

Assessment of a New Medical Device (PirifixTM) for Positioning and Maintaining the Upper Dental Arch during Le Fort I Osteotomy

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
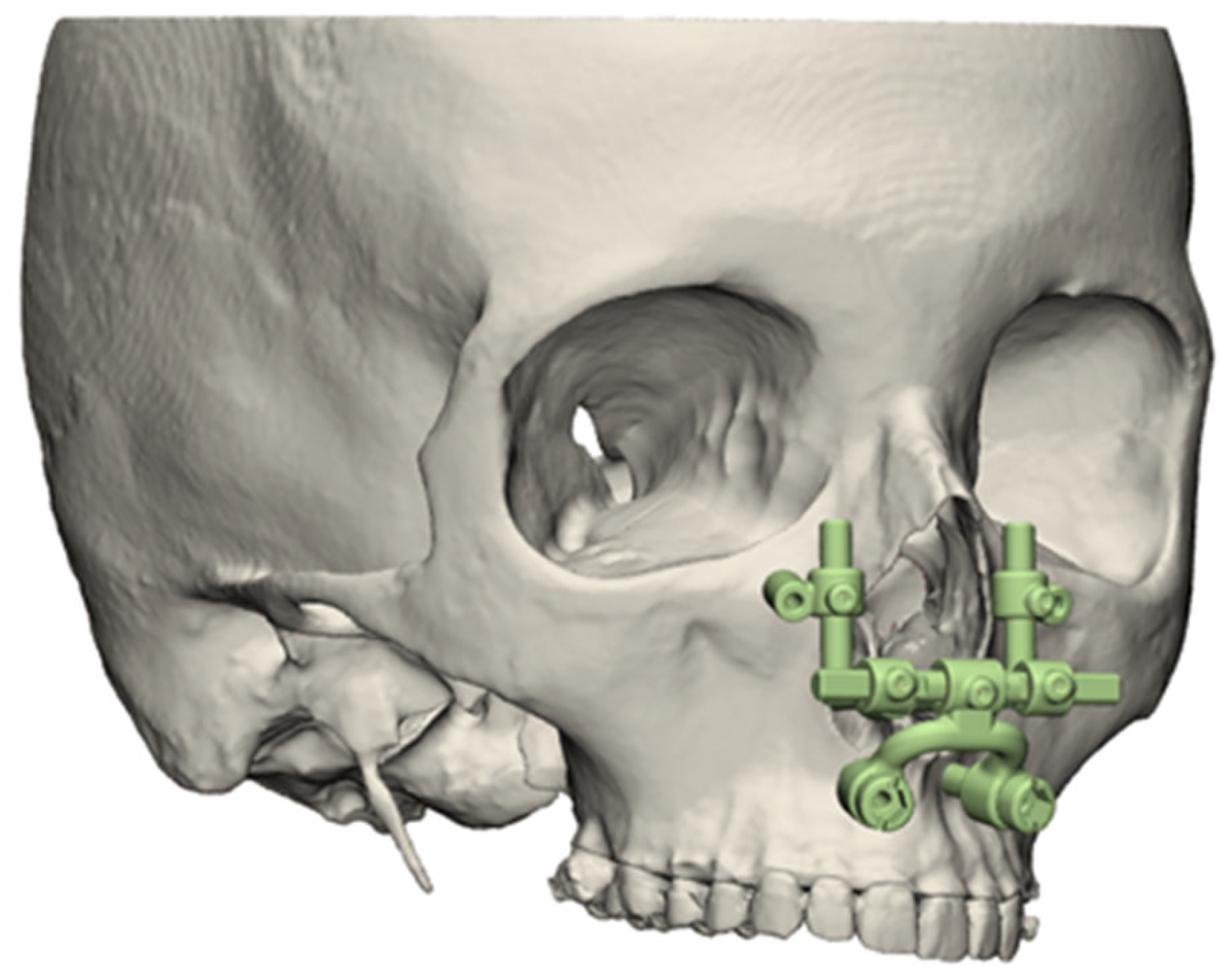
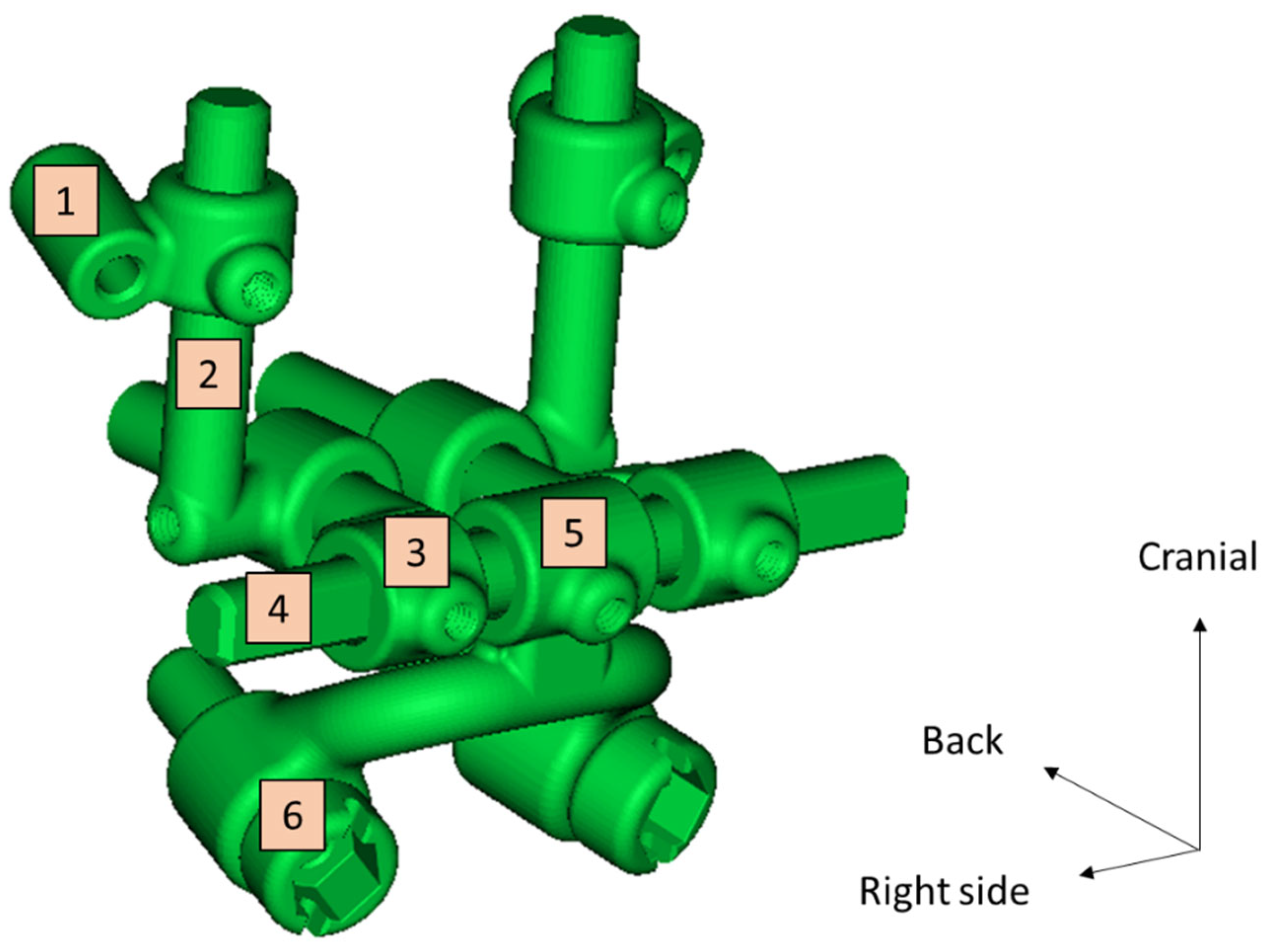
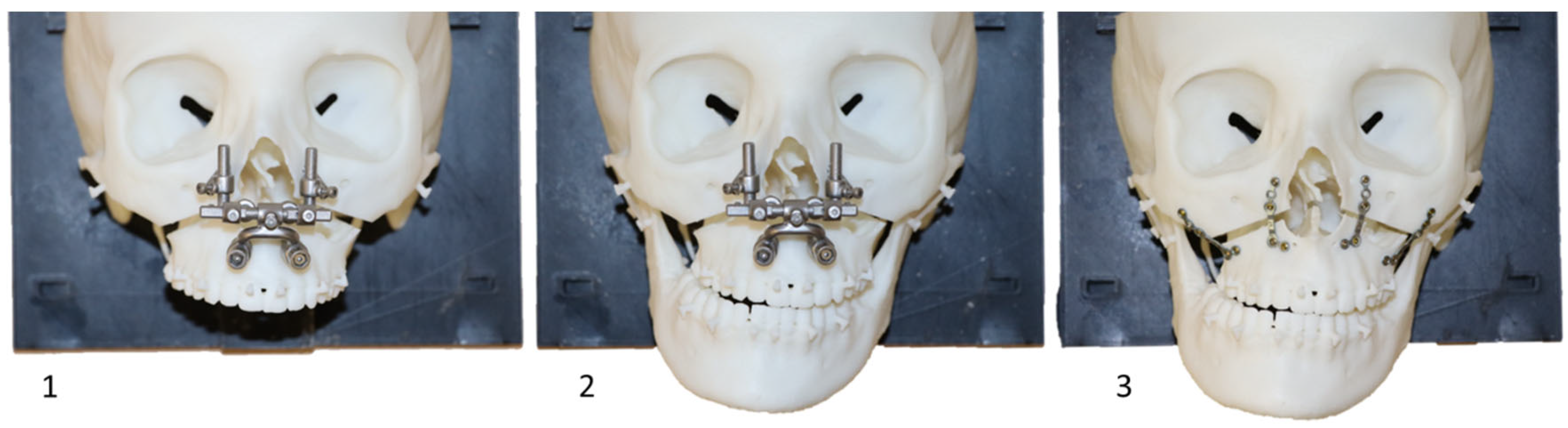
2.1. Description of the Medical Device
2.2. Creation of an Experimental Model
2.2.1. Data Selection
2.2.2. Conception
2.2.3. Planned Models
2.2.4. Splint Design
2.2.5. Three-Dimensional Printing
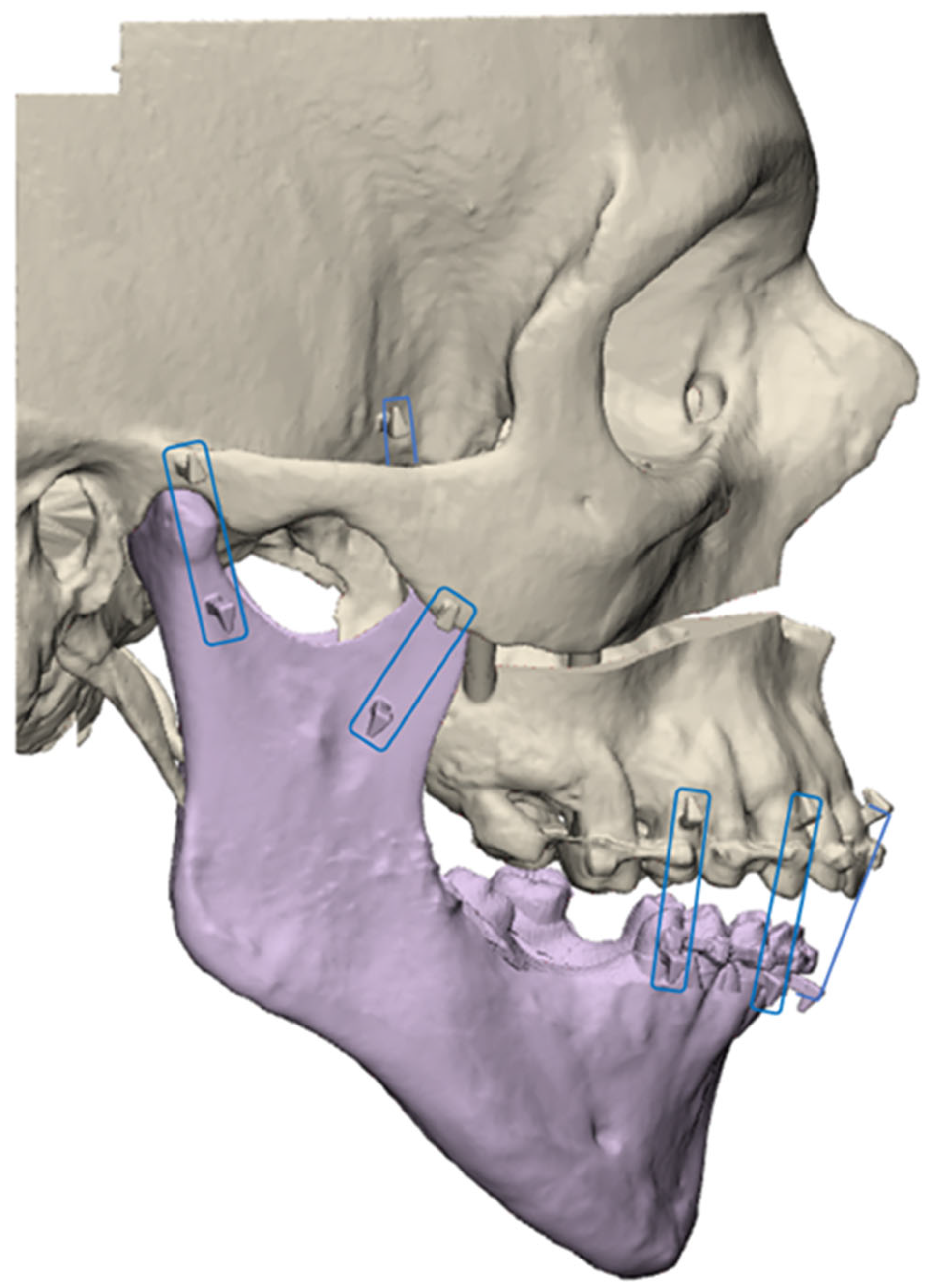
2.2.6. Digitalizing
2.2.7. Comparison
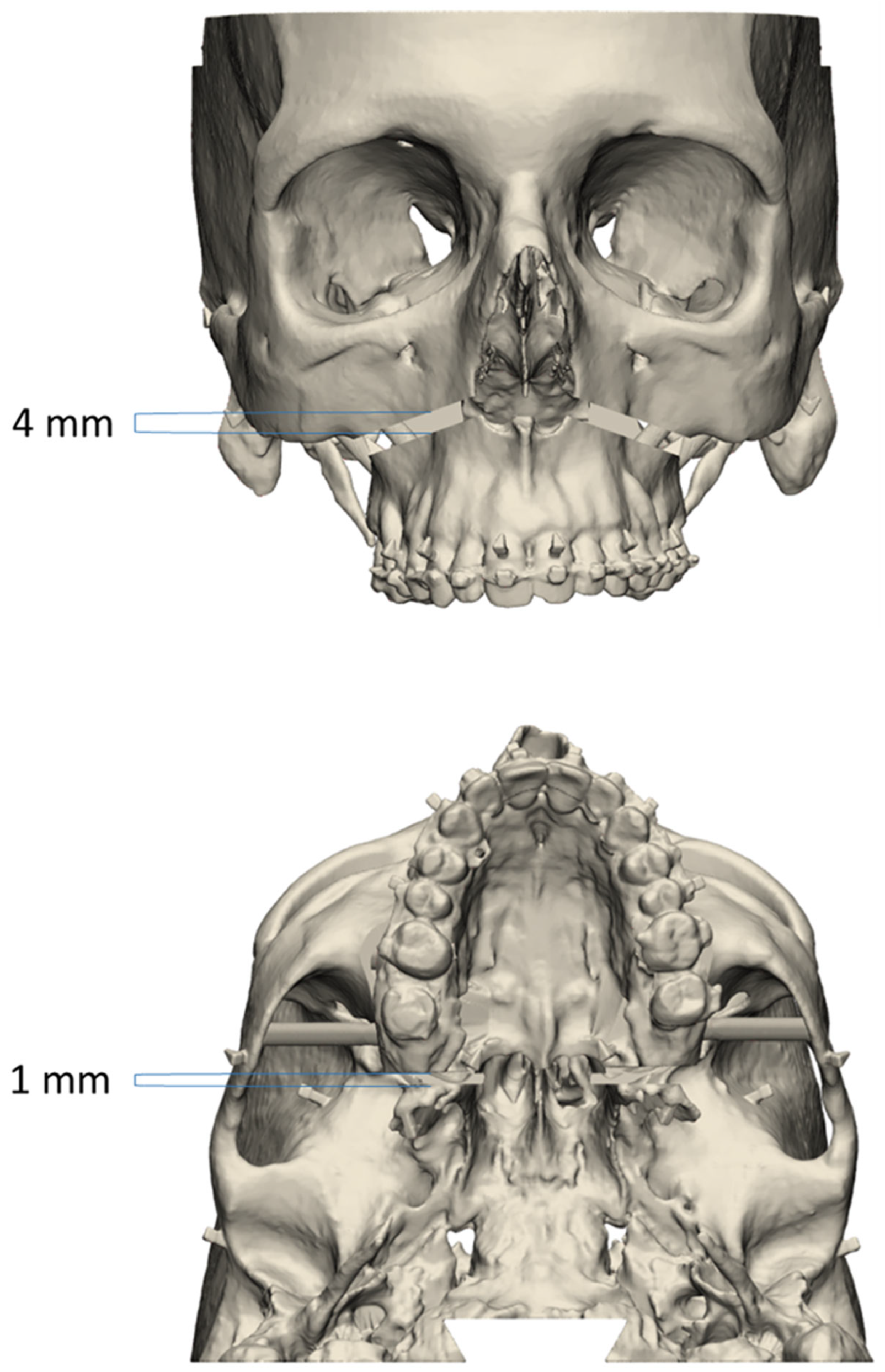
2.3. Evaluation of Device-Aided UDA Positioning Accuracy
2.3.1. Positioning Procedure
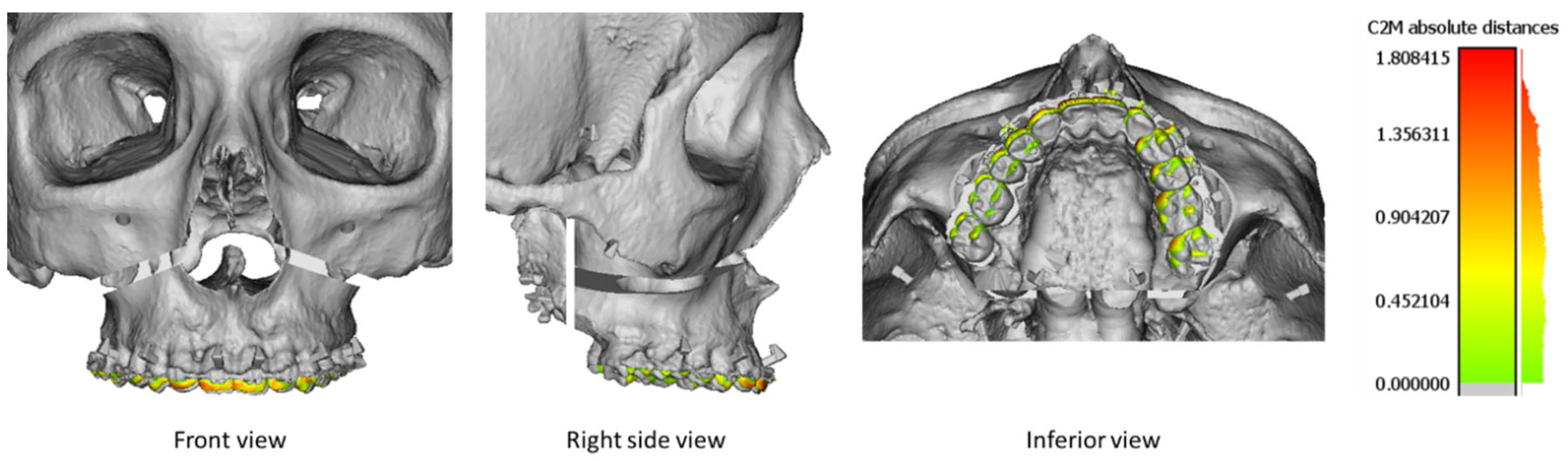
2.3.2. Digitalizing
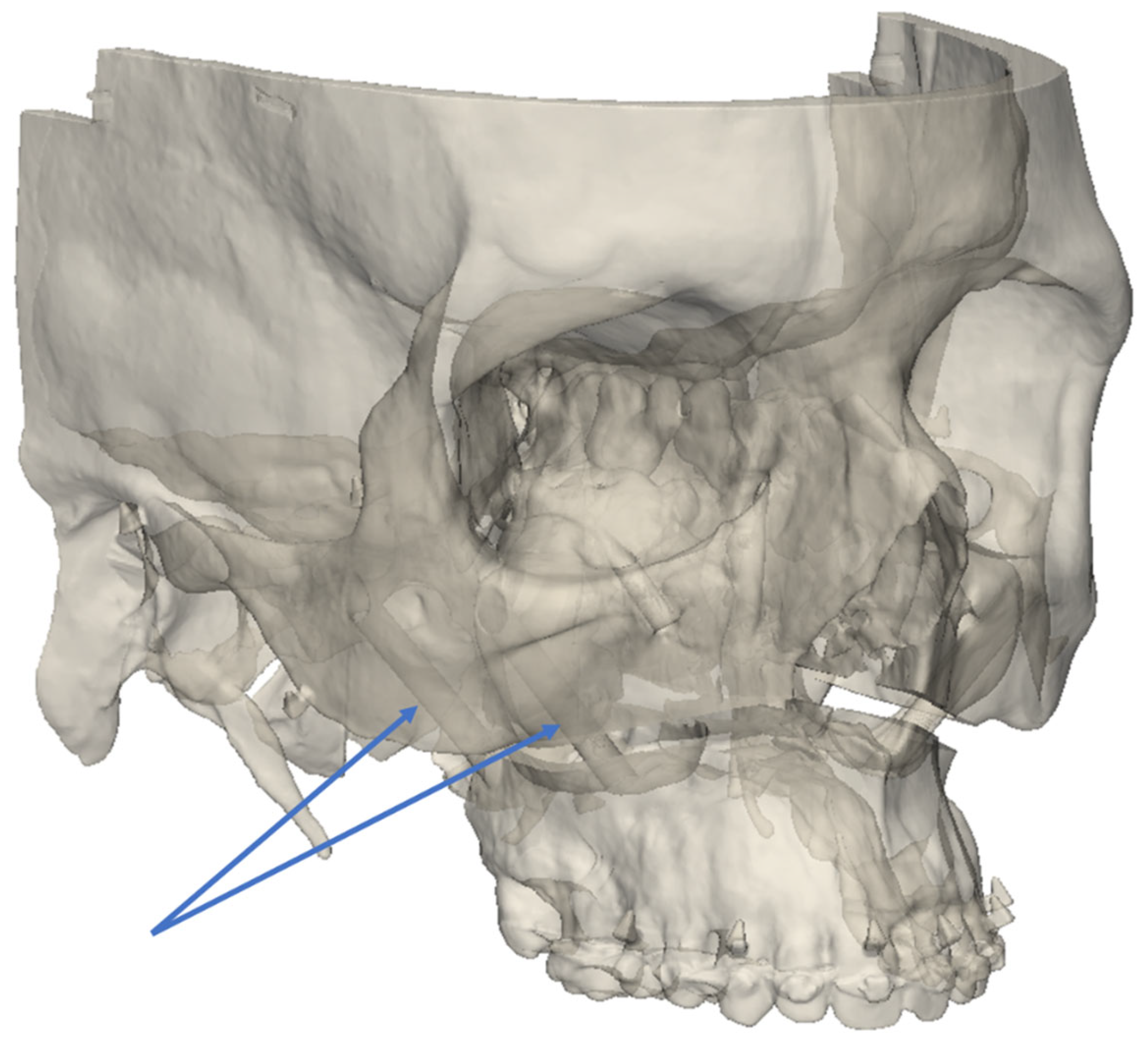
2.3.3. Comparison of Precision
2.4. Statistical Analysis
3. Results
3.1. Experimental Models
3.2. Assessment of Group Comparability before the Separation of the UDA
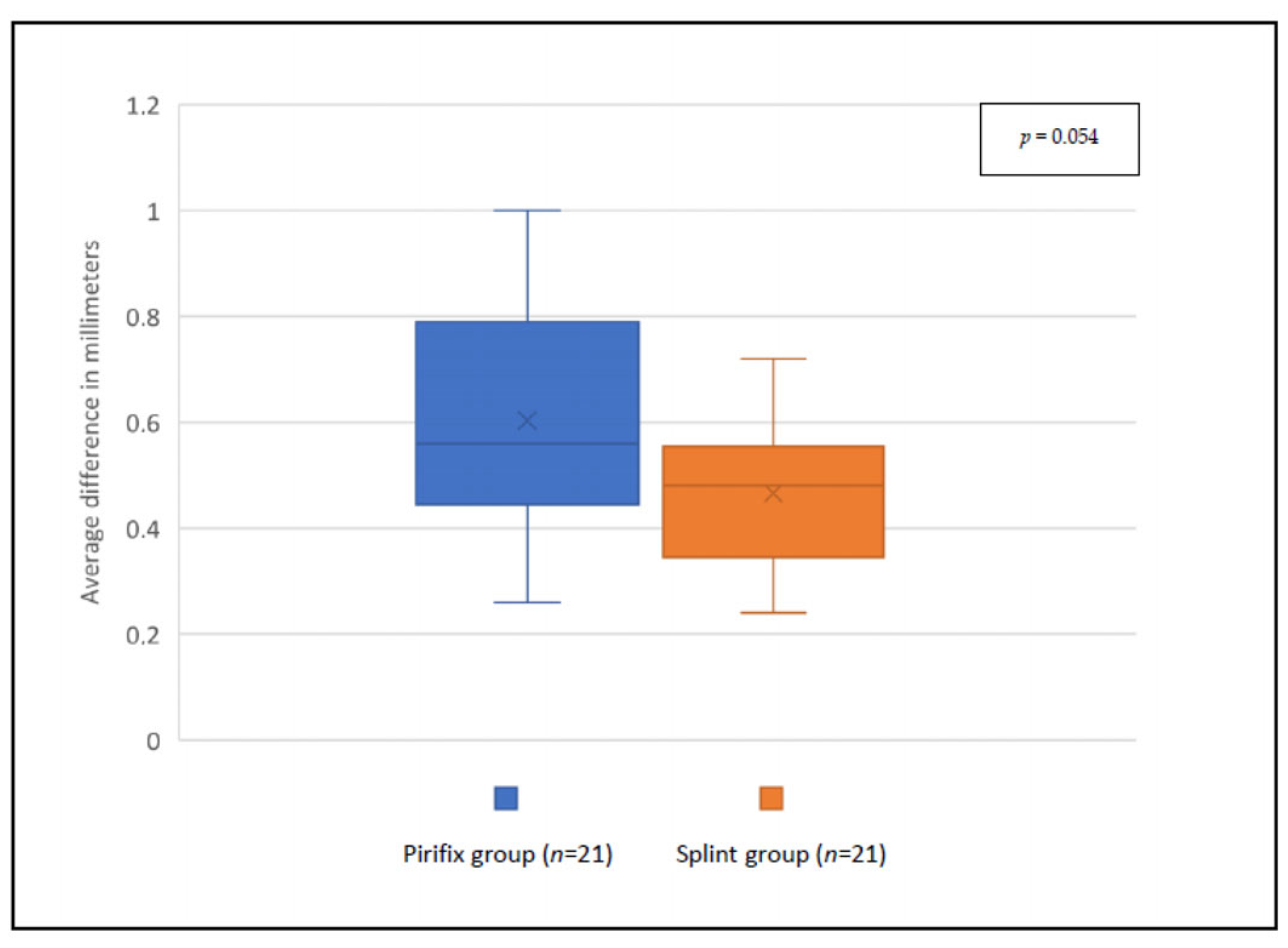
3.3. Evaluation of Device-Aided UDA Positioning Accuracy
4. Discussion
4.1. Experimental Models
4.2. Occlusal Splints
4.3. Assessment of PirifxTM
