
The First Prospective Study Investigating the Safety and Feasibility of a Spray-Type Adhesion Barrier (AdSpray™) in Minimally Invasive Hepatectomy: An Analysis of 124 Cases at Our Institution



Abstract
1. Introduction
2. Patients and Methods
3. Results
3.1. Patient Background Characteristics and Short-Term Outcomes
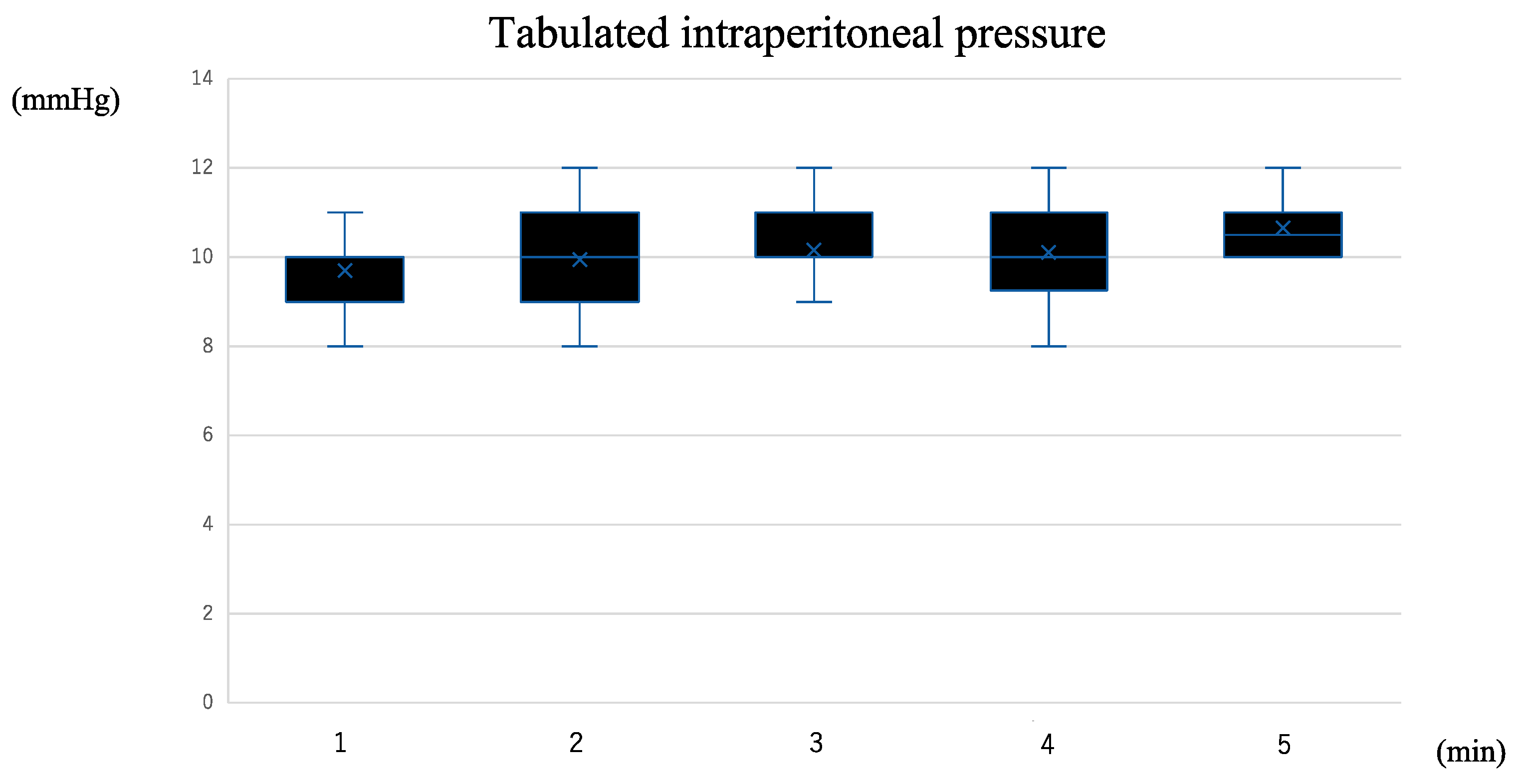
3.2. Results of AdSpray™ Application
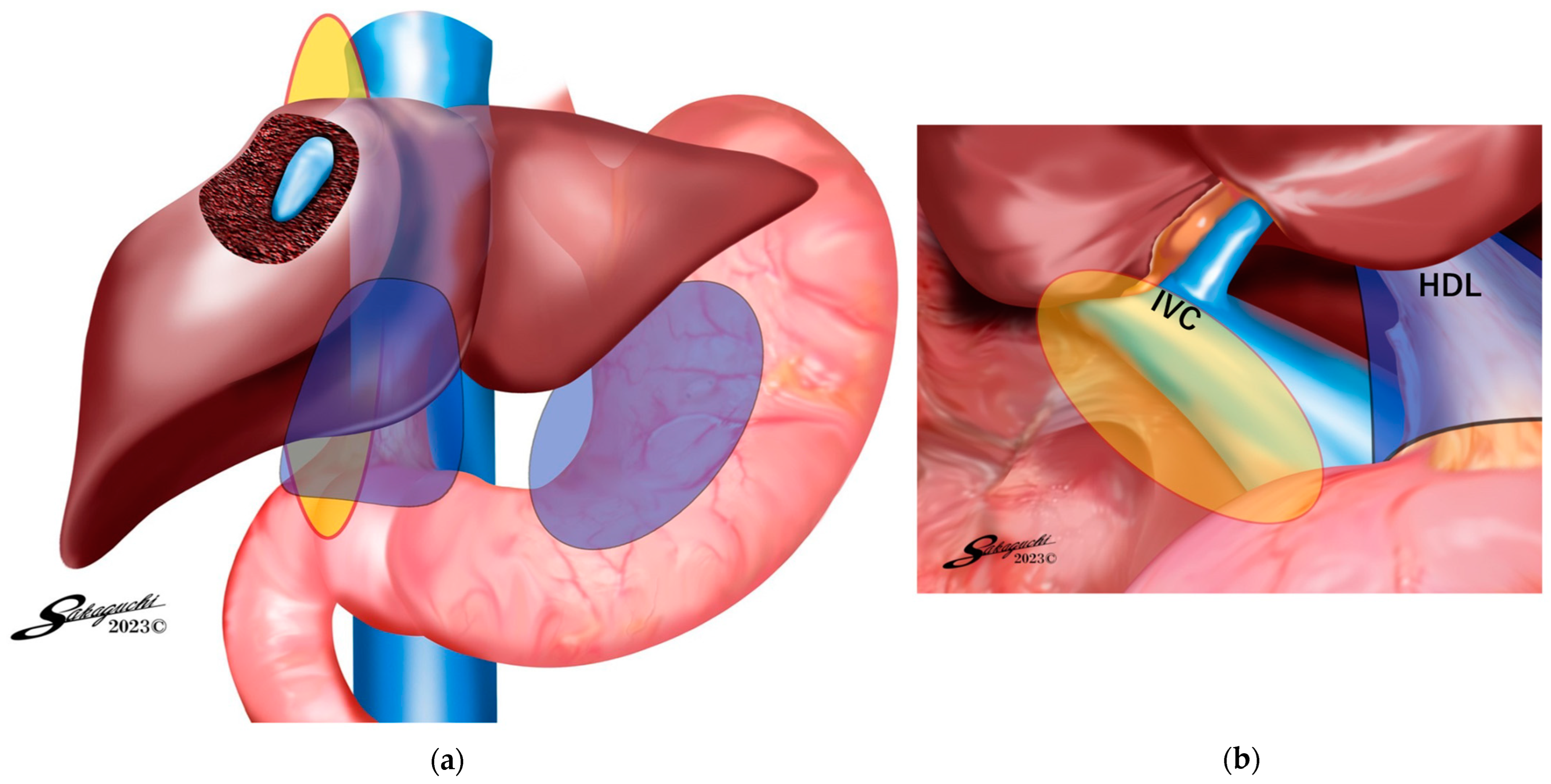
3.3. Analysis According to the Adhesion Barrier Application Site
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
References
- Takahara, T.; Wakabayashi, G.; Konno, H.; Gotoh, M.; Yamaue, H.; Yanaga, K.; Fujimoto, J.; Kaneko, H.; Unno, M.; Endo, I.; et al. Comparison of laparoscopic major hepatectomy with propensity score matched open cases from the National Clinical Database in Japan. J. Hepatobiliary Pancreat. Sci. 2016, 23, 721–734. [Google Scholar] [CrossRef]
- Belli, G.; Cioffi, L.; Fantini, C.; D’Agostino, A.; Russo, G.; Limongelli, P.; Belli, A. Laparoscopic redo surgery for recurrent hepatocellular carcinoma in cirrhotic patients: Feasibility, safety, and results. Surg. Endosc. 2009, 23, 1807–1811. [Google Scholar] [CrossRef] [PubMed]
- Ome, Y.; Hashida, K.; Yokota, M.; Nagahisa, Y.; Yamaguchi, K.; Okabe, M.; Kawamoto, K. The feasibility and efficacy of pure laparoscopic repeat hepatectomy. Surg. Endosc. 2018, 32, 3474–3479. [Google Scholar] [CrossRef] [PubMed]
- Mise, Y.; Hasegawa, K.; Shindoh, J.; Ishizawa, T.; Aoki, T.; Sakamoto, Y.; Sugawara, Y.; Makuuchi, M.; Kokudo, N. The feasibility of third or more repeat hepatectomy for recurrent hepatocellular carcinoma. Ann. Surg. 2015, 262, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Yan, T.D.; Sim, J.; Black, D.; Niu, R.; Morris, D.L. Systematic review on safety and efficacy of repeat hepatectomy for recurrent liver metastases from colorectal carcinoma. Ann. Surg. Oncol. 2007, 14, 2069–2077. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Vaillant, J.C. Repeat resections for recurrent colorectal liver metastases. In Cancer Treatment and Research; Springer: Boston, MA, USA, 1994; pp. 57–61. [Google Scholar]
- Lorenz, M.; DeMatteo, R.; Heinrich, S.; Encke, A.; Blumgart, L.; Fong, Y. Second liver resections are safe and effective treatment for recurrent hepatic metastases from colorectal cancer: A bi-institutional analysis. Ann. Surg. 2002, 235, 863–871. [Google Scholar]
