
Characteristics of Kidney Transplant Recipients with Prolonged Pre-Transplant Dialysis Duration as Identified by Machine Learning Consensus Clustering: Pathway to Personalized Care


 , , , ,
, , , ,  ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Data Collection
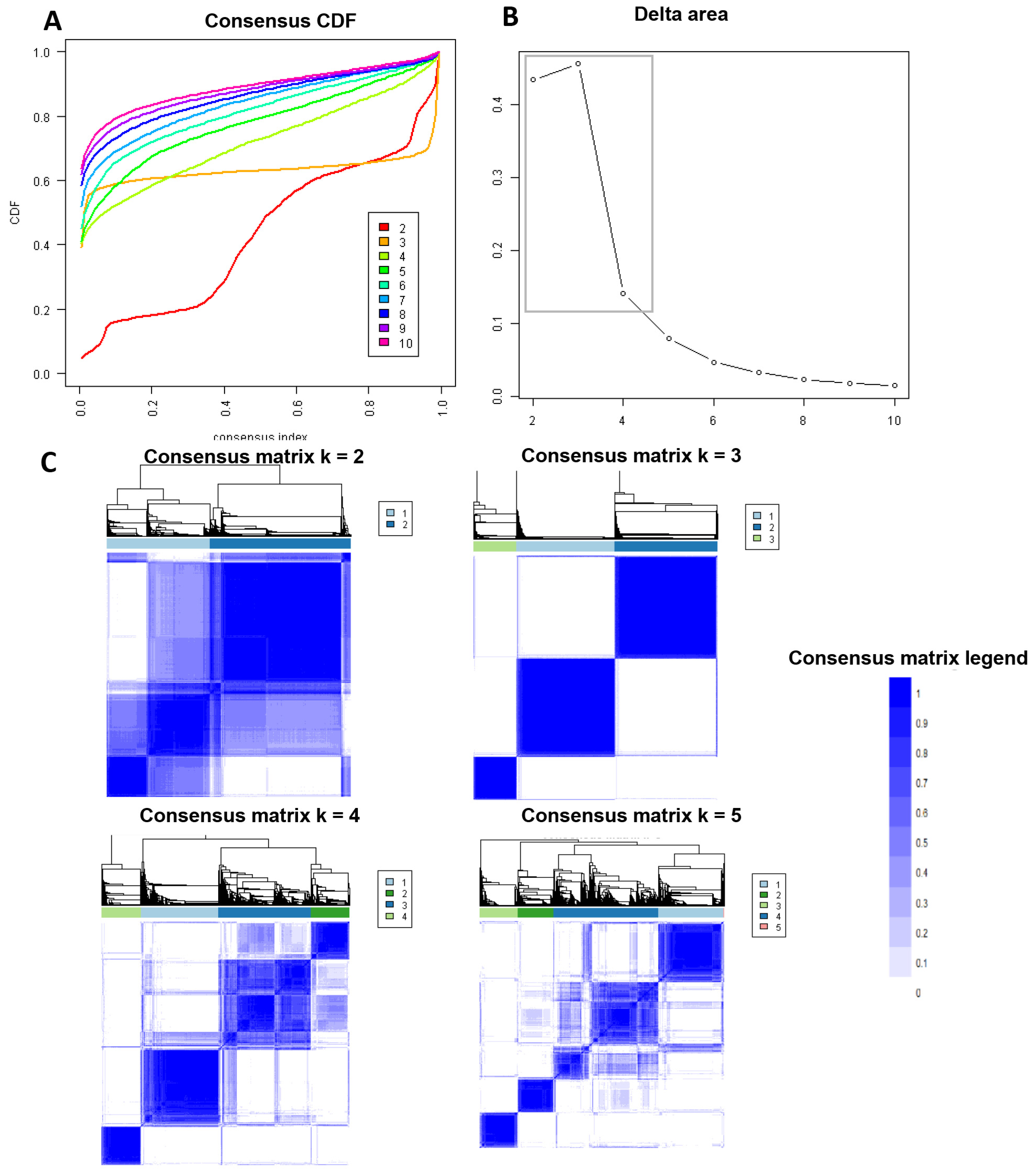
2.3. Clustering Analysis
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Each Kidney Transplant Cluster
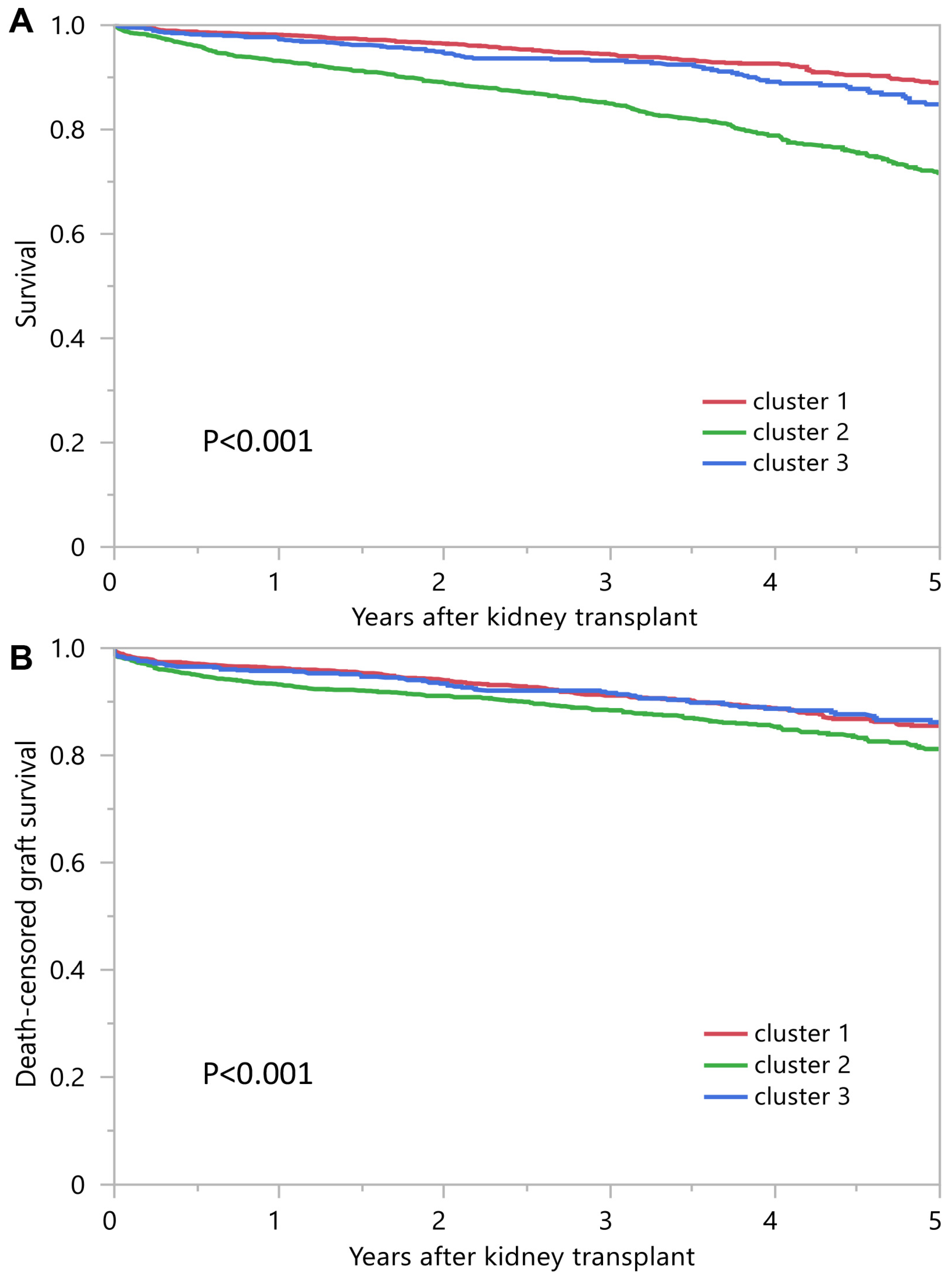
3.2. Posttransplant Outcomes of Each Kidney Transplant Cluster
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Queeley, G.L.; Campbell, E.S. Comparing Treatment Modalities for End-Stage Renal Disease: A Meta-Analysis. Am. Health Drug Benefits 2018, 11, 118–127. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Oniscu, G.C.; Brown, H.; Forsythe, J.L. Impact of cadaveric renal transplantation on survival in patients listed for transplantation. J. Am. Soc. Nephrol. 2005, 16, 1859–1865. [Google Scholar] [CrossRef] [PubMed]
- Rabbat, C.G.; Thorpe, K.E.; Russell, J.D.; Churchill, D.N. Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J. Am. Soc. Nephrol. 2000, 11, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef]
- Schold, J.D.; Mohan, S.; Huml, A.; Buccini, L.D.; Sedor, J.R.; Augustine, J.J.; Poggio, E.D. Failure to Advance Access to Kidney Transplantation over Two Decades in the United States. J. Am. Soc. Nephrol. 2021, 32, 913–926. [Google Scholar] [CrossRef] [PubMed]
- United States Renal Data System. 2021 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2021.
