
Prognostic Value of Post-PCI Angiography-Derived Fractional Flow Reserve: A Systematic Review and Meta-Analysis of Cohort Studies

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Research
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
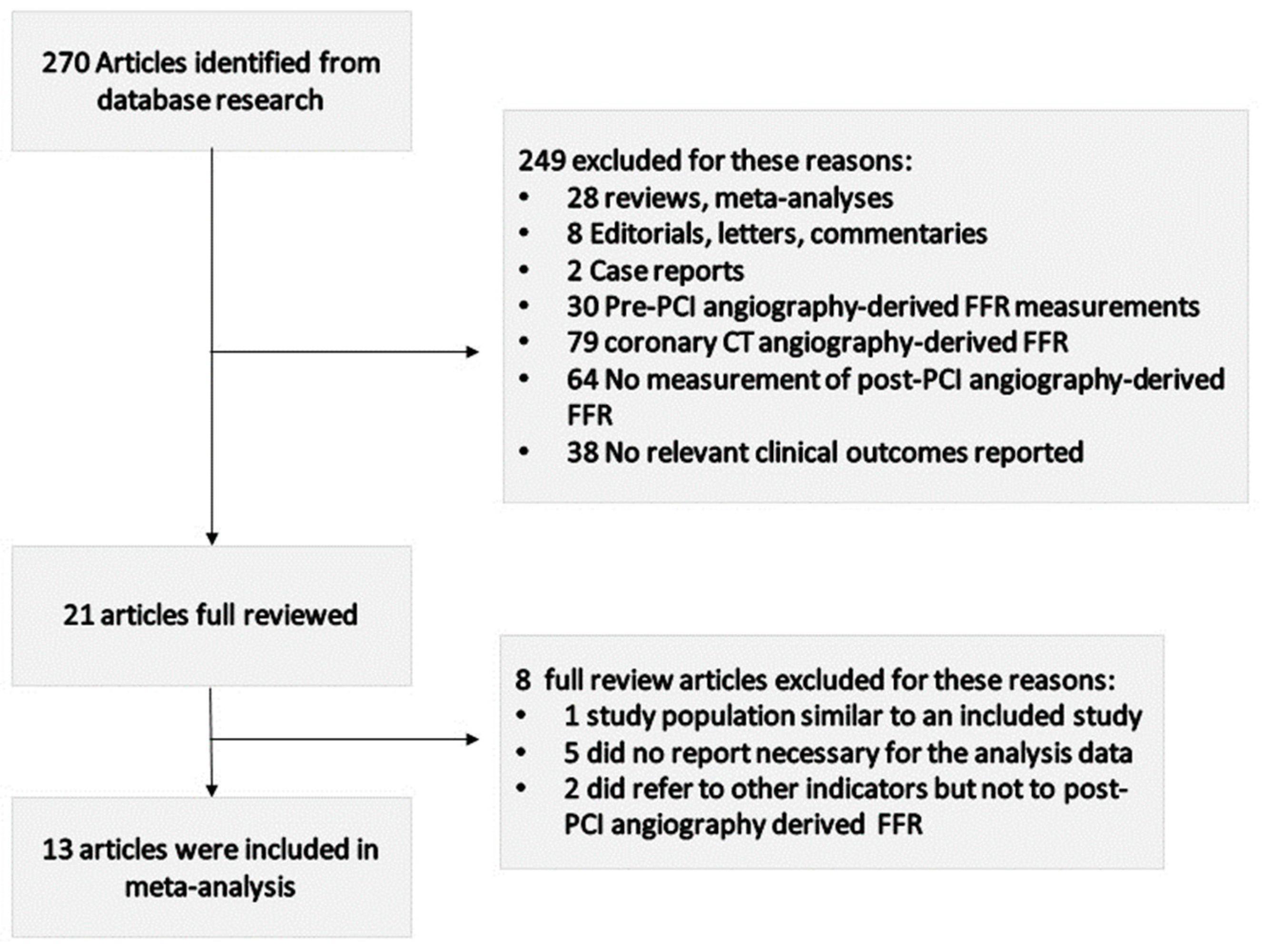
3.1. Literature Search Results
3.2. Study Characteristics
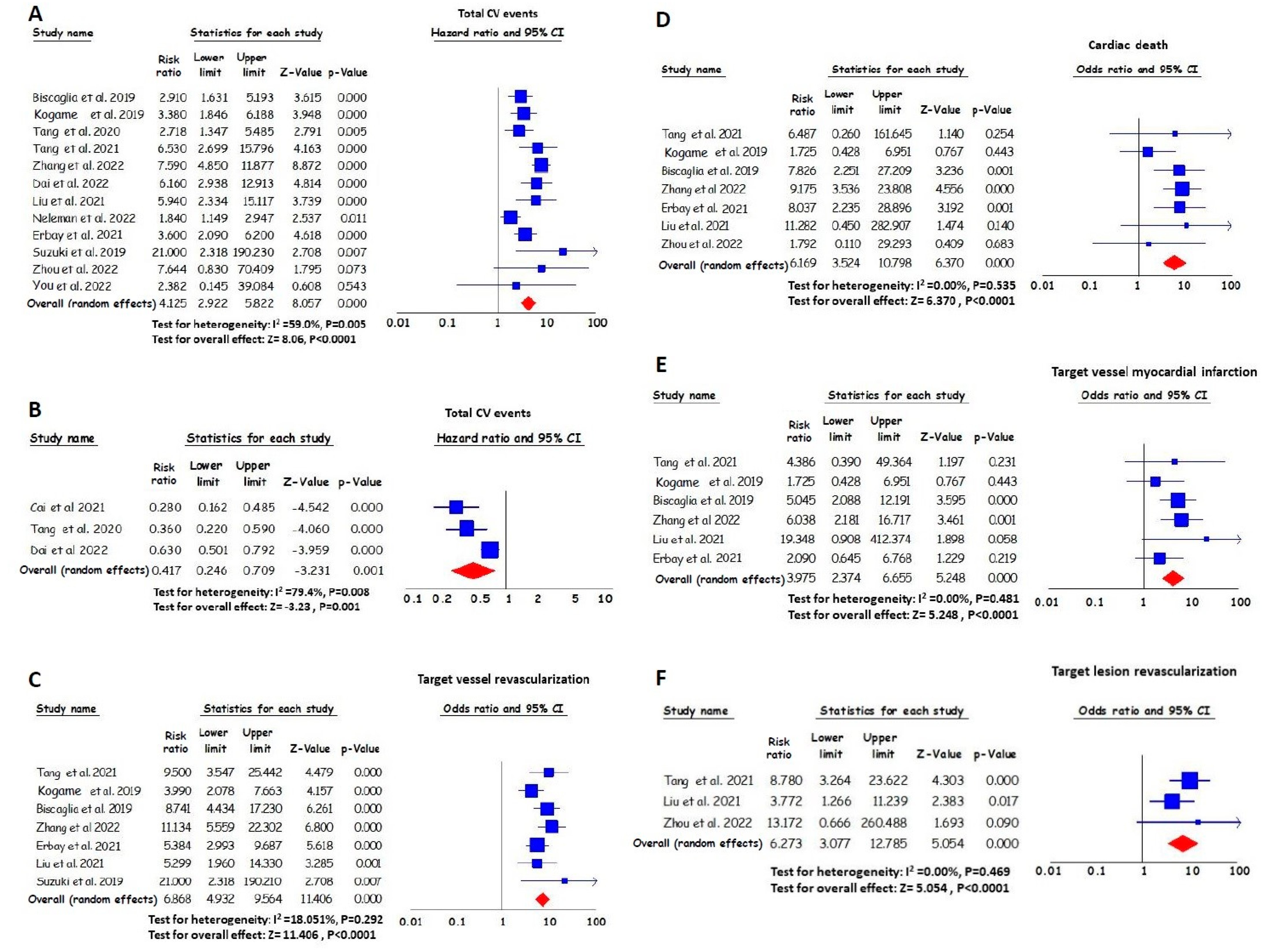
3.3. The Effect of the Post-PCI Angiography-Derived FFR on Total Cardiovascular Events
3.4. The Effect of the Post-PCI Angiography-Derived FFR on TVR
3.5. The Effect of the Post-PCI Angiography-Derived FFR on Cardiac Death
3.6. The Effect of the Post-PCI Angiography-Derived FFR on Target Vessel MI
3.7. The Effect of the Post-PCI Angiography-Derived FFR on TLR
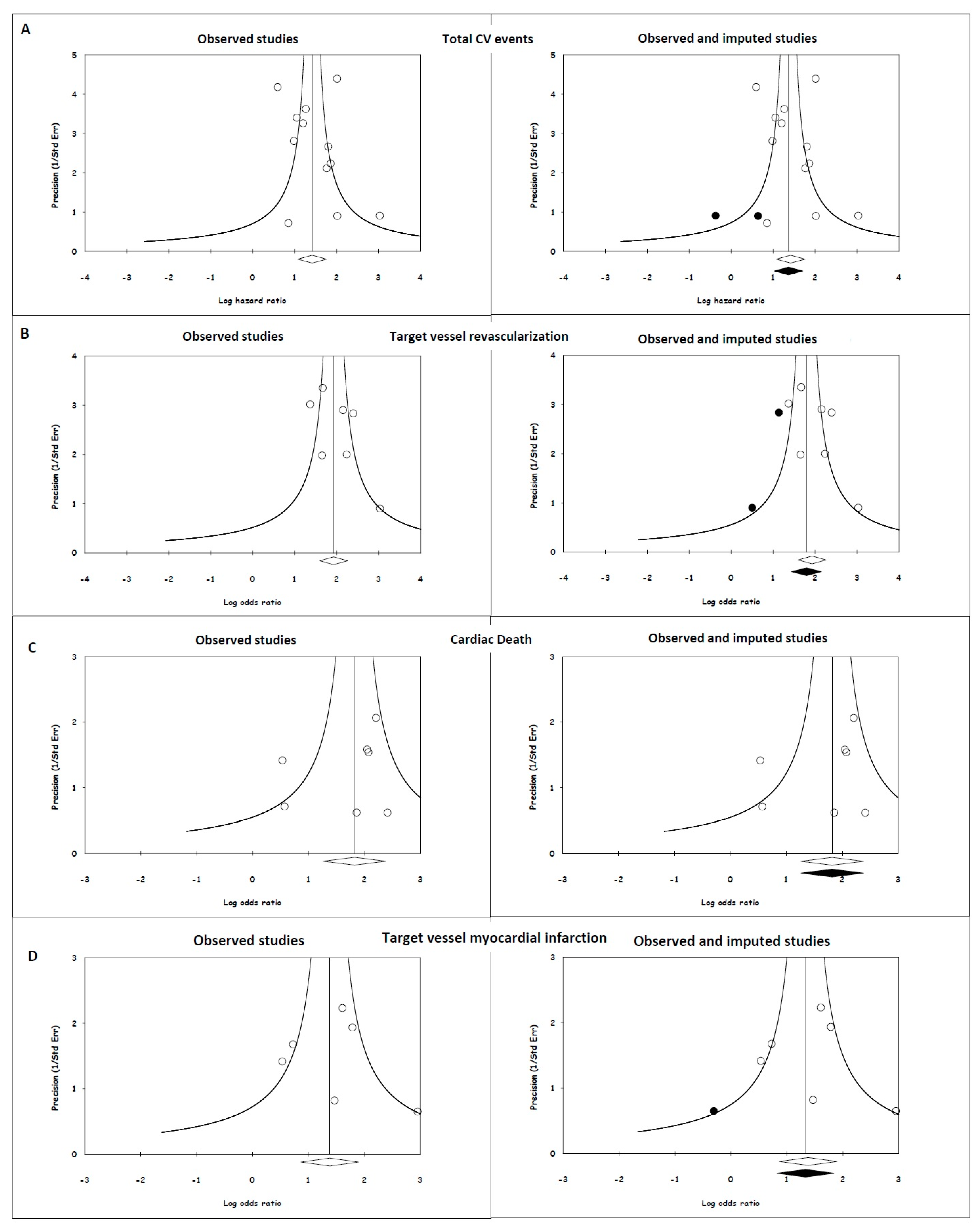
3.8. Publication Bias
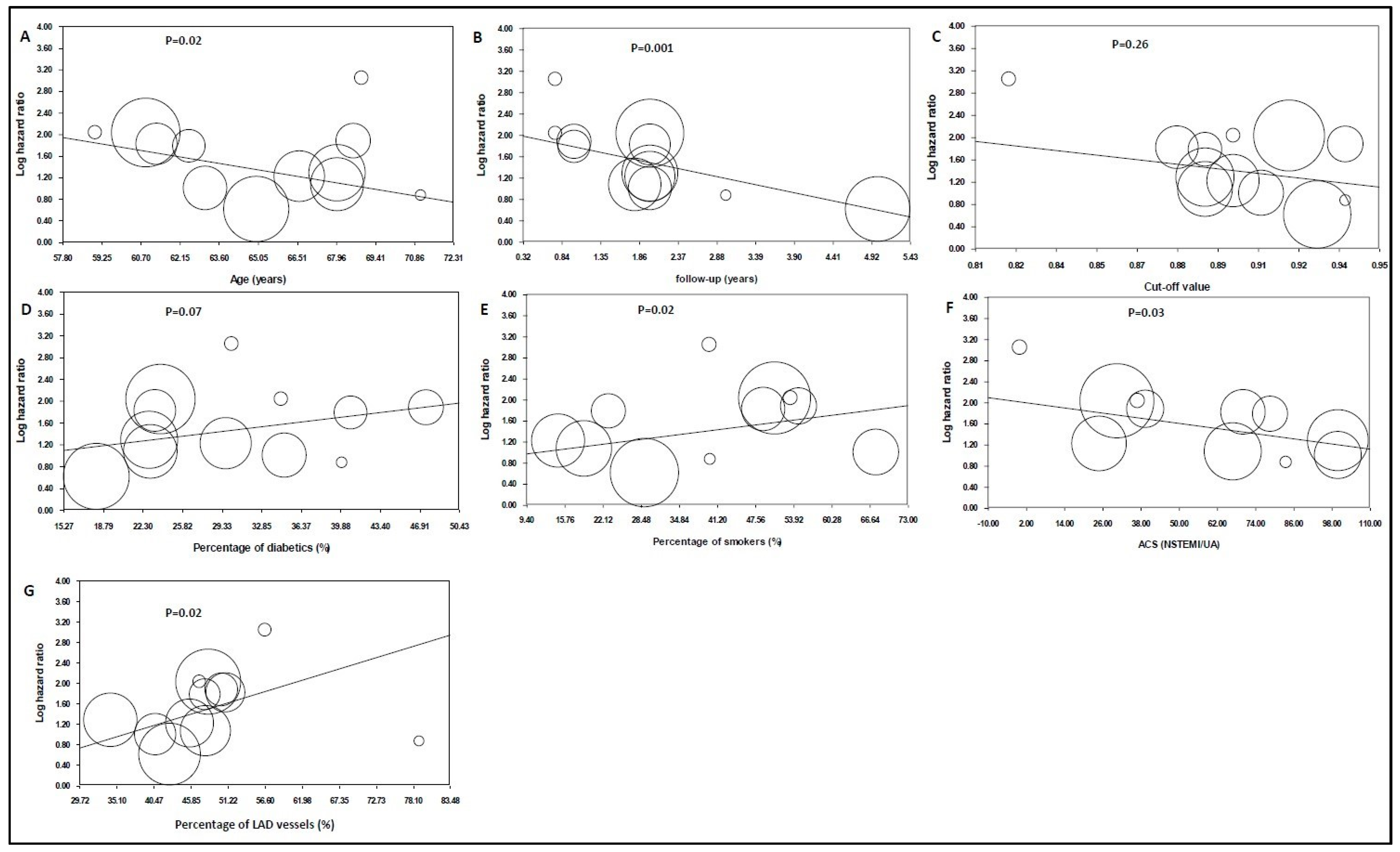
3.9. Meta-Regression Analysis
4. Discussion
4.1. Clinical Implications
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; Alkatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S.; et al. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef] [PubMed]
- Chacko, L.; Howard, J.; Rajkumar, C.; Nowbar, A.N.; Kane, C.; Mahdi, D.; Foley, M.; Shun-Shin, M.; Cole, G.; Sen, S.; et al. Effects of Percutaneous Coronary Intervention on Death and Myocardial Infarction Stratified by Stable and Unstable Coronary Artery Disease: A Meta-Analysis of Randomized Controlled Trials. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006363. [Google Scholar] [CrossRef] [PubMed]
- Sedlis, S.P.; Hartigan, P.M.; Teo, K.K.; Maron, D.J.; Spertus, J.A.; Mancini, G.J.; Kostuk, W.; Chaitman, B.R.; Berman, D.; Lorin, J.D.; et al. Effect of PCI on Long-Term Survival in Patients with Stable Ischemic Heart Disease. N. Engl. J. Med. 2015, 373, 1937–1946. [Google Scholar] [CrossRef] [PubMed]
- van Nunen, L.X.; Zimmermann, F.M.; Tonino, P.A.; Barbato, E.; Baumbach, A.; Engstrøm, T.; Klauss, V.; MacCarthy, P.A.; Manoharan, G.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet 2015, 7, 1853–1860. [Google Scholar] [CrossRef] [PubMed]
- Xaplanteris, P.; Fournier, S.; Pijls, N.H.; Fearon, W.F.; Barbato, E.; Tonino, P.A.; Engstrøm, T.; Kääb, S.; Dambrink, J.H.; Rioufol, G.; et al. Five-Year Outcomes with PCI Guided by Fractional Flow Reserve. N. Engl. J. Med. 2018, 379, 250–259. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Terentes-Printzios, D.; Oikonomou, D.; Gkini, K.-P.; Gardikioti, V.; Aznaouridis, K.; Dima, I.; Tsioufis, K.; Vlachopoulos, C. Angiography-based estimation of coronary physiology: A frame is worth a thousand words. Trends Cardiovasc. Med. 2022, 32, 366–374. [Google Scholar] [CrossRef]
- Buono, A.; Mühlenhaus, A.; Schäfer, T.; Trieb, A.-K.; Schmeißer, J.; Koppe, F.; Münzel, T.; Anadol, R.; Gori, T. QFR Predicts the Incidence of Long-Term Adverse Events in Patients with Suspected CAD: Feasibility and Reproducibility of the Method. J. Clin. Med. 2020, 9, 220. [Google Scholar] [CrossRef]