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lonic, D.; Pai, B.C.-J.; Yamaguchi, K.; Chortrakarnkij, P.; Lin, H.-H.; Lo, L.-J. Computer-Assisted Orthognathic Surgery for Patients with Cleft Lip/Palate: From Traditional Planning to Three-Dimensional Surgical Simulation. PLoS ONE 2016, 11, e0152014. [Google Scholar] [CrossRef] [PubMed]
- Terajima, M.; Nakasima, A.; Aoki, Y.; Goto, T.K.; Tokumori, K.; Mori, N.; Hoshino, Y. A 3-dimensional method for analyzing the morphology of patients with maxillofacial deformities. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Béziat, J.-L. Chirurgie Orthognathique Piézoélectrique; EDP Sciences: Les Ulis, France, 2013; ISBN 978-2-7598-0650-8. [Google Scholar]
- Mulier, D.; Shaheen, E.; Shujaat, S.; Fieuws, S.; Jacobs, R.; Politis, C. How accurate is digital-assisted Le Fort I maxillary osteotomy? A three-dimensional perspective. Int. J. Oral Maxillofac. Surg. 2020, 49, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Dumrongwongsiri, S.; Lin, H.-H.; Niu, L.-S.; Lo, L.-J. Customized Three-Dimensional Printing Spacers for Bone Positioning in Orthognathic Surgery for Correction and Prevention of Facial Asymmetry. Plast. Reconstr. Surg. 2019, 144, 246e–251e. [Google Scholar] [CrossRef]
