Abstract
The lubrication of the cartilaginous structures in human joints is provided by a fluid from a specialized layer of cells at the surface of a delicate tissue called the synovial lining. Little is known about the characteristics of the fluids produced after a joint arthroplasty procedure. A literature review was carried out to identify papers that characterized the synovial lining and the synovial fluids formed after total hip or knee arthroplasty. Five papers about synovial lining histology and six papers about the lubricating properties of the fluids were identified. The cells making up the re-formed synovial lining, as well as the lining of interface membranes, were similar to the typical Type A and B synoviocytes of normal joints. The synovial fluids around joint replacement devices were typically lower in viscosity than pre-arthroplasty fluids but the protein concentration and phospholipid concentrations tended to be comparable, suggesting that the lining tissue function was preserved after arthroplasty. The widespread, long-term success of joint arthroplasty suggests that the lubricant formed from implanted joint synovium is adequate for good clinical performance in the majority of joints. The role the fluid plays in component wear or failure is a topic for future study.
1. Introduction
1.1. Synovial Tissue
An appreciation of the microanatomy of the lining tissues of the human articular joints is important to the understanding of the clinical performance of joint replacement devices used to restore function to degenerative and painful joints. For the normal cartilage-capped articular joint, lubrication of the bony, cartilaginous, ligamentous, and fibrous tissue structures is provided by a fluid produced from a specialized layer of cells found at the surface of a delicate tissue called the synovial lining (from ovum or egg, because of the similarity with egg white). This synovial tissue is composed of specialized layers of cells starting at the outermost (joint-facing) level with the intima, which overlies a vascular subintimal layer, and is supported by a fibrous stroma forming the joint capsule [1,2,3]. Of note, there is a wide range of variability in the thickness of the intimal and subintimal layers, the degree of continuity and cellularity of the intima and the presence of folds and villi (finger-like projections) depending upon numerous factors including the health of the joint, the age of the host, and the location of the sample within the joint.
The synovial tissue has been described as “controlling the environment of the joint” [4]. It does this by participating in immune reactions to bacteria, phagocytosis (removal of detritus material), lubrication, and cartilage nutrition [1,5]. In young, healthy synovium, the 1–2 cell thick intimal layer is composed of macrophage-like type A cells which are mainly phagocytic and absorptive in nature, and fibroblast-like type B cells which are secretory in nature [1,2,6,7,8,9,10,11]. This intimal layer shows low degrees of cell division, suggesting that many of the lining cells migrate to the synovial surface from underlying blood vessels and that they are bone-marrow-derived cells [12]. The synovial tissue is able to respond quickly to injury or disuse. The changes can include thickening of the intimal layer, increased vascularity and inflammatory cell infiltration of the subsynovial layer, and the formation of multiple finger-like projections (villi) into the joint. The synovial tissue of an aged individual with osteoarthritis will look very different grossly and microscopically from that of a healthy young individual.
The surgical removal of chronically inflamed synovial tissue from arthritic, tuberculoid or traumatized joints was once a common orthopaedic procedure; fortunately, the synovial tissue can regenerate [13,14]. It is this regenerative capacity that allows implanted artificial joints to be lubricated despite surgical removal or damage to the synovial tissues. The microanatomy of the re-formed joint lining tissue and the quality of the lubricating fluid that it produces are the subjects of the present review.
Following joint replacement surgery, in addition to the regeneration of the lining of the joint capsule, membranes that form between the bone and the cement, or bone and implant (known as the interface) often show a synovium-like microstructure (so-called pseudo-synovial linings) [15,16,17,18,19]. It has been suggested that motion at the interface induces the production of this specialized tissue because it was observed in association with loose implants [20,21]. More recently, it has been shown that one of the constituents of synovial fluid, hyaluronan (also referred as hyaluronic acid), can induce the synovial-like interface membrane features [22]. A synovial-like membrane can be produced in the rat or mouse dorsal air pouch by disrupting the subcutaneous connective tissue by repeated injection of air [23]. The resulting cavity develops a lining structure as early as six days later which has many features of a synovial lining, including the production of fluid, and this has become a useful experimental model of the periprosthetic tissue [23,24,25].
1.2. Synovial Fluid
The lubrication for the natural joint is provided by a small amount of viscous fluid consisting of mainly hyaluronic acid, proteins and other factors such as lubricin and surface-active phospholipid (SAPL) that allow for effective gliding of the joints [26]. As with the tissue, the characteristics and properties of the fluid vary considerably as the result of joint health, injury status and other host factors such as inflammation and hypersensitivity. Injury to the joint may result in an abundance of fluid (a joint effusion), distension of the tissues and interruption of the normal functions of the synovial tissue [13]. Under normal biological conditions, the coefficient of friction is only 0.001 to 0.006 and wear is nearly zero because of the special tribologic properties of cartilage and synovial fluid [27]. Boundary lubrication is thought to be provided by surface-active phospholipid (SAPL) complexed with lubricin and hyaluronic acid, which allows for load-bearing capacities for the joint [28,29]. Lubricin, a component found to be plentiful in synovial fluid, is thought to be the lubricating molecule that facilitates the gliding motion of joints [30]. Lubricin may be a carrier of surface-active phospholipids because the SAPL are super hydrophobic and adsorb to the joint surfaces. Hyaluronic acid (HA), found abundantly in synovial fluid, while providing a lubrication effect, does not provide the load-bearing capabilities for joints [31]. Instead, the HA portion is thought to maintain the viscosity of the synovial fluid [32,33,34] and facilitate the formation of lipid multilayers on the lubricating surface by complexing with phospholipids, providing lubrication at the joint [35]. The purpose of this review was to examine the state of knowledge regarding the changes that occur in the synovial lining and lubrication properties of the surrounding fluid after implantation of a total joint prosthesis. This review will (1) summarize the characteristics of the synovial lining tissue histomorphology and (2) the composition of synovial fluid from published studies.
2. Methods
2.1. Synovial Lining Papers
A review of PubMed- and Embase-indexed studies up to November 2014 was carried out to identify studies regarding the histological characterization of the synovial lining of joints following total hip or knee replacement (hereafter called implanted tissue). This electronic search was supplemented by a manual search of the reference lists of the included papers. Conference proceedings, single case studies, and reviews were not included in the search and only studies in English language were included. Search strings included various combinations of the terms “synovium OR synovial lining OR synovial-like membrane OR interface membrane OR synovial lining cells OR synovitis OR intima, arthroplasty OR implant OR implanted, histological OR histology, and morphology OR morphological.” Articles of interest were selected if detailed histomorphological characterization of the synovial lining or the interface membrane was performed and described. Articles were excluded for the following reasons: in vitro studies, animal studies, studies involving infection or rheumatoid arthritis exclusively, non-retrieval studies, and non-arthroplasty related studies. Articles that focused on the changes of the subintimal layers due to wear debris, but without describing the intima, were excluded from final selection. The resulting potential studies were reviewed, summarized, and critically evaluated (Figure 1).
Five articles were selected which reported the histological characterization of a synovial lining or a synovial-like membrane from implanted tissue and evaluated various bearing material combinations. Tissue specimens from a total of 173 patients were histologically examined and the morphology of the intimal layer was characterized in detail. Immunohistochemistry was performed using monoclonal and polyclonal antibodies to identify the cell subsets or the presence of prostaglandins, fibronectin, and other factors produced by the lining cells. All papers involved retrospective studies from implanted tissue. A summary of the overall findings of each selected article are presented in Table 1 and Table 2.
