
Pathophysiology of Chylous Anasarca Caused by Lymphatic Occlusion: A Case Report and Review of the Literature

 ,
,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
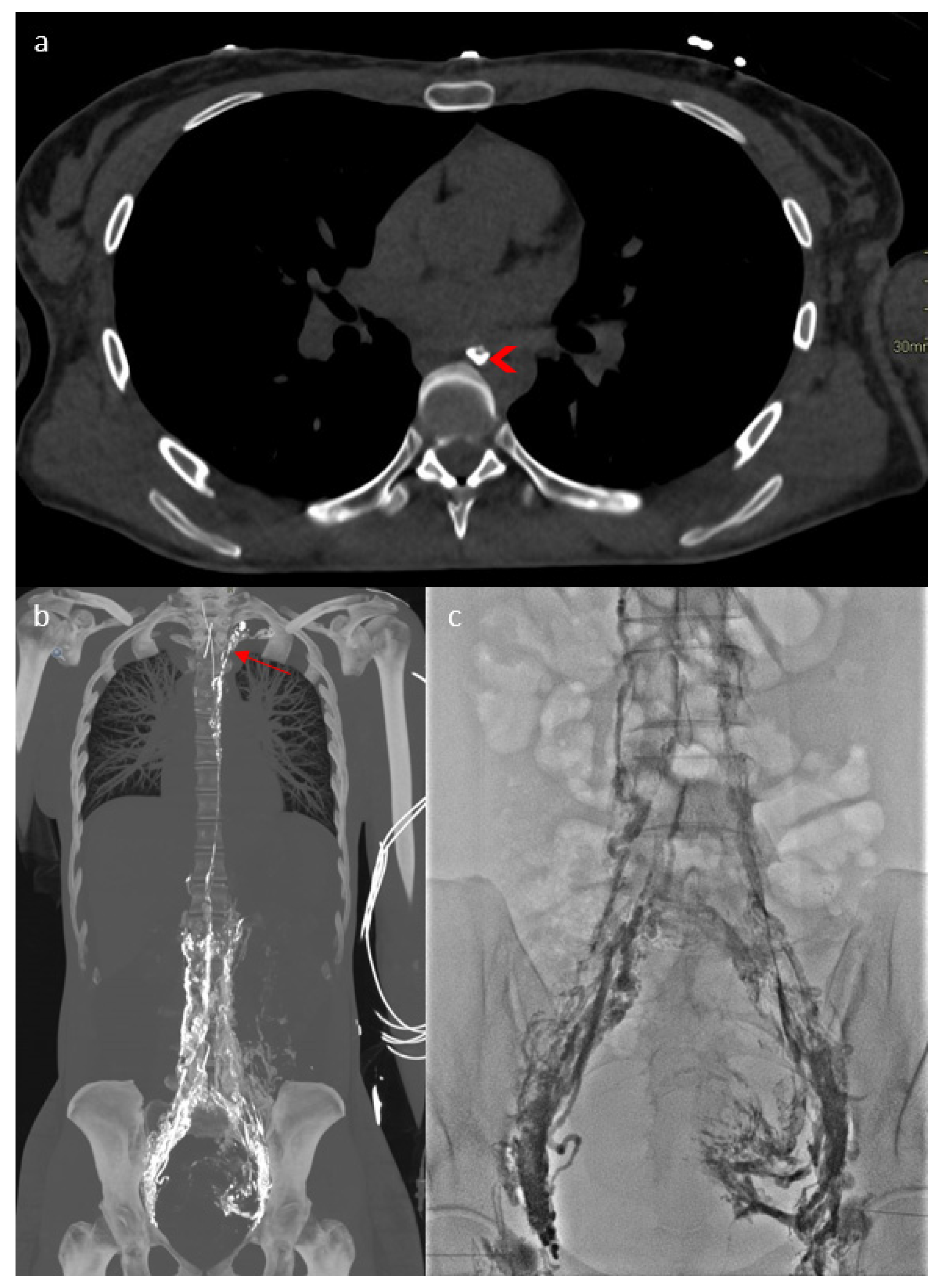
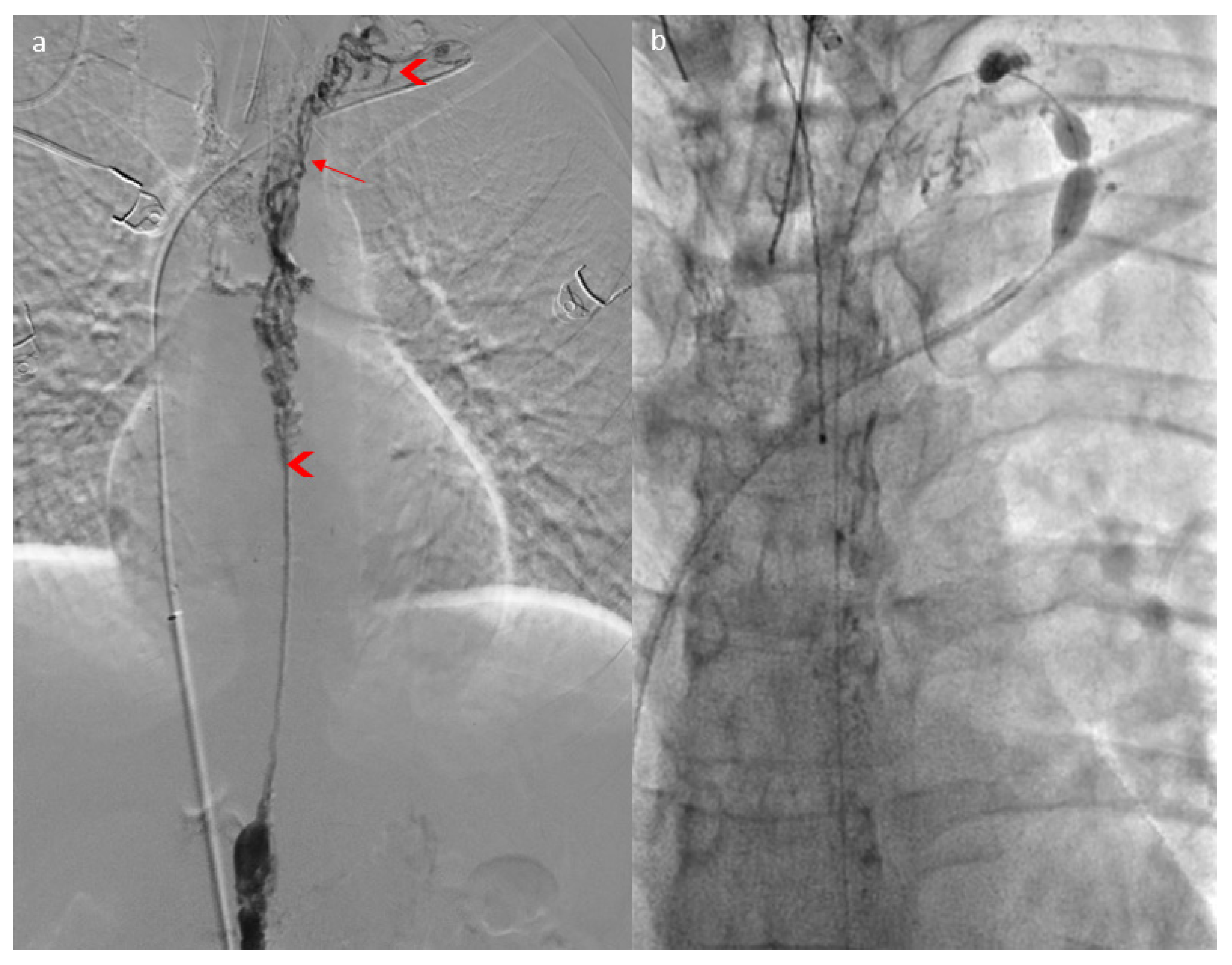