- Abu-Serriah, M.; Wong, L.; Saeed, N. Adjunct to intraoperative control of vertical movement in inferiorly positioned Le Fort I maxillary osteotomy. Br. J. Oral Maxillofac. Surg. 2017, 55, 222–223. [Google Scholar] [CrossRef]
- Huang, S.-F.; Lo, L.-J.; Lin, C.-L. Biomechanical optimization of a custom-made positioning and fixing bone plate for Le Fort I osteotomy by finite element analysis. Comput. Biol. Med. 2016, 68, 49–56. [Google Scholar] [CrossRef]
- Wong, A.; Goonewardene, M.S.; Allan, B.P.; Mian, A.S.; Rea, A. Accuracy of maxillary repositioning surgery using CAD/CAM customized surgical guides and fixation plates. Int. J. Oral Maxillofac. Surg. 2021, 50, 494–500. [Google Scholar] [CrossRef]
- Tankersley, A.C.; Nimmich, M.C.; Battan, A.; Griggs, J.A.; Caloss, R. Comparison of the Planned Versus Actual Jaw Movement Using Splint-Based Virtual Surgical Planning: How Close Are We at Achieving the Planned Outcomes? J. Oral Maxillofac. Surg. 2019, 77, 1675–1680. [Google Scholar] [CrossRef]
- Lin, H.-H.; Lonic, D.; Lo, L.-J. 3D printing in orthognathic surgery—A literature review. J. Formos. Med. Assoc. 2018, 117, 547–558. [Google Scholar] [CrossRef]