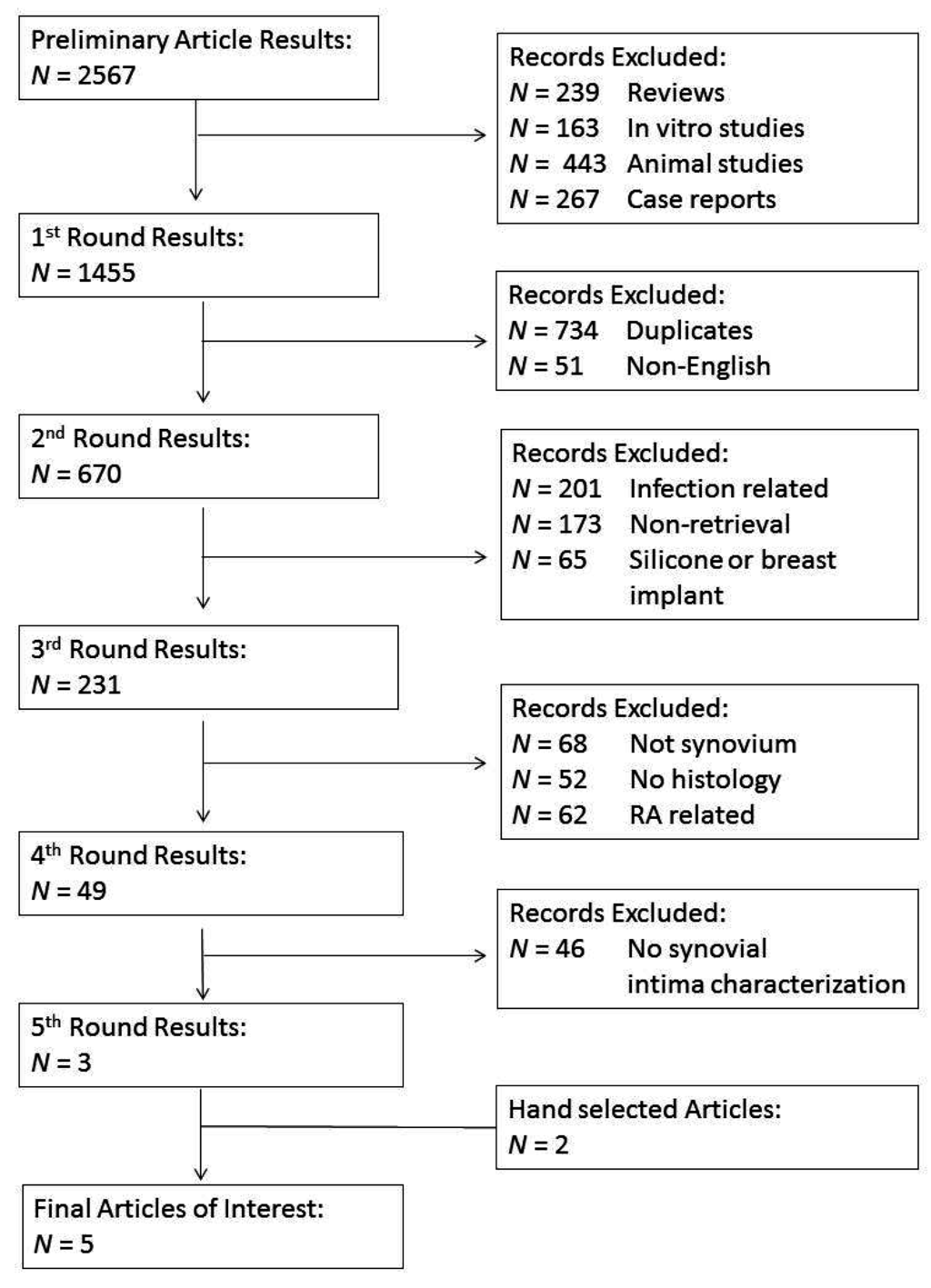
Figure 1.
Flowchart of synovial lining article selection.
Figure 1.
Flowchart of synovial lining article selection.
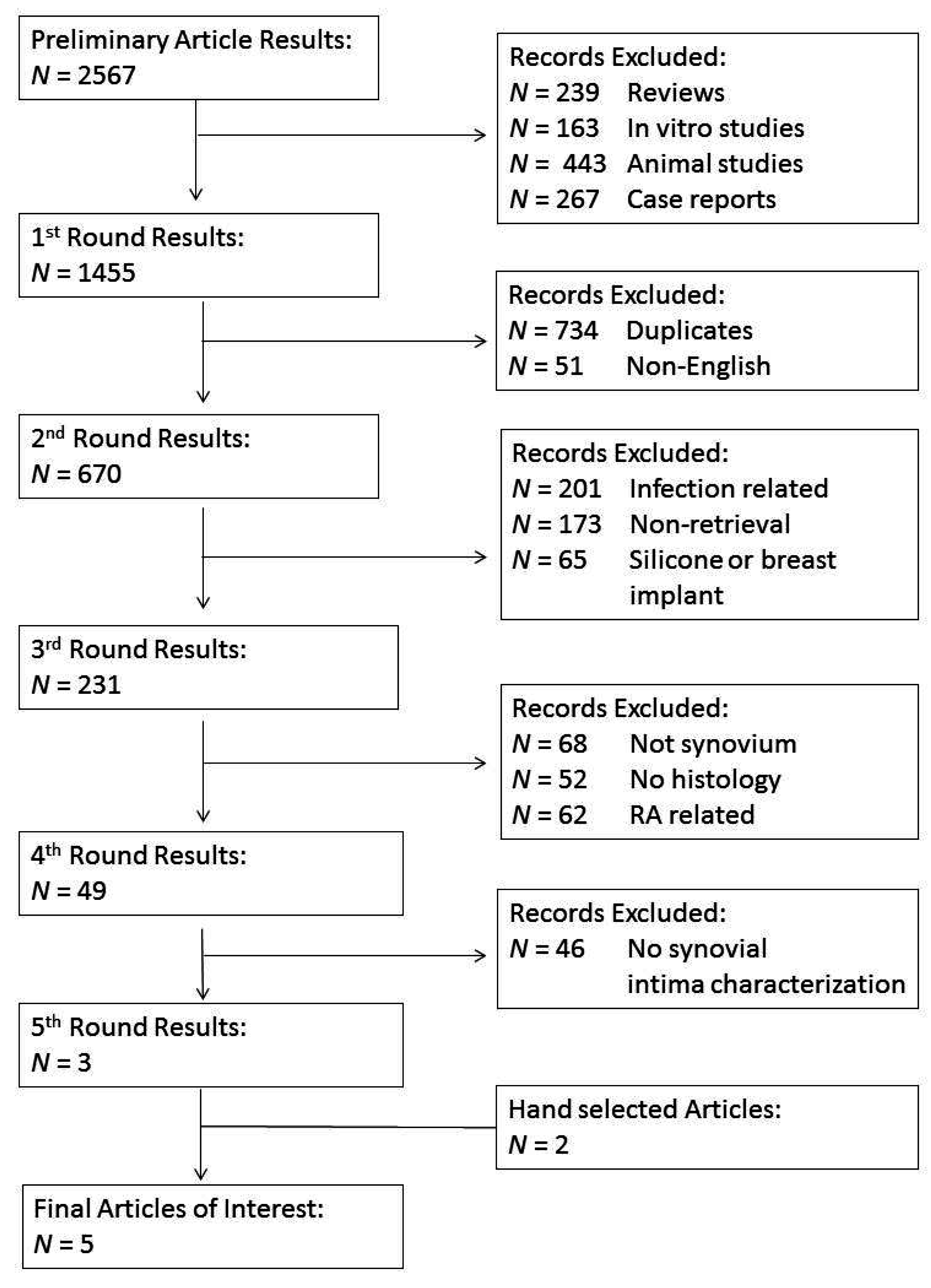

Table 1.
Overall general findings for articles selected describing synovial lining characterization.
| Author | Bearing Type 1 | Patients | Characterization of Synovial-Like Membrane | Main Synovium Findings | ||
|---|---|---|---|---|---|---|
| Layer Thickness | Synovial Lining Cells | Presence of Particulate Debris in Synovial Lining 2 | ||||
| Goldring et al. (1983) [17] | Metal on Polyethylene | N = 20 | cells |
| 0 | Membrane at cement-bone interface with histological and histochemical characteristics of normal synovium found in patients with implant loosening. |
| ||||||
| ||||||
| Goldring et al. (1986) [16] | Metal on Polyethylene | N = 41 | 1–2 cells |
| 1 | Study confirmed formation of synovial-like lining at bone-cement interface taken from patients with loosened THA components |
| ||||||
| Lennox et al. (1987) [19] | Metal on Polyethylene; Ceramic on Polyethylene | N = 61 | 1–3 cells |
| 1 | Cemented, press-fit, and biologic ingrowth prostheses showed similar formation of pseudosynovial lining at the implant-bone interface membrane. |
| ||||||
| Lalor and Revell (1993) [18] | Metal on Polyethylene and Polyethylene on Delrin THA and TKA | N = 29, 23 hip; 6 knee | 1–10 cells |
| 1 | The newly formed bone-implant interface membrane closely resembled true synovium and contained macrophage-like type A cells and fibroblast type B cells, but not necessarily always in distinct layers |
| ||||||
| Burkandt et al. (2011) [15] | Metal on Polyethylene THA; Metal on Metal HRA | N = 22, 10 with synovitis; 12 with arthroplasty. | 1–5 cells |
| 1 | Tissues from patients revised due to suggested metal hypersensitivity showed increased proliferation of synovial lining cell layer similar to cases with rheumatoid arthritis and high-grade synovitis, with 2 patients showing paucicellular synovial membrane covered by a fibrinous exudate. |
| ||||||
1 Specimens from revised hip arthroplasty unless otherwise noted and this column gives the bearing combinations; 2 the relative amounts of debris noted histologically in excised synovial lining layer: 0 = none, 1 = rare, 2 = minimal, 3 = moderate, 4 = severe; THA = total hip arthroplasty, HRA = hip resurfacing arthroplasty, TKA = Total Knee Arthroplasty; Macrophage markers: OKM1, OKM5, CD163+; Fibroblast markers: MAB67, D2-406.
Table 2.
