Evaluation of the Performance of OTOPLAN-Based Cochlear Implant Electrode Array Selection: A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Speech Perception Tests
2.3. 3D-Imaging
2.4. Data Analysis
3. Results
3.1. Participants
3.2. Electrode Array Implanted versus the 3D Imaging Recommendation
3.3. Cochlear Duct Length and Angular Insertion Depth
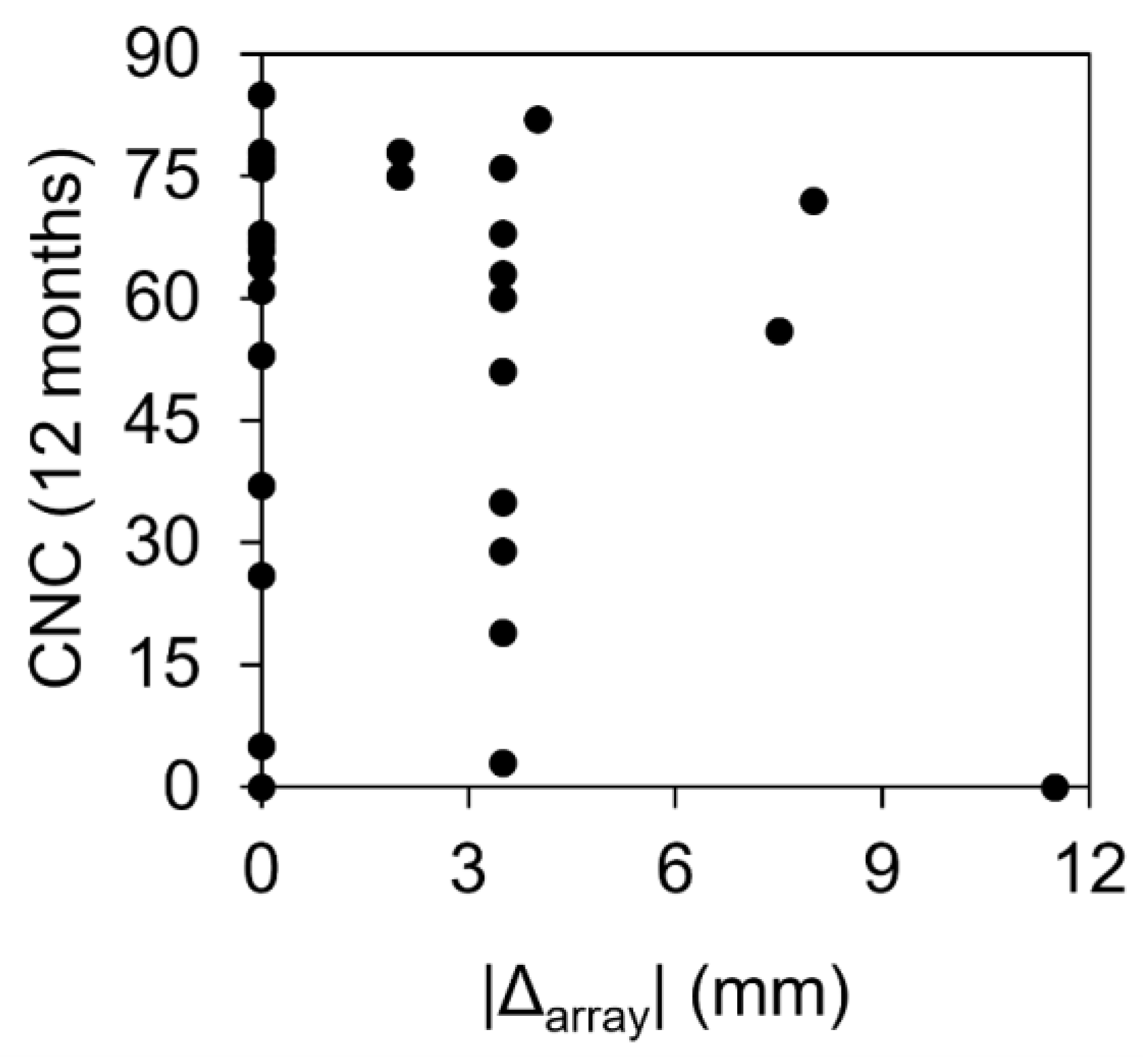
3.4. Speech-in-Quiet Tests in the BiHL Group
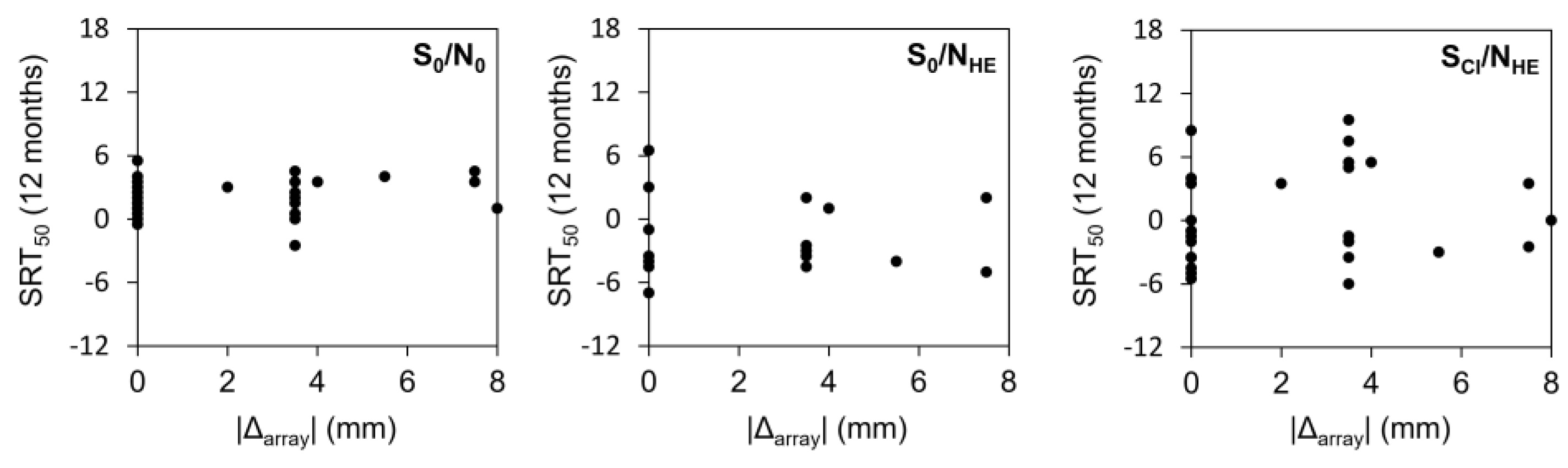
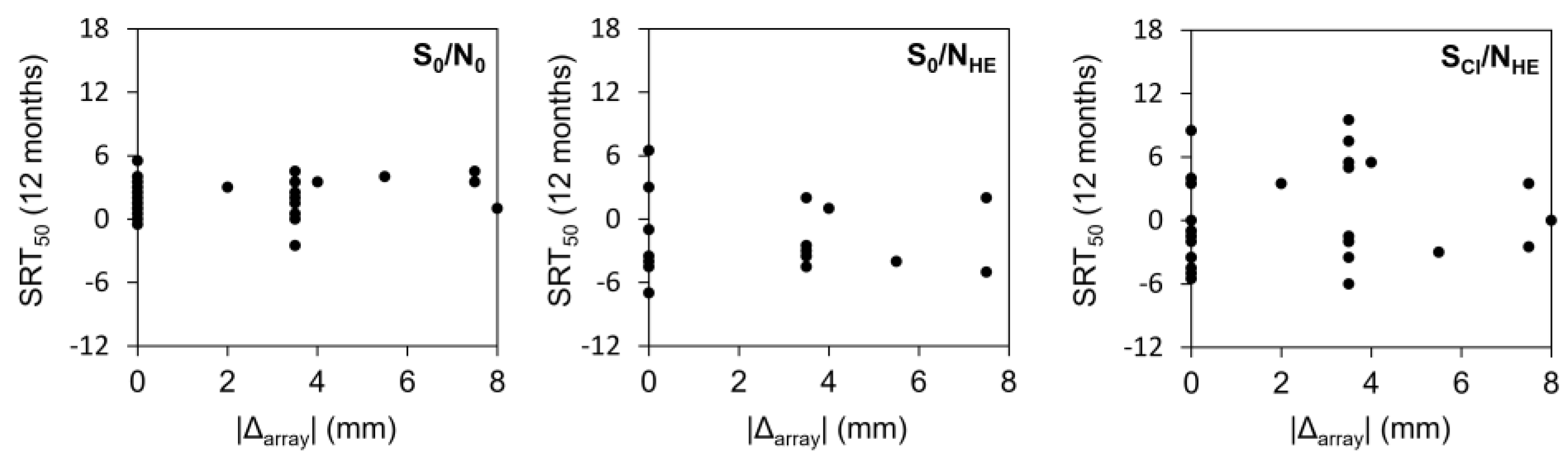
3.5. Speech-in-Noise Tests in the SSD Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Avci, E.; Nauwelaers, T.; Lenarz, T.; Hamacher, V.; Kral, A. Variations in microanatomy of the human cochlea. J. Comp. Neurol. 2014, 522, 3245–3261. [Google Scholar] [CrossRef] [PubMed]
- Mistrík, P.; Jolly, C. Optimal electrode length to match patient specific cochlear anatomy. Eur. Ann. Otorhinolaryngol. Head Neck. Dis. 2016, 133 (Suppl. S1), S68–S71. [Google Scholar] [CrossRef]
- Spiegel, J.L.; Polterauer, D.; Hempel, J.M.; Canis, M.; Spiro, J.E.; Müller, J. Variation of the cochlear anatomy and cochlea duct length: Analysis with a new tablet-based software. Eur. Arch. Otorhinolaryngol. 2022, 279, 1851–1861. [Google Scholar] [CrossRef] [PubMed]
- Alexiades, G.; Dhanasingh, A.; Jolly, C. Method to estimate the complete and two-turn cochlear duct length. Otol. Neurotol. 2015, 36, 904–907. [Google Scholar] [CrossRef] [PubMed]
- Escudé, B.; James, C.; Deguine, O.; Cochard, N.; Eter, E.; Fraysse, B. The size of the cochlea and predictions of insertion depth angles for cochlear implant electrodes. Audiol Neurotol. 2006, 11 (Suppl. S1), 27–33. [Google Scholar] [CrossRef] [PubMed]
- Hardy, M. The length of the organ of Corti in man. Am. J. Anat. 1938, 62, 291–311. [Google Scholar] [CrossRef]
- Kuthubutheen, J.; Grewal, A.; Symons, S. The Effect of Cochlear Size on Cochlear Implantation Outcomes. Biomed. Res. Int. 2019, 2019, 5849871. [Google Scholar] [CrossRef]