- Kraeima, J.; Schepers, R.H.; Spijkervet, F.K.L.; Maal, T.J.J.; Baan, F.; Witjes, M.J.H.; Jansma, J. Splintless surgery using patient-specific osteosynthesis in Le Fort I osteotomies: A randomized controlled multi-centre trial. Int. J. Oral Maxillofac. Surg. 2020, 49, 454–460. [Google Scholar] [CrossRef]
- Suojanen, J.; Leikola, J.; Stoor, P. The use of patient-specific implants in orthognathic surgery: A series of 32 maxillary osteotomy patients. J. Cranio-Maxillofac. Surg. 2016, 44, 1913–1916. [Google Scholar] [CrossRef]
- Kraeima, J.; Jansma, J.; Schepers, R.H. Splintless surgery: Does patient-specific CAD-CAM osteosynthesis improve accuracy of Le Fort I osteotomy? Br. J. Oral Maxillofac. Surg. 2016, 54, 1085–1089. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Wei, H.; Jiang, T.; Qian, Y.; Zhang, T.; Yu, H.; Zhang, L.; Wang, X. Randomized Clinical Trial of the Accuracy of Patient-Specific Implants versus CAD/CAM Splints in Orthognathic Surgery. Plast. Reconstr. Surg. 2021, 148, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Mo, S.; Fan, X.; You, Y.; Ye, G.; Zhou, N. A Meta-analysis and Systematic Review Comparing the Effectiveness of Traditional and Virtual Surgical Planning for Orthognathic Surgery: Based on Randomized Clinical Trials. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2021, 79, 471.e1–471.e19. [Google Scholar] [CrossRef]