Overall general findings for articles selected describing synovial fluid properties.
| Author | Arthroplasty | Experiment | Key Findings |
|---|---|---|---|
| Costa et al. (2001) [36] | 10 UHMWPE hip implants | Mass spectrophotometry and FTIR were performed after cyclohexane extraction for adsorbed products on the liners. | Methyl esters of hexadecanoic acid, octadecanoic acid, squalene, and of cholesterol were found in the extracts as well as a protein-like material at the surface. |
| Mazzucco et al. (2002) [37] | 58 index TKA; 19 revision TKA; 2 effused previous TKA | Sufficient SF samples were obtained from 36 index TKA, 14 revised TKA, and 2 effused previous TKA for flow property examination. | SF from revision TKA tended to have lower viscosity than that from index TKA. The difference was found to not be statistically significant. |
| Mazzucco et al. (2004) [38] | 77 index TKA; 20 revised TKA; 3 effused previous TKA | SF from 24 index TKA and 7 revised TKA had their composition of protein, phospholipids and HA determined and correlated. | Protein and phospholipids were found to have a positive correlation in regards to each other. Protein and phospholipids were found to have a negative correlation with HA. |
| Gale et al. (2007) [39] | 38 Metal on Polyethylene THA; 2 Metal on Polyethylene TKA | The bearing surfaces of the implants were rinsed and analyzed by HPLC for phospholipids. | 8 species of phosphatidylcholine were identified. 3 species of unsaturated phosphatidylcholine predominated; PLPC, POPC, and SLPC. |
| Bergmann et al. Part 1 (2001) [40] | Type 1 telemeterized cemented PE cup, 1 temperature measurement at neck; Type 2 telemeterized non-cemented, AC head, PE or AC cup, titanium shaft | Patients were monitored doing various physical activities and the temperatures inside their telemeterized implant were recorded. | The highest peak temperature were observed in the head of the implant and reached as high as 43.1 °C, greater than what is believed to affect the synovial fluids lubrication ability. |
| Bergmann et al. Part 2 (2001) [41] | (See above) | Data from Bergmann et al. 2001 part 1 was used to generate a finite element model to calculate the steady- state within the implant during walking. | The model shows that if the cup of an implant is made of a material with good conductivity, heat will be transferred away from the synovial fluid, capsule and stem towards the acetabular bone. |
THA = total hip arthroplasty, TKA = Total Knee Arthroplasty, MS = Mass spectrometry, FTIR = Fourier transform infrared spectroscopy, AC = aluminum oxide ceramic, PE = polyethylene, SF = synovial fluid, (PLPC) = Palmitoyl-linoleoyl-phosphatidylcholine, POPC = Palmitoyl-oleoyl-phosphatidylcholine, SLPC = Stearoyl-linoleoyl-phosphatidylcholine (SLPC).
2.2. Synovial Lubrication Papers
A review of PubMed studies from the time period of 2000 through 2014 was performed to find papers relevant to the lubrication characteristics of synovial fluid (SF) after joint arthroplasty. Search strings included “Synovial Fluid AND Prosthetic (136 results), Synovial Fluid AND Arthroplasty (391 results), Synovial Fluid AND Implant (91 results) and Synovial Fluid AND Revision (132 results)” for a total of 750 articles. The article titles and abstracts were examined and papers were excluded for the following reasons: SF analysis of biomarkers for periprosthetic infections, ion/cytokine/particle/cell levels, arthritic joint analysis before arthroplasty only, in vitro studies, pain only, wear/friction only, animal studies, case studies, literature reviews, and surgical procedure and imaging studies only (Figure 2).
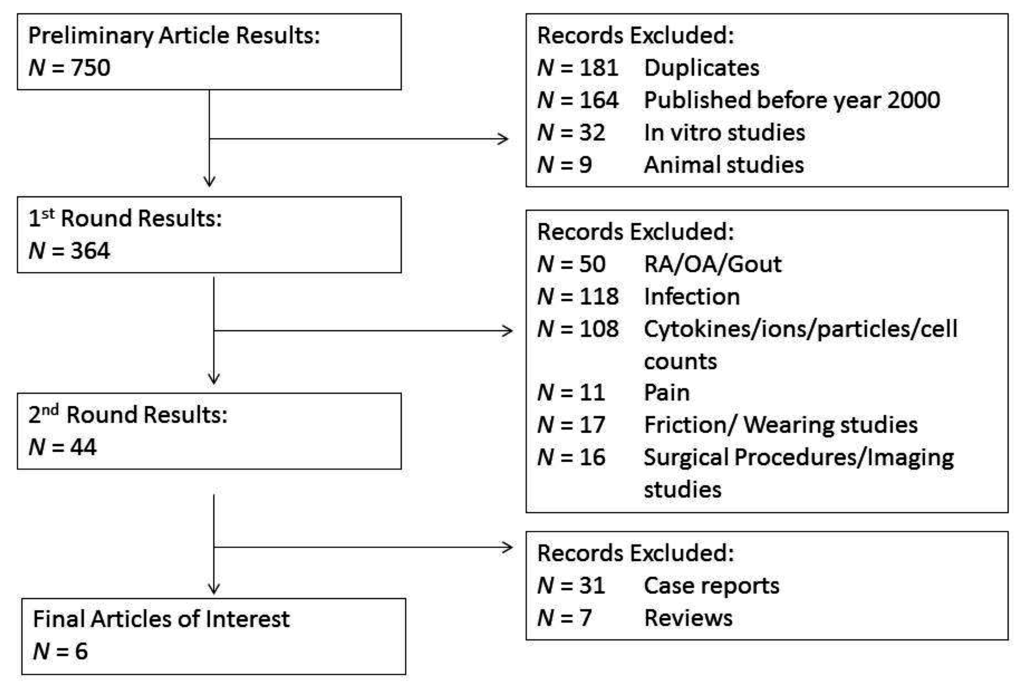
Figure 2.
Flowchart of synovial lubrication article selection.
Figure 2.
Flowchart of synovial lubrication article selection.
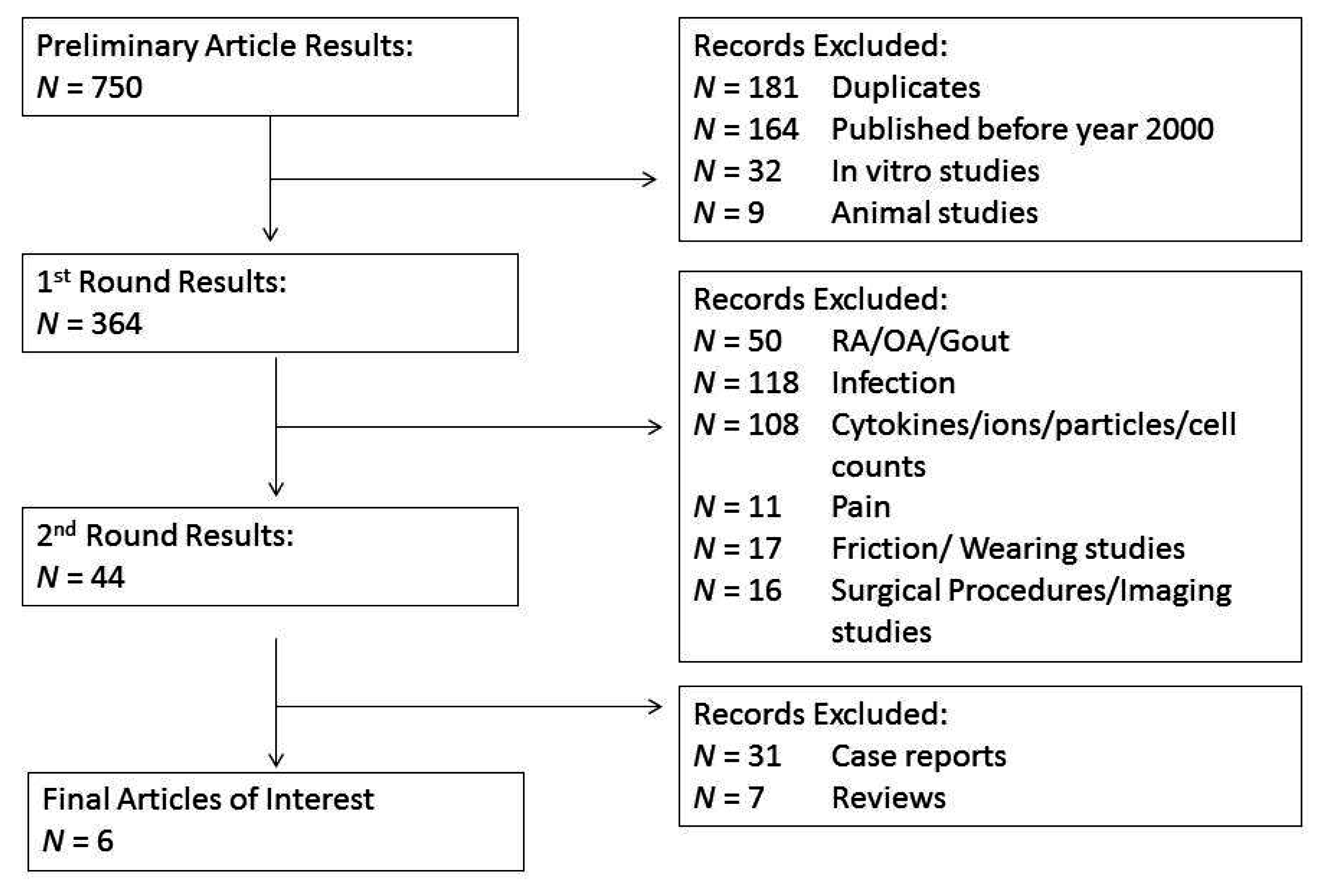
Six suitable papers were selected. Of these papers, four dealt specifically with the composition of the synovial fluid and the role this had on lubrication, while two discussed the role of increased temperature on lubricating protein degradation.
