
Is Psychological Distress Associated with Self-Perceived Health, Perceived Social Support and Physical Activity Level in Spanish Adults with Diabetes?

 , ,
, ,  , ,
, ,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Data Sources and Ethical Concerns
2.2. Participants
2.3. Procedures
- Successful Coping: derived from the total of the items Q.47.1, Q.47.3, Q.47.4, Q47.7, Q47.8 and Q.47.12, with punctuation ranging from 0 to 18, where 0 is the best and 18 is the worst coping level, and has an external validity of 0.82 with a p-value of 0.001.
- Self-esteem: derived from the sum of the items Q.47.6, Q.47.9, Q.47.10 and Q.47.11, ranging from 0 to 12, where 0 is the best and 12 is the worst, and has an external validity of 0.70 with a p-value of 0.001.
- Stress: derived from the sum of the items Q.47.2, Q.47.5 and Q.47.9; ranging from 0 to 9, where 0 is the best and 9 is the worst, and has an external validity of 0.75, with a p-value of 0.001.
2.4. Statistical Analysis
3. Results
- R2 = 17.8%, positively explained by mental health (constant: β = 21.22, t = 19.30, p < 0.001; PSS: β = −0.204, t = −10.35, p < 0.001; PAL: β = −1.38, t = −6.33, p < 0.001; sex: β = 1.82, t = 5.54, p < 0.001)
- R2 = 15.5%, positively explained by successful coping (constant: β = 10.24, t = 23.93, p < 0.001; PSS: β = −0.075, t = −9.73, p < 0.001; PAL: β = −0.472, t = −5.57, p < 0.001; sex: β = 0.61, t = 4.81, p < 0.001)
- R2 = 14.7%, positively explained by self-esteem (constant: β = 7.23, t = 13.51, p < 0.001; PSS: β = −0.647, t = −9.25, p < 0.001; PAL: β = −0.647, t = −6.11, p < 0.001; sex: β = 0.679, t = 4.25, p < 0.001)
- R2 = 13.0%, positively explained by stress (constant: β = 5.86, t = 13.12, p < 0.001; PSS: β = −0.068, t = −8.48, p < 0.001; PAL: β = −0.408, t = −4.62, p < 0.001; sex: β = 0.751, t = 5.63, p < 0.001)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aldossari, K.K.; Shubair, M.M.; Al-Ghamdi, S.H.; Alduraywish, A.A.; Almeshari, A.A.; Alrasheed, A.A.; Aldahash, R.; Angawi, K.; Gaissi, A.; Alhumud, H.A.; et al. Psychological Wellbeing of Diabetic Individuals, Prediabetics, and Non-Diabetics: A Population-Based Study in Saudi Arabia. Front. Psychol. 2022, 13, 863861. [Google Scholar] [CrossRef] [PubMed]
- Quiroz-Mora, C.; Serrato-Ramírez, D.M.; Bergonzoli-Peláez, G. Factores Asociados Con La Adherencia a La Actividad Física En El Tiempo Libre. Educ. Física Deporte 2014, 33, 129–151. [Google Scholar] [CrossRef]
- IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019; ISBN 9782930229874.