- O’connell, B.P.; Cakir, A.; Hunter, J.B.; Francis, D.O.; Noble, J.H.; Labadie, R.F.; Zuniga, G.; Dawant, B.M.; Rivas, A.; Wanna, G.B. Electrode location and angular insertion depth are predictors of audiologic outcomes in cochlear implantation. Otol. Neurotol. 2016, 37, 1016–1023. [Google Scholar] [CrossRef]
- Büchner, A.; Illg, A.; Majdani, O.; Lenarz, T. Investigation of the effect of cochlear implant electrode length on speech comprehension in quiet and noise compared with the results with users of electro-acoustic-stimulation, a retrospective analysis. PLoS ONE 2017, 12, e0174900. [Google Scholar] [CrossRef]
- Canfarotta, M.W.; Dillon, M.T.; Buss, E.; Pillsbury, H.C.; Brown, K.D.; O’Connell, B.P. Frequency-to-Place Mismatch: Characterizing Variability and the Influence on Speech Perception Outcomes in Cochlear Implant Recipients. Ear Hear. 2020, 41, 1349–1361. [Google Scholar] [CrossRef]
- Gstoettner, W.; Plenk, H.; Franz, P.; Hamzavi, J.; Baumgartner, W.; Czerny, C.; Ehrenberger, K. Cochlear implant deep electrode insertion: Extent of insertional trauma. Acta Otolaryngol. 1997, 117, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Gantz, B.J.; Dunn, C.; Oleson, J.; Hansen, M.; Parkinson, A.; Turner, C. Multicenter clinical trial of the Nucleus Hybrid S8 cochlear implant: Final outcomes. Laryngoscope 2016, 126, 962–973. [Google Scholar] [CrossRef] [PubMed]
- Suhling, M.-C.; Majdani, O.; Salcher, R.; Leifholz, M.; Büchner, A.; Lesinski-Schiedat, A.; Lenarz, T. The Impact of Electrode Array Length on Hearing Preservation in Cochlear Implantation. Otol. Neurotol. 2016, 37, 1006–1015. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, B.P.; Hunter, J.B.; Haynes, D.S.; Holder, J.T.; Dedmon, M.M.; Noble, J.H.; Dawant, B.M.; Wanna, G.B. Insertion depth impacts speech perception and hearing preservation for lateral wall electrodes. Laryngoscope 2017, 127, 2352–2357. [Google Scholar] [CrossRef] [PubMed]
