 88 | 55.3 | 71 | 44.7 | 52 | 32.7 | 107 | 67.3 | |||||
| Student | 185 | 44.3 | 233 | 55.7 | 178 | 42.6 | 240 | 57.4 | |||||
| Retired | 10 | 35.7 | 18 | 64.3 | 10 | 35.7 | 18 | 64.3 | |||||
| Smoking | Smoker | 32 | 34.8 | 60 | 65.2 | 0.09 | 0.02 | 33 | 35.9 | 59 | 64.1 | 0.02 | 0.88 |
| Non-smoker | 439 | 49.9 | 441 | 50.1 | 338 | 38.4 | 542 | 61.6 | |||||
| X-smoker | 22 | 47.8 | 24 | 52.2 | 17 | 37.0 | 29 | 63.0 | |||||
| Income (SAR) | ≤5000 | 262 | 47.3 | 292 | 52.7 | 0.05 | 0.58 | 219 | 39.5 | 335 | 60.5 | 0.09 | 0.05 |
| 5000–9999 | 71 | 45.2 | 86 | 54.8 | 51 | 32.5 | 106 | 67.5 | |||||
| 10,000–14,999 | 68 | 52.3 | 62 | 47.7 | 49 | 37.7 | 81 | 62.3 | |||||
| 15,000–19,999 | 64 | 53.3 | 56 | 46.7 | 39 | 32.5 | 81 | 67.5 | |||||
| ≥20,000 | 28 | 49.1 | 29 | 50.9 | 30 | 52.6 | 27 | 47.4 | |||||
| Living environment | Urban | 381 | 49.1 | 395 | 50.9 | 0.02 | 0.44 | 299 | 38.5 | 477 | 61.5 | 0.02 | 0.60 |
| Rural | 112 | 46.3 | 130 | 53.7 | 89 | 36.8 | 153 | 63.2 | |||||
| PA level | Low | 182 | 40.4 | 269 | 59.6 | 0.15 | <0.01 | 160 | 35.5 | 291 | 64.5 | 0.07 | 0.04 |
| Moderate | 246 | 55.5 | 197 | 44.5 | 169 | 38.1 | 274 | 61.9 | |||||
| High | 65 | 52.4 | 59 | 46.6 | 59 | 47.6 | 65 | 52.4 | |||||
| Knowledge (Resistance) | Yes | 123 | 53.2 | 108 | 46.8 | 0.05 | 0.09 | 85 | 36.8 | 146 | 63.2 | 0.02 | 0.64 |
| No | 370 | 47.0 | 417 | 53.0 | 303 | 38.5 | 484 | 76.8 | |||||
| Knowledge (Aerobic) | Yes | 206 | 53.1 | 182 | 46.9 | 0.07 | 0.02 | ||||||
| No | 287 | 45.6 | 343 | 54.4 | |||||||||
| Meet PA Guidelines | ||
|---|---|---|
| Variable | aOR (95% CI) | |
| Gender | ||
| Male | Referent | |
| Female | 0.54 (0.40–0.74) | |
| Age | ||
| 17–34 | Referent | |
| 35–49 | 0.67 (0.42–1.05) | |
| 50–64 | 0.59 (0.30–1.15) | |
| BMI | ||
| Underweight | 1.13 (0.64–1.99) | |
| Normal weight | 0.95 (0.65–1.34) | |
| Overweight | 1.15 (0.78–1.70) | |
| Obese | Referent | |
| Education | ||
| Bachelor’s degree and above | 1.22 (0.88–1.71) | |
| In progress of completing bachelor’s degree but did not complete | 0.78 (0.52–1.17) | |
| Secondary school | 0.83 (0.36–1.88) | |
| Lower than secondary school | Referent | |
| Marital status | ||
| Single | Referent | |
| Married | 1.13 (0.73–1.75) | |
| Divorced/widowed | 1.44 (0.67–3.14) | |
| Job | ||
| Employed | Referent | |
| Unemployed | 0.96 (0.60–1.54) | |
| Student | 1.01 (0.67–1.67) | |
| Retired | 1.76 (0.71–4.41) | |
| Smoking | ||
| Smoker | Referent | |
| Non-smoker | 0.91 (0.56–1.47) | |
| X-smoker | 2.43 (1.04–5.67) | |
| Income (SAR) | ||
| ≤5000 | Referent | |
| 5000–9999 | 0.77 (0.50–1.18) | |
| 10,000–14,999 | 0.85 (0.50–1.43) | |
| 15,000–19,999 | 0.67 (0.39–1.15) | |
| ≥20,000 | 0.52 (0.28–0.95) | |
| Living environment | ||
| Urban | Referent | |
| Rural | 0.72 (0.53–0.99) | |
| Awareness of PA guidelines | ||
| Yes | 2.03 (1.55–2.65) | |
| No | Referent | |
| Knowledge of aerobic PA guidelines | Yes | 1.11 (0.85–1.45) |
| No | Referent | |
| Knowledge of muscle strength PA guidelines | Yes | 1.32 (0.95–1.79) |
| No | Referent |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wafi, A.M.; Wadani, S.N.; Daghriri, Y.Y.; Alamri, A.I.; Zangoti, A.M.; Khiswi, A.A.; Al-Ebrahim, E.Y.; Jesudoss, H.J.; Alharbi, A.A. Awareness and Knowledge of the Physical Activity Guidelines and Their Association with Physical Activity Levels. Sports 2024, 12, 174. https://doi.org/10.3390/sports12070174
Wafi AM, Wadani SN, Daghriri YY, Alamri AI, Zangoti AM, Khiswi AA, Al-Ebrahim EY, Jesudoss HJ, Alharbi AA. Awareness and Knowledge of the Physical Activity Guidelines and Their Association with Physical Activity Levels. Sports. 2024; 12(7):174. https://doi.org/10.3390/sports12070174
Chicago/Turabian StyleWafi, Ahmed M., Saud N. Wadani, Yazan Y. Daghriri, Ali I. Alamri, Abdulrahim M. Zangoti, Ayman A. Khiswi, Elyas Y. Al-Ebrahim, Hemachandran J. Jesudoss, and Abdullah A. Alharbi. 2024. "Awareness and Knowledge of the Physical Activity Guidelines and Their Association with Physical Activity Levels" Sports 12, no. 7: 174. https://doi.org/10.3390/sports12070174
APA StyleWafi, A. M., Wadani, S. N., Daghriri, Y. Y., Alamri, A. I., Zangoti, A. M., Khiswi, A. A., Al-Ebrahim, E. Y., Jesudoss, H. J., & Alharbi, A. A. (2024). Awareness and Knowledge of the Physical Activity Guidelines and Their Association with Physical Activity Levels. Sports, 12(7), 174. https://doi.org/10.3390/sports12070174