- Gon, H.; Kido, M.; Tanaka, M.; Kuramitsu, K.; Komatsu, S.; Awazu, M.; So, S.; Toyama, H.; Fukumoto, T. Laparoscopic repeat hepatectomy is a more favorable treatment than open repeat hepatectomy for contralateral recurrent hepatocellular carcinoma cases. Surg. Endosc. 2021, 35, 2896–2906. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.; Lovegrove, R.E.; Tilney, H.S.; Heriot, A.G.; John, T.G.; Rees, M.; Tekkis, P.P.; Welsh, F.K. Meta-analysis of clinical outcome after first and second liver resection for colorectal metastases. Surgery 2007, 141, 9–18. [Google Scholar] [CrossRef]
- Sa Cunha, A.; Laurent, C.; Rault, A.; Couderc, P.; Rullier, E.; Saric, J. A second liver resection due to recurrent colorectal liver metastases. Arch. Surg. 2007, 142, 1144–1149. [Google Scholar] [CrossRef]
- Ten Broek, R.P.G.; Stommel, M.W.J.; Strik, C.; van Laarhoven, C.J.H.M.; Keus, F.; van Goor, H. Benefits and harms of adhesion barriers for abdominal surgery: A systematic review and meta-analysis. Lancet 2014, 383, 48–59. [Google Scholar] [CrossRef]
- Dupré, A.; Lefranc, A.; Buc, E.; Delpero, J.R.; Quenet, F.; Passot, G.; Evrard, S.; Rivoire, M. Use of bioresorbable membranes to reduce abdominal and perihepatic adhesions in 2-stage hepatectomy of liver metastases from colorectal cancer: Results of a prospective, randomized controlled phase II trial. Ann. Surg. 2013, 258, 30–36. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Shindoh, J.; Okubo, S.; Tani, K.; Morito, M.; Igata, Y.; Kojima, K.; Umino, R.; Akabane, M.; Hashimoto, M. Hyaluronic acid/carboxymethyl cellulose-based adhesion barrier reduces surgical difficulty and complication in repeat hepatectomy. HPB 2021, 23, 907–914. [Google Scholar] [CrossRef]
- Suto, T.; Watanabe, M.; Endo, T.; Komori, K.; Ohue, M.; Kanemitsu, Y.; Ito, M.; Takii, Y.; Yatsuoka, T.; Shiozawa, M.; et al. The primary result of prospective randomized multicenter trial of new spray-type bio-absorbable adhesion barrier system (TCD-11091) against postoperative adhesion formation. J. Gastrointest. Surg. 2017, 21, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Okubo, S.; Shindoh, J.; Kobayashi, Y.; Matsumura, M.; Hashimoto, M. Adhesions as a risk factor for postoperative morbidity in patients undergoing repeat hepatectomy and the potential efficacy of adhesion barriers. J. Hepatobiliary Pancreat. Sci. 2022, 29, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, A.; Kai, M.; Tasaki, M.; Chino, N.; Hasegawa, K.; Kokudo, N. Evaluation of adhesion barrier types in a rat hepatectomy-induced adhesion model. BMC Surg. 2020, 20, 252. [Google Scholar] [CrossRef]