- Incerti, P.V.; Ching, T.Y.C.; Cowan, R. A systematic review of electric-acoustic stimulation. Trends Amplif. 2013, 17, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Takagi, A.; Sando, I. Computer-aided three-dimensional reconstruction: A method of measuring temporal bone structures including the length of the cochlea. Ann. Otol. Rhinol. Laryngol. 1989, 98, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Koch, R.W.; Ladak, H.M.; Elfarnawany, M.; Agrawal, S.K. Measuring cochlear duct length—A historical analysis of methods and results. J. Otolaryngol. Head Neck. Surg. 2017, 46, 19. [Google Scholar] [CrossRef]
- Dhanasingh, A.; Hochmair, I. Thirty years of translational research behind MED-EL. Acta Otolaryngol. 2021, 141, 1–198. [Google Scholar] [CrossRef]
- Canfarotta, M.W.; Dillon, M.T.; Buss, E.; Pillsbury, H.C.; Brown, K.D.; O’Connell, B.P. Validating a new tablet-based tool in the determination of cochlear implant angular insertion depth. Otol. Neurotol. 2019, 40, 1006–1010. [Google Scholar] [CrossRef]
- Khurayzi, T.; Almuhawas, F.; Sanosi, A. Direct measurement of cochlear parameters for automatic calculation of the cochlear duct length. Ann. Saudi. Med. 2020, 40, 212–218. [Google Scholar] [CrossRef]
- Canfarotta, M.W.; Dillon, M.T.; Brown, K.D.; Pillsbury, H.C.; Dedmon, M.M.; O’Connell, B.P. Insertion depth and cochlear implant speech recognition outcomes: A comparative study of 28- and 31.5-mm lateral wall arrays. Otol. Neurotol. 2021, 43, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Dutrieux, N.; Quatre, R.; Péan, V.; Schmerber, S. Correlation between cochlear length, insertion angle, and tonotopic mismatch for MED-EL FLEX28 electrode arrays. Otol. Neurotol. 2021, 43, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chen, J.; Tan, H. Cochlear duct length calculation: Comparison between using otoplan and curved multiplanar reconstruction in nonmalformed cochlea. Otol. Neurotol. 2021, 42, e875–e880. [Google Scholar] [CrossRef] [PubMed]
- Lovato, A.; de Filippis, C. Utility of OTOPLAN reconstructed images for surgical planning of cochlear implantation in a case of post-meningitis ossification. Otol. Neurotol. 2019, 40, e60–e61. [Google Scholar] [CrossRef] [PubMed]