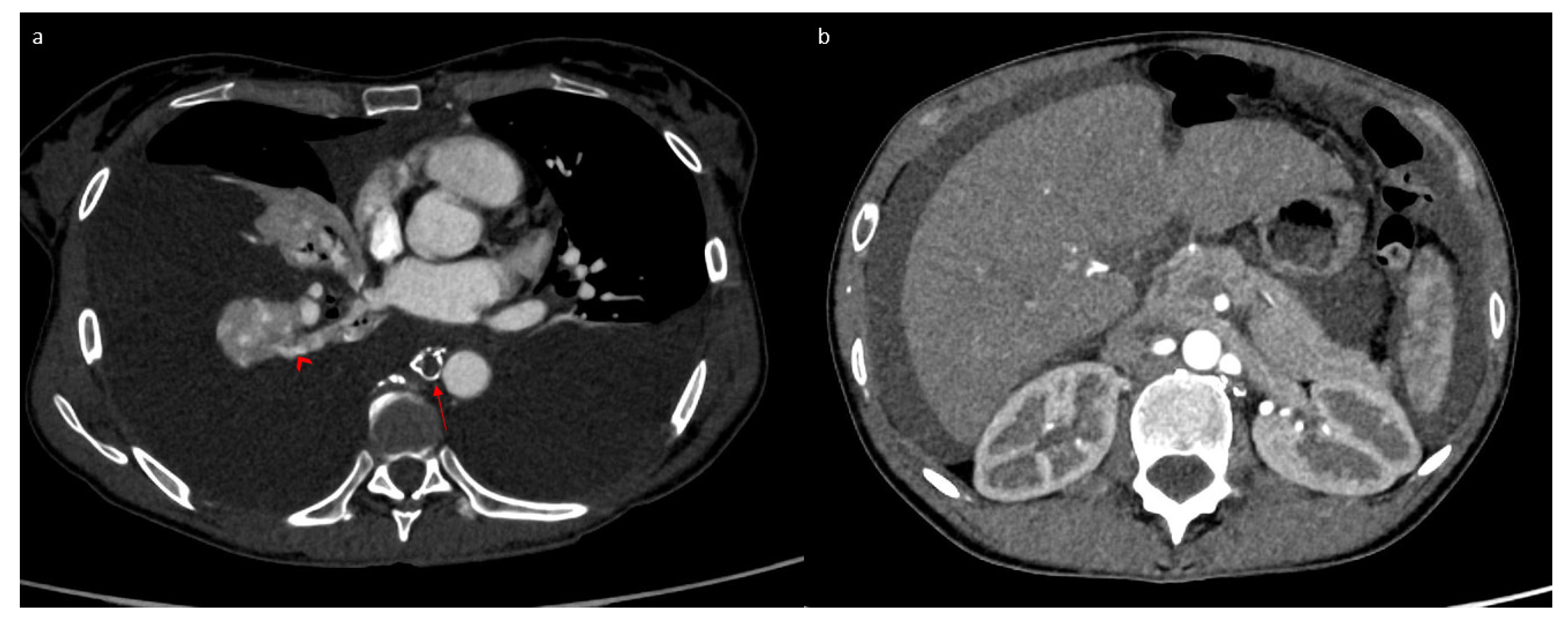
2. Case Report
3. Discussion
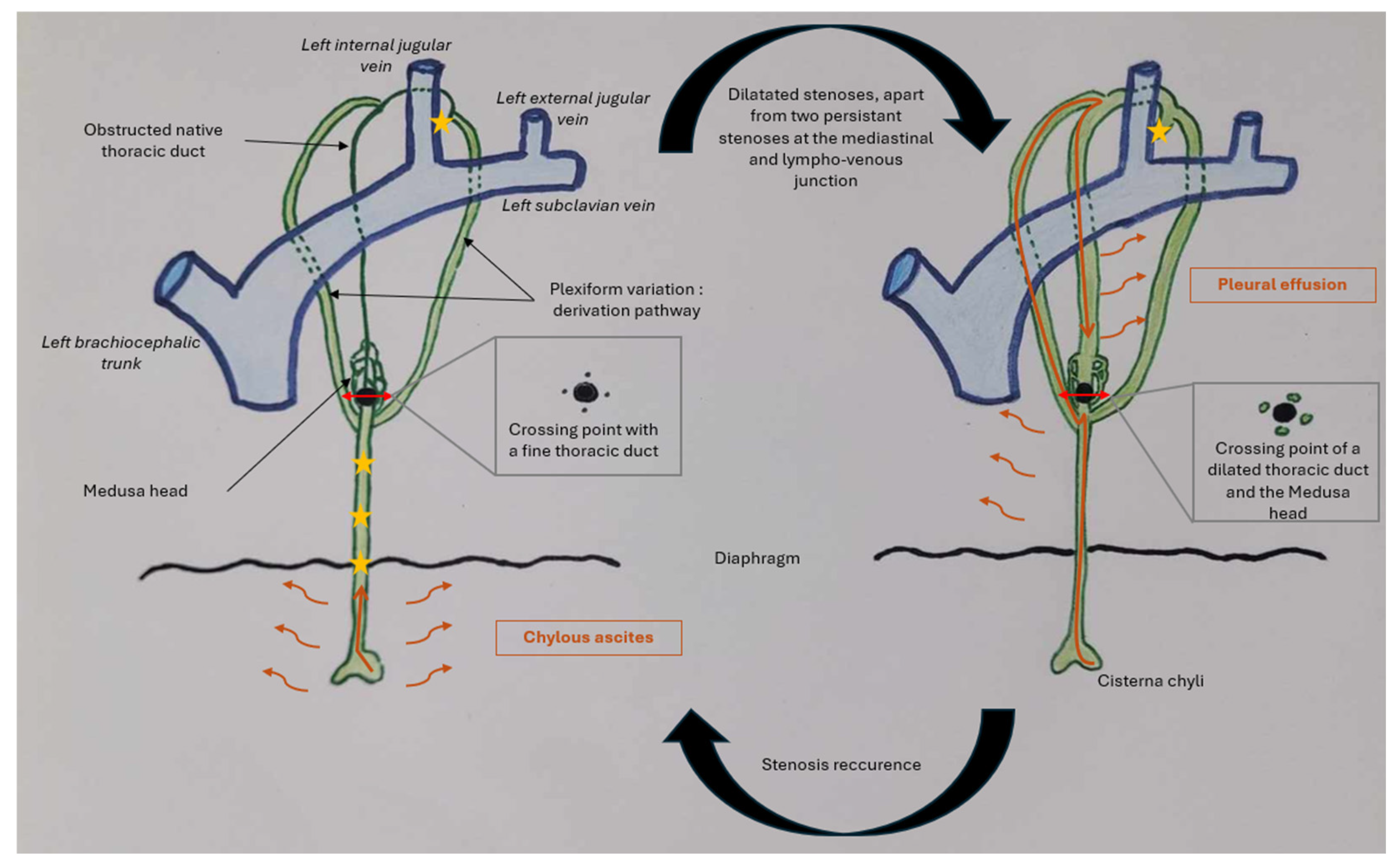
3.1. Case Discussion and Physiopathological Hypothesis
3.2. Comprehensive Review of the Literature About CCLA Etiologies and Therapeutic Strategies
3.2.1. Definition
3.2.2. Etiologies
- Congenital obstructions, with a dysplastic thoracic duct or stenosis of the lympho-venous junction; many advances have been made in this domain, and genetic mutations have been identified [5].
- Acquired obstructions, with accidental thoracic duct ligation during thoracic surgery.
- Functional anomalies, with high central venous pressure preventing lymphatic drainage from the thoracic duct into the venous system.