- Choi, K.H.; Lee, S.H.; Lee, J.M.; Hwang, D.; Zhang, J.; Kim, J.; Im, S.Y.; Kim, H.K.; Nam, C.W.; Doh, J.H.; et al. Clinical relevance and prognostic implications of contrast quantitative flow ratio in patients with coronary artery disease. Int. J. Cardiol. 2021, 325, 23–29. [Google Scholar] [CrossRef]
- Xu, B.; Tu, S.; Song, L.; Jin, Z.; Yu, B.; Fu, G.; Zhou, Y.; Wang, J.A.; Chen, Y.; Pu, J.; et al. Angiographic quantitative flow ratio-guided coronary intervention (FAVOR III China): A multicentre, randomised, sham-controlled trial. Lancet 2021, 398, 2149–2159. [Google Scholar] [CrossRef]
- Song, L.; Xu, B.; Tu, S.; Guan, C.; Jin, Z.; Yu, B.; Fu, G.; Zhou, Y.; Wang, J.A.; Chen, Y.; et al. 2-Year Outcomes of Angiographic Quantitative Flow Ratio-Guided Coronary Interventions. J. Am. Coll. Cardiol. 2022, 80, 2089–2101. [Google Scholar] [CrossRef]
- De Luca, L.; Rosano, G.M.; Spoletini, I. Post-percutaneous coronary intervention angina: From physiopathological mechanisms to individualized treatment. Cardiol. J. 2022, 29, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.K.; Kasula, S.; Hacioglu, Y.; Ahmed, Z.; Uretsky, B.F.; Hakeem, A. Utilizing Post-Intervention Fractional Flow Reserve to Optimize Acute Results and the Relationship to Long-Term Outcomes. JACC Cardiovasc. Interv. 2016, 9, 1022–1031. [Google Scholar] [CrossRef] [PubMed]
- Piroth, Z.; Toth, G.G.; Tonino, P.A.; Barbato, E.; Aghlmandi, S.; Curzen, N.; Rioufol, G.; Pijls, N.H.; Fearon, W.F.; Jüni, P.; et al. Prognostic Value of Fractional Flow Reserve Measured Immediately After Drug-Eluting Stent Implantation. Circ. Cardiovasc. Interv. 2017, 10, e005233. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Huang, J.; Westra, J.; Cohen, D.J.; Chen, Y.; Andersen, B.K.; Holm, N.R.; Xu, B.; Tu, S.; Wijns, W. Immediate post-procedural functional assessment of percutaneous coronary intervention: Current evidence and future directions. Eur. Heart J. 2021, 42, 2695–2707. [Google Scholar] [CrossRef]
- Liu, L.; Ding, F.; Gutiérrez-Chico, J.L.; Zhu, J.; Zhu, Z.; Du, R.; Yang, Z.; Hu, J.; Tu, S.; Zhang, R. Prognostic value of post-procedural μQFR for drug-coated balloons in the treatment of in-stent restenosis. Cardiol. J. 2023, 30, 167–177. [Google Scholar] [CrossRef]
- You, W.; Zhou, Y.; Wu, Z.; Meng, P.; Pan, D.; Yin, D.; Yang, S.; Wu, X.; Ye, F. Post-PCI quantitative flow ratio predicts 3-year outcome after rotational atherectomy in patients with heavily calcified lesions. Clin. Cardiol. 2022, 45, 558–566. [Google Scholar] [CrossRef]
- Zhang, R.; Wu, S.; Yuan, S.; Guan, C.; Zou, T.; Qiao, Z.; Xie, L.; Wang, H.; Song, L.; Xu, B.; et al. Effects of diabetes mellitus on post-intervention coronary physiological assessment derived by quantitative flow ratio in patients with coronary artery disease underwent percutaneous coronary intervention. Diabetes Res. Clin. Pract. 2022, 186, 109839. [Google Scholar] [CrossRef]