- Lovato, A.; Marioni, G.; Gamberini, L.; Bonora, C.; Genovese, E.; de Filippis, C. OTOPLAN in cochlear implantation for far-advanced otosclerosis. Otol. Neurotol. 2020, 41, e1024–e1028. [Google Scholar] [CrossRef]
- Jurawitz, M.-C.; Büchner, A.; Harpel, T.; Schüssler, M.; Majdani, O.; Lesinski-Schiedat, A.; Lenarz, T. Hearing preservation outcomes with different cochlear implant electrodes: Nucleus® HybridTM-L24 and Nucleus FreedomTM CI422. Audiol. Neurotol. 2014, 19, 293–309. [Google Scholar] [CrossRef]
- Adunka, O.; Kiefer, J. Impact of electrode insertion depth on intracochlear trauma. Otolaryngol. Head Neck. Surg. 2006, 135, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Erixon, E.; Köbler, S.; Rask-Andersen, H. Cochlear implantation and hearing preservation: Results in 21 consecutively operated patients using the round window approach. Acta Otolaryngol. 2012, 132, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Helbig, S.; Helbig, M.; Leinung, M.; Stöver, T.; Baumann, U.; Rader, T. Hearing preservation and improved speech perception with a flexible 28-mm electrode. Otol. Neurotol. 2015, 36, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Tarabichi, O.; Jensen, M.; Hansen, M.R. Advances in hearing preservation in cochlear implant surgery. Curr. Opin. Otolaryngol. Head Neck. Surg. 2021, 29, 385–390. [Google Scholar] [CrossRef]
- Mertens, G.; Van de Heyning, P.; Vanderveken, O.; Topsakal, V.; Van Rompaey, V. The smaller the frequency-to-place mismatch the better the hearing outcomes in cochlear implant recipients? Eur. Arch. Otorhinolaryngol. 2022, 279, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Canfarotta, M.W.; O’Connell, B.P.; Buss, E.; Pillsbury, H.C.; Brown, K.D.; Dillon, M.T. Influence of Age at Cochlear Implantation and Frequency-to-Place Mismatch on Early Speech Recognition in Adults. Otolaryngol. Head Neck. Surg. 2020, 162, 926–932. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| 3D-Imaging-Based Choice | Implanted Array | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Relative Length | FLEX24 | FLEX26 | FLEX28 | FLEXsoft | FORM19 | FORM24 | MEDIUM | STANDARD | Total (%) | |
