
Prophylactic Antibiotics before Gynecologic Surgery: A Comprehensive Review of Guidelines

 ,
,  ,
,
Abstract
1. Introduction
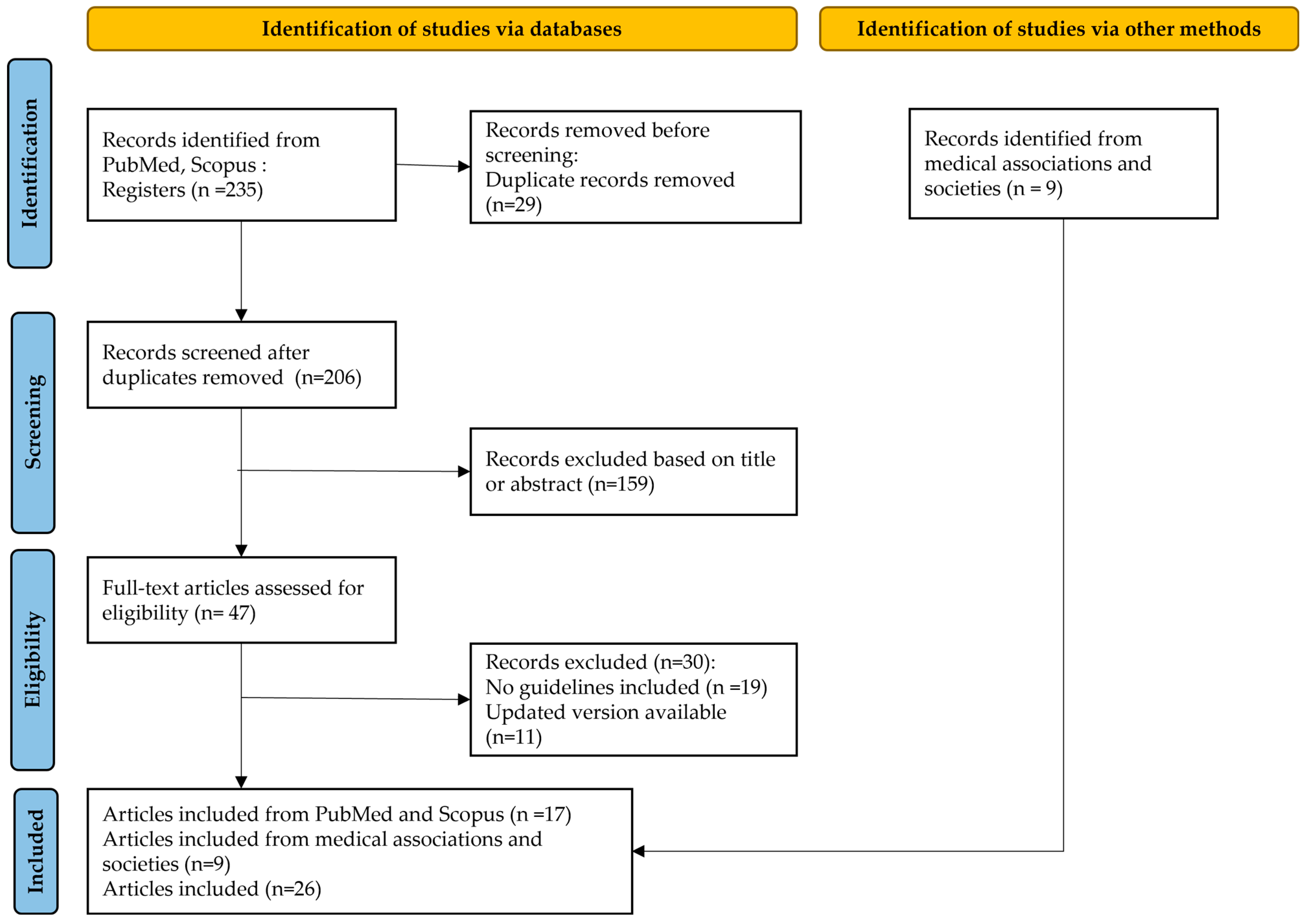
2. Materials and Methods
3. Results
3.1. Antibiotic Prophylaxis According to the Type of Gynecologic Procedure
3.1.1. Vaginal, Abdominal, or Laparoscopic Hysterectomy
3.1.2. Laparotomy without Entry into Bowel or Vagina
3.1.3. Laparoscopy without Entry into Bowel or Vagina
3.1.4. Diagnostic or Operative Hysteroscopy
3.1.5. Hysterosalpingography
3.1.6. Intrauterine Device Insertion
3.1.7. Cervical Tissue Excision Procedures (e.g., Large Loop Excision of Transformation Zone)
3.1.8. Uterine Evacuation
3.1.9. Endometrial Biopsy
3.1.10. Vulvectomy
3.1.11. Urogynecology Procedures
3.1.12. Urodynamic Studies
3.2. Special Cases in Antibiotic Prophylaxis
3.2.1. Hypersensitivity to Penicillin
3.2.2. Obese Patients
3.2.3. Prolonged Procedures
3.2.4. Excessive Blood Loss
3.2.5. Colonization or High Risk of Colonization with MRSA
3.3. Time of Administration of Antibiotic Prophylaxis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Surgical Site Infection Event (SSI). Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf (accessed on 24 August 2023).
- Surgical Site Infections. Available online: https://www.ecdc.europa.eu/en/surgical-site-infections (accessed on 15 June 2023).
- Kulkarni, S.P.; Kothari, O. Surgical Site Infection in Obstetric and Gynecological Surgeries: A Prospective Observational Study. Cureus 2023, 15, e34855. [Google Scholar] [CrossRef]
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Silver, L.C.; Jarvis, W.R. Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am. J. Infect. Control 1999, 27, 97–132. [Google Scholar] [CrossRef] [PubMed]
- Enzler, M.J.; Berbari, E.; Osmon, D.R. Antimicrobial Prophylaxis in Adults. Mayo Clin. Proc. 2011, 86, 686–701. [Google Scholar] [CrossRef]