- Trikkalinou, A.; Papazafiropoulou, A.K.; Melidonis, A. Type 2 Diabetes and Quality of Life. World J. Diabetes 2017, 8, 120–171. [Google Scholar] [CrossRef]
- Grigsby, A.B.; Anderson, R.J.; Freedland, K.E.; Clouse, R.E.; Lustman, P.J. Prevalence of Anxiety in Adults with Diabetes a Systematic Review. J. Psychosom. Res. 2002, 53, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Kruse, J.; Schmitz, N.; Thefeld, W. On the Association between Diabetes and Mental Disorders in a Community Sample: Results From the German National Health Interview and Examination Survey. Diabetes Care 2003, 26, 1841–1846. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.M.; Corcoran, P.; Perry, I.J. Anxiety and Depression Symptoms in Patients with Diabetes: Original Article: Psychology. Diabet. Med. 2009, 26, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Fisher, L.; Skaff, M.M.; Mullan, J.T.; Arean, P.; Mohr, D.; Masharani, U.; Glasgow, R.; Laurencin, G. Clinical Depression Versus Distress Among Patients with Type 2 Diabetes: Not Just a Question of Semantics. Diabetes Care 2007, 30, 542–548. [Google Scholar] [CrossRef]
- Das-Munshi, J.; Stewart, R.; Ismail, K.; Bebbington, P.E.; Jenkins, R.; Prince, M.J. Diabetes, Common Mental Disorders, and Disability: Findings From the UK National Psychiatric Morbidity Survey. Psychosom. Med. 2007, 69, 543–550. [Google Scholar] [CrossRef]
- Anderson, R.J. Anxiety and Poor Glycemic Control: A Meta-Analytic Review of the Literature. Int. J. Psychiatry Med. 2002, 32, 235–247. [Google Scholar] [CrossRef]
- Egede, L.E.; Ellis, C.; Grubaugh, A.L. The Effect of Depression on Self-Care Behaviors and Quality of Care in a National Sample of Adults with Diabetes. Gen. Hosp. Psychiatry 2009, 31, 422–427. [Google Scholar] [CrossRef]
- Egede, L.; Zheng, D.; Simpson, K. Comorbid Depression Is Associated With Increased Health Care Use And. Diabetes Care 2002, 25, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J.N.; Carcelen, C.M.G.; Felipe, G.; Sanchez, L. Barriers to Physical Activity in People with Diabetes Residing in Spain. Atena J. Public Health 2020, 2, 3. [Google Scholar]
- Gómez-García, A.R.; Portalanza-Chavarría, C.A.; Arias-Ulloa, C.A.; Espinoza-Samaniego, C.E. Salaried Workers’ Self-Perceived Health and Psychosocial Risk in Guayaquil, Ecuador. Int. J. Environ. Res. Public Health 2020, 17, 9099. [Google Scholar] [CrossRef] [PubMed]
- Au, N.; Johnston, D.W. Self-Assessed Health: What Does It Mean and What Does It Hide? Soc. Sci. Med. 2014, 121, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Romero, D.; Urbina, A.; Cristancho-Montenegro, A.; Rombaldi, A. Impact of Smoking and Physical Inactivity on Self-Rated Health in Women in Colombia. Prev. Med. Rep. 2019, 16, 100976. [Google Scholar] [CrossRef]
- Almagiá, E.B. Apoyo Social, Estrés y Salud. Psicol. Salud 2004, 14, 237–243. [Google Scholar]
- Newsom, J.T.; Schulz, R. Social Support as a Mediator in the Relation between Functional Status and Quality of Life in Older Adults. Psychol. Aging 1996, 11, 34–44. [Google Scholar] [CrossRef]