- Lentine, K.L.; Smith, J.M.; Hart, A.; Miller, J.; Skeans, M.A.; Larkin, L.; Robinson, A.; Gauntt, K.; Israni, A.K.; Hirose, R.; et al. OPTN/SRTR 2020 Annual Data Report: Kidney. Am. J. Transpl. 2022, 22 (Suppl. 2), 21–136. [Google Scholar] [CrossRef]
- Chertow, G.M.; Johansen, K.L.; Lew, N.; Lazarus, J.M.; Lowrie, E.G. Vintage, nutritional status, and survival in hemodialysis patients. Kidney Int. 2000, 57, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Meier-Kriesche, H.U.; Kaplan, B. Waiting time on dialysis as the strongest modifiable risk factor for renal transplant outcomes: A paired donor kidney analysis. Transplantation 2002, 74, 1377–1381. [Google Scholar] [CrossRef]
- Meier-Kriesche, H.U.; Port, F.K.; Ojo, A.O.; Rudich, S.M.; Hanson, J.A.; Cibrik, D.M.; Leichtman, A.B.; Kaplan, B. Effect of waiting time on renal transplant outcome. Kidney Int. 2000, 58, 1311–1317. [Google Scholar] [CrossRef]
- Aufhauser, D.D., Jr.; Peng, A.W.; Murken, D.R.; Concors, S.J.; Abt, P.L.; Sawinski, D.; Bloom, R.D.; Reese, P.P.; Levine, M.H. Impact of prolonged dialysis prior to renal transplantation. Clin. Transpl. 2018, 32, e13260. [Google Scholar] [CrossRef]
- Knoll, G.; Cockfield, S.; Blydt-Hansen, T.; Baran, D.; Kiberd, B.; Landsberg, D.; Rush, D.; Cole, E. Canadian Society of Transplantation consensus guidelines on eligibility for kidney transplantation. Cmaj 2005, 173, 1181–1184. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.C.; Sehgal, A.R. Barriers to cadaveric renal transplantation among blacks, women, and the poor. JAMA 1998, 280, 1148–1152. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; London, W.; Ellison, M.D. Race and socioeconomic factors influencing early placement on the kidney transplant waiting list. J. Am. Soc. Nephrol. 1998, 9, 2142–2147. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Matas, A.J.; Ellison, M.D.; Gill, J.S.; Kausz, A.T. Preemptive kidney transplantation: The advantage and the advantaged. J. Am. Soc. Nephrol. 2002, 13, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Schold, J.D.; Gregg, J.A.; Harman, J.S.; Hall, A.G.; Patton, P.R.; Meier-Kriesche, H.U. Barriers to evaluation and wait listing for kidney transplantation. Clin. J. Am. Soc. Nephrol. 2011, 6, 1760–1767. [Google Scholar] [CrossRef] [PubMed]
- Patzer, R.E.; Plantinga, L.C.; Paul, S.; Gander, J.; Krisher, J.; Sauls, L.; Gibney, E.M.; Mulloy, L.; Pastan, S.O. Variation in Dialysis Facility Referral for Kidney Transplantation Among Patients With End-Stage Renal Disease in Georgia. JAMA 2015, 314, 582–594. [Google Scholar] [CrossRef]
- Patzer, R.E.; McClellan, W.M. Influence of race, ethnicity and socioeconomic status on kidney disease. Nat. Rev. Nephrol. 2012, 8, 533–541. [Google Scholar] [CrossRef]
- Patzer, R.E.; Amaral, S.; Wasse, H.; Volkova, N.; Kleinbaum, D.; McClellan, W.M. Neighborhood poverty and racial disparities in kidney transplant waitlisting. J. Am. Soc. Nephrol. 2009, 20, 1333–1340. [Google Scholar] [CrossRef]