- Okasha, H. Risk Factors and Key Principles for Prevention of Surgical Site Infections. In Surgical Infections–Some Facts; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef]
- Munckhof, W. Antibiotics for Surgical Prophylaxis. Aust. Prescr. 2005, 28, 38–40. [Google Scholar] [CrossRef]
- ACOG Practice Bulletin No. 195: Prevention of Infection After Gynecologic Procedures. Obstet. Gynecol. 2018, 131, e172–e189. [CrossRef]
- Van Eyk, N.; van Schalkwyk, J. No. 275-Antibiotic Prophylaxis in Gynaecologic Procedures. J. Obstet. Gynaecol. Can. 2018, 40, e723–e733. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Auboyer, C.; Boisson, M.; Dupont, H.; Gauzit, R.; Kitzis, M.; Leone, M.; Lepape, A.; Mimoz, O.; Montravers, P.; et al. Antibioprophylaxis in Surgery and Interventional Medicine (Adult Patients). Update 2017. Anaesth. Crit. Care Pain Med. 2019, 38, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.W.; Houck, P.M.; Surgical Infection Prevention Guidelines Writers Workgroup; American Academy of Orthopaedic Surgeons; American Association of Critical Care Nurses; American Association of Nurse Anesthetists; American College of Surgeons; American College of Osteopathic Surgeons; American Geriatrics Society; American Society of Anesthesiologists; et al. Antimicrobial Prophylaxis for Surgery: An Advisory Statement from the National Surgical Infection Prevention Project. Clin. Infect. Dis. 2004, 38, 1706–1715. [Google Scholar] [CrossRef]
- Prophylactic Antibiotics in Obstetrics and Gynaecology. Available online: https://ranzcog.edu.au/wp-content/uploads/2022/05/Prophylactic-Antibiotics-in-Obstetrics-and-Gynaecology.pdf (accessed on 24 August 2023).
- Surgical Antibiotic Prophylaxis Guideline. Available online: https://thewomens.r.worldssl.net/images/uploads/downloadable-records/clinical-guidelines/surgical-antibiotic-prophylaxis-guideline_280720.pdf (accessed on 24 August 2023).