| Same | FLEX28 | 41 | 41 | |||||||
| FLEXsoft | 6 | 7 | 13 | |||||||
| Subtotal | 41 | 6 | 7 | 54 (47.4) | ||||||
| Shorter a | FLEX28 | 1 | 1 | 2 | 4 | |||||
| FLEXsoft | 2 | 1 | 30 | 1 | 1 | 35 | ||||
| Subtotal | 3 | 1 | 30 | 1 | 3 | 1 | 39 (34.2) | |||
| Longer b | FLEX20 | 2 | 3 | 1 | 6 | |||||
| FLEX24 | 1 | 1 | ||||||||
| FLEX26 | 4 | 1 | 5 | |||||||
| FLEX28 | 3 | 6 | 9 | |||||||
| Subtotal | 2 | 8 | 4 | 7 | 21 (18.4) | |||||
| Total | 5 | 9 | 75 | 6 | 1 | 3 | 1 | 14 | 114 | |
| Relative Length (n) | Statistic | CDL (mm) | AID (Deg): 3D-Imaging-Based Choice | AID (Deg): Implanted | C1 Frequency (Hz): 3D-Imaging-Based Choice | C1 Frequency (Hz): Implanted |
|---|---|---|---|---|---|---|
| Same (54) | Mean | 34.4 | 611.8 | 611.8 | 230.6 | 230.6 |
| Median | 34.2 | 605.3 | 605.3 | 227.6 | 227.6 | |
| SD | 1.7 | 28.8 | 28.8 | 78.1 | 78.1 | |
| Range | 31.6–39.6 | 566.3–680.0 | 566.3–680.0 | 124.6–562.7 | 124.6–562.7 | |
| Shorter a (39) | Mean | 36.2 | 637.1 | 511.4 | 181.5 | 433.9 |
| Median | 36.1 | 635.1 | 532.6 | 180.0 | 360.7 | |
| SD | 1.4 | 35.1 | 62.8 | 47.8 | 200.6 | |
| Range | 33.3–38.8 | 576.8–734.1 | 304.5–612.7 | 74.9–272.5 | 211.8–1311.7 | |
| Longer b (21) | Mean | 33.5 | 523.9 | 668.4 | 493.0 | 223.5 |
| Median | 33.6 | 593.2 | 695.4 | 418.8 | 115.8 | |
| SD | 2.3 | 119.2 | 112.8 | 355.2 | 202.2 | |
| Range | 27.9–38.3 | 315.7–655.0 | 459.5–851.7 | 153.0–1235.2 | 7.0–631.6 |
| Relative Length | Statistic | Pre-op CNC | 12-Month CNC |
|---|---|---|---|
| IE Aided | CI Alone | ||
| Same | N | 16 | 15 |
| Mean | 6.9 | 55.9 | |
| Median | 0.0 | 66.0 | |
| SD | 18.2 | 26.8 | |
| Range | 0–72 | 0–85 | |
| Shorter a | N | 13 | 9 |
| Mean | 10.4 | 42.7 | |
| Median | 0.0 | 51.0 | |
| SD | 18.0 | 22.3 | |
| Range | 0–53 | 3–68 | |
| Longer b | N | 7 | 6 |
| Mean | 21.7 | 63.8 | |
| Median | 0.0 | 75.5 | |
| SD | 28.9 | 31.4 | |
| Range | 0–65 | 0–82 |
| Relative Length | Statistic | S0N0 | S0NHE | SCINHE | |||
|---|---|---|---|---|---|---|---|