3. Results
3.1. Synovial Lining Characterization
Very few papers specifically described the histomorphology of the synovial intima in the periprosthetic capsular tissues and four of the five selected studies described the synovial-like membranes at interfaces. A common finding from those four studies of a synovial-like membrane at the bone-implant or bone-cement interface was the close resemblance to the true synovial lining membrane in cellular structure and cell type within the surface layer of excised implanted tissue. A range of histological presentations was also noted in each study, which was more pronounced in the implanted tissues compared with non-implanted tissues.
The study by Goldring et al. [17] was the first which characterized the new membrane that formed at the bone-cement interface into three distinct histological zones: (1) a synovial-like layer of lining cells at the cement surface; (2) sheets of histiocytes and giant cells in the subintima; and (3) a fibrous layer that blended into the bone and becomes continuous with the adjacent bone marrow. The membrane was lined with large polygonal cells, often with nuclei pointing away from the surface and a coating of fibrin around the surface. Cytoplasm was abundant and the nuclei were oval dark and uniform. Occasionally, multinucleated giant cells appeared within the lining cells. In a later study of prosthetic loosening after total hip arthroplasty, Goldring et al. confirmed the presence of a synovial-like lining with the same morphology in lining tissues adjacent to the implant [16]. Tissue cultures from implanted specimens showed three distinct cell types identified as stellate or dendritic cells, macrophage-like cells with phagocytosed latex or India-ink particles, and elongated fibroblast-like cells.
In a comparison of tissues from cemented, press-fit and biologic ingrowth prostheses revised due to aseptic loosening, Lennox et al. [19] described variations in the histomorphology and described three types of lining tissues. Type 1 linings comprised large, rounded or teardrop-shaped cells that were 1–3 cell layers thick. Type 2 membranes were composed of weakly stained collagenous matrix containing large dendritic-shaped cells with eccentrically located nuclei and long cellular processes extending toward the surface. Type 3 surfaces consisted of thick collagen fibers oriented perpendicular to the surface. All three surfaces were present on interface membranes from cemented, press-fit, and biologic ingrowth prostheses.
Lalor and Revell [18] compared the interface membrane of implanted tissue excised during revision surgery to normal synovium and rheumatoid arthritis tissue controls. They found that the new interface tissue had a layer of cells adjacent to the implant similar in appearance to normal synovial intima. This surface layer varied in thickness from 1 to 10 cells deep in a palisading structure, depending on each case and sample. Antibody staining for macrophage-like type A cells and fibroblast-like B cells was positive in the implanted tissue and showed the intermixing of the two cell types within the lining, similar to unimplanted tissue. Unlike the normal synovial lining and rheumatoid arthritis control tissues, separate distinct layers of macrophages and deeper fibroblasts were not seen in the implanted tissues, which could be because of the abundant macrophage infiltration of the subintimal area in response to wear debris.