- Del Toro López, M.D.; Arias Díaz, J.; Balibrea, J.M.; Benito, N.; Canut Blasco, A.; Esteve, E.; Horcajada, J.P.; Ruiz Mesa, J.D.; Manuel Vázquez, A.; Muñoz Casares, C.; et al. Executive Summary of the Consensus Document of the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) and of the Spanish Association of Surgeons (AEC) in Antibiotic Prophylaxis in Surgery. Cir. Esp. (Engl. Ed.) 2021, 99, 11–26. [Google Scholar] [CrossRef]
- Nelson, G.; Fotopoulou, C.; Taylor, J.; Glaser, G.; Bakkum-Gamez, J.; Meyer, L.A.; Stone, R.; Mena, G.; Elias, K.M.; Altman, A.D.; et al. Enhanced Recovery after Surgery (ERAS®) Society Guidelines for Gynecologic Oncology: Addressing Implementation Challenges—2023 Update. Gynecol. Oncol. 2023, 173, 58–67. [Google Scholar] [CrossRef]
- Guideline No 3 Prophylactic Antibiotics in Gynecologic Surgeries. Available online: https://www.eof.gr/c/document_library/get_file?p_l_id=34765&folderId=776074&name=DLFE-3203.pdf (accessed on 24 August 2023).
- Mladenovic Segedi, L.; Segedi, D.; Radaković, J.; Ilić, M.; Kojić, S. The Guidelines on Antibiotic Application in Gynaecological Oncology. Arch. Oncol. 2005, 13, 83–85. [Google Scholar] [CrossRef]
- Deffieux, X.; de Rochambeau, B.; Chene, G.; Gauthier, T.; Huet, S.; Lamblin, G.; Agostini, A.; Marcelli, M.; Golfier, F. Hysterectomy for Benign Disease: Clinical Practice Guidelines from the French College of Obstetrics and Gynecology. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 202, 83–91. [Google Scholar] [CrossRef]
- Surgical Site Infections: Prevention and Treatment. Available online: https://www.nice.org.uk/guidance/ng125/resources/surgical-site-infections-prevention-and-treatment-pdf-66141660564421 (accessed on 24 August 2023).
- Deffieux, X.; Gauthier, T.; Ménager, N.; Legendre, G.; Agostini, A.; Pierre, F. Prevention of the complications related to hysteroscopy: Guidelines for clinical practice. J. Gynécologie Obs. Biol. Reprod. 2013, 42, 1032–1049. [Google Scholar] [CrossRef]
- Altman, A.D.; Robert, M.; Armbrust, R.; Fawcett, W.J.; Nihira, M.; Jones, C.N.; Tamussino, K.; Sehouli, J.; Dowdy, S.C.; Nelson, G. Guidelines for Vulvar and Vaginal Surgery: Enhanced Recovery After Surgery Society Recommendations. Am. J. Obstet. Gynecol. 2020, 223, 475–485. [Google Scholar] [CrossRef]
- Sarfani, S.; Stone, C.A.; Murphy, G.A.; Richardson, D.R. Understanding Penicillin Allergy, Cross-Reactivity, and Antibiotic Selection in the Preoperative Setting. J. Am. Acad. Orthop. Surg. 2022, 30, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Pinto, B.; Blumenthal, K.G.; Courtney, L.; Mancini, C.M.; Jeffres, M.N. Assessment of the Frequency of Dual Allergy to Penicillins and Cefazolin: A Systematic Review and Meta-Analysis. JAMA Surg. 2021, 156, e210021. [Google Scholar] [CrossRef] [PubMed]
- Yong, P.J.; Thurston, J.; Singh, S.S.; Allaire, C. Guideline No. 386-Gynaecologic Surgery in the Obese Patient. J. Obstet. Gynaecol. Can. 2019, 41, 1356–1370.e7. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, J.E.; Toledo, P.; Soper, D.E.; Bradford, W.C.; Cruz, D.A.; Levy, B.S.; Lemieux, L.A. Consensus Bundle on Prevention of Surgical Site Infections After Major Gynecologic Surgery. Anesth. Analg. 2017, 124, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Position Paper on Prevention of Surgical Site Infections in Obstetric and Gynecological Surgery–JOG. Available online: http://www.gynaecology-obstetrics-journal.com/position-paper-on-prevention-of-surgical-site-infections-in-obstetric-and-gynecological-surgery/ (accessed on 30 January 2024).