- MacEachern, S.J.; Forkert, N.D. Machine learning for precision medicine. Genome 2021, 64, 416–425. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kaewput, W.; Kovvuru, K.; Hansrivijit, P.; Kanduri, S.R.; Bathini, T.; Chewcharat, A.; Leeaphorn, N.; Gonzalez-Suarez, M.L.; Cheungpasitporn, W. Promises of Big Data and Artificial Intelligence in Nephrology and Transplantation. J. Clin. Med. 2020, 9, 1107. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Kashani, K. Electronic Data Systems and Acute Kidney Injury. Contrib. Nephrol. 2016, 187, 73–83. [Google Scholar] [CrossRef]
- Chaudhary, K.; Vaid, A.; Duffy, A.; Paranjpe, I.; Jaladanki, S.; Paranjpe, M.; Johnson, K.; Gokhale, A.; Pattharanitima, P.; Chauhan, K.; et al. Utilization of Deep Learning for Subphenotype Identification in Sepsis-Associated Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2020, 15, 1557–1565. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kaewput, W.; Choudhury, A.; Hansrivijit, P.; Mao, M.A.; Cheungpasitporn, W. Is It Time for Machine Learning Algorithms to Predict the Risk of Kidney Failure in Patients with Chronic Kidney Disease? J. Clin. Med. 2021, 10, 1121. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Hansrivijit, P.; Bathini, T.; Vallabhajosyula, S.; Mekraksakit, P.; Kaewput, W.; Cheungpasitporn, W. Predicting Acute Kidney Injury after Cardiac Surgery by Machine Learning Approaches. J. Clin. Med. 2020, 9, 1767. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Vaitla, P.; Nissaisorakarn, V.; Mao, M.A.; Genovez, J.L.Z.; Kattah, A.G.; Pattharanitima, P.; Vallabhajosyula, S.; Keddis, M.T.; Qureshi, F.; et al. Clinically Distinct Subtypes of Acute Kidney Injury on Hospital Admission Identified by Machine Learning Consensus Clustering. Med. Sci. 2021, 9, 60. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Yoon, H.K.; Nam, K.; Cho, Y.J.; Kim, T.K.; Kim, W.H.; Bahk, J.H. Derivation and Validation of Machine Learning Approaches to Predict Acute Kidney Injury after Cardiac Surgery. J. Clin. Med. 2018, 7, 322. [Google Scholar] [CrossRef] [PubMed]
- Geubbels, N.; de Brauw, L.M.; Acherman, Y.I.; van de Laar, A.W.; Bruin, S.C. Risk Stratification Models: How Well do They Predict Adverse Outcomes in a Large Dutch Bariatric Cohort? Obes. Surg. 2015, 25, 2290–2301. [Google Scholar] [CrossRef]
- Stenberg, E.; Cao, Y.; Szabo, E.; Naslund, E.; Naslund, I.; Ottosson, J. Risk Prediction Model for Severe Postoperative Complication in Bariatric Surgery. Obes. Surg. 2018, 28, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Monti, S.; Tamayo, P.; Mesirov, J.; Golub, T. Consensus clustering: A resampling-based method for class discovery and visualization of gene expression microarray data. Mach. Learn. 2003, 52, 91–118. [Google Scholar] [CrossRef]
- Wilkerson, M.D.; Hayes, D.N. ConsensusClusterPlus: A class discovery tool with confidence assessments and item tracking. Bioinformatics 2010, 26, 1572–1573. [Google Scholar] [CrossRef] [PubMed]
- Șenbabaoğlu, Y.; Michailidis, G.; Li, J.Z. Critical limitations of consensus clustering in class discovery. Sci. Rep. 2014, 4, 6207. [Google Scholar] [CrossRef]
- USRDS Annual Data Report—2019. Available online: www.usrds.org/media/2371/2019-executive-summary.pdf (accessed on 5 December 2021).