In another comparison study of non-implanted and implanted tissues by Burkandt et al. [15] immunohistochemical staining was used to compare tissues from patients with low and high grade synovitis (inflammation), metal or polyethylene (PE) wear particle-induced synovitis and proliferative desquamative synovitis (associated with suspected metal hypersensitivity). The authors reasoned that, since proliferation of the synovial lining cell layer is a characteristic feature of autoimmune joint diseases, morphological changes of the synovial lining in periprosthetic tissues may indicate the presence of an immune response. The intimal lining of the PE wear particle-induced synovitis group was 1–2 cells thick, comparable to the unimplanted low grade synovitis group. By contrast the tissue from the high grade unimplanted synovitis tissue lining was five or more cells thick while the tissues from two metal-on-metal cases with extensive metal wear particle staining had a denuded cellular lining. The tissues from five cases with suspected metal hypersensitivity had a proliferating, viable synovial lining containing abundant fibroblast-like cells. Interestingly, the subsynovial layer of those tissues contained lymphocytes, an immune cell that was only seen in the high-grade rheumatoid synovitis tissues but not in the PE hip tissues. The authors suggested that the morphological similarities between tissues from patients revised for suspected metal hypersensitivity and patients with rheumatoid arthritis adds to the evidence that metal hypersensitivity shares characteristic morphological features with autoimmune diseases of the joints.
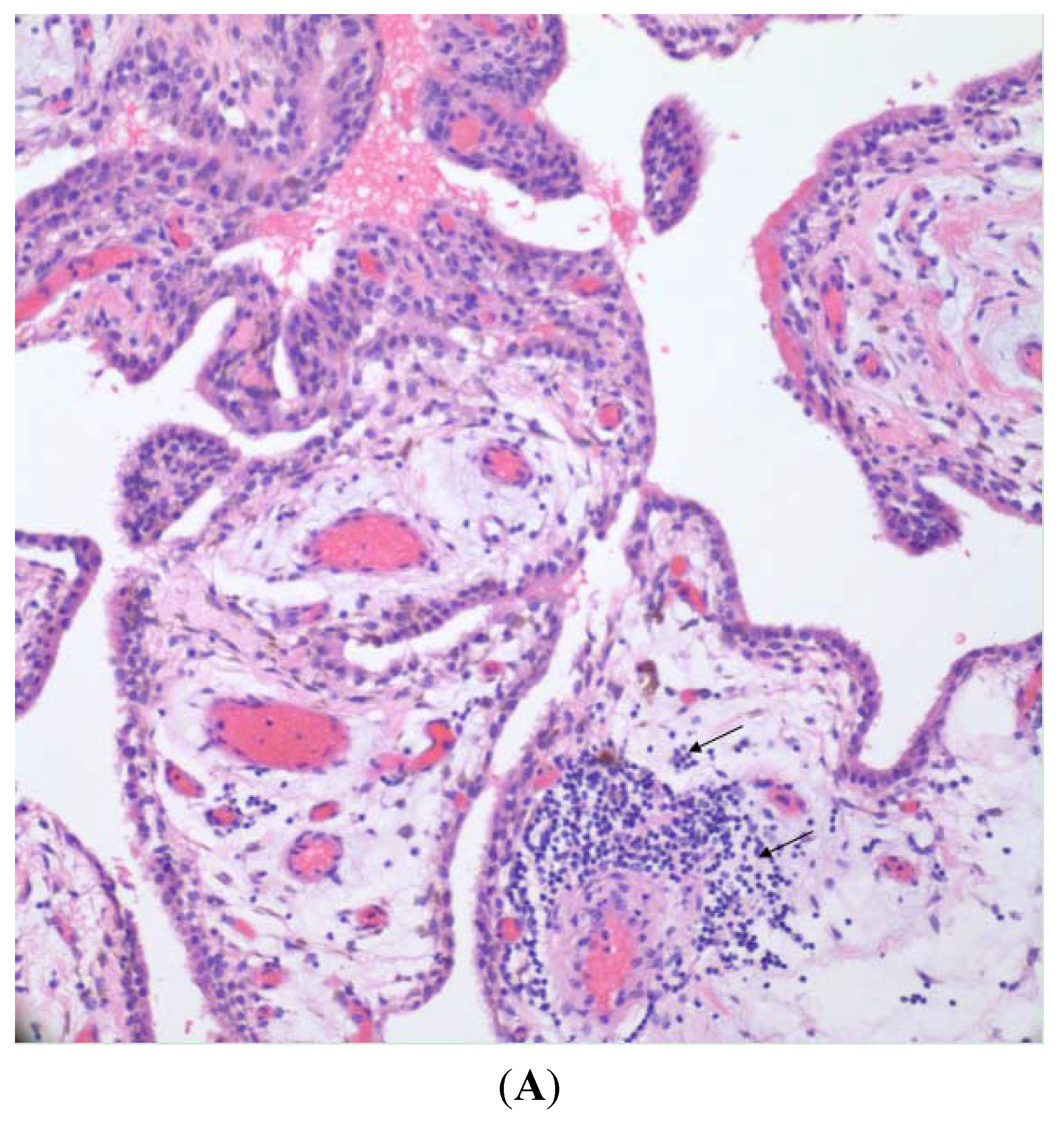
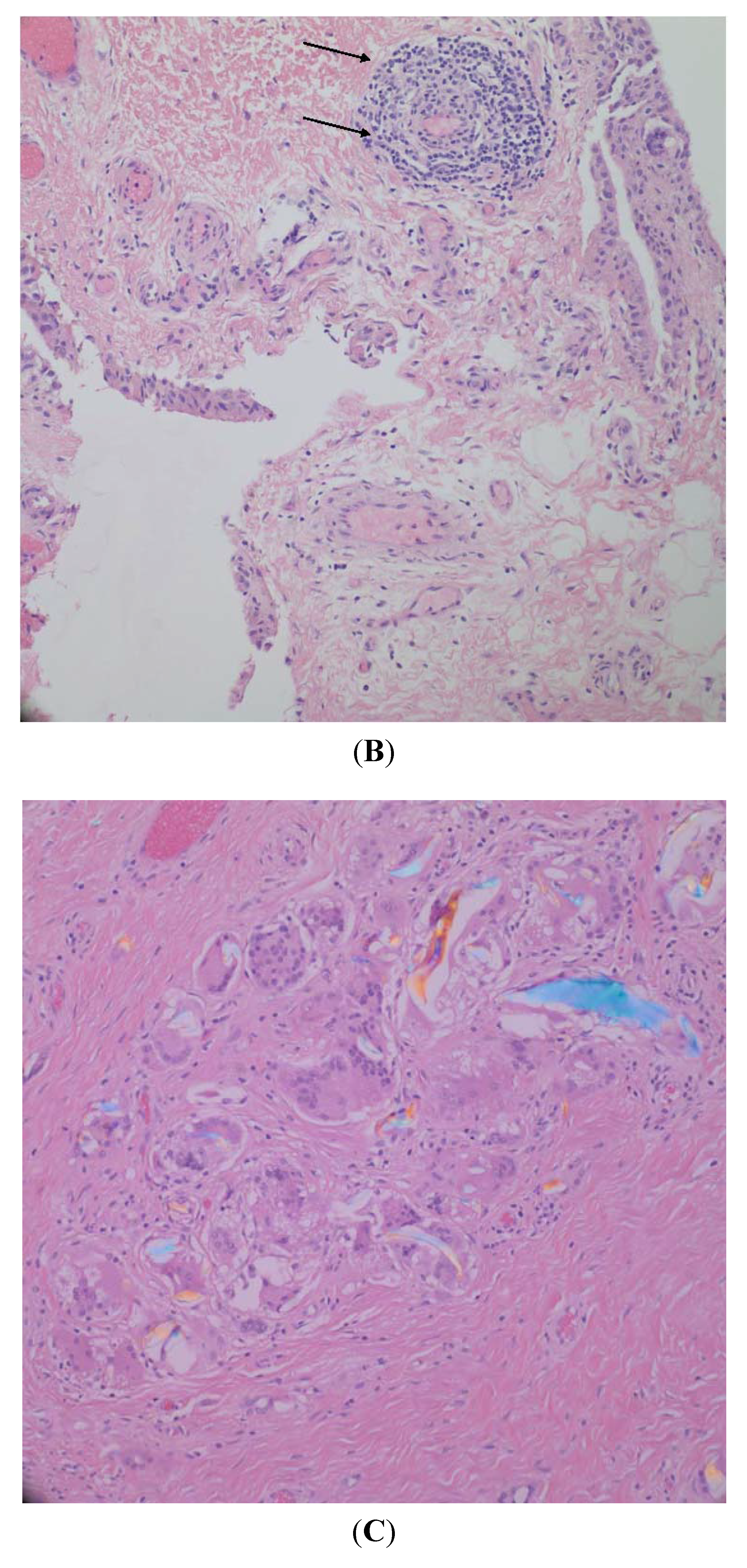
Figure 3 shows light micrographs of synovial tissue from an osteoarthritic joint prior to metal-on-polyethylene joint replacement (Figure 3A) and then following revision of that joint replacement (Figure 3B) in the same patient. Microscopic examination of both pre- and post-revision specimens in this patient shows an intimal/synovial lining with an underlying, non-specific, lymphoplasmacytic, chronic inflammatory infiltrate adjacent to, or centered around blood vessels. The post-revision specimen displays a denser collagenous subintimal layer (Figure 3B). Also present in the post-revision tissues are fragments of polarizable polyethylene with accompanying chronic inflammation including foreign body giant cells (Figure 3C).

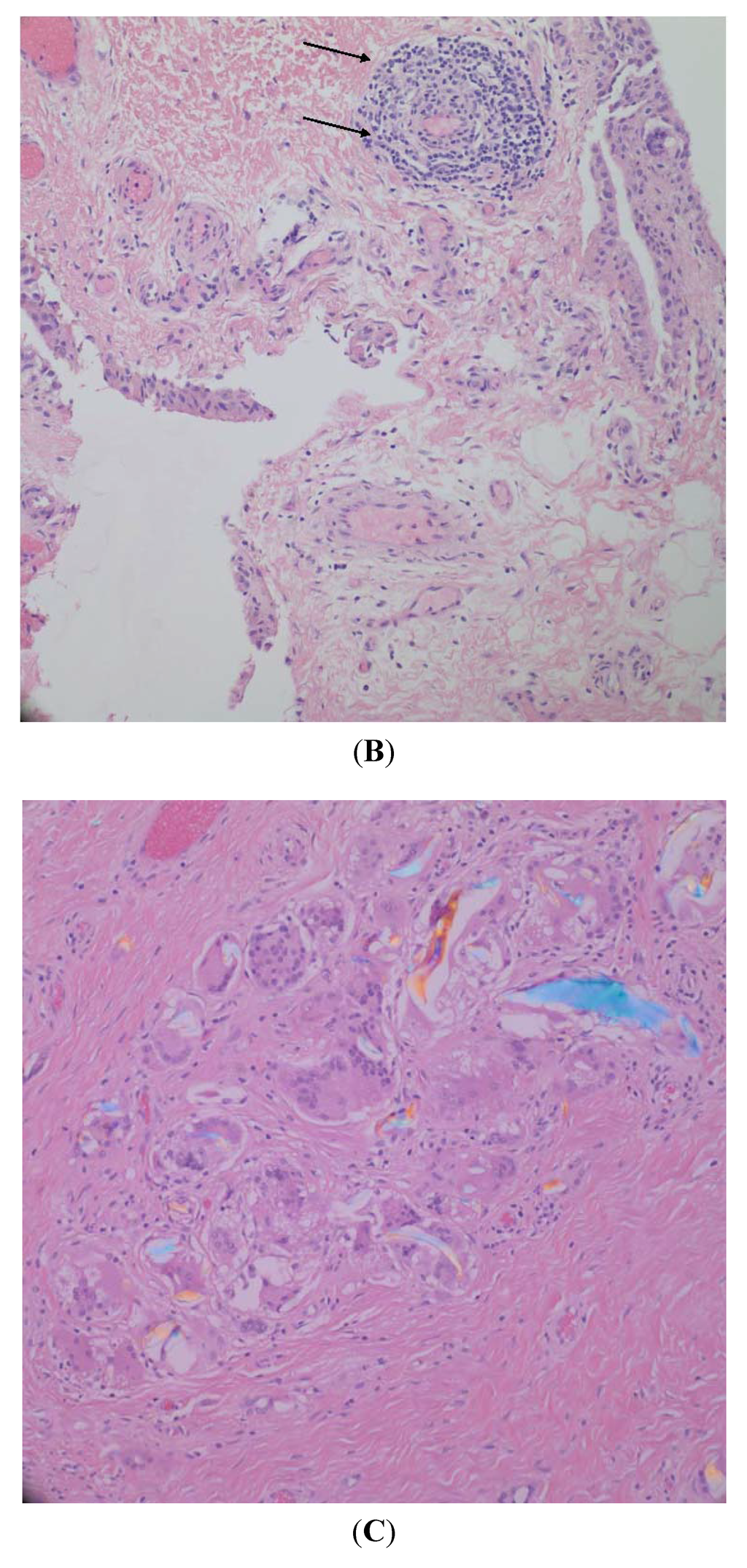
Figure 3.
(A) Pre-revision specimen showing synovial lining with intact intimal layer and non-specific chronic inflammatory infiltrate (H&E 200×); (B) post-revision specimen showing intact intimal layer, denser subintimal collagenous tissue, and non-specific chronic inflammatory infiltrate (arrows) (H&E 200×); and (C) post-revision specimen, deep to the synovial lining showing multiple fragments of polyethylene with accompanying chronic inflammatory infiltrate including foreign body giant cells (H&E, polarized, 200×).
Figure 3.
(A) Pre-revision specimen showing synovial lining with intact intimal layer and non-specific chronic inflammatory infiltrate (H&E 200×); (B) post-revision specimen showing intact intimal layer, denser subintimal collagenous tissue, and non-specific chronic inflammatory infiltrate (arrows) (H&E 200×); and (C) post-revision specimen, deep to the synovial lining showing multiple fragments of polyethylene with accompanying chronic inflammatory infiltrate including foreign body giant cells (H&E, polarized, 200×).