- Fotopoulou, C.; Planchamp, F.; Aytulu, T.; Chiva, L.; Cina, A.; Ergönül, Ö.; Fagotti, A.; Haidopoulos, D.; Hasenburg, A.; Hughes, C.; et al. European Society of Gynaecological Oncology Guidelines for the Peri-Operative Management of Advanced Ovarian Cancer Patients Undergoing Debulking Surgery. Int. J. Gynecol. Cancer 2021, 31, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Mengistu, D.A.; Alemu, A.; Abdukadir, A.A.; Mohammed Husen, A.; Ahmed, F.; Mohammed, B.; Musa, I. Global Incidence of Surgical Site Infection Among Patients: Systematic Review and Meta-Analysis. Inquiry 2023, 60, 469580231162549. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Wei, Z.; Wang, W.; Tan, L.; Jiang, H.; Tian, L.; Cao, Y.; Nie, S. The Incidence and Distribution of Surgical Site Infection in Mainland China: A Meta-Analysis of 84 Prospective Observational Studies. Sci. Rep. 2014, 4, 6783. [Google Scholar] [CrossRef] [PubMed]
- Alemkere, G.; Tadeg, H.; Getahun, W.; Shewarega, W.; Agalu, A.; Joshi, M.P.; Konduri, N. Optimizing Prophylactic Antibiotic Use among Surgery Patients in Ethiopian Hospitals. J. Infect. Public. Health 2023, 16 (Suppl. S1), 82–89. [Google Scholar] [CrossRef] [PubMed]
- Standard Treatment Guidelines for General Hospital. Available online: https://e-library.moh.gov.et/library/wp-content/uploads/2021/07/STG-4th-edition-2021.pdf (accessed on 24 August 2023).

{kind=link}
| Class 1 wounds (Clean) | An uninfected operative wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tract is not entered. In addition, clean wounds are primarily closed and, if necessary, drained with closed drainage. Operative incisional wounds that follow nonpenetrating (blunt) trauma should be included in this category if they meet the criteria. |
| Class 2 wounds (Clean–contaminated) | An operative wound in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination. Specifically, operations involving the biliary tract, appendix, vagina, and oropharynx are included in this category, provided no evidence of infection or major break in technique is encountered. |
| Class 3 wounds (Contaminated) | Open, fresh, accidental wounds. In addition, operations with major breaks in sterile technique (e.g., open cardiac massage) or gross spillage from the gastrointestinal tract, and incisions in which acute nonpurulent inflammation is encountered are included in this category. |
| Class 4 wounds (Dirty–infected) | Old traumatic wounds with retained devitalized tissue and those that involve existing clinical infection or perforated viscera. This definition suggests that the organisms causing postoperative infection were present in the operative field before the operation. |
| Issued | The Royal Australian and New Zealand College of Obstetricians and Gynecologists (RANCOG) 2021 | American College of Obstetricians and Gynecologists (ACOG) 2018 | Society of Obstetricians and Gynecologists of Canada (SOGC) 2018 | Société Française d’ Anésthesie et de Réanimation (SFAR) 2017 | |
| Hysterectomy: Laparotomy Laparoscopy Vaginal | Cefazolin 2 g iv PLUS metronidazole 500 mg iv | Cefazolin 2 g iv | Single dose of first- or second-generation cephalosporin iv | Cefazolin 2 g iv Cefamandole 1.5 g iv Cefuroxime 1.5 g iv | |
| Laparotomy without entry into bowel or vagina | Cefazolin 2 g iv PLUS metronidazole 500 mg iv | Consider cefazolin 2 g iv | NR | NR | |
| Laparoscopy without entry into bowel or vagina | Not recommended | Not recommended | Not recommended | Not recommended | |
| Hysteroscopy: Diagnostic Operative | Not recommended | Not recommended | Not recommended | Not recommended | |
| Hysterosalpingography | Not recommended 1 | Not recommended 1 | Insufficient evidence 3 | Not recommended | |