3.2.3. Imaging
3.2.4. Treatments
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 4D-CT | Four-Dimensional Computed Tomography |
| CCLAs | Central Conducting Lymphatic Anomalies |
| CCLDs | Central Conducting Lymphatic Disorders |
References
- Trenor, C.C.; Chaudry, G. Complex Lymphatic Anomalies. Semin. Pediatr. Surg. 2014, 23, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Laje, P.; Dori, Y.; Smith, C.; Pinto, E.; Taha, D.; Maeda, K. Surgical Management of Central Lymphatic Conduction Disorders: A Review. J. Pediatr. Surg. 2024, 59, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Laje, P.; Dori, Y.; Smith, C.; Maeda, K. Surgical Management of Thoracic Duct Anomalies. Semin. Pediatr. Surg. 2024, 33, 151421. [Google Scholar] [CrossRef]
- Laje, P.; Dori, Y.; Smith, C.; Maeda, K. Surgical Management of Chronic Lymphatic Pleural Effusions and Chronic Lymphatic Ascites. Lymphat. Conduct. Disord. 2024, 33, 151420. [Google Scholar] [CrossRef] [PubMed]
- Garlisi Torales, L.D.; Sempowski, B.A.; Krikorian, G.L.; Woodis, K.M.; Paulissen, S.M.; Smith, C.L.; Sheppard, S.E. Central Conducting Lymphatic Anomaly: From Bench to Bedside. J. Clin. Investig. 2024, 134, e172839. [Google Scholar] [CrossRef]
- Chen, E.; Itkin, M. Thoracic Duct Embolization for Chylous Leaks. Semin. Interv. Radiol. 2011, 28, 63–74. [Google Scholar] [CrossRef]
- Nair, S.K.; Petko, M.; Hayward, M.P. Aetiology and Management of Chylothorax in Adults. Eur. J. Cardiothorac. Surg. 2007, 32, 362–369. [Google Scholar] [CrossRef]
- Wohlgemuth, W.A.; Brill, R.; Dendl, L.M.; Stangl, F.; Stoevesandt, D.; Schreyer, A.G. Abdominal Lymphatic Malformations. Radiologe 2018, 58, 29–33. [Google Scholar] [CrossRef]
- Chalret du Rieu, M.; Baulieux, J.; Rode, A.; Mabrut, J.Y. Prise en charge du chylothorax postopératoire. J. De Chir. Viscérale 2011, 148, 392–399. [Google Scholar] [CrossRef]
- Rabattu, P.Y.; Sole Cruz, E.; El Housseini, N.; El Housseini, A.; Bellier, A.; Verot, P.L.; Cassiba, J.; Quillot, C.; Faguet, R.; Chaffanjon, P.; et al. Anatomical Study of the Thoracic Duct and Its Clinical Implications in Thoracic and Pediatric Surgery, a 70 Cases Cadaveric Study. Surg. Radiol. Anat. 2021, 43, 1481–1489. [Google Scholar] [CrossRef]
- Lippi, G.; Favaloro, E.J.; Cervellin, G. Hemostatic Properties of the Lymph: Relationships with Occlusion and Thrombosis. Semin. Thromb. Hemost. 2012, 38, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A.; Smith, C.; Krishnamurthy, G.; Escobar, F.; Biko, D.; Dori, Y. Characterization and Treatment of Thoracic Duct Obstruction in Patients with Lymphatic Flow Disorders. Catheter. Cardiovasc. Interv. 2023, 101, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Snyder, E.J.; Sarma, A.; Borst, A.J.; Tekes, A. Lymphatic Anomalies in Children: Update on Imaging Diagnosis, Genetics, and Treatment. Am. J. Roentgenol. 2022, 218, 1089–1101. [Google Scholar] [CrossRef] [PubMed]
- Ghelfi, J.; Frandon, J.; Itkin, M.; Guiu, B.; Decaens, T. Acute Central Lymphatic Obstruction Associated with Decompensated Cirrhotic Ascites and Hydrothorax. J. Vasc. Interv. Radiol. 2023, 34, 1626–1629. [Google Scholar] [CrossRef]