- Young, C.F.; Shubrook, J.H.; Valencerina, E.; Wong, S.; Lo, S.N.H.; Dugan, J.A. Associations between Social Support and Diabetes-Related Distress in People with Type 2 Diabetes Mellitus. J. Am. Osteopath. Assoc. 2020, 120, 721–731. [Google Scholar] [CrossRef]
- Morres, I.D.; Touloudi, E.; Hatzigeorgiadis, A.; Jamurtas, A.Z.; Androutsos, O.; Theodorakis, Y. Daily Life Physical Activity, Quality of Life and Symptoms of Depression and Anxiety in Adult Patients with Type 2 Diabetes: A Preliminary Study. Psychology 2021, 12, 1277–1286. [Google Scholar] [CrossRef]
- Semenkovich, K.; Brown, M.E.; Svrakic, D.M.; Lustman, P.J. Depression in Type 2 Diabetes Mellitus: Prevalence, Impact, and Treatment. Drugs 2015, 75, 577–587. [Google Scholar] [CrossRef]
- Kuru, T.; Acar, G.; Elcin, E.; Özgül, B.; Demirbuken, I.; Alkaç, Ç. Association Between the Physical Activity Level and the Quality of LLfe of Patients with Type 2 Diabetes Mellitus. J. Phys. Ther. Sci. 2016, 28, 142–147. [Google Scholar] [CrossRef]
- Velasco, N. Terapia Insulínica y Ejercicio En Diabetes Tipo I. ARS MEDICA Rev. Cienc. Méd. 2017, 21, 29–31. [Google Scholar] [CrossRef]
- Barreira, E.; Novo, A.; Vaz, J.A.; Pereira, A.M.G. Dietary Program and Physical Activity Impact on Biochemical Markers in Patients with Type 2 Diabetes: A Systematic Review. Aten. Primaria 2018, 50, 590–610. [Google Scholar] [CrossRef] [PubMed]
- Batt, M.E.; Tanji, J.; Börjesson, M. Exercise at 65 and Beyond. Sports Med. 2013, 43, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Visvanathan, R.; Chapman, I. Preventing Sarcopaenia in Older People. Maturitas 2010, 66, 383–388. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Consumo y Bienestar Social; Gobierno de España. Encuesta Nacional de Salud 2017 ENSE 2017 Metodología; Ministerio de Sanidad, Consumo y Bienestar Social; Gobierno de España: Madrid, Spain, 2017. [Google Scholar]
- Ministerio de Salud Pública y Asistencia Social; Instituto Nacional de Estadística; Secretaría de Planificación y Programación de la Presidencia. Segeplán Encuesta Nacional de Salud; Ministerio de Salud Pública y Asistencia Social; Instituto Nacional de Estadística; Secretaría de Planificación y Programación de la Presidencia: Madrid, Spain, 2017; p. 748. [Google Scholar]
- Goldberg, P. The User’s Guide to the General Health Questionnaire; NFER-NELSON: Fontainebleau, France, 1988. [Google Scholar]
- Rocha, K.B.; Pérez, K.; Rodríguez-Sanz, M.; Borrell, C.; Obiols, J.E. Propiedades Psicométricas y Valores Normativos Del General Health Questionnaire (GHQ-12) En Población General Española TT—Psychometric Properties and Normative Values of General Health Questionnaire (GHQ-12) in Spanish Population. Int. J. Clin. Health Psychol. 2011, 11, 125–139. [Google Scholar]
- del Pilar Sánchez-López, M.; Dresch, V. The 12-Item General Health Questionnaire (GHQ-12): Reliability, External Validity and Factor Structure in the Spanish Population. Psicothema 2008, 20, 839–843. [Google Scholar]
- Muñoz-Bermejo, L.; Adsuar, J.C.; Postigo-Mota, S.; Casado-Verdejo, I.; de Melo-Tavares, C.M.; Garcia-Gordillo, M.Á.; Pérez-Gómez, J.; Carlos-Vivas, J. Relationship of Perceived Social Support with Mental Health in Older Caregivers. Int. J. Environ. Res. Public Health 2020, 17, 3886. [Google Scholar] [CrossRef]