| Intrauterine device insertion | Not recommended | Not recommended | Not recommended 4 | Not recommended | |
| Endometrial biopsy | NR | Not recommended | Insufficient evidence | Not recommended | |
| Cervical tissue excision procedures (e.g., Large loop excision of transformation zone) | Not recommended | Not recommended | NR | NR | |
| Uterine evacuation | Surgical termination of pregnancy when STIs have not been excluded: doxycycline 100 mg po before and 200 mg po after the procedure OR doxycycline 400 mg po with food 10–12 h prior to the procedure 2 | Suction D&C, D&E: Doxycycline 200 mg D&C for nonpregnancy indications: Not recommended | Induced (therapeutic) surgical abortion: Doxycycline 100 mg po pre-procedure PLUS 200 mg po post-procedure Surgery for a missed or incomplete abortion: Not recommended | Surgical termination of pregnancy: Not recommended | |
| Vulvectomy | NR | Cefazolin 2 g iv | NR | NR | |
| Urogynecology procedures | cefazolin 2 g iv PLUS metronidazole 500 mg iv | NR | NR | NR | |
| Vaginal sling placement | NR | Cefazolin 2 g iv | Single dose of first-generation cephalosporin iv | Aminopenicillin and β-lactamase inhibitor 2 g iv (for prolapse) | |
| Colporrhaphy | NR | Cefazolin 2 g iv | NR | NR | |
| Cystoscopy | NR | Not recommended | NR | Not recommended | |
| Urodynamic studies | NR | Not recommended | Not recommended 5 | Not recommended | |
| Issued | Surgical Antibiotic Prophylaxis Guideline at the Women’s in Parkville and in Sandringham 2020 | Hellenic Society of Obstetricians and Gynecologists (HSOG) 2013 | The guidelines on antibiotic application in gynecological Oncology (Serbia) 2005 | Surgical Infection Prevention Guideline Writers Workgroup (SIPGWW) 2004 | |
| Hysterectomy: Laparotomy Laparoscopic Vaginal | Cefazolin 2 g iv within 60 min (ideally 15–30 min) before surgical incision (repeat dose if procedure > 4 h) PLUS Metronidazole 500 mg iv within 120 min (ideally 15–30 min) before surgical incision | Laparotomy: First- or second-generation cephalosporin OR Amoxicillin–clavulanic acid Laparoscopic and vaginal: First-generation cephalosporin (cefazolin) | Abdominal: 1 g of first generation cephalosporin (cephazolin, cefotetan, or cefoxitin) in one or maximum three doses. im 1 h or iv 20–30 min prior to the procedure 13 Vaginal: 2 g of cephalosporin with anaerobic activity (Cefotaxime or Cephazolin) OR amikacin 500 mg | Cefazolin, cefotetan, cefoxitin, or cefuroxime 11 | |
| Laparotomy without entry into bowel or vagina | Cefazolin 2 g iv within 60 min (ideally 15–30 min) before surgical incision (repeat dose if procedure > 4 h) PLUS Metronidazole 500 mg IV within 60 min (ideally 15–30 min) before surgical incision | NR | NR | NR | |
| Laparoscopy without entry into bowel or vagina | Not recommended 8 | Not recommended | Not recommended unless major and lengthy operation | NR | |
| Hysteroscopy: Diagnostic Operative | Not recommended 9 | Not recommended | NR | NR | |
| Hysterosalpingography | Not recommended 9 | Not recommended 12 | NR | NR | |
| Intrauterine device placement | Not recommended 10 | Not recommended 10 | NR | NR | |
| Endometrial biopsy | Not recommended | Not recommended | NR | NR | |
| Cervical tissue excision procedures (e.g., Large loop excision of transformation zone) | NR | NR | NR | NR | |
| Surgical Termination of pregnancy | Screen patient for STIs: C. trachomatis, N. gonorrhoeae, M.genitalium, and bacterial vaginosis. Treat the woman and her partner(s) prior to termination of pregnancy. | Doxycycline 100 mg before and 200 mg after the procedure OR Doxycycline 400 mg before the procedure OR Metronidazole400 mg prior to the procedure and repeat 4 and 8 h after. | NR | NR | |
