

The Prevalence of “at Risk” Eating Disorders among Athletes in Jordan

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neumark-Sztainer, D.; Levine, M.P.; Paxton, S.; Smolak, L.; Piran, N.; Wertheim, E. Prevention of Body Dissatisfaction and Disordered Eating: What Next? Eat. Disord. 2006, 14, 265–285. [Google Scholar] [CrossRef] [PubMed]
- Rukavishnikov, G.V.; Verbitskaya, E.V.; Vekovischeva, O.Y.; Bobrovsky, A.V.; Kibitov, A.O.; Mazo, G.E. The association of obesity with eating disorders risk: Online survey of a large cohort of Russian-speaking individuals seeking medical weight correction assistance. J. Eat. Disord. 2021, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- Alvero-Cruz, J.R.; Mathias, V.P.; García-Romero, J.C. Somatotype components as useful predictors of disordered eating attitudes in young female ballet dance students. J. Clin. Med. 2020, 9, 2024. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; García-Hermoso, A.; Smith, L.; Trott, M.; López-Bueno, R.; Gutiérrez-Espinoza, H.; Mesas, A.E.; Tárraga-López, P.J. Physical fitness and disordered eating among adolescents: Results from the EHDLA study. Appetite 2022, 178, 106272. [Google Scholar] [CrossRef]
- Koushiou, M.; Nikolaou, P.; Karekla, M. Prevalence and correlates of eating disorders in greek-cypriot adolescents and young adults. Eur. J. Couns. Psychol. 2020, 8, 3–18. [Google Scholar] [CrossRef]
- Nichols, J.F.; Rauh, M.J.; Barrack, M.T.; Barkai, H.-S.; Pernick, Y. Disordered Eating and Menstrual Irregularity in High School Athletes in Lean-Build and Nonlean-Build Sports. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 364–377. [Google Scholar] [CrossRef]
- Mancine, R.P.; Gusfa, D.W.; Moshrefi, A.; Kennedy, S.F. Prevalence of disordered eating in athletes categorized by emphasis on leanness and activity type—A systematic review. J. Eat. Disord. 2020, 8, 47. [Google Scholar] [CrossRef]
- Sharps, F.R.; Wilson, L.J.; Graham, C.A.; Curtis, C. Prevalence of Disordered Eating, Eating Disorders and Risk of Low Energy Availability in Professional, Competitive and Recreational Female Athletes Based in the United Kingdom. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34121611/ (accessed on 1 August 2022).
- Eichstadt, M.; Luzier, J.; Cho, D.; Weisenmuller, C. Eating Disorders in Male Athletes. Sports Health A Multidiscip. Approach 2020, 12, 327–333. [Google Scholar] [CrossRef]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef]
- Walter, N.; Heinen, T.; Elbe, A.M. Factors Associated with Disordered Eating and Eating Disorder Symptoms in Adolescent Elite Athletes. Available online: https://econtent.hogrefe.com/doi/pdf/10.1024/2674-0052/a000012 (accessed on 1 August 2022).
- Arvinder-Singh, H.S.; Azhar Shah, S.; Safian, N. Eating Disorder Screening Tools for Athletes: A Systematic Review of Literature Focusing on Scales Developed in the Last 10 Years (2011–2021). 2022. Available online: https://www.tandfonline.com/action/journalInformation?journalCode=yssa20 (accessed on 1 August 2022).
- Bould, H.; De Stavola, B.; Lewis, G.; Micali, N. Do disordered eating behaviours in girls vary by school characteristics? A UK cohort study. Eur. Child Adolesc. Psychiatry 2018, 27, 1473–1481. [Google Scholar] [CrossRef]
- Orbitello, B.; Ciano, R.; Corsaro, M.; Rocco, P.L.; Taboga, C.; Tonutti, L.; Armellini, M.; Balestrieri, M. The EAT-26 as screening instrument for clinical nutrition unit attenders. Int. J. Obes. 2006, 30, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M.; Bennett, S.; Olmsted, M.P.; Lawson, M.L.; Rodin, G. Disordered eating attitudes and behaviours in teenaged girls: A school-based study. CMAJ 2001, 165, 547–552. [Google Scholar] [PubMed]
- Asl, E.M.; Mahaki, B.; Bardezard, Y.A.; Mohammadian, Y. Eating Disorders Screening Tools: The Psychometric Properties of the Persian Version of Eating Attitude Test. 2020. Available online: www.ijpvmjournal.net/www.ijpm.ir (accessed on 1 August 2022).