- Dai, N.; Yuan, S.; Dou, K.; Zhang, R.; Hu, N.; He, J.; Guan, C.; Zou, T.; Qiao, Z.; Duan, S.; et al. Prognostic Implications of Prestent Pullback Pressure Gradient and Poststent Quantitative Flow Ratio in Patients Undergoing Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2022, 11, e024903. [Google Scholar] [CrossRef]
- Tang, J.; Chu, J.; Hou, H.; Lai, Y.; Tu, S.; Chen, F.; Yao, Y.; Ye, Z.; Gao, Y.; Mao, Y.; et al. Clinical implication of QFR in patients with ST-segment elevation myocardial infarction after drug-eluting stent implantation. Int. J. Cardiovasc. Imaging 2021, 37, 755–766. [Google Scholar] [CrossRef]
- Cai, X.; Tian, F.; Jing, J.; Jin, Q.; Zhou, S.; Yin, W.; Chen, Y.; Wu, Q.; Fu, Z.; Chen, Y. Prognostic value of quantitative flow ratio measured immediately after drug-coated balloon angioplasty for in-stent restenosis. Catheter. Cardiovasc. Interv. 2021, 97, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Hou, H.; Chu, J.; Chen, F.; Yao, Y.; Gao, Y.; Ye, Z.; Zhuang, S.; Lai, Y.; Liu, X. Clinical implication of quantitative flow ratio to predict clinical events after drug-coated balloon angioplasty in patients with in-stent restenosis. Clin. Cardiol. 2021, 44, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Erbay, A.; Penzel, L.; Abdelwahed, Y.S.; Klotsche, J.; Heuberger, A.; Schatz, A.S.; Steiner, J.; Haghikia, A.; Sinning, D.; Fröhlich, G.M.; et al. Prognostic Impact of Pancoronary Quantitative Flow Ratio Assessment in Patients Undergoing Percutaneous Coronary Intervention for Acute Coronary Syndromes. Circ. Cardiovasc. Interv. 2021, 14, e010698. [Google Scholar] [CrossRef] [PubMed]
- Biscaglia, S.; Tebaldi, M.; Brugaletta, S.; Cerrato, E.; Erriquez, A.; Passarini, G.; Ielasi, A.; Spitaleri, G.; Di Girolamo, D.; Mezzapelle, G.; et al. Prognostic Value of QFR Measured Immediately After Successful Stent Implantation: The International Multicenter Prospective HAWKEYE Study. JACC Cardiovasc. Interv. 2019, 12, 2079–2088. [Google Scholar] [CrossRef] [PubMed]
- Kogame, N.; Takahashi, K.; Tomaniak, M.; Chichareon, P.; Modolo, R.; Chang, C.C.; Komiyama, H.; Katagiri, Y.; Asano, T.; Stables, R.; et al. Clinical Implication of Quantitative Flow Ratio After Percutaneous Coronary Intervention for 3-Vessel Disease. JACC Cardiovasc. Interv. 2019, 12, 2064–2075. [Google Scholar] [CrossRef]
- Suzuki, N.; Nishide, S.; Kimura, T.; Aoyagi, T.; Kanamori, K.; Shiratori, Y.; Hayami, N.; Murakawa, Y.; Kozuma, K. Relationship of quantitative flow ratio after second-generation drug-eluting stent implantation to clinical outcomes. Heart Vessels 2020, 35, 743–749. [Google Scholar] [CrossRef]