- Benassarou, M.; Benassarou, A.; Meyer, C. La navigation en chirurgie orthognathique. Application à l’ostéotomie de Le Fort I. Rev. Stomatol. Chir. Maxillo-Faciale Chir. Orale 2013, 114, 219–227. [Google Scholar] [CrossRef]
- Lartizien, R.; Zaccaria, I.; Noyelles, L.; Bettega, G. Quantification of the inaccuracy of conventional articulator model surgery in Le Fort 1 osteotomy: Evaluation of 30 patients controlled by the Orthopilot® navigation system. Br. J. Oral Maxillofac. Surg. 2019, 57, 672–677. [Google Scholar] [CrossRef]
- Lartizien, R.; Zaccaria, I.; Noyelles, L.; Bettega, G. Improvement in accuracy of maxillary repositioning of Le Fort I osteotomy with OrthopilotTM Navigation System: Evaluation of 30 patients. Br. J. Oral Maxillofac. Surg. 2020, 58, 1116–1122. [Google Scholar] [CrossRef]
- Marmulla, R.; Mühling, J.; Lüth, T.; Hassfeld, S. Physiological shift of facial skin and its influence on the change in precision of computer-assisted surgery. Br. J. Oral Maxillofac. Surg. 2006, 44, 273–278. [Google Scholar] [CrossRef]