- Johnson, O.W.; Chick, J.F.B.; Chauhan, N.R.; Fairchild, A.H.; Fan, C.-M.; Stecker, M.S.; Killoran, T.P.; Suzuki-Han, A. The Thoracic Duct: Clinical Importance, Anatomic Variation, Imaging, and Embolization. Eur. Radiol. 2016, 26, 2482–2493. [Google Scholar] [CrossRef]
- Mathivet, A.; Frandon, J.; Quéré, I.; Ghelfi, J.; Gris, J.-C.; Prudhomme, M.; Bertrand, M.M. L’anatomie du conduit thoracique. J. D’imagerie Diagn. Interv. 2025, S254334312500051X. [Google Scholar] [CrossRef]
- Loukas, M.; Wartmann, C.T.; Louis, R.G., Jr.; Tubbs, R.S.; Salter, E.G.; Gupta, A.A.; Curry, B. Cisterna Chyli: A Detailed Anatomic Investigation. Clin. Anat. 2007, 20, 683–688. [Google Scholar] [CrossRef]
- Moazzam, S.; O’Hagan, L.A.; Clarke, A.R.; Itkin, M.; Phillips, A.R.J.; Windsor, J.A.; Mirjalili, S.A. The Cisterna Chyli: A Systematic Review of Definition, Prevalence, and Anatomy. Am. J. Physiol. -Heart Circ. Physiol. 2022, 323, H1010–H1018. [Google Scholar] [CrossRef]
- Defize, I.L.; Schurink, B.; Weijs, T.J.; Roeling, T.A.P.; Ruurda, J.P.; van Hillegersberg, R.; Bleys, R.L.A.W. The Anatomy of the Thoracic Duct at the Level of the Diaphragm: A Cadaver Study. Ann. Anat. 2018, 217, 47–53. [Google Scholar] [CrossRef]
- Davis, H.K. A Statistical Study of the Thoracic Duct in Man. Am. J. Anat. 1915, 17, 211–244. [Google Scholar] [CrossRef]
- Adachi, B. Der Ductus Thoracicus Der Japaner. In Das lymphgefasssystem der Japaner; Kenkyusha: Tokyo, Japan, 1953; pp. 1–83. [Google Scholar]
- Phang, K.; Bowman, M.; Phillips, A.; Windsor, J. Review of Thoracic Duct Anatomical Variations and Clinical Implications. Clin. Anat. 2014, 27, 637–644. [Google Scholar] [CrossRef]
- Ratnayake, C.B.B.; Escott, A.B.J.; Phillips, A.R.J.; Windsor, J.A. The Anatomy and Physiology of the Terminal Thoracic Duct and Ostial Valve in Health and Disease: Potential Implications for Intervention. J. Anat. 2018, 233, 1–14. [Google Scholar] [CrossRef] [PubMed]
- O’Hagan, L.A.; Windsor, J.A.; Itkin, M.; Russell, P.S.; Phillips, A.R.J.; Mirjalili, S.A. The Lymphovenous Junction of the Thoracic Duct: A Systematic Review of Its Structural and Functional Anatomy. Lymphat. Res. Biol. 2021, 19, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Bellier, A.; Pardo Vargas, J.S.; Cassiba, J.; Desbrest, P.; Guigui, A.; Chaffanjon, P. Anatomical Variations in Distal Portion of the Thoracic Duct—A Systematic Review. Clin. Anat. 2020, 33, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Sato, I. Morphological and Histological Analysis of the Thoracic Duct at the Jugulo-Subclavian Junction in Japanese Cadavers. Clin. Anat. 1997, 10, 163–172. [Google Scholar] [CrossRef]
- De-xin, Y.; Xiang-xing, M.; Xiao-ming, Z.; Qing, W.; Chuan-fu, L. Morphological Features and Clinical Feasibility of Thoracic Duct: Detection with Nonenhanced Magnetic Resonance Imaging at 3.0 T. J. Magn. Reson. Imaging 2010, 32, 94–100. [Google Scholar] [CrossRef]
- Benjamin, J.; O’Leary, C.; Hur, S.; Gurevich, A.; Klein, W.M.; Itkin, M. Imaging and Interventions for Lymphatic and Lymphatic-Related Disorders. Radiology 2023, 307, e220231. [Google Scholar] [CrossRef]