- Okubo, S.; Shindoh, J.; Kobayashi, Y.; Hashimoto, M. Safety of a new spray-type adhesion barrier (AdSpray®) in liver surgery. J. Hepatobiliary Pancreat. Sci. 2020, 27, 648–654. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Garden, O.J.; Padbury, R.; Rahbari, N.N.; Adam, R.; Capussotti, L.; Fan, S.T.; Yokoyama, Y.; Crawford, M.; Makuuchi, M.; et al. Bile leakage after hepatobiliary and pancreatic surgery: A definition and grading of severity by the International Study Group of Liver Surgery. Surgery 2011, 149, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Okubo, S.; Shindoh, J.; Kobayashi, Y.; Hashimoto, M. Safety of use of a sheet-type adhesion barrier (Interceed®) during liver surgery. World J. Surg. 2020, 44, 4214–4220. [Google Scholar] [CrossRef]
- Cezar, C.; Korell, M.; Tchartchian, G.; Ziegler, N.; Senshu, K.; Herrmann, A.; Larbig, A.; De Wilde, R.L. How to avoid risks for patients in minimal-access trials: Avoiding complications in clinical first-in-human studies by example of the ADBEE study. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 35, 84–96. [Google Scholar] [CrossRef]
- Kawahara, T.; Hagiwara, M.; Takahashi, H.; Tanaka, M.; Imai, K.; Sawada, J.; Kunisawa, T.; Furukawa, H. Cerebral infarction by paradoxical gas embolism during laparoscopic liver resection with injury of the hepatic vessels in a patient without a right-to-left systemic shunt. Am. J. Case Rep. 2017, 18, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, A.; Shirozu, K.; Karashima, Y.; Matsushita, K.; Yamaura, K. Cerebral infarction detected after laparoscopic partial hepatectomy: Case report. JA Clin. Rep. 2019, 5, 82. [Google Scholar] [CrossRef] [PubMed]
- Vidovich, C.; Laserna, A.; Karan, S.B. Venous gas embolism during radical robotic prostatectomy: A case report and evidence-based management algorithm. Cureus 2021, 13, 17296. [Google Scholar] [CrossRef]
- Otsuka, Y.; Katagiri, T.; Ishii, J.; Maeda, T.; Kubota, Y.; Tamura, A.; Tsuchiya, M.; Kaneko, H. Gas embolism in laparoscopic hepatectomy: What is the optimal pneumoperitoneal pressure for laparoscopic major hepatectomy? J. Hepatobiliary Pancreat. Sci. 2013, 20, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.; Laurent, A.; Tayar, C.; Cherqui, D. Laparoscopic liver resection-understanding its role in current practice: The Henri Mondor Hospital experience. Ann. Surg. 2009, 250, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Dagher, I.; Di Giuro, G.; Dubrez, J.; Lainas, P.; Smadja, C.; Franco, D. Laparoscopic versus open right hepatectomy: A comparative study. Am. J. Surg. 2009, 198, 173–177. [Google Scholar] [CrossRef]