- Sun, Y.; Luebbers, H.-T.; Agbaje, J.O.; Schepers, S.; Vrielinck, L.; Lambrichts, I.; Politis, C. Evaluation of 3 different registration techniques in image-guided bimaxillary surgery. J. Craniofac. Surg. 2013, 24, 1095–1099. [Google Scholar] [CrossRef]
- Berger, M.; Nova, I.; Kallus, S.; Ristow, O.; Eisenmann, U.; Freudlsperger, C.; Seeberger, R.; Hoffmann, J.; Dickhaus, H. Electromagnetic navigated positioning of the maxilla after Le Fort I osteotomy in preclinical orthognathic surgery cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 298–304. [Google Scholar] [CrossRef]
- Le Parlement Européen et le Conseil de l’Union Européenne. Règlement (UE) 2017/745 du Parlement Européen et du Conseil—Du 5 avril 2017—Relatif aux dispositifs médicaux, modifiant la directive 2001/83/CE, le règlement (CE) no 178/2002 et le règlement (CE) no 1223/2009 et abrogeant les directives du conseil 90/385/CEE et 93/42/CEE. J. Off. l’Union Eur. 2017, 117, 175. [Google Scholar]
- Lauren, M.; McIntyre, F. A new computer-assisted method for design and fabrication of occlusal splints. Am. J. Orthod. Dentofac. Orthop. 2008, 133, S130–S135. [Google Scholar] [CrossRef]