- Broadhead, W.E.; Gehlbach, S.H.; De Gruy, F.V.; Kaplan, B.H. The Duke-UNC Functional Social Support Questionnaire: Measurement of Social Support in Family Medicine Patients. Med. Care 1988, 26, 709–723. [Google Scholar] [CrossRef]
- Saameño, J.B.B.; Sánchez, A.D.; Castillo, J.L.D.L.; Claret, P.L. Validity and Reliability of the Duke-UNC-11 Questionnaire of Functional Social Support. Aten. Primaria 1996, 18, 153–156. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Nes, B.M.; Janszky, I.; Vatten, L.J.; Nilsen, T.I.L.; Aspenes, S.T.; Wisløff, U. Estimating VO2 Peak from a Nonexercise Prediction Model: The HUNT Study, Norway. Med. Sci. Sports Exerc. 2011, 43, 2024–2031. [Google Scholar] [CrossRef] [PubMed]
- Denche-Zamorano, Á.; Franco-García, J.M.; Carlos-Vivas, J.; Mendoza-Muñoz, M.; Pereira-Payo, D.; Pastor-Cisneros, R.; Merellano-Navarro, E.; Adsuar, J.C. Increased Risks of Mental Disorders: Youth with Inactive Physical Activity. Healthcare 2022, 10, 237. [Google Scholar] [CrossRef] [PubMed]
- Denche-Zamorano, Á.; Pastor-Cisneros, R.; Carlos-Vivas, J.; Manuel, J.; Pereira-payo, D.; Barrios-fernandez, S.; Rojo-ramos, J.; Mendoza-muñoz, M. Associations between Psychological Distress, Perceived Social Support and Physical Activity Level in Spanish Adults with Depression. Healthcare 2022, 10, 1620. [Google Scholar] [CrossRef] [PubMed]
- Mondragón, M.A. Uso de La Correlación de Spearman En Un Estudio de Intervención En Fisioterapia. Mov. Científ. 2014, 8, 98–104. [Google Scholar] [CrossRef]
- Reig-Ferrer, A.; Cabrero-García, J.; Lizán Tudela, L. Assessment of Functional Capacity, Psychological Well-Being and Mental Health in Primary Care. Aten. Primaria 2009, 41, 515–519. [Google Scholar] [CrossRef]
- Denche-Zamorano, Á.; Mendoza-Muñoz, M.; Carlos-Vivas, J.; Muñoz-Bermejo, L.; Rojo-Ramos, J.; Pastor-Cisneros, R.; Giakoni-Ramírez, F.; Godoy-Cumillaf, A.; Barrios-Fernandez, S. A Cross-Sectional Study on Self-Perceived Health and Physical Activity Level in the Spanish Population. Int. J. Environ. Res. Public Health 2022, 19, 5656. [Google Scholar] [CrossRef]
- Manzaneda, A.; Lazo, M.; Malaga, G. Actividad Física en Pcientes Ambulatorios Con Diabetes Mellitus 2 de un Hospital Nacional del Perú. Med. Exp. Salud Publica 2015, 32, 311–315. [Google Scholar] [CrossRef]
- Thomas, N.; Alder, E.; Leese, G.P. Barriers to Physical Activity in Patients with Diabetes. Postgrad. Med. J. 2004, 80, 287–291. [Google Scholar] [CrossRef]
- Rubio, R.; Varela, M. Barreras Percibidas En Jóvenes Universitarios Para Realizar Actividad Física. Rev. Cuba. Salud Pública 2016, 42, 61–69. [Google Scholar]
- Esteban y Peña, M.M.; Hernandez Barrera, V.; Fernández Cordero, X.; Gil de Miguel, A.; Rodríguez Pérez, M.; Lopez-de Andres, A.; Jiménez-García, R. Self-Perception of Health Status, Mental Health and Quality of Life Among Adults with Diabetes Residing in a Metropolitan Area. Diabetes Metab. 2010, 36, 305–311. [Google Scholar] [CrossRef]