- Purnell, T.S.; Hall, Y.N.; Boulware, L.E. Understanding and overcoming barriers to living kidney donation among racial and ethnic minorities in the United States. Adv. Chronic Kidney Dis. 2012, 19, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Alvaro, E.M.; Siegel, J.T.; Turcotte, D.; Lisha, N.; Crano, W.D.; Dominick, A. Living kidney donation among Hispanics: A qualitative examination of barriers and opportunities. Prog. Transpl. 2008, 18, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Boulware, L.E.; Hill-Briggs, F.; Kraus, E.S.; Melancon, J.K.; Senga, M.; Evans, K.E.; Troll, M.U.; Ephraim, P.; Jaar, B.G.; Myers, D.I.; et al. Identifying and addressing barriers to African American and non-African American families’ discussions about preemptive living related kidney transplantation. Prog. Transpl. 2011, 21, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Waterman, A.D.; Stanley, S.L.; Covelli, T.; Hazel, E.; Hong, B.A.; Brennan, D.C. Living donation decision making: Recipients’ concerns and educational needs. Prog. Transpl. 2006, 16, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Rodrigue, J.R.; Cornell, D.L.; Kaplan, B.; Howard, R.J. A randomized trial of a home-based educational approach to increase live donor kidney transplantation: Effects in blacks and whites. Am. J. Kidney Dis. 2008, 51, 663–670. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 5092) | Cluster 1 (n = 2043) | Cluster 2 (n = 2153) | Cluster 3 (n = 896) | p-Value | |
|---|---|---|---|---|---|
| Recipient age (year) | 50.5 ± 10.9 | 43.6 ± 9.3 | 56.9 ± 8.6 | 51.1 ± 10.1 | <0.001 |
| Recipient male sex | 2990 (59) | 1375 (67) | 1426 (66) | 192 (21) | <0.001 |
| Recipient race | <0.001 | ||||
| - White | 709 (14) | 266 (13) | 260 (12) | 709 (14) | |
| - Black | 2655 (52) | 934 (46) | 1324 (62) | 2655 (52) | |
| - Hispanic | 1286 (25) | 649 (32) | 403 (19) | 1286 (25) | |
| - Other | 442 (9) | 194 (10) | 166 (8) | 442 (9) | |
| ABO blood group | 0.007 | ||||
| - A | 1109 (22) | 438 (21) | 445 (21) | 226 (25) | |
| - B | 856 (22) | 336 (16) | 398 (18) | 122 (14) | |
| - AB | 120 (17) | 56 (3) | 45 (2) | 19 (2) | |
| - O | 3007 (59) | 1213 (59) | 1265 (59) | 529 (59) | |
| Body mass index (kg/m2) | 28.0 ± 6.0 | 25.6 ± 5.0 | 30.4 ± 5.8 | 27.6 ± 6.0 | <0.001 |
| Dialysis duration (year), median (Q25, Q75) | 11.8 (10.7–13.9) | 11.9 (10.7–14.0) | 11.5 (10.6–13.3) | 12.4 (10.9–15.3) | <0.001 |
| Cause of end-stage kidney disease | <0.001 | ||||
| - Diabetes mellitus | 851 (17) | 70 (3) | 668 (31) | 113 (13) | |
| - Hypertension | 2111 (41) | 878 (43) | 917 (43) | 316 (35) | |
| - Glomerular disease | 1058 (21) | 575 (28) | 251 (12) | 232 (26) | |
| - PKD | 300 (6) | 109 (5) | 128 (6) | 63 (7) | |
| - Other | 772 (15) | 411 (20) | 189 (9) | 172 (19) | |
| Comorbidity | |||||
| - Diabetes mellitus | 1056 (21) | 96 (5) | 812 (38) | 148 (17) | <0.001 |
| - Malignancy | 423 (8) | 120 (6) | 229 (11) | 74 (8) | <0.001 |
| - Peripheral vascular disease | 535 (11) | 123 (6) | 332 (15) | 80 (9) | <0.001 |