- Neleman, T.; Scoccia, A.; Masdjedi, K.; Tomaniak, M.; Ligthart, J.M.; Witberg, K.T.; Vermaire, A.; Wolff, Q.; Visser, L.; Cummins, P.; et al. The prognostic value of angiography-based vessel fractional flow reserve after percutaneous coronary intervention: The FAST Outcome study. Int. J. Cardiol. 2022, 15, 14–19. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhu, B.; Fan, F.; Yang, F.; Fang, S.; Wang, Z.; Qiu, L.; Gong, Y.; Huo, Y. Prognostic Value of Coronary Angiography-Derived Fractional Flow Reserve Immediately After Stenting. Front. Cardiovasc. Med. 2022, 21, 834553. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Erriquez, A.; Uretsky, B.F.; Brugaletta, S.; Spitaleri, G.; Cerrato, E.; Quadri, G.; Manfrini, M.; Pompei, G.; Scancarello, D.; Trichilo, M.; et al. Impact of trans-stent gradient on outcome after PCI: Results from a HAWKEYE substudy. Int. J. Cardiovasc. Imaging 2022, 38, 2819–2827. [Google Scholar] [CrossRef] [PubMed]
- Meng, P.N.; Liu, B.; Li, L.B.; Yin, D.L.; Zhang, H.; Pan, D.F.; You, W.; Wu, Z.M.; Wu, X.Q.; Zhao, L.; et al. Cut-off values of lesion and vessel quantitative flow ratio in de novo coronary lesion post-drug-coated balloon therapy predicting vessel restenosis at mid-term follow-up. Chin. Med. J. 2021, 134, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Dai, N.; Zhang, R.; Yuan, S.; Hu, N.; Guan, C.; Zou, T.; Qiao, Z.; He, J.; Duan, S.; Xie, L.; et al. Prognostic Implications of Quantitative Flow Ratio-Derived Physiological 2-Dimensional Residual Disease Patterns After Stenting. JACC Cardiovasc. Interv. 2022, 15, 1624–1634. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Chen, Q.; Zhong, J.; Chen, L.; Chen, L.; Ye, M.; Yan, Y.; Chen, L.; Luo, Y. Impact of diabetes on coronary physiology evaluated by quantitative flow ratio in patients who underwent percutaneous coronary intervention. J. Diabetes Investig. 2022, 12, 1203–1212. [Google Scholar] [CrossRef]
- Zhong, J.; Chen, Q.; Chen, L.; Ye, Z.; Chen, H.; Sun, J.; Hong, J.; Ye, M.; Yan, Y.; Chen, L.; et al. Physiological benefits evaluated by quantitative flow ratio in patients with reduced left ventricular ejection fraction who underwent percutaneous coronary intervention. BMC Cardiovasc. Disord. 2020, 20, 523. [Google Scholar] [CrossRef]
- Zhang, R.; Dou, K.; Guan, C.; Zou, T.; Zhang, M.; Yuan, S.; Qiao, Z.; Xie, L.; Sun, Z.; Song, L.; et al. Outcomes of quantitative flow ratio-based percutaneous coronary intervention in an all-comers study. EuroIntervention 2022, 17, 1240–1251. [Google Scholar] [CrossRef]
- Kirigaya, H.; Okada, K.; Hibi, K.; Maejima, N.; Iwahashi, N.; Matsuzawa, Y.; Minamimoto, Y.; Kosuge, M.; Ebina, T.; Tamura, K.; et al. Post-procedural quantitative flow ratio gradient and target lesion revascularization after drug-coated balloon or plain-old balloon angioplasty. J. Cardiol. 2022, 80, 511–517. [Google Scholar] [CrossRef]
- Griffioen, A.M.; Oord, S.C.H.V.D.; Teerenstra, S.; Damman, P.; Van Royen, N.; Van Geuns, R.J.M. Clinical Relevance of Impaired Physiological Assessment After Percutaneous Coronary Intervention: A Meta-analysis. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100448. [Google Scholar]