- Huntington, C.R.; Prince, J.; Hazelbaker, K.; Lopes, B.; Webb, T.; LeMaster, C.B.; Huntington, T.R. Safety first: Significant risk of air embolism in laparoscopic gasketless insufflation systems. Surg. Endosc. 2019, 33, 3964–3969. [Google Scholar] [CrossRef]
- Weenink, R.P.; Kloosterman, M.; Hompes, R.; Zondervan, P.J.; Beerlage, H.P.; Tanis, P.J.; Hulst, R.A. The AirSeal(R) insufflation device can entrain room air during routine operation. Tech. Coloproctol. 2020, 24, 1077–1082. [Google Scholar] [CrossRef]
- Shimizu, K.; Usuda, M.; Kakizaki, Y.; Narita, T.; Suzuki, O.; Fukuoka, K. Cerebral infarction by paradoxical gas embolism detected after laparoscopic partial hepatectomy with an insufflation management system: A case report. Surg. Case Rep. 2023, 9, 34. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Liver Surface 2. Hepatoduodenal Ligament (HDL) 3. Port Sites | 1. Mobilized Liver Surface 2. Exposed IVC Surface 3. Root of Hepatic Vein | Liver Resected Surface | |
|---|---|---|---|
| Group 1 (n = 53) | ⃝ | × | × |
| Group 2 (n = 49) | ⃝ | ⃝ | × |
| Group 3 (n = 21) | ⃝ | ⃝ | ⃝ |
| Background Characteristics | AdSpray® Group n = 124 | Control Group n = 20 | p-Value |
|---|---|---|---|
| Age | 69 (16–84) | 64 (40–84) | 0.622 |
| Male gender | 76 (61.3%) | 12 (60.0%) | 0.937 |
| BMI | 23.5 (14.8–33.5) | 22.5 (14.8–30.8) | 0.433 |
| ASA score ≥ 3 | 0 | 0 | - |
| Diabetes mellitus | 20 (16%) | 6 (30%) | 0.128 |
| Hepatocellular carcinoma | 65 (52.4%) | 10 (50%) | 0.869 |
| Past history of hepatectomy | 45 (36.3%) | 8 (40%) | 0.564 |
| Albumin (g/dL) | 4.0 (2.6–4.8) | 4.0 (3.0–4.5) | 0.722 |
| Bilirubin (mg/dL) | 0.8 (0.3–1.9) | 0.75 (0.3–1.0) | 0.788 |
| Platelet count (104/mm3) | 14.7 (1.4–50.6) | 18.3 (9.1–34.4) | 0.701 |
| Prothrombin (%) | 98 (79–124.3) | 100 (78–124) | 0.701 |
| ICG-R15 (%) | 9.1 (2.6–33.5) | 1 (1.4–25.9) | 0.365 |
| Surgical Procedures | |||
| laparoscopic hepatectomy | 80 (44.5%) | 9 (45.0%) | 0.0882 |
| robotic hepatectomy | 44 (35.5%) | 11 (55.0%) | 0.105 |
| ≥2 segments resection | 11 (8.9%) | 2 (10.0%) | 0.842 |