| PRA, median (Q25, Q75) | 0 (0,24) | 0 (0,0) | 0 (0,0) | 85 (66,98) | <0.001 |
| Positive HCV serostatus | 393 (8) | 124 (6) | 203 (9) | 66 (7) | <0.001 |
| Positive HBs antigen | 148 (3) | 65 (3) | 65 (3) | 18 (2) | 0.202 |
| Positive HIV serostatus | 262 (5) | 136 (7) | 107 (5) | 19 (2) | <0.001 |
| Functional status | <0.001 | ||||
| - 10–30% | 13 (0) | 2 (0) | 8 (0) | 3 (0) | |
| - 40–70% | 2439 (48) | 848 (42) | 1144 (53) | 447 (50) | |
| - 80–100% | 2640 (52) | 1193 (58) | 1001 (46) | 446 (50) | |
| Working income | 886 (17) | 472 (23) | 272 (13) | 142 (16) | <0.001 |
| Public insurance | 4661 (92) | 1835 (90) | 2011 (93) | 815 (91) | <0.001 |
| US resident | 4858 (95) | 1881 (92) | 2114 (98) | 863 (96) | <0.001 |
| Undergraduate education or above | 1985 (39) | 728 (36) | 899 (42) | 358 (40) | <0.001 |
| Serum albumin (g/dL) | 4.0 ± 0.6 | 4.2 ± 0.6 | 3.9 ± 0.5 | 4.0 ± 0.6 | 0.335 |
| Kidney donor status | <0.001 | ||||
| - Non-ECD deceased | 4457 (88) | 1937 (95) | 1726 (80) | 794 (89) | |
| - ECD deceased | 456 (9) | 25 (1) | 379 (18) | 52 (6) | |
| - Living | 179 (4) | 81 (4) | 48 (2) | 50 (6) | |
| Donor age | 37.9 ± 14.5 | 30.7 ± 13.5 | 45.1 ± 11.7 | 36.7 ± 14.3 | <0.001 |
| Donor male sex | 2998 (59) | 1223 (60) | 1248 (58) | 527 (59) | 0.458 |
| Donor race | <0.001 | ||||
| - White | 2871 (56) | 1049 (51) | 1343 (62) | 479 (53) | |
| - Black | 950 (19) | 423 (21) | 346 (16) | 181 (20) | |
| - Hispanic | 984 (19) | 453 (22) | 342 (16) | 189 (21) | |
| - Other | 287 (6) | 118 (6) | 122 (6) | 47 (5) | |
| History of hypertension in donor | 1275 (25) | 243 (12) | 822 (38) | 210 (23) | <0.001 |
| KDPI | <0.001 | ||||
| - Living donor | 179 (4) | 81 (4) | 48 (2) | 50 (6) | |
| - KDPI < 85 | 4707 (92) | 1958 (96) | 1928 (90) | 821 (92) | |
| - KDPI ≥ 85 | 206 (4) | 4 (0) | 177 (8) | 25 (3) | |
| HLA mismatch, median (Q25, Q75) | 5 (4, 5) | 5 (4, 6) | 5 (4, 6) | 4 (2, 5) | <0.001 |
| Cold ischemia time (hours) | 16.1 ± 8.8 | 15.1 ± 8.4 | 17.2 ± 9.2 | 16.1 ± 8.3 | <0.001 |
| Kidney on pump | 2011 (39) | 662 (32) | 1048 (49) | 301 (34) | <0.001 |
| Delay graft function | 1829 (36) | 596 (29) | 970 (45) | 263 (29) | <0.001 |
| Allocation type | <0.001 | ||||
| - Local | 4197 (82) | 1808 (89) | 1797 (83) | 592 (66) | |
| - Regional | 449 (9) | 125 (6) | 215 (10) | 109 (12) | |
| - National | 446 (9) | 110 (5) | 141 (7) | 195 (22) | |
| EBV status | 0.888 | ||||
| - Low risk | 26 (1) | 10 (0) | 10 (0) | 6 (1) | |
| - Moderate risk | 4626 (91) | 1849 (91) | 1963 (91) | 814 (91) | |
| - High risk | 440 (9) | 184 (9) | 180 (8) | 76 (8) | |
| CMV status | 0.088 | ||||
| - D−/R− | 440 (9) | 186 (9) | 191 (9) | 63 (7) | |
| - D−/R+ | 1427 (28) | 599 (26) | 577 (27) | 251 (28) | |
| - D+/R+ | 2505 (49) | 972 (48) | 1064 (49) | 469 (52) | |
| - D+/R− | 720 (14) | 286 (14) | 321 (15) | 113 (13) | |
| Induction immunosuppression | |||||
| - Thymoglobulin | 2975 (58) | 1161 (57) | 1192 (55) | 622 (69) | <0.001 |
| - Alemtuzumab | 714 (14) | 247 (12) | 324 (15) | 143 (16) | 0.004 |
| - Basiliximab | 1117 (22) | 529 (26) | 505 (23) | 83 (9) | <0.001 |