- Shaheen, E.; Sun, Y.; Jacobs, R.; Politis, C. Three-dimensional printed final occlusal splint for orthognathic surgery: Design and validation. Int. J. Oral Maxillofac. Surg. 2017, 46, 67–71. [Google Scholar] [CrossRef]
- Zinser, M.J.; Sailer, H.F.; Ritter, L.; Braumann, B.; Maegele, M.; Zöller, J.E. A paradigm shift in orthognathic surgery? A comparison of navigation, computer-aided designed/computer-aided manufactured splints, and “classic” intermaxillary splints to surgical transfer of virtual orthognathic planning. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2013, 71, 2151.e1–2151.e21. [Google Scholar] [CrossRef] [PubMed]
- Kokich, V.O.; Kiyak, H.A.; Shapiro, P.A. Comparing the perception of dentists and lay people to altered dental esthetics. J. Esthet. Dent. 1999, 11, 311–324. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Data | |
|---|---|---|
| Sex | ||
| Female | 15 (71.4%) | |
| Male | 6 (28.6%) | |
| Age | ||
| <20 yo | 5 (23.8%) | |
| 20 to 30 yo | 8 (38.1%) | |
| 30 to 40 yo | 3 (14.3%) | |
| >40 yo | 5 (23.8%) | |
| Average | 28.6 yo (16 to 55) | |
| Angle’s classification | ||
| II | 9 (42.9%) | |
| III | 12 (57.1%) | |
| Surgery | ||
| LFIO only | 2 (9.5%) | |