- Garner, D.M.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Papini, N.M.; Jung, M.; Cook, A.; Lopez, N.V.; Ptomey, L.T.; Herrmann, S.D.; Kang, M. Psychometric properties of the 26-item eating attitudes test (EAT-26): An application of rasch analysis. J. Eat. Disord. 2022, 10, 62. [Google Scholar] [CrossRef] [PubMed]
- Gorini, A.; Griez, E.; Petrova, A.; Riva, G. Open Access Primary Research. Ann. Gen. Psychiatr. 2010, 9. Available online: http://www.annals-general-psychiatry.com/content/9/1/30 (accessed on 1 August 2022).
- Khaled, S.M.; Kimmel, L.; Le Trung, K. Assessing the factor structure and measurement invariance of the eating attitude test (EAT-26) across language and BMI in young Arab women. J. Eat. Disord. 2018, 6, 14. [Google Scholar] [CrossRef]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. Available online: http://bjsm.bmj.com/ (accessed on 1 August 2022). [CrossRef]
- Mann, A.H.; Wakeling, A.; Wood, K.; Monck, E.; Dobbs, R.; Szmukler, G. Screening for abnormal eating attitudes and psychiatric morbidity in an unselected population of 15-year-old schoolgirls. Psychol. Med. 1983, 13, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Alhaj, O.A.; Fekih-Romdhane, F.; Sweidan, D.H.; Saif, Z.; Khudhair, M.F.; Ghazzawi, H.; Nadar, M.S.; Alhajeri, S.S.; Levine, M.P.; Jahrami, H. The prevalence and risk factors of screen-based disordered eating among university students: A global systematic review, meta-analysis, and meta-regression. Eat. Weight Disord.—Stud. Anorexia Bulim. Obes. 2022. Available online: https://link.springer.com/10.1007/s40519-022-01452-0 (accessed on 1 August 2022).
- Fekih-Romdhane, F.; Daher-Nashif, S.; Alhuwailah, A.H.; Al Gahtani, H.M.S.; Hubail, S.A.; Shuwiekh, H.A.M.; Khudhair, M.F.; Alhaj, O.A.; Bragazzi, N.L.; Jahrami, H. The prevalence of feeding and eating disorders symptomology in medical students: An updated systematic review, meta-analysis, and meta-regression. Eat. Weight Disord.—Stud. Anorexia Bulim. Obes. 2022, 27, 1991–2010. [Google Scholar] [CrossRef] [PubMed]
- Al-Adawi, S.; Dorvlo, A.S.S.; Burke, D.T.; Moosa, S.; Al-Bahlani, S. A survey of anorexia nervosa using the Arabic version of the EAT-26 and “gold standard” interviews among Omani adolescents. Eat. Weight. Disord. 2002, 7, 304–311. [Google Scholar] [CrossRef]
- Lassale, C.; Péneau, S.; Touvier, M.; Julia, C.; Galan, P.; Hercberg, S.; Kesse-Guyot, E. Validity of Web-Based Self-Reported Weight and Height: Results of the Nutrinet-Santé Study. J. Med. Internet Res. 2013, 15, e152. [Google Scholar] [CrossRef] [PubMed]