- Guillemard, S.; Frandon, J.; Ghelfi, J.; Quéré, I.; Adham, S.; Belgrado, J.-P.; Kovacsik, H.; Mestre, S. Exploration Fonctionnelle et Imagerie Du Système Lymphatique. La Presse Médicale Form. 2023, 4, 353–368. [Google Scholar] [CrossRef]
- Okuda, I.; Udagawa, H.; Takahashi, J.; Yamase, H.; Kohno, T.; Nakajima, Y. Magnetic Resonance-Thoracic Ductography: Imaging Aid for Thoracic Surgery and Thoracic Duct Depiction Based on Embryological Considerations. Gen. Thorac. Cardiovasc. Surg. 2009, 57, 640–646. [Google Scholar] [CrossRef]
- Lopez-Gutierrez, J.C.; Tovar, J.A. Chylothorax and Chylous Ascites: Management and Pitfalls. Semin. Pediatr. Surg. 2014, 23, 298–302. [Google Scholar] [CrossRef]
- Dulmovits, B.M.; Taha, D.K. Neonatal Perspective on Central Lymphatic Disorders. Semin. Pediatr. Surg. 2024, 33, 151424. [Google Scholar] [CrossRef]
- Chen, L.; Yu, S.; Chen, S.; Han, Z.; Chen, S.; Chen, M.; Lin, J.; Kang, M. Application of Imaging Technique in Thoracic Duct Anatomy. Ann. Palliat. Med. 2020, 9, 1249256. [Google Scholar] [CrossRef] [PubMed]
- Toliyat, M.; Singh, K.; Sibley, R.C.; Chamarthy, M.; Kalva, S.P.; Pillai, A.K. Interventional Radiology in the Management of Thoracic Duct Injuries: Anatomy, Techniques and Results. Clin. Imaging 2017, 42, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Ghelfi, J.; Brusset, B.; Thony, F.; Decaens, T. Successful Management of Refractory Ascites in Non-TIPSable Patients Using Percutaneous Thoracic Duct Stenting. J. Hepatol. 2022, 76, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Taghinia, A.H.; Upton, J.; Trenor, C.C.; Alomari, A.I.; Lillis, A.P.; Shaikh, R.; Burrows, P.E.; Fishman, S.J. Lymphaticovenous Bypass of the Thoracic Duct for the Treatment of Chylous Leak in Central Conducting Lymphatic Anomalies. J. Pediatr. Surg. 2019, 54, 562–568. [Google Scholar] [CrossRef]
- Reisen, B.; Kovach, S.J.; Levin, L.S.; Pinto, E.; Nadolski, G.J.; Itkin, M.; Dori, Y.; Laje, P. Thoracic Duct-to-Vein Anastomosis for the Management of Thoracic Duct Outflow Obstruction in Newborns and Infants: A CASE Series. J. Pediatr. Surg. 2020, 55, 234–239. [Google Scholar] [CrossRef]
- Weinzierl, A.; Grünherz, L.; Puippe, G.D.; Gnannt, R.; von Reibnitz, D.; Giovanoli, P.; Vetter, D.; Möhrlen, U.; Wildgruber, M.; Müller, A.; et al. Microsurgical Central Lymphatic Reconstruction-the Role of Thoracic Duct Lymphovenous Anastomoses at Different Anatomical Levels. Front. Surg. 2024, 11, 1415010. [Google Scholar] [CrossRef]
- Bundy, J.J.; Shin, D.S.; Chick, J.F.B.; Monsky, W.L.; Jones, S.T.; List, J.; Hage, A.N.; Vaidya, S.S. Percutaneous Extra-Anatomic Lymphovenous Bypass Creation: Toward Treatment of Central Conducting Lymphatic Obstructions. Cardiovasc. Interv. Radiol. 2020, 43, 1392–1397. [Google Scholar] [CrossRef]
- Hayashida, K.; Yamakawa, S.; Shirakami, E. Lymphovenous Anastomosis for the Treatment of Persistent Congenital Chylothorax in a Low-Birth-Weight Infant: A Case Report. Medicine 2019, 98, e17575. [Google Scholar] [CrossRef]
- Ishiura, R.; Mitsui, K.; Danno, K.; Banda, C.H.; Inoue, M.; Narushima, M. Successful Treatment of Large Abdominal Lymphatic Malformations and Chylous Ascites with Intra-Abdominal Lymphovenous Anastomosis. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 9, 499–503. [Google Scholar] [CrossRef]