| Pre-op | 12-Month | Pre-op | 12-Month | Pre-op | 12-Month | ||
| Same | N | 7 | 7 | 5 | 5 | 7 | 7 |
| Mean | 4.6 | 2.4 | 0.0 | −1.8 | 5.6 | −0.2 | |
| Median | 4.0 | 2.0 | −1.0 | −2.5 | 4.0 | −0.5 | |
| SD | 2.2 | 2.1 | 3.7 | 3.3 | 3.5 | 3.0 | |
| Range | 1.5–8.5 | 0.0–5.0 | −5.0–5.0 | −5.0–3.0 | 2.0–10.5 | −3.5–5.0 | |
| Shorter a | N | 7 | 7 | 3 | 3 | 7 | 7 |
| Mean | 4.6 | 2.7 | −0.7 | −0.5 | 7.1 | 2.8 | |
| Median | 4.5 | 3.0 | −1.0 | 0.5 | 9.0 | 2.0 | |
| SD | 1.7 | 2.3 | 3.0 | 2.6 | 2.5 | 5.1 | |
| Range | 2.5–6.5 | −2.0–5.0 | −3.5–2.5 | −3.5–1.5 | 3.0–9.0 | −2.0–12.0 | |
| Longer b | N | 3 | 3 | 1 | 1 | 3 | 3 |
| Mean | 4.0 | 2.7 | −3.5 | −2.5 | 2.5 | −1.7 | |
| Median | 4.5 | 2.5 | −3.5 | −2.5 | 2.0 | −3.5 | |
| SD | 1.3 | 1.3 | − | − | 2.3 | 3.6 | |
| Range | 2.5–5.0 | 1.5–4.0 | − | − | 0.5–5.0 | −4.0–2.5 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Távora-Vieira, D.; Voola, M.; Kuthubutheen, J.; Friedland, P.; Gibson, D.; Acharya, A. Evaluation of the Performance of OTOPLAN-Based Cochlear Implant Electrode Array Selection: A Retrospective Study. J. Pers. Med. 2023, 13, 1276. https://doi.org/10.3390/jpm13081276
Távora-Vieira D, Voola M, Kuthubutheen J, Friedland P, Gibson D, Acharya A. Evaluation of the Performance of OTOPLAN-Based Cochlear Implant Electrode Array Selection: A Retrospective Study. Journal of Personalized Medicine. 2023; 13(8):1276. https://doi.org/10.3390/jpm13081276
Chicago/Turabian StyleTávora-Vieira, Dayse, Marcus Voola, Jafri Kuthubutheen, Peter Friedland, Daren Gibson, and Aanand Acharya. 2023. "Evaluation of the Performance of OTOPLAN-Based Cochlear Implant Electrode Array Selection: A Retrospective Study" Journal of Personalized Medicine 13, no. 8: 1276. https://doi.org/10.3390/jpm13081276
APA StyleTávora-Vieira, D., Voola, M., Kuthubutheen, J., Friedland, P., Gibson, D., & Acharya, A. (2023). Evaluation of the Performance of OTOPLAN-Based Cochlear Implant Electrode Array Selection: A Retrospective Study. Journal of Personalized Medicine, 13(8), 1276. https://doi.org/10.3390/jpm13081276