- de Rubeis, V.; Bayat, S.; Griffith, L.E.; Smith, B.T.; Anderson, L.N. Validity of self-reported recall of anthropometric measures in early life: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1426–1440. [Google Scholar] [CrossRef] [PubMed]
- Jan, A.; Weir, C.B. BMI Classification Percentile and Cut Off Points; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Bendavid, I.; Lobo, D.N.; Barazzoni, R.; Cederholm, T.; Coëffier, M.; de van der Schueren, M.; Fontaine, E.; Hiesmayr, M.; Laviano, A.; Pichard, C.; et al. The centenary of the Harris–Benedict equations: How to assess energy requirements best? Recommendations from the ESPEN expert group. Clin. Nutr. 2020, 40, 690–701. [Google Scholar] [CrossRef] [PubMed]
- Luy, S.C.; Center, Q.C.S.L.M.; Dampil, O.A. Comparison of the Harris-Benedict Equation, Bioelectrical Impedance Analysis, and Indirect Calorimetry for Measurement of Basal Metabolic Rate among Adult Obese Filipino Patients with Prediabetes or Type 2 Diabetes Mellitus. J. ASEAN Fed. Endocr. Soc. 2018, 33, 152–159. [Google Scholar] [CrossRef] [PubMed]
- López, E.R.; Hernández, D.P.; López, N.L.; Serna-Gutiérrez, A.; Calderón-Ramos, Z.; Omaña-Covarrubias, A.; Flores-Guillen, E.; Tijerina-Sáenz, A. Comparison of perceived weight as ideal against ideal body weight formulas and body mass index of 22 kg/m2 in young adult women. Rev. Salud Públ. Y Nutr. 2018, 17, 7–15. [Google Scholar]
- Alejandro, W.S.; Ortega Sofia, V.; Pablo, W.A. Validation of the Broca index as the most practical method to calculate the ideal body weight. J. Clin. Investig. Stud. 2018, 1, 1–4. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L.; Moreno, S.G. Assessing publication bias in meta-analyses in the presence of between-study heterogeneity. J. R. Statist. Soc. A 2010, 173, 575–591. [Google Scholar] [CrossRef]
- Verbraecken, J.; van de Heyning, P.; de Backer, W.; van Gaal, L. Body surface area in normal-weight, overweight, and obese adults. A comparison study. Metabolism 2006, 55, 515–524. [Google Scholar] [CrossRef]
- Borgelt, S.; Burmeister, J.M. Disordered eating in collegiate English equestrian athletes in aesthetic and nonaesthetic disciplines. Eat Behav. 2022, 46, 101661. [Google Scholar] [CrossRef]
- Gusfa, D.; Mancine, R.; Do, S.K.; Bashir, D.A.; Do, M.S. The relationship between disordered eating behaviors and injury rates in adolescent athletes. Int. J. Eat. Disord. 2021, 55, 131–134. Available online: https://onlinelibrary.wiley.com/doi/10.1002/eat.23642 (accessed on 1 February 2022). [CrossRef]