3.2. Synovial Fluid Properties
There is a large amount of information on the topic of synovial fluid properties and there is also a substantial body of literature on the tribology of artificial prosthetic joints. One review and analysis of the last decade of literature reiterated the complex nature of SF as a lubricant in both natural and artificial joints [42]. Two major mechanisms are theorized to play a role in both natural and artificial joints; boundary lubrication and fluid film lubrication. Macromolecules within the synovial fluid play a key role in both forms of lubrication. Another important mechanism of lubrication not addressed by the articles presented in this review is the theory of self-pressurized hydrostatic lubrication or biphasic lubrication. Cartilage has a biphasic nature in which a porous elastic matrix is infiltrated by interstitial fluid [43]. As the interstitial fluid is forced to flow through the permeable matrix a pressure gradient develops. The cartilage interstitial water supports most of the joint contact load. Pressurization of this fluid shifts most of the contact load away from the collagen-proteoglycan matrix resulting in a stress shielding effect and a low friction coefficient [43,44]. It should also be noted that with articulating cartilage and soft tissue, fluid pressurization is another distinct mechanism, besides boundary and fluid film lubrication, which is important. However, this review showed that there is little information about the characteristics of the fluid lubricating prosthetic joints or how alterations in implanted synovial tissue affect lubricant production, composition or efficiency.
In a study by Costa et al. [36] the constituents of synovial fluids that had been absorbed into the surfaces of ten revised PE hip implants (5 ethylene oxide/5 gamma ray sterilized in air) that were implanted for degenerative arthritis and replaced because of aseptic failure after 6–23 years were characterized. These products were extracted with cyclohexane then examined by mass spectrophotometry and Fourier transform infrared (FTIR) analysis was performed on the cross sections of the implants. Methyl esters of hexadecanoic and octadecanoic acids, of squalene, and of cholesterol were found in the extracts and a protein-like material was found on the surface of the implants. The diffusion of these molecules was postulated to cause the semi-crystalline polymer to become plasticized, especially at the surface where the greatest amount of absorbed material was found. This could cause changes to the ultimate tensile strength and ultimate elongation of the polymer, which could lead to a softer surface and decreased resistance to abrasion. The authors noted that accelerated simulated artificial joint testing may not allow time for the adsorption of synovial fluid constituents.
Joint fluid flow properties likely play an important role in fluid-film lubrication. A study by Mazzucco et al. [37] examined the flow properties of synovial fluid at the time of total knee arthroplasty (TKA) and at revision. Fifty-eight samples were obtained from patients undergoing index TKA surgery for osteoarthritis, 19 from revision TKA in other patients and two samples from aspirated effused joints that had undergone previous TKA. The volume of 22 samples from TKA, and five from revision TKA were insufficient for testing. Of the 14 samples from revision TKA, seven were revised because of wear and seven for mechanical problems not specific to wear. The average age of the tested patients was 70 years old (42 to 89 years). Synovial fluid at revision had lower viscosity in comparison to fluid at index TKA, which was more often within the normal range. However, the difference was not found to be statistically significant by the authors. There was variation in terms of viscosity in both pre- and post-revision groups and viscosity in both was decreased compared to synovial fluid from healthy young individuals. The authors suggested that, since hyaluronic acid (HA) is considered the major component of SF that affects its viscosity, the addition of HA to the lubricants used in joint simulation studies could provide an artificial joint fluid with viscosity more similar to natural SF. Previous studies performed on animals [45] have shown decreased HA concentrations after joint replacement which may explain the observations in these revision fluids.
Having explored fluid-film lubrication previously, Mazzucco et al. [38] explored the correlation of certain molecules associated with boundary lubrication and their association with flow properties. These boundary lubricants included phospholipids and proteins that passively diffuse through the joint capsule to reach the synovial fluid via filtration, and lubricin and superficial zone proteins (SZP) that are actively secreted into the joint fluid by synoviocytes. One hundred joint fluid samples were obtained, 77 from patients undergoing TKA for osteoarthritis (except 1 from post-traumatic arthritis), 20 from revision TKA, and 3 samples from aspirated effused joints that had previously undergone TKA. However, the majority of the samples (69) were insufficient in volume for analysis. Of the 14 revision samples examined, 10 were revised for wear related osteolysis and 4 for non-wear specific mechanical problems. A positive correlation was found between protein concentration and phospholipid concentration in pre and post-TKA synovial fluid. This indicated that the joint capsule functioned the same as before surgery and allowed diffusion of these macromolecules from interstitial fluid to the joint SF. A negative correlation was seen between these two components of SF and hyaluronic acid i.e., when HA levels were low, protein and phospholipids were high, or when HA levels were high, protein and phospholipids were low. The authors offered two explanations for this. One was that when HA was low, the synovial membrane could compensate by allowing increased entry of proteins into the synovial fluid. Another explanation was that when protein content was high synoviocytes down-regulate production of HA. Seemingly the ability of the joint capsule to synthesize SF components and regulate macromolecule filtration is linked to one another. These findings were found in both pre and post-TKA specimens.
The surface-active phospholipids (SAPLs) in lubricin are believed to play an important role in boundary lubrication and analyzing the surfaces of revised implants for their presence was performed by Gale et al. [39]. The bearing surfaces of 38 revised total hips and 2 total knees, all with metal-on-polyethylene bearings were rinsed and analyzed by HPLC for phospholipids. In total eight different species of phosphatidylcholines were identified by the study. Palmitoyl linoleoyl phosphatidylcholine palmitoyl oleoyl phosphatidylcholine and stearoyl linoleoyl phosphatidylcholine were identified as the phospholipids most likely responsible for boundary lubrication. The authors recommended that a combination of saturated and unsaturated phosphatidylcholines be added to joint simulator lubricants to produce an artificial joint fluid that more closely simulated the boundary lubrication properties of normal SF.
In a novel study using an instrumented total hip prosthesis with a metal-on-polyethylene bearing, Bergmann et al. [40] measured the temperature resulting from friction at the bearing surfaces caused by walking and other physical activities. In part 1 of the study, temperatures inside two types of telemeterized hip prostheses were recorded at 9 locations along the prosthesis length. The implant comprised a titanium shaft, aluminum oxide ceramic head and a polyethylene cup. This non-cemented prosthesis was used in 4 patients, one of which has a second contralateral instrumented implant with a ceramic cup. Steady state temperatures were reached after 60 min of walking. The temperatures often rose above the critical level (42 °C) needed to cause synovial fluid protein degradation and precipitation. The joint fluid components lost to precipitation could result in decreased lubrication properties.
The authors noted that the volume of the synovial fluid and its lubricating function play a large role in the generation of heat in the active joint. If the acetabular cup material has good conductivity such as ceramic and metal, it would facilitate transfer of heat to the acetabular bone and away from the synovial fluid, capsule, and stem. The same is true of the stem, where a good heat conducting material like cobalt chromium alloy transfers heat away from the femoral head to the colder part of the implant. The authors suggested that an implant with better head and cup separation during the swing phase of walking would allow for better lubrication and heat dissipation. Bergmann et al. [41] noted that if hip simulators use a constant controlled temperature of 37 °C, such conditions may not mimic the rising and falling temperatures related to variable levels of in vivo joint activity.
4. Discussion
The purpose of this review of the literature was to examine (1) what is known about the synovial lining tissue histomorphology and (2) the composition of synovial fluid in joints following implantation of prosthetic implants.
Specifically, the primary focus of this review was to find papers in which the intimal layer of the synovial lining was characterized because type A and type B synoviocytes reside there, and they are the cells that contribute to the lubrication properties of the joint. Therefore, stringent criteria were set in our search for articles of interest. Many key implant retrieval articles described changes in the synovial tissue in general but were excluded because they focused on the subintimal layer and the inflammatory responses due to wear debris. Of note, several studies of the histological features of tissues from metal-on-metal total hips have reported the partial or complete loss of the synovial lining cells and their replacement by fibrin or by necrotic tissue [46,47,48,49,50]. How this might affect the lubrication of those bearings has not been addressed. In addition, many papers described the synovial lining in great detail but were excluded because the studies were focused on tissues excised from arthritic or diseased joints, not implanted joints [1,2,3,51].
The membranes that form at the interfaces of implants have been consistently described as resembling the normal synovial lining. With immunohistochemical methods, implanted synovial-like membrane cells tested positive for macrophage-like and fibroblast-like markers [15,16,17,18,19]. These findings imply that the formation of an interfacial membrane after implantation is a natural response to the influence of micromotion or from chemical mediators such as hyaluronic acid. The similarity in the intimal cell types and arrangement in membranes and joint linings has led to the conclusion that these tissues are likely to be capable of inflammatory cytokine production leading to bone loss and local tissue damage in the same way that the rheumatoid synovial pannus is responsible for local tissue destruction [17].
Under conditions of osteoarthritis and rheumatoid arthritis, synovitis is present and the increase in cell layer thickness, the excess of synoviocytes and increased fluid production are thought to contribute to the destruction of articular cartilage, and the formation of bone cysts. The thickening of fibrotic tissue in the synovial lining and dense cellular infiltrates of lymphocytes and monocytes are common morphological observations of the diseased synovium [52]. These changes in the synovial lining structure may transform the natural lubrication properties of the synovial fluid after joint replacement surgery. Delecrin et al. found that the level of total synovial fluid after total arthroplasty increased in a rabbit model, but the level of hyaluronic acid remained significantly lower than the internal controls [45] and the decrease in HA after implantation was found to be similar in humans as well [53].