- Andersen, B.K.; Ding, D.; Mogensen, L.J.H.; Tu, S.; Holm, N.R.; Westra, J.; Wijns, W. Predictive value of post-percutaneous coronary intervention fractional flow reserve: A systematic review and meta-analysis. Eur. Heart J. Qual. Care Clin. Outcomes 2023, 9, 99–108. [Google Scholar] [CrossRef]
- Hwang, D.; Koo, B.K.; Zhang, J.; Park, J.; Yang, S.; Kim, M.; Yun, J.P.; Lee, J.M.; Nam, C.W.; Shin, E.S.; et al. Prognostic Implications of Fractional Flow Reserve After Coronary Stenting: A Systematic Review and Meta-analysis. JAMA Netw. Open. 2022, 5, e2232842. [Google Scholar] [CrossRef]
- Chung, J.H.; Ann, S.H.; Koo, B.K.; Nam, C.W.; Doh, J.H.; Singh, G.B.; Kim, H.I.; Shin, E.S. Assessment of stent edge dissections by fractional flow reserve. Int. J. Cardiol. 2015, 15, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Nam, C.W.; Yoon, H.J.; Cho, Y.K.; Park, H.S.; Kim, H.; Hur, S.H.; Kim, Y.N.; Chung, I.S.; Koo, B.K.; Tahk, S.J.; et al. Outcomes of percutaneous coronary intervention in intermediate coronary artery disease: Fractional flow reserve-guided versus intravascular ultrasound-guided. JACC Cardiovasc. Interv. 2010, 3, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Kaziród-Wolski, K.; Sielski, J.; Gąsior, M.; Bujak, K.; Hawranek, M.; Pyka, Ł.; Gierlotka, M.; Pawłowski, T.; Siudak, Z. Factors affecting short- and long-term survival of patients with acute coronary syndrome treated invasively using intravascular ultrasound and fractional flow reserve: Analysis of data from the Polish Registry of Acute Coronary Syndromes 2017–2020. Kardiol. Pol. 2023, 81, 265–272. [Google Scholar] [CrossRef]
- Modi, B.N.; Sankaran, S.; Kim, H.J.; Ellis, H.; Rogers, C.; Taylor, C.A.; Rajani, R.; Perera, D. Predicting the Physiological Effect of Revascularization in Serially Diseased Coronary Arteries. Circ. Cardiovasc. Interv. 2019, 12, e007577. [Google Scholar] [CrossRef] [PubMed]
- Kruk, M.; Rudziński, P.N.; Demkow, M.; Kępka, C. Is the Majority Benefitting at the Costs of the Minority Among Patients Undergoing CTA as the First-Line Diagnostic in Highly Suspected Coronary Artery Disease? JACC Cardiovasc. Imaging 2019, 12, 944. [Google Scholar] [CrossRef]
- Tang, C.X.; Qiao, H.Y.; Zhang, X.L.; Di Jiang, M.; Schoepf, U.J.; Rudziński, P.N.; Giovagnoli, D.P.; Lu, M.J.; Li, J.H.; Wang, Y.N.; et al. Functional CAD-RADS using FFRCT on therapeutic management and prognosis in patients with coronary artery disease. Eur. Radiol. 2022, 32, 5210–5221. [Google Scholar] [CrossRef]
- Sonck, J.; Nagumo, S.; Norgaard, B.L.; Otake, H.; Ko, B.; Zhang, J.; Mizukami, T.; Maeng, M.; Andreini, D.; Takahashi, Y.; et al. Clinical Validation of a Virtual Planner for Coronary Interventions Based on Coronary CT Angiography. JACC Cardiovasc. Imaging 2022, 15, 1242–1255. [Google Scholar] [CrossRef]