| LFIO and BSSO | 19 (90.5%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serree, P.-E.; Bertin, E.; Coussens, C.; Brumpt, E.; Devoti, J.-F.; Louvrier, A. Assessment of a New Medical Device (PirifixTM) for Positioning and Maintaining the Upper Dental Arch during Le Fort I Osteotomy. J. Pers. Med. 2024, 14, 324. https://doi.org/10.3390/jpm14030324
Serree P-E, Bertin E, Coussens C, Brumpt E, Devoti J-F, Louvrier A. Assessment of a New Medical Device (PirifixTM) for Positioning and Maintaining the Upper Dental Arch during Le Fort I Osteotomy. Journal of Personalized Medicine. 2024; 14(3):324. https://doi.org/10.3390/jpm14030324
Chicago/Turabian StyleSerree, Pierre-Etienne, Eugénie Bertin, Camille Coussens, Eleonore Brumpt, Jean-François Devoti, and Aurélien Louvrier. 2024. "Assessment of a New Medical Device (PirifixTM) for Positioning and Maintaining the Upper Dental Arch during Le Fort I Osteotomy" Journal of Personalized Medicine 14, no. 3: 324. https://doi.org/10.3390/jpm14030324
APA StyleSerree, P.-E., Bertin, E., Coussens, C., Brumpt, E., Devoti, J.-F., & Louvrier, A. (2024). Assessment of a New Medical Device (PirifixTM) for Positioning and Maintaining the Upper Dental Arch during Le Fort I Osteotomy. Journal of Personalized Medicine, 14(3), 324. https://doi.org/10.3390/jpm14030324