- Martinez-Rodriguez, A. Efectos de la dieta y práctica de deportes aeróbicos o anaeróbicos sobre los trastornos del comportamiento alimentario. Nutr. Hosp. 2015, 31, 1240–1245. [Google Scholar]
- Thein-Nissenbaum, J.M.; Carr, K.E.; Hetzel, S.; Dennison, E. Disordered Eating, Menstrual Irregularity, and Musculoskeletal Injury in High School Athletes: A Comparison of Oral Contraceptive Pill Users and Nonusers. Sports Health 2014, 6, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Rousselet, M.; Guérineau, B.; Paruit, M.C.; Guinot, M.; Lise, S.; Destrube, B.; Ruffio-Thery, S.; Dominguez, N.; Brisseau-Gimenez, S.; Dubois, V.; et al. Disordered eating in French high-level athletes: Association with type of sport, doping behavior, and psychological features. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2017, 22, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Al-Jumayan, A.A.; Al-Eid, N.A.; AlShamlan, N.A.; AlOmar, R.S. Prevalence and associated factors of eating disorders in patrons of sport centers in Saudi Arabia. J. Fam. Commun. Med. 2021, 28, 94–102. [Google Scholar]
- Ravi, S.; Ihalainen, J.K.; Taipale-Mikkonen, R.S.; Kujala, U.M.; Waller, B.; Mierlahti, L.; Lehto, J.; Valtonen, M. Self-Reported Restrictive Eating, Eating Disorders, Menstrual Dysfunction, and Injuries in Athletes Competing at Different Levels and Sports. Nutrients 2021, 13, 3275. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, M.N.; Dundar, C. The relationship between orthorexia nervosa, anxiety, and self-esteem: A cross-sectional study in Turkish faculty members. BMC Psychol. 2022, 10, 82. [Google Scholar] [CrossRef] [PubMed]
- Rosendahl, J.; Bormann, B.; Aschenbrenner, K.; Strauss, B. Dieting and disordered eating in German high school athletes and non-athletes. Scand. J. Med. Sci. Sports 2009, 19, 731–739. [Google Scholar] [CrossRef]
- Kong, P.; Harris, L.M. The Sporting Body: Body Image and Eating Disorder Symptomatology Among Female Athletes from Leanness Focused and Nonleanness Focused Sports. J. Psychol. 2015, 149, 141–160. Available online: https://www.tandfonline.com/action/journalInformation?journalCode=vjrl20 (accessed on 12 June 2022). [CrossRef]
- Kampouri, D.; Kotopoulea-Nikolaidi, M.; Daskou, S.; Giannopoulou, I. European Journal of Sport Science Prevalence of Disordered Eating in Elite Female Athletes in Team Sports in Greece. 2019. Available online: https://pubmed.ncbi.nlm.nih.gov/25511202/ (accessed on 15 June 2022).