- Papakonstantinou, P.E.; Apostolou, I.; Papathanasiou, L.; Papagikas, P.; Hamilos, M.; Aggeli, C.; Spanos, A.; Milkas, A. Noninvasive estimation of Fraction Flow Reserve (FFR): The first real-time FFRangio™ application in Greece. Hell. J. Cardiol. 2019, 60, 324–326. [Google Scholar] [CrossRef]
- Luo, Y.; Mao, M.; Xiang, R.; Han, B.; Chang, J.; Zuo, Z.; Wu, F.; Ma, K. Diagnostic performance of computed tomography-based fraction flow reserve in identifying myocardial ischemia caused by coronary artery stenosis: A meta-analysis. Hell. J. Cardiol. 2022, 63, 1–7. [Google Scholar] [CrossRef]
- Nishi, T.; Murai, T.; Ciccarelli, G.; Shah, S.V.; Kobayashi, Y.; Derimay, F.; Waseda, K.; Moonen, A.; Hoshino, M.; Hirohata, A.; et al. Prognostic Value of Coronary Microvascular Function Measured Immediately After Percutaneous Coronary Intervention in Stable Coronary Artery Disease: An International Multicenter Study. Circ. Cardiovasc. Interv. 2019, 12, e007889. [Google Scholar] [CrossRef]
- Geng, Y.; Wu, X.; Liu, H.; Zheng, D.; Xia, L. Index of microcirculatory resistance: State-of-the-art and potential applications in computational simulation of coronary artery disease. J. Zhejiang Univ. B 2022, 23, 123–140. [Google Scholar] [CrossRef] [PubMed]
- De Maria, G.L.; Oxford Acute Myocardial Infarction (OXAMI) Study Investigators; Scarsini, R.; Shanmuganathan, M.; Kotronias, R.A.; Terentes-Printzios, D.; Borlotti, A.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.P.; et al. Angiography-derived index of microcirculatory resistance as a novel, pressure-wire-free tool to assess coronary microcirculation in ST elevation myocardial infarction. Int. J. Cardiovasc. Imaging 2020, 36, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Takahashi, T.; Rios, S.A.; Latib, A.; Lee, J.M.; Fearon, W.F.; Kobayashi, Y. Diagnostic performance and prognostic impact of coronary angiography-based Index of Microcirculatory Resistance assessment: A systematic review and meta-analysis. Catheter. Cardiovasc. Interv. 2022, 99, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Kotronias, R.A.; Terentes-Printzios, D.; Shanmuganathan, M.; Marin, F.; Scarsini, R.; Bradley-Watson, J.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.; Kharbanda, R.K.; et al. Long-Term Clinical Outcomes in Patients With an Acute ST-Segment-Elevation Myocardial Infarction Stratified by Angiography-Derived Index of Microcirculatory Resistance. Front. Cardiovasc. Med. 2021, 8, 717114. [Google Scholar] [CrossRef]