For the selection of papers describing or characterizing implanted joint fluids, we excluded a large number of articles that focused on clinical management, synovial biomarkers, in vitro simulation studies and others that mentioned synovial fluid but not from the implanted joint. This left only a handful of studies of synovial fluids after arthroplasty. These studies reported that even though post-implantation SF properties are similar to pre-arthroplasty SF properties in some regards, significant alterations in composition and properties exist after arthroplasty surgery. Phospholipid overall contribution to boundary lubrications still remains unclear. Initial studies into its role utilized phospholipases, but it appears these early studies were contaminated with low levels of proteolytic enzymes. Later studies with proteolytic inhibitors did not show this increase in friction after phospholipase digestion. Studies performed in vivo in rabbits, however, have shown a reduced coefficient of frictions when DPPC liposomes and hyaluronic acid were delivered via intraarticular injections to damaged joints in comparison to only hyaluronic acid injections [54]. Studies have found that hyaluronic acid plays a key role in fluid film lubrication and the viscosity of the synovial fluid. Decreased production of HA by type B synoviocytes could explain the decreased viscosity in post arthroplasty fluid and a reciprocal increase of joint wear [37,38]. Lubricin has previously been identified as a key protein in boundary lubrication [55]. The role of species other than HA and lubricin, such as the various phosphatidylcholines, in post arthroplasty lubrication should be explored in future studies as they may have significance in boundary lubrication. These include hexadecanoic acid, octadecanoic acids, squalene, and cholesterol. [36] These proteins adsorb at the cobalt chromium surface to form thin, discontinuous deposited films in vitro. Because increasing protein content increases film thickness and can be directly correlated with femoral head wear, it seems likely that patient SF chemistry plays an important role in lubrication [56]. The choice of the optimal implant bearing materials for a given patient may, in future, be based on a better understanding of this individual SF chemistry.
One of the themes throughout the small number of studies characterizing post arthroplasty lubricants was the comparison with artificial joint simulator lubricants. Joint simulator studies have been performed for decades but there are often large differences between labs in the properties of the lubricants used to conduct the tests [42,57,58,59]. The conditions that these simulations are run under also differ markedly from joint function in vivo including the volume and temperature of the fluids. Several authors noted that artificial lubricant differs from post arthroplasty synovial fluid in many regards and suggested ways that this could be improved. For example, supplementation of hyaluronic acid, and a mixture of saturated and unsaturated phosphatidylcholine could lead to an artificial synovial fluid with properties more similarly seen in vivo. Brandt et al. suggest the addition of hyaluronic acid and phosphate-buffered saline to alpha-calf serum to be essential constituents in artificial lubricants [60]. Running the simulators with temperatures measured in vivo and for a longer duration could lead to tribological conditions that more closely resemble what an artificial joint experiences in the body [40].
In addition, higher serum degradation and larger wear particles were observed with smaller fluid volumes used for testing [61]. Despite the differences between in vitro and in vivo joint lubrication, the overall success of joint replacement components shows that the fundamental requirements for clinical use have been met.
5. Conclusions
There was a surprising lack of studies on implanted synovial tissue and the lubricating fluid it produces, although that tissue presumably plays an important role in the tribology and success of joint arthroplasty. The synovial lining tissue regenerates after implantation and produces a lubricating fluid that is sufficient in volume and lubricating constituents to allow the majority of joint replacements to function successfully, possibly for decades. The exact conditions for well-functioning implants are unclear; however, preserving the integrity of the joint including the synovial lining and natural lubricating fluid properties for joint arthroplasty may be key to successful implant survivorship. Whether the degree of implant wear or if some cases of failure can be attributed to any synovial tissue or lubricant deficiency are questions that remain to be answered and warrant future investigation.
Author Contributions
Michael Shang Kung and John Markantonis performed the systematic review. Patricia Campbell and Scott D. Nelson designed the study, assisted with the literature search and reviewed the histology. All authors were involved in the manuscript preparation and editing for final submission.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ghadially, F.N. Fine Structure of Synovial Joints: A Text and Atlas of the Ultrastructure of Normal and Pathological Articular Tissues; Butterworths: London, UK; Boston, MA, USA, 1983. [Google Scholar]
- Ghadially, F.N.; Roy, S. Ultrastructure of Synovial Joints in Health and Disease; Butterworths: London, UK, 1969. [Google Scholar]
- Key, J.A. The Synovial Membrane of Joints and Bursae, 2nd ed.; Paul, B., Hober: New York, NY, USA, 1932. [Google Scholar]
- Bronner, F.; Farach-Carson, M.C. Bone and Osteoarthritis; Springer-Verlag: London, UK, 2007; Volume 4. [Google Scholar]
- Pavlovich, R.I.; Lubowitz, J. Current concepts in synovial tissue of the knee joint. Orthopedics 2008, 31, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Athanasou, N.A.; Quinn, J.; Heryet, A.; Puddle, B.; Woods, C.G.; McGee, J.O. The immunohistology of synovial lining cells in normal and inflamed synovium. J. Pathol. 1988, 155, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Barland, P.; Novikoff, A.B.; Hamerman, D. Electron microscopy of the human synovial membrane. J. Cell Biol. 1962, 14, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, T.; Shikichi, M.; Kitamura, H.; Yanase, H.; Nozawa-Inoue, K. Morphology and functional roles of synoviocytes in the joint. Arch. Histol. Cytol. 2000, 63, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Mapp, P.I.; Revell, P.A. Fibronectin production by synovial intimal cells. Rheumatol. Int. 1985, 5, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, T.; Spycher, M.A.; Ruttner, J.R.; Fehr, K. The ultrastructural localization of fibronectin in the lining layer of rheumatoid arthritis synovium: The synthesis of fibronectin by type B lining cells. Rheumatol. Int. 1983, 3, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Yielding, K.L.; Tomkins, G.M.; Bunim, J.J. Synthesis of hyaluronic acid by human synovial tissue slices. Science 1957, 125, 1300. [Google Scholar] [CrossRef] [PubMed]
- Hogg, N.; Palmer, D.G.; Revell, P.A. Mononuclear phagocytes of normal and rheumatoid synovial membrane identified by monoclonal antibodies. Immunology 1985, 56, 673–681. [Google Scholar] [PubMed]
- Depalma, A.F. Diseases of the Knee: Management in Medicine and Surgery, 1st ed.; J.B. Lippincott Company: Philadelphia, PA, USA, 1954. [Google Scholar]
- Key, J.A. The reformation of synovial membrane in the knees of rabbits after synovectomy. J. Bone Joint Surg. 1925, 7, 793–813. [Google Scholar]
- Burkandt, A.; Katzer, A.; Thaler, K.; Von Baehr, V.; Friedrich, R.E.; Ruther, W.; Amling, M.; Zustin, J. Proliferation of the synovial lining cell layer in suggested metal hypersensitivity. In Vivo 2011, 25, 679–686. [Google Scholar] [PubMed]
- Goldring, S.R.; Jasty, M.; Roelke, M.S.; Rourke, C.M.; Bringhurst, F.R.; Harris, W.H. Formation of a synovial-like membrane at the bone-cement interface. Its role in bone resorption and implant loosening after total hip replacement. Arthritis Rheum. 1986, 29, 836–842. [Google Scholar]
- Goldring, S.R.; Schiller, A.L.; Roelke, M.; Rourke, C.M.; O’Neil, D.A.; Harris, W.H. The synovial-like membrane at the bone-cement interface in loose total hip replacements and its proposed role in bone lysis. J. Bone Joint Surg. 1983, 65, 575–584. [Google Scholar] [PubMed]
- Lalor, P.A.; Revell, P.A. The presence of a synovial layer at the bone-implant interface: An immunohistological study demonstrating the close similarity to true synovium. Clin. Mater. 1993, 14, 91–100. [Google Scholar] [CrossRef]
- Lennox, D.W.; Schofield, B.H.; McDonald, D.F.; Riley, L.H., Jr. A histologic comparison of aseptic loosening of cemented, press-fit, and biologic ingrowth prostheses. Clin. Orthop. Relat. Res. 1987, 171–191. [Google Scholar]
- Drachman, D.B.; Sokoloff, L. Role of movement in embryonic joint development. Dev. Biol. 1966, 14, 401–420. [Google Scholar] [CrossRef]