| Urogynecological procedures (mid-urethral sling/TVT, colposuspension, and vaginal prolapse surgery +/− mesh/SSF) | Cefazolin 2 g iv within 60 min before surgical incision PLUS Metronidazole 500 mg IV within 120 min before surgical incision | First-generation cephalosporin | NR | NR | |
| Urodynamic studies | Not recommended | ||||
| Issued | Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) and Spanish Association of Surgeons (AEC) 2020 | Enhanced Recovery After Surgery (ERAS) Society 2015, 2019, 2020, 2023 | Italian Society of Gynecology and Obstetrics (SIGO) 2020 | National Institute for Health and Care Excellence (NICE) 2019 | Consensus Bundle on Prevention of Surgical Site Infections After Major Gynecologic Surgery 2017 |
| Hysterectomy: Laparotomy Laparoscopy Vaginal | Cefazolin OR Cefotaxime OR amoxicillin– clavulanic acid | Cefazolin OR Amoxicillin– clavulanic acid | |||
| Laparotomy without entry into bowel or vagina | Recommended for clean procedures with implantation of foreign material, clean–contaminated, or contaminated procedures | NR | |||
| Laparoscopy without entry into bowel or vagina | Not recommended | Not recommended | |||
| Hysteroscopy: Diagnostic Operative | NR | NR | |||
| Hysterosalpingography | NR | NR | |||
| Intrauterine device insertion | NR | NR | |||
| Endometrial biopsy | NR | NR | |||
| Cervical tissue excision procedures (e.g., Large loop excision of transformation zone) | NR | NR | |||
| Uterine evacuation | Induced abortion or puerperal curettage: Doxycycline 100 mg po/2 h or iv prior to the procedure OR azithromycin 1 g po/iv plus metronidazole 500 mg po | NR | |||
| Vulvectomy | NR | Single dose of antibiotic 7 | |||
| Urogynecology procedures | NR | NR | |||
| Vaginal sling placement | NR | Insufficient evidence 6 | |||
| Colporrhaphy | NR | Insufficient evidence | |||
| Cystoscopy | Not recommended (unless risk factors) | NR | |||
| Urodynamic studies | Not recommended (unless risk factors) | NR | |||
| The Royal Australian and New Zealand College of Obstetricians and Gynecologists (RANCOG) | American College of Obstetricians and Gynecologists (ACOG) | Society of Obstetricians and Gynecologists of Canada (SOGC) | Société Française d’ Anésthesie et de Réanimation (SFAR) | |
| Non-severe hypersensitivity to penicillin | No difference | No difference | No difference | No distinction between non-severe and severe allergic reaction |
| Immediate or delayed severe hypersensitivity to penicillin (e.g., anaphylaxis or Stevens–Johnson syndrome) | Clindamycin 600 mg iv PLUS Gentamicin 2 mg/kg iv | Clindamycin 900 mg Metronidazole 500 mg PLUS 1 Gentamicin 2 5 mg/kg Aztreonam 2 g | Clindamycin 600 mg iv erythromycin 500 mg iv metronidazole | Hysterectomy: Clindamycin 900 mg iv PLUS Gentamicin 5 mg/kg/day Prolapse surgery: Gentamicin 5 mg/kg/d PLUS Metronidazole 1 g |
| Obese patients | 3 g iv cefazolin if patient >120 kg | 3 g iv cefazolin if patient >120 kg | Consider doubling the dose in patients with morbid obesity (BMI > 35 kg/m2) | Double the dose in patients with BMI > 35 kg/m2 |
| Prolonged procedure | Consider an additional dose if >3 h | Additional intraoperative doses administered at intervals of two times the half-life of the drug (after the first dose) Cefazolin should be redosed after 4 h | Additional dose may be administered 3 to 4 h after the initial dose if >3 h | Hysterectomy: Cefazolin if >2 h additional 1 g Cefamandole if >2 h additional 0.75 g Cefuroxime if >2 h additional 0.75 g Prolapse surgery: Aminopenicillin and β-lactamase inhibitor 1 g if >2 h In general, either additional dose or use of an antibiotic with longer half-life. |
| Excessive blood loss | No recommendation | A second dose may be appropriate when blood loss > 1500 mL | Additional dose may be administered 3 to 4 h after the initial dose if blood loss > 1500 mL | No recommendation |