| - Other | 83 (2) | 29 (1) | 43 (2) | 11 (1) | 0.194 |
| - No induction | 429 (8) | 175 (9) | 193 (9) | 61 (7) | 0.142 |
| Maintenance Immunosuppression | |||||
| - Tacrolimus | 4703 (92) | 1897 (93) | 1977 (92) | 829 (93) | 0.447 |
| - Cyclosporine | 76 (1) | 35 (2) | 29 (1) | 12 (1) | 0.568 |
| - Mycophenolate | 4806 (94) | 1944 (95) | 2010 (93) | 852 (95) | 0.025 |
| - Azathioprine | 7 (0) | 5 (0) | 2 (0) | 0 (0) | 0.196 |
| - mTOR inhibitors | 31 (1) | 15 (1) | 12 (1) | 4 (0) | 0.602 |
| - Steroid | 3783 (74) | 1547 (76) | 1534 (71) | 702 (78) | <0.001 |
| Cluster 1 | Cluster 2 | Cluster 3 | |
|---|---|---|---|
| 1-year death-censored graft survival | 96.3% | 93.2% | 95.8% |
| HR for 1-year death-censored graft failure | 1 (ref) | 1.84 (1.38–2.44) | 1.16 (0.77–1.72) |
| 5-year death-censored graft survival | 85.5% | 81.2% | 86.2% |
| HR for 5-year death-censored graft failure | 1 (ref) | 1.40 (1.16–1.71) | 1.00 (0.76–1.30) |
| 1-year survival | 98.2% | 93.2% | 97.3% |
| HR for 1-year death | 1 (ref) | 3.75 (2.61–5.52) | 1.45 (0.84–2.46) |
| 5-year survival | 89.0% | 71.5% | 84.8% |
| HR for 5-year death | 1 (ref) | 2.98 (2.43–3.68) | 1.38 (1.03–1.84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Tangpanithandee, S.; Jadlowiec, C.C.; Mao, S.A.; Mao, M.A.; Vaitla, P.; Acharya, P.C.; Leeaphorn, N.; Kaewput, W.; Pattharanitima, P.; et al. Characteristics of Kidney Transplant Recipients with Prolonged Pre-Transplant Dialysis Duration as Identified by Machine Learning Consensus Clustering: Pathway to Personalized Care. J. Pers. Med. 2023, 13, 1273. https://doi.org/10.3390/jpm13081273
Thongprayoon C, Tangpanithandee S, Jadlowiec CC, Mao SA, Mao MA, Vaitla P, Acharya PC, Leeaphorn N, Kaewput W, Pattharanitima P, et al. Characteristics of Kidney Transplant Recipients with Prolonged Pre-Transplant Dialysis Duration as Identified by Machine Learning Consensus Clustering: Pathway to Personalized Care. Journal of Personalized Medicine. 2023; 13(8):1273. https://doi.org/10.3390/jpm13081273
Chicago/Turabian StyleThongprayoon, Charat, Supawit Tangpanithandee, Caroline C. Jadlowiec, Shennen A. Mao, Michael A. Mao, Pradeep Vaitla, Prakrati C. Acharya, Napat Leeaphorn, Wisit Kaewput, Pattharawin Pattharanitima, and et al. 2023. "Characteristics of Kidney Transplant Recipients with Prolonged Pre-Transplant Dialysis Duration as Identified by Machine Learning Consensus Clustering: Pathway to Personalized Care" Journal of Personalized Medicine 13, no. 8: 1273. https://doi.org/10.3390/jpm13081273
APA StyleThongprayoon, C., Tangpanithandee, S., Jadlowiec, C. C., Mao, S. A., Mao, M. A., Vaitla, P., Acharya, P. C., Leeaphorn, N., Kaewput, W., Pattharanitima, P., Suppadungsuk, S., Krisanapan, P., Nissaisorakarn, P., Cooper, M., Craici, I. M., & Cheungpasitporn, W. (2023). Characteristics of Kidney Transplant Recipients with Prolonged Pre-Transplant Dialysis Duration as Identified by Machine Learning Consensus Clustering: Pathway to Personalized Care. Journal of Personalized Medicine, 13(8), 1273. https://doi.org/10.3390/jpm13081273