- Sans-Roselló, J.; Fernández-Peregrina, E.; Duran-Cambra, A.; Carreras-Mora, J.; Sionis, A.; Álvarez-García, J.; García-García, H.M. Prognostic Value of Microvascular Resistance at Rest in Patients With Takotsubo Syndrome. JACC Cardiovasc. Imaging 2022, 15, 1784–1795. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author. Year (Ref.) | Sample Size | Mean Age ± SD | FU (Years) | Men (%) | LAD (%) | LCX (%) | RCA (%) | Indication | Method | Cut-Off | Outcomes | Results | Adjusted for | NOS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biscaglia et al., 2019 [24] | 602 | 68 | 1.8 | 443 (74.0) | 356 (48.0) | 184 (24.0) | 211 (28.0) | SIHD NSTE-ACS | QAngio XA 3D (Medis Medical Imaging Systems) | ≤0.89 | VOCE CV death TVMI TVR | Post-PCI QFR was significantly lower in vessels with the vessel-oriented composite endpoint during follow-up compared with those without it. | Diabetes, prior MI and post-PCI diameter stenosis | 9 |
| Kogame et al., 2019 [25] | 440 | 66.6 | 2 | 364 (92.3) | 352 (45.7) | 243 (31.5) | 176 (22.8) | SIHD NSTE-ACS | QAngio XA 3D (Medis Medical Imaging Systems) | <0.91 | VOCE CV death TVMI TVR | The incidence of 2-year VOCE in the vessels with post-PCI QFR <0.91 was significantly higher compared with vessels with post-PCI QFR≥ 0.91. | Creatinine clearance, LAD stenosis and SYNTAX score | 9 |
| Tang et al., 2020 [20] | 186 | 63.1 | 2 | 140 (75.3) | 169 (40.7) | 106 (25.5) | 140 (33.7) | STEMI | QFR system software (AngioPlus, Pulse Medical Imaging Technology) | ≤0.91 | VOCE | The multivariable model demonstrated that low post-PCI QFR was an independent predictor of 2-year VOCE. | Diabetes mellitus, culprit lesion, diffuse disease and peak troponin I during the first hospitalization | 8 |
| Tang et al., 2021 [22] | 177 | 68.6 | 1 | 143 (81.1) | 93 (50.3) | 37 (20.0) | 55 (29.7) | DES-ISR lesions treated with DCB | QFR system software (AngioPlus, Pulse Medical Imaging Technology) | ≤0.94 | VOCE CV death TVMI TVR | Post-procedural QFR ≤ 0.94 was an independent predictor of 1-year VOCE. | Diabetes mellitus and diameter stenosis (post-procedural in stent) | 8 |
| Zhang et al., 2022 [18] | 1805 | 60.9 | 2 | 1268 (70.2) | 1078 (48.4) | 481 (21.6) | 663 (30.0) | SIHD ACS | QFR system software (AngioPlus, Pulse Medical Imaging Technology) | ≤0.92 | VOCE | Post-PCI QFR results ≤0.92 were associated with a higher risk of 2-year VOCE. | No adjustment | 9 |
| Dai et al., 2022 [19] | 1395 | 61.3 | 2 | 960 (68.8) | 857 (50.9) | 369 (21.9) | 459 (27.2) | SIHD ACS | QAngio XA 3D (Medis Medical Imaging Systems, Leiden, The Netherlands) | <0.89 | VOCE | Vessels with low post- PCI QFR demonstrated higher vessel- oriented composite outcome risk after stent implantation. | No adjustment | 8 |
| You et al., 2022 [17] | 224 | 71.1 | 3 | 152 (67.9) | 177 (79.0) | 35 (15.6) | 12 (5.4) | SIHD ACS | QFR system software (AngioPlus, Pulse Medical Imaging Technology) | ≤0.94 | TLF | Post-PCI QFR results ≤0.94 was not a predictor of TLF. | No adjustment | 7 |
| Liu et al., 2021 [16] | 169 | 62.5 | 1 | 128 (75.5) | 81 (47.9) | 25 (14.8) | 63 (37.3) | SIHD NSTE-ACS DES-ISR lesions treated with DCB | QAngio XA 7.3 (Medis Medical Imaging) | ≤0.89 | VOCE | Post-procedural µQFR ≤ 0.89 was associated with a 6-fold higher risk of VOCE than lesions with µQFR > 0.89. | Diabetes mellitus Difference of DCB diameter and RVD (per 0.10-mm increase) | 8 |