| Colonization or high risk of colonization with MRSA | ADD Vancomycin 15 mg/kg iv | Hospital-recommended MRSA antibiotic prophylaxis protocol or addition of a single preoperative iv dose of vancomycin to the preoperative antibiotic prophylactic regimen | Patient screening debatable | |
| Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) and Spanish Association of Surgeons (AEC) | Enhanced Recovery After Surgery (ERAS) Society | National Institute for Health and Care Excellence (NICE) | Surgical Antibiotic Prophylaxis Guideline at the Women’s in Parkville and in Sandringham | |
| Non-severe hypersensitivity to penicillin | No distinction between non-severe and severe allergic reaction | No distinction between non-severe and severe allergic reaction | Use of cephalosporins can be considered | |
| immediate or delayed severe hypersensitivity to penicillin (e.g., anaphylaxis or Stevens–Johnson syndrome) | Clindamycin PLUS gentamycin Vancomycin PLUS gentamycin | Standard surgical antibiotic prophylaxis including cefazolin or ertapenem 4 | Avoid penicillin and cephalosporins Clindamycin 600 mg iv within 120 min before skin incision PLUS Gentamicin 2 mg/kg IV over 3–5 min within 120 min before skin incision | |
| Obese patients | May require higher initial doses 3 | Increase dose in patients with BMI > 35 kg/m2 or >100 kg | ||
| Prolonged procedure | Additional dose if the surgical procedure exceeds 2 times the half-life of the antibiotic. Additional dose at 3 h for cefazolin or other antibiotic with similar half-life. | Additional dose after 1–2 times the half-life of the antibiotic in prolonged operations (e.g., 3 h for cefazolin; half-life 1.8 h) | Additional dose of antibiotic prophylaxis when the operation is longer than the half-life of the antibiotic administered | Additional dose if the surgical procedure exceeds 2 times the half-life of the antibiotic. |
| Excessive blood loss | Additional dose if blood loss > 1500 mL in adults or >25 mg/kg in children | Additional dose if blood loss > 1500 mL | ||
| Colonization or high risk of colonization with MRSA | Consider use of glycopeptide | Cefazolin 2 g iv within 60 min before skin incision PLUS vancomycin 15 mg/kg iv, 15 to 120 min before skin incision. | ||
| Italian Society of Gynecology and Obstetrics (SIGO) | Hellenic Society of Obstetricians and Gynecologists (HSOG) | Consensus Bundle on Prevention of Surgical Site Infections After Major Gynecologic Surgery | Surgical Infection Prevention Guideline Writers Workgroup (SIPGWW) | |
| Non-severe hypersensitivity to penicillin | Consider patient-specific antibiotic regimen | |||
| Immediate or delayed severe hypersensitivity to penicillin (e.g., anaphylaxis or Stevens–Johnson syndrome) | Clindamycin 600 mg iv PLUS erythromycin 500 mg iv | Consider patient-specific antibiotic regimen |
| |
| Obese patients | Double the dose if BMI > 35 kg/m2 | Consider patient-specific antibiotic regimen | ||
| Prolonged procedure | Additional dose if the surgical procedure exceeds 2 times the half-life of the antibiotic. | Additional dose after 3–4 h if the procedure lasts longer than 3 h | Additional dose if the procedure lasts longer than 2–3 h (redose at 1–2 times the half-life of the drug) | |
| Excessive blood loss | Additional dose if excessive blood loss (>1500 mL) | Additional dose after 3–4 h if blood loss > 1500 mL | Additional dose if excessive blood loss (>1500 mL) | |
| Colonization or high risk of colonization with MRSA | Consider patient-specific antibiotic regimen | Colonization: Vancomycin High risk: No evidence about the use of vancomycin |