- Melduni, R.M.; Oh, J.K.; Bunch, T.J.; Sinak, L.J.; Gloviczki, P. Reconstruction of Occluded Thoracic Duct for Treatment of Chylopericardium: A Novel Surgical Therapy. J. Vasc. Surg. 2008, 48, 1600–1602. [Google Scholar] [CrossRef]
- Miller, T.J.; Gilstrap, J.N.; Maeda, K.; Rockson, S.; Nguyen, D.H. Correction of Complete Thoracic Duct Obstruction with Lymphovenous Bypass: A Case Report. Microsurgery 2019, 39, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Othman, S.; Azoury, S.C.; Klifto, K.; Toyoda, Y.; Itkin, M.; Kovach, S.J. Microsurgical Thoracic Duct Lymphovenous Bypass in the Adult Population. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3875. [Google Scholar] [CrossRef] [PubMed]
- Rezkalla, J.; Husain, M.; Slack, G.; Sinha, S. Novel Use of a SynovisTM Coupler Device for a Surgical Lymphovenous Anastomosis for the Treatment of Refractory Chylothorax in a Patient with Central Lymphatic Flow Disorder. Clin. Case Rep. 2022, 10, e05636. [Google Scholar] [CrossRef] [PubMed]
- Veziant, J.; Sakka, L.; Galvaing, G.; Tardy, M.M.; Cassagnes, L.; Filaire, M. Lymphovenous Anastomosis for Recurrent Swelling Syndrome and Chylous Effusion Due to Cervical Thoracic Duct Cyst. J. Vasc. Surg. 2015, 62, 1068–1070. [Google Scholar] [CrossRef]
- Weissler, J.M.; Cho, E.H.; Koltz, P.F.; Carney, M.J.; Itkin, M.; Laje, P.; Levin, L.S.; Dori, Y.; Kanchwala, S.K.; Kovach, S.J. Lymphovenous Anastomosis for the Treatment of Chylothorax in Infants: A Novel Microsurgical Approach to a Devastating Problem. Plast. Reconstr. Surg. 2018, 141, 1502–1507. [Google Scholar] [CrossRef]
- Woo, S.J.; Hur, S.; Kim, H.S.; Chang, H.; Kim, J.-Y.; Park, S.J.; Jin, U.S. Hybrid Lymphovenous Anastomosis Surgery Guided by Intraoperative Mesenteric Intranodal Lymphangiography for Refractory Nontraumatic Chylous Ascites: A Case Report. Arch. Plast. Surg. 2024, 51, 130–134. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathivet, A.; Bertrand, M.; Quere, I.; Gris, J.-C.; Ghelfi, J.; Frandon, J. Pathophysiology of Chylous Anasarca Caused by Lymphatic Occlusion: A Case Report and Review of the Literature. J. Pers. Med. 2025, 15, 216. https://doi.org/10.3390/jpm15060216
Mathivet A, Bertrand M, Quere I, Gris J-C, Ghelfi J, Frandon J. Pathophysiology of Chylous Anasarca Caused by Lymphatic Occlusion: A Case Report and Review of the Literature. Journal of Personalized Medicine. 2025; 15(6):216. https://doi.org/10.3390/jpm15060216
Chicago/Turabian StyleMathivet, Antoine, Martin Bertrand, Isabelle Quere, Jean-Christophe Gris, Julien Ghelfi, and Julien Frandon. 2025. "Pathophysiology of Chylous Anasarca Caused by Lymphatic Occlusion: A Case Report and Review of the Literature" Journal of Personalized Medicine 15, no. 6: 216. https://doi.org/10.3390/jpm15060216
APA StyleMathivet, A., Bertrand, M., Quere, I., Gris, J.-C., Ghelfi, J., & Frandon, J. (2025). Pathophysiology of Chylous Anasarca Caused by Lymphatic Occlusion: A Case Report and Review of the Literature. Journal of Personalized Medicine, 15(6), 216. https://doi.org/10.3390/jpm15060216