| anatomic resection | 54 (43.9%) | 10 (50%) | 0.984 |
| non-anatomic resection | 70 (56.1%) | 10 (50%) | 0.984 |
| Short-Term Outcomes | AdSpray® Group | Control Group | p-Value |
|---|---|---|---|
| n = 124 | n = 20 | ||
| Intraperitoneal pressure during spraying AdSpray® (mmHg) * (n = 20) | 10 (8–15) * | - | - |
| Operation time (min) | 322 (148–1062) | 519 (176–1096) | 0.108 |
| Estimated blood loss (g) | 65 (5–2432) | 174.5 (5–976) | 0.132 |
| Major complications | 7 (5.6%) | 1 (5%) | 0.365 |
| Bile leak | 5 (4.0%) | 0 (0%) | 0.168 |
| Abscess | 4 (3.2%) | 1 (5%) | 0.775 |
| Refractory ascites | 1 (0.8%) | 0 (0%) | 0.702 |
| Liver dysfunction | 0 (0%) | 0 (0%) | - |
| Bleeding | 0 (0%) | 0 (0%) | - |
| Bowel perforation | 0 (0%) | 1 (5%) | 0.365 |
| Operative Outcomes | Group 1 (n = 59) | Group 2 (n = 43) | Group 3 (n = 21) | Control (n = 20) |
|---|---|---|---|---|
| Operation time (min) | 354 (148–925) | 303 (126–1035) | 351 (191–732) | 519 (176–1096) |
| Estimated blood loss (g) | 65 (2–1279) | 64 (5–2432) | 62 (3–570) | 174.5 (5–976) |
| Major complication rate | 5.1% | 4.7% | 14.3% | 5.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kojima, M.; Sugioka, A.; Kato, Y. The First Prospective Study Investigating the Safety and Feasibility of a Spray-Type Adhesion Barrier (AdSpray™) in Minimally Invasive Hepatectomy: An Analysis of 124 Cases at Our Institution. J. Pers. Med. 2024, 14, 309. https://doi.org/10.3390/jpm14030309
Kojima M, Sugioka A, Kato Y. The First Prospective Study Investigating the Safety and Feasibility of a Spray-Type Adhesion Barrier (AdSpray™) in Minimally Invasive Hepatectomy: An Analysis of 124 Cases at Our Institution. Journal of Personalized Medicine. 2024; 14(3):309. https://doi.org/10.3390/jpm14030309
Chicago/Turabian StyleKojima, Masayuki, Atsushi Sugioka, and Yutaro Kato. 2024. "The First Prospective Study Investigating the Safety and Feasibility of a Spray-Type Adhesion Barrier (AdSpray™) in Minimally Invasive Hepatectomy: An Analysis of 124 Cases at Our Institution" Journal of Personalized Medicine 14, no. 3: 309. https://doi.org/10.3390/jpm14030309
APA StyleKojima, M., Sugioka, A., & Kato, Y. (2024). The First Prospective Study Investigating the Safety and Feasibility of a Spray-Type Adhesion Barrier (AdSpray™) in Minimally Invasive Hepatectomy: An Analysis of 124 Cases at Our Institution. Journal of Personalized Medicine, 14(3), 309. https://doi.org/10.3390/jpm14030309