| The Royal Australian and New Zealand College of Obstetricians and Gynecologists (RANCOG) | At least 30 min prior to incision |
| American College of Obstetricians and Gynecologists (ACOG) | Within 1 h from skin incision (e.g., cefazolin). For quinolones or vancomycin, the infusion should begin before up to 2 h |
| Society of Obstetricians and Gynecologists of Canada (SOGC) | 15–60 min prior to incision |
| Société Française d’ Anésthesie et de Réanimation (SFAR) | 30 min prior to incision. For vancomycin, the infusion must be finished at least 30 min prior to the procedure. |
| Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) and Spanish Association of Surgeons (AEC) | For βlactams (e.g., penicillin and cephalosporins such as cefazolin, cefoxitin, and cefuroxime) within 60 min from incision For vancomycin, aminoglycosides, or fluoroquinolones, intravenous infusion should begin 90 min prior to incision. |
| Enhanced Recovery After Surgery (ERAS) Society | Within 60 min from skin incision. |
| Hellenic Society of Obstetricians and Gynecologists (HSOG) | 15–60 min prior to incision |
| National Institute for Health and Care Excellence (NICE) | Consider the timing and pharmacokinetics (for example, the serum half-life) and necessary infusion time of the antibiotic. |
| The guidelines on antibiotic application in gynecological Oncology (Serbia) | Intramuscularly 1 h or intravenously 20–30 min prior to the surgery. |
| Surgical Antibiotic Prophylaxis Guideline at the Women’s in Parkville and in Sandringham | Within 15–120 min from skin incision depending on the procedure and the antibiotic used. |
| Italian Society of Gynecology and Obstetrics (SIGO) | within 120 min from the incision, considering the half-life of the antibiotic |
| Consensus Bundle on Prevention of Surgical Site Infections After Major Gynecologic Surgery | Within 60 min before skin incision (most effective if administered 0–30 min before skin incision). Within 120 min for antibiotics that require slow infusion. |
| Surgical Infection Prevention Guideline Writers Workgroup (SIPGWW) | Within 60 min from incision. For fluoroquinolone or vancomycin, the infusion should begin within 120 min before incision |
| European Society of Gynecological Oncology (ESGO) | 2 h time window before surgical incision, while considering the half-life of the antibiotic. Repeat intraoperative dosing of the antibiotic prophylaxis should be performed depending on the half-life time of the antibiotic and the duration of the surgery. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petousis, S.; Angelou, P.; Almperis, A.; Laganà, A.S.; Titilas, G.; Margioula-Siarkou, C.; Dinas, K. Prophylactic Antibiotics before Gynecologic Surgery: A Comprehensive Review of Guidelines. J. Pers. Med. 2024, 14, 327. https://doi.org/10.3390/jpm14030327
Petousis S, Angelou P, Almperis A, Laganà AS, Titilas G, Margioula-Siarkou C, Dinas K. Prophylactic Antibiotics before Gynecologic Surgery: A Comprehensive Review of Guidelines. Journal of Personalized Medicine. 2024; 14(3):327. https://doi.org/10.3390/jpm14030327
Chicago/Turabian StylePetousis, Stamatios, Panagiota Angelou, Aristarchos Almperis, Antonio Simone Laganà, Gerasimos Titilas, Chrysoula Margioula-Siarkou, and Konstantinos Dinas. 2024. "Prophylactic Antibiotics before Gynecologic Surgery: A Comprehensive Review of Guidelines" Journal of Personalized Medicine 14, no. 3: 327. https://doi.org/10.3390/jpm14030327
APA StylePetousis, S., Angelou, P., Almperis, A., Laganà, A. S., Titilas, G., Margioula-Siarkou, C., & Dinas, K. (2024). Prophylactic Antibiotics before Gynecologic Surgery: A Comprehensive Review of Guidelines. Journal of Personalized Medicine, 14(3), 327. https://doi.org/10.3390/jpm14030327