- Chatterton, J.M.; Petrie, T.A. Eating Disorders the Journal of Treatment & Prevention Prevalence of Disordered Eating and Pathogenic Weight Control Behaviors Among Male Collegiate Athletes. 2013. Available online: https://www.tandfonline.com/action/journalInformation?journalCode=uedi20 (accessed on 1 August 2022).
- Karrer, Y.; Halioua, R.; Mötteli, S.; Iff, S.; Seifritz, E.; Jäger, M.; Claussen, M.C. Disordered eating and eating disorders in male elite athletes: A scoping review. BMJ Open Sport Exerc. Med. 2020, 6, e000801. [Google Scholar] [CrossRef]
- Witkowski, K.; Superson, M.; Cde, P. Body composition and motor potential of judo athletes in selected weight categories. Arch. BUDO 2021, 17, 161–175. Available online: https://www.archbudo.com (accessed on 15 June 2022).
- Martinsen, M.; Sundgot-Borgen, J. Higher prevalence of eating disorders among adolescent elite athletes than controls. Med. Sci. Sports Exerc. 2013, 45, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Galli, N.; Petrie, T.A.; Reel, J.J.; Chatterton, J.M.; Baghurst, T.M. Assessing the validity of the Weight Pressures in Sport Scale for Male Athletes. Psychol. Men Masc. 2014, 15, 170–180. [Google Scholar] [CrossRef]
- Pustivšek, S.; Hadic, V.; Derviševic, E. O-26 Comparison of prevalence of risk for eating disorders and body composition among adolescent athletes and non-athletes: Abstract O-26 Table 1. Br. J. Sports Med. 2016, 50 (Suppl. 1), A15. [Google Scholar] [CrossRef]
- Spivak-Lavi, Z.; Peleg, O.; Tzischinsky, O.; Stein, D.; Latzer, Y. Differences in the Factor Structure of the Eating Attitude Test-26 (EAT-26) in Different Cultures in Israel: Jews, Muslims, and Christians. Nutrients 2021, 13, 1899. [Google Scholar] [CrossRef]


{kind=link}
| Female | 41% | |||
| Male | 59% | |||
| Underweight | 4% | |||
| Normal weight | 49% | |||
| Overweight | 36% | |||
| Obese | 12% | |||
| At risk (EAT-26 > 20) | 34% | |||
| No risk (EAT-26 < 20) | 66% | |||
| 95% CI | ||||
| Mean | SD | Lower | Upper | |
| Age (years) both sexes | 31 | 8 | 31 | 32 |
| Female | 32 | 8 | 31 | 34 |
| Male | 31 | 8 | 30 | 32 |
| Sports (years) both sexes | 8 | 4 | 8 | 9 |
| Female | 8 | 4 | 8 | 9 |
| Male | 8 | 4 | 8 | 9 |
| Weight (kg) both sexes | 74 | 17 | 72 | 76 |
| Female | 62 | 11 | 60 | 65 |
| Male | 81 | 16 | 79 | 84 |
| Ideal weight * (kg) both sexes | 65 | 10 | 64 | 66 |
| Female | 56 | 6 | 55 | 57 |
| Male | 71 | 6 | 70 | 72 |
| Height (cm) both sexes | 171 | 9 | 170 | 172 |