| Erbay et al., 2021 [23] | 792 | 68 | 2 | 548 (62.9) | 691 (34.2) | 650 (32.1) | 682 (33.7) | ACS | QAngio XA/3D (Medis) | ≤0.89 | MACE | Independent predictor of major adverse cardiovascular events after ACS. | Age, sex, medical history, type of ACS and, LVEF | 9 |
| Cai et al., 2021 [21] | 208 | 63.3 | 0.75 | 163 (78.4) | 98 (47.1) | 32 (15.4) | 74 (35.6) | SIHD DES-ISR lesions treated with DCB | QAngio XA/3D (Medis) | ≤0.9 | ISR | Independently associated with recurrent restenosis after DCB angioplasty. | Vessel caliber, lesion length and diameter stenosis at baseline | 7 |
| Neleman et al., 2022 [27] | 748 | 65 | 5 | 526 (70.3) | 356 (42.8) | NR | NR | SIHD ACS | CAAS Workstation 8.2 (Pie Medical Imaging) | ≤0.93 | TVF | Lower post-PCI vFFR values are associated with significantly increased risks of TVF and TVR at 5-year follow-up. | No adjustment | 7 |
| Suzuki et al., 2019 [26] | 45 | 68.9 | 1.5–2.5 | 41 (91) | NR | NR | NR | PCI DES | QAngio XA/3D (Medis) | ≤0.82 | TVR | Vessel QFR was significantly lower in TVR group. | No adjustment | 5 |
| Zhou et al., 2022 [28] | 136 | 59 | 0.75 | 91 (66.9) | 90 (56.6) | 33 (20.8) | 36 (22.6) | PCI DES | FLASH ANGIO (Rainmed) | <0.90 | TVF | Lower post-PCI caFFR was associated with a higher rate of 9-month TVF. | Age, gender and diabetes mellitus | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terentes-Printzios, D.; Gkini, K.-P.; Oikonomou, D.; Gardikioti, V.; Aznaouridis, K.; Dima, I.; Tsioufis, K.; Vlachopoulos, C. Prognostic Value of Post-PCI Angiography-Derived Fractional Flow Reserve: A Systematic Review and Meta-Analysis of Cohort Studies. J. Pers. Med. 2023, 13, 1251. https://doi.org/10.3390/jpm13081251
Terentes-Printzios D, Gkini K-P, Oikonomou D, Gardikioti V, Aznaouridis K, Dima I, Tsioufis K, Vlachopoulos C. Prognostic Value of Post-PCI Angiography-Derived Fractional Flow Reserve: A Systematic Review and Meta-Analysis of Cohort Studies. Journal of Personalized Medicine. 2023; 13(8):1251. https://doi.org/10.3390/jpm13081251
Chicago/Turabian StyleTerentes-Printzios, Dimitrios, Konstantia-Paraskevi Gkini, Dimitrios Oikonomou, Vasiliki Gardikioti, Konstantinos Aznaouridis, Ioanna Dima, Konstantinos Tsioufis, and Charalambos Vlachopoulos. 2023. "Prognostic Value of Post-PCI Angiography-Derived Fractional Flow Reserve: A Systematic Review and Meta-Analysis of Cohort Studies" Journal of Personalized Medicine 13, no. 8: 1251. https://doi.org/10.3390/jpm13081251
APA StyleTerentes-Printzios, D., Gkini, K.-P., Oikonomou, D., Gardikioti, V., Aznaouridis, K., Dima, I., Tsioufis, K., & Vlachopoulos, C. (2023). Prognostic Value of Post-PCI Angiography-Derived Fractional Flow Reserve: A Systematic Review and Meta-Analysis of Cohort Studies. Journal of Personalized Medicine, 13(8), 1251. https://doi.org/10.3390/jpm13081251