- Engh, C.A.; Oconnor, D.; Jasty, M.; Mcgovern, T.F.; Bobyn, J.D.; Harris, W.H. Quantification of implant micromotion, strain shielding, and bone-resorption with porous-coated anatomic medullary locking femoral prostheses. Clin. Orthop. Relat. Res. 1992, 285, 13–29. [Google Scholar] [PubMed]
- Konttinen, Y.T.; Li, T.F.; Mandelin, J.; Ainola, M.; Lassus, J.; Virtanen, I.; Santavirta, S.; Tammi, M.; Tammi, R. Hyaluronan synthases, hyaluronan, and its CD44 receptor in tissue around loosened total hip prostheses. J. Pathol. 2001, 194, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.C.; Sedgwick, A.D.; Willoughby, D.A. The formation of a structure with the features of synovial lining by subcutaneous injection of air: An in vivo tissue culture system. J. Pathol. 1981, 134, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Pap, G.; Machner, A.; Rinnert, T.; Horler, D.; Gay, R.E.; Schwarzberg, H.; Neumann, W.; Michel, B.A.; Gay, S.; Pap, T. Development and characteristics of a synovial-like interface membrane around cemented tibial hemiarthroplasties in a novel rat model of aseptic prosthesis loosening. Arthritis Rheum. 2001, 44, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, A.D.; Sin, Y.M.; Edwards, J.C.W.; Willoughby, D.A. Increased inflammatory reactivity in newly formed lining tissue. J. Pathol. 1983, 141, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Radin, E.L.; Paul, I.L.; Swann, D.A.; Schottstaedt, E.S. Lubrication of synovial membrane. Ann. Rheum. Dis. 1971, 30, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Konttinen, Y.T.; Zhao, D.; Beklen, A.; Ma, G.; Takagi, M.; Kivela-Rajamaki, M.; Ashammakhi, N.; Santavirta, S. The microenvironment around total hip replacement prostheses. Clin. Orthop. Relat. Res. 2005, 430, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Hills, B.A.; Butler, B.D. Surfactants identified in synovial fluid and their ability to act as boundary lubricants. Ann. Rheum. Dis. 1984, 43, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Seror, J.; Zhu, L.; Goldberg, R.; Day, A.J.; Klein, J. Supramolecular synergy in the boundary lubrication of synovial joints. Nat. Commun. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Radin, E.L.; Swann, D.A.; Weisser, P.A. Separation of a hyaluronate-free lubricating fraction from synovial fluid. Nature 1970, 228, 377–378. [Google Scholar] [CrossRef] [PubMed]
- McCutchen, C.W. Joint lubrication. Bull. Hosp. Jt. Dis. Orthop. Inst. 1983, 43, 118–129. [Google Scholar]
- Balazs, E.A. The Physical Properties of Synovial Fluid and the Specific Role of Hyaluronic Acid; J B Lippincott: Philadelphia, PA, USA, 1982. [Google Scholar]
- Balazs, E.A.; Watson, D.; Duff, I.F.; Roseman, S. Hyaluronic acid in synovial fluid. I. Molecular parameters of hyaluronic acid in normal and arthritis human fluids. Arthritis Rheum. 1967, 10, 357–376. [Google Scholar]
- Ogston, A.G.; Stanier, J.E. The physiological function of hyaluronic acid in synovial fluid; viscous, elastic and lubricant properties. J. Physiol. 1953, 119, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Liu, C.; Thormann, E.; Dedinaite, A. Hyaluronan and phospholipid association in biolubrication. Biomacromolecules 2013, 14, 4198–4206. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.; Bracco, P.; del Prever, E.B.; Luda, M.P.; Trossarelli, L. Analysis of products diffused into UHMWPE prosthetic components in vivo. Biomaterials 2001, 22, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Mazzucco, D.; McKinley, G.; Scott, R.D.; Spector, M. Rheology of joint fluid in total knee arthroplasty patients. J. Orthop. Res. 2002, 20, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Mazzucco, D.; Scott, R.; Spector, M. Composition of joint fluid in patients undergoing total knee replacement and revision arthroplasty: Correlation with flow properties. Biomaterials 2004, 25, 4433–4445. [Google Scholar] [CrossRef] [PubMed]
- Gale, L.R.; Chen, Y.; Hills, B.A.; Crawford, R. Boundary lubrication of joints: Characterization of surface-active phospholipids found on retrieved implants. Acta Orthop. 2007, 78, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, G.; Graichen, F.; Rohlmann, A.; Verdonschot, N.; van Lenthe, G.H. Frictional heating of total hip implants. Part 1: Measurements in patients. J. Biomech. 2001, 34, 421–428. [Google Scholar]
- Bergmann, G.; Graichen, F.; Rohlmann, A.; Verdonschot, N.; van Lenthe, G.H. Frictional heating of total hip implants. Part 2: Finite element study. J. Biomech. 2001, 34, 429–435. [Google Scholar]
- Ghosh, S.; Choudhury, D.; Das, N.S.; Pingguan-Murphy, B. Tribological role of synovial fluid compositions on artificial joints—A systematic review of the last 10 years. Lubr. Sci. 2014, 26, 387–410. [Google Scholar] [CrossRef]
- Bonnevie, E.D.; Baro, V.J.; Wang, L.; Burris, D.L. Fluid load support during localized indentation of cartilage with a spherical probe. J. Biomech. 2012, 45, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Caligaris, M.; Ateshian, G.A. Effects of sustained interstitial fluid pressurization under migrating contact area, and boundary lubrication by synovial fluid, on cartilage friction. Osteoarthritis Cartilage 2008, 16, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Delecrin, J.; Oka, M.; Takahashi, S.; Yamamuro, T.; Nakamura, T. Changes in joint fluid after total arthroplasty. A quantitative study on the rabbit knee joint. Clin. Orthop. Relat. Res. 1994, 307, 240–249. [Google Scholar]
- Campbell, P.; Ebramzadeh, E.; Nelson, S.; Takamura, K.; De Smet, K.; Amstutz, H.C. Histological features of pseudotumor-like tissues from metal-on-metal hips. Clin. Orthop. Relat. Res. 2010, 468, 2321–2327. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.P.; Willert, H.G.; Campbell, P.A.; Learmonth, I.D.; Case, C.P. An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements. J. Bone Joint Surg. 2005, 87, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Grammatopoulos, G.; Pandit, H.; Kamali, A.; Maggiani, F.; Glyn-Jones, S.; Gill, H.S.; Murray, D.W.; Athanasou, N. The correlation of wear with histological features after failed hip resurfacing arthroplasty. J. Bone Joint Surg. 2013, 95, e81. [Google Scholar] [CrossRef] [PubMed]
- Howie, D.W.; Cain, C.M.; Cornish, B.L. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J. Bone Joint Surg. 1991, 73, 29–32. [Google Scholar]
- Willert, H.G.; Buchhorn, G.H.; Fayyazi, A.; Flury, R.; Windler, M.; Koster, G.; Lohmann, C.H. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints. A clinical and histomorphological study. J. Bone Joint Surg. 2005, 87, 28–36. [Google Scholar] [CrossRef]
- Hirohata, K.; Kobayashi, I. Fine structures of the synovial tissues in rheumatoid arthritis. Kobe J. Med. Sci. 1964, 10, 195–225. [Google Scholar] [PubMed]
- Haraoui, B.; Pelletier, J.P.; Cloutier, J.M.; Faure, M.P.; Martel-Pelletier, J. Synovial membrane histology and immunopathology in rheumatoid arthritis and osteoarthritis. In vivo effects of antirheumatic drugs. Arth. Rheum. 1991, 34, 153–163. [Google Scholar]
- Walker, P.S. A comparison of normal and artificial human joints. Acta Orthop. Belg. 1973, 39, 43–54. [Google Scholar] [PubMed]
- Jay, G.D.; Waller, K.A. The biology of lubricin: Near frictionless joint motion. Matrix Boil. J. Int. Soc. Matrix Biol. 2014, 39, 17–24. [Google Scholar] [CrossRef]
- Swann, D.A.; Silver, F.H.; Slayter, H.S.; Stafford, W.; Shore, E. The molecular structure and lubricating activity of lubricin isolated from bovine and human synovial fluids. Biochem. J. 1985, 225, 195–201. [Google Scholar] [PubMed]
- Fan, J.; Myant, C.; Underwood, R.; Cann, P. Synovial fluid lubrication of artificial joints: Protein film formation and composition. Faraday Discuss. 2012, 156, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Gispert, M.P.; Serro, A.P.; Colaco, R.; Saramago, B. Friction and wear mechanisms in hip prosthesis: Comparison of joint materials behaviour in several lubricants. Wear 2006, 260, 149–158. [Google Scholar] [CrossRef]
- Roba, M.; Bruhin, C.; Ebneter, U.; Ehrbar, R.; Crockett, R.; Spencer, N.D. Latex on glass: An appropriate model for cartilage-lubrication studies? Tribol. Lett. 2010, 38, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.; Essner, A.; Schmidig, G. The effects of lubricant composition on in vitro wear testing of polymeric acetabular components. J. Biomed. Mater. Res. B Appl. Biomater. 2004, 68, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Brandt, J.M.; Briere, L.K.; Marr, J.; MacDonald, S.J.; Bourne, R.B.; Medley, J.B. Biochemical comparisons of osteoarthritic human synovial fluid with calf sera used in knee simulator wear testing. J. Biomed. Mater. Res. A 2010, 94, 961–971. [Google Scholar] [PubMed]
- Reinders, J.; Sonntag, R.; Kretzer, J.P. Synovial fluid replication in knee wear testing: An investigation of the fluid volume. J. Orthop. Res. 2015, 33, 92–97. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).