| Female | 164 | 6 | 163 | 165 |
| Male | 176 | 7 | 175 | 177 |
| BMI (kg/cm 2) both sexes | 25 | 4 | 24 | 26 |
| Female | 23 | 4 | 22 | 24 |
| Male | 26 | 4 | 26 | 27 |
| Body surface area ** both sexes | 1.9 | 0.3 | 1.8 | 1.9 |
| Female | 1.7 | 0.2 | 1.7 | 1.7 |
| Male | 2.0 | 0.2 | 2.0 | 2.0 |
| Basal metabolic rate *** (kcal/day) both sexes | 1657 | 267 | 1624 | 1691 |
| Female | 1478 | 152 | 1448 | 1508 |
| Male | 1780 | 259 | 1737 | 1822 |
| Highest weight (kg) | 80 | 16 | 78 | 82 |
| Female | 78 | 17 | 75 | 82 |
| Male | 81 | 16 | 78 | 83 |
| EAT-26 score (20 at risk) | 18 | 10 | 17 | 19 |
| Female | 18 | 9 | 17 | 20 |
| Male | 18 | 10 | 16 | 20 |
| Risk | Counts (Out of 249) | % of total |
|---|---|---|
| At Risk | 84 | 34% |
| No Risk | 165 | 66% |
| Subgroup Analysis of the Prevalence among At-Risk Participants N = 84 with 34% | ||
| Out of 84 | Out of 34% | |
| By age category | ||
| >=30 Years | 45 | 18% |
| <30 Years | 39 | 16% |
| By BMI category | ||
| Underweight | 1 | 0% |
| Normal weight | 49 | 20% |
| Overweight | 26 | 10% |
| Obese | 8 | 3% |
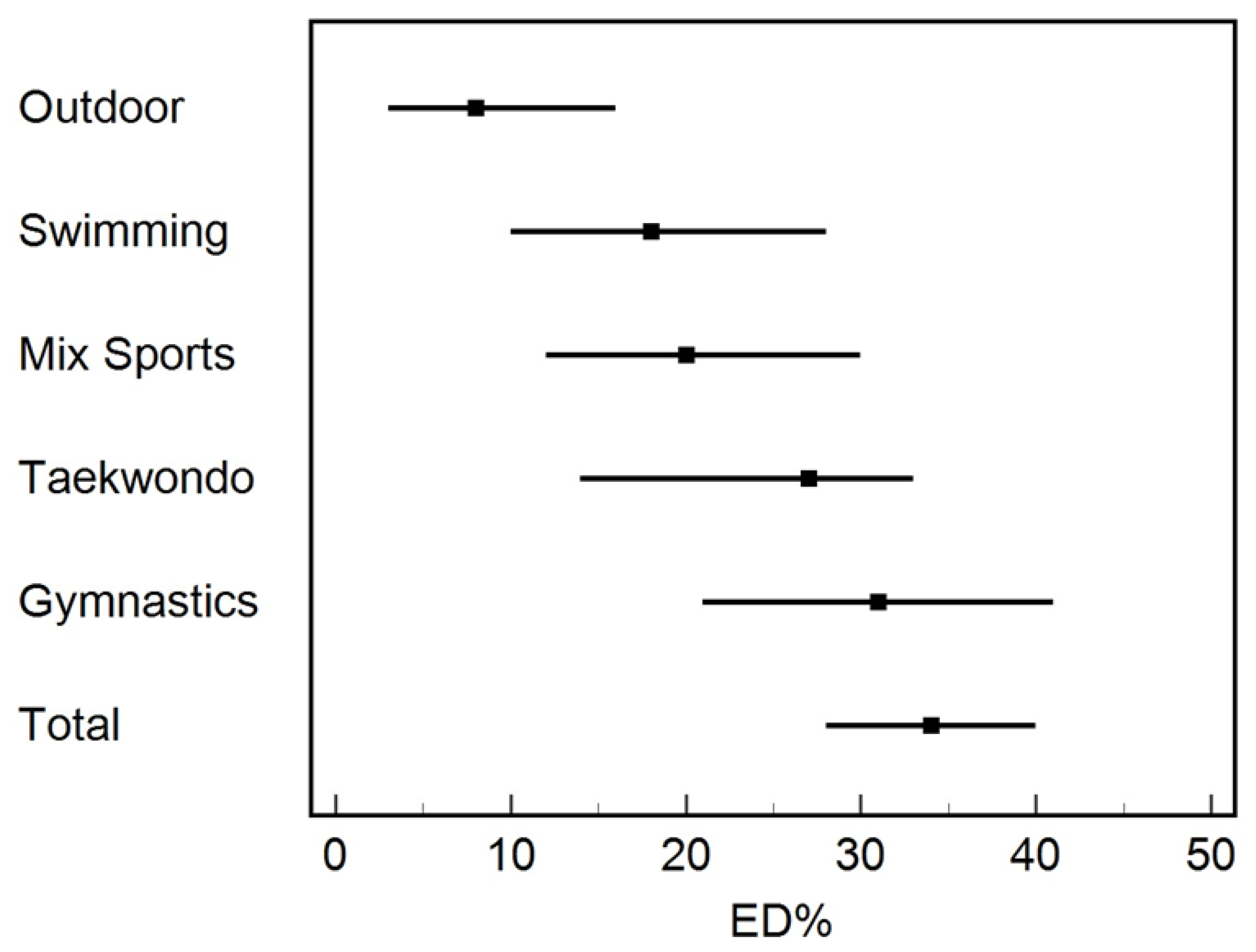
| By sport type | ||
| Outdoor | 7 | 3% |
| Swimming | 15 | 6% |
| Mix (multi-type of sports) | 17 | 7% |
| Taekwondo | 19 | 8% |
| Gymnastics | 26 | 10% |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Age | 1.02 (0.98, 1.05) | 0.38 |
| Sex | 1.63 (0.49, 5.44) | 0.42 |
| Weight | 1.06 (0.89, 1.27) | 0.50 |
| Maximum weight | 0.95 (0.8, 1.13) | 0.57 |
| BMI | 0.86 (0.51, 1.44) | 0.56 |
| Sports (years) | 1.01 (0.95, 1.08) | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghazzawi, H.A.; Alhaj, O.A.; Nemer, L.S.; Amawi, A.T.; Trabelsi, K.; Jahrami, H.A. The Prevalence of “at Risk” Eating Disorders among Athletes in Jordan. Sports 2022, 10, 182. https://doi.org/10.3390/sports10110182
Ghazzawi HA, Alhaj OA, Nemer LS, Amawi AT, Trabelsi K, Jahrami HA. The Prevalence of “at Risk” Eating Disorders among Athletes in Jordan. Sports. 2022; 10(11):182. https://doi.org/10.3390/sports10110182
Chicago/Turabian StyleGhazzawi, Hadeel A., Omar A. Alhaj, Lana S. Nemer, Adam T. Amawi, Khaled Trabelsi, and Haitham A. Jahrami. 2022. "The Prevalence of “at Risk” Eating Disorders among Athletes in Jordan" Sports 10, no. 11: 182. https://doi.org/10.3390/sports10110182
APA StyleGhazzawi, H. A., Alhaj, O. A., Nemer, L. S., Amawi, A. T., Trabelsi, K., & Jahrami, H. A. (2022). The Prevalence of “at Risk” Eating Disorders among Athletes in Jordan. Sports, 10(11), 182. https://doi.org/10.3390/sports10110182