- Jimenez-Garcia, R.; Martinez Huedo, M.A.; Hernandez-Barrera, V.; De Andres, A.L.; Martinez, D.; Jimenez-Trujillo, I.; Carrasco-Garrido, P. Psychological Distress and Mental Disorders among Spanish Diabetic Adults: A Case-Control Study. Prim. Care Diabetes 2012, 6, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Garcia, R.; Jiménez-Trujillo, I.; Hernandez-Barrera, V.; Carrasco-Garrido, P.; Lopez, A.; Angel, G. Ten-Year Trends in Self-Rated Health Among Spanish Adults with Diabetes, 1993–2003. Diabetes Care 2008, 31, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Lazo, C.; Durán-Agüero, S. Efecto Del Diagnóstico de La Diabetes Mellitus y Su Complicación Con Los Trastornos de La Conducta Alimentaria. Rev. Chil. Nutr. 2019, 46, 352–360. [Google Scholar] [CrossRef]
- Gazmararian, J.A.; Ziemer, D.C.; Barnes, C. Perception of Barriers to Self-Care Management among Diabetic Patients. Diabetes Educ. 2009, 35, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Brazeau, A.S.; Rabasa-Lhoret, R.; Strychar, I.; Mircescu, H. Barriers to Physical Activity among Patients with Type 1 Diabetes. Diabetes Care 2008, 31, 2108–2109. [Google Scholar] [CrossRef]
- González, N.F.; Rivas, A.D. Actividad Física y Ejercicio En La Mujer. Rev. Colomb. Cardiol. 2018, 25, 125–131. [Google Scholar] [CrossRef]
- Albert, P.R. Why Is Depression More Prevalent in Women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef]
- Hulin, B.T.; Gabbett, T.J.; Lawson, D.W.; Caputi, P.; Sampson, J.A. The Acute: Chronic Workload Ratio Predicts Injury: High Chronic Workload May Decrease Injury Risk in Elite Rugby League Players. Br. J. Sports Med. 2016, 50, 231–236. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total n = 1006 | Men n = 572 | Women n = 434 | p/p * |
|---|---|---|---|---|
| Age (Years) | p | |||
| Median (IQR) | 61 (12) | 61 (10) | 61 (13) | 0.323 |
| Mean (SD) | 58.4 (9.2) | 58.8 (8.5) | 57.9 (10.0) | |
| PAI | p | |||
| Median (IQR) | 0 (0) | 0 (0) | 0 (0) | 0.014 |
| Mean (SD) | 5.9 (13.2) | 6.8 (14.1) | 4.7 (11.7) | |
| Mental Health | p | |||
| Median (IQR) | 11 (6) | 10 (5) | 11 (7) | <0.001 |
| Mean (SD) | 11.4 (5.5) | 10.7 (5.0) | 12.4 (6.0) | |
| Successful Coping | p | |||
| Median (IQR) | 6 (1) | 6 (0) | 6 (1) | <0.001 |
| Mean (SD) | 6.7 (2.2) | 6.4 (1.9) | 7.0 (2.4) | |
| Self-Esteem | p | |||
| Median (IQR) | 2 (4) | 2 (4) | 3 (4) | <0.001 |
| Mean (SD) | 2.7 (2.6) | 2.4 (2.5) | 3.1 (2.8) | |
| Stress | p | |||
| Median (IQR) | 3 (3) | 3 (3) | 3 (3) | <0.001 |
| Mean (SD) | 2.9 (2.2) | 2.6 (2.0) | 3.3 (2.3) | |
| Perceived Social Support | Total n = 946 | Men n = 531 | Women n = 415 | p |
| Median (IQR) | 50 (9) | 48 (10) | 49 (12) | 0.918 |
| Mean (SD) | 47.6 (7.4) | 46.7 (8.2) | 46.7 (8.3) | |
| Self-Perceived Health | Total n = 1006 | Men n = 572 | Women n = 434 | p * |
| Negative n (%) | 576 (57.3) | 297 (51.9) | 279 (64.3) * | <0.001 |
| Positive n (%) | 430 (42.7) | 275 (48.1) | 155 (35.7) * | |
| PAL | ||||
| Inactives n (%) | 199 (19.8%) | 111 (19.4%) | 88 (20.3%) | 0.098 |
| Walkers n (%) | 589 (58.5%) | 322 (54.7%) | 267 (61.5%) | |
| Actives n (%) | 169 (16.8%) | 105 (18.4%) | 64 (14.7%) | |
| Very actives n (%) | 49 (4.9%) | 34 (5.9%) | 15 (3.5%) |
| Physical Activity Levels | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Inactive | Walkers | Active | Very Active | ||||||||
| Self-Perceived Health | n (%) | n (%) | n (%) | n (%) | X2 | df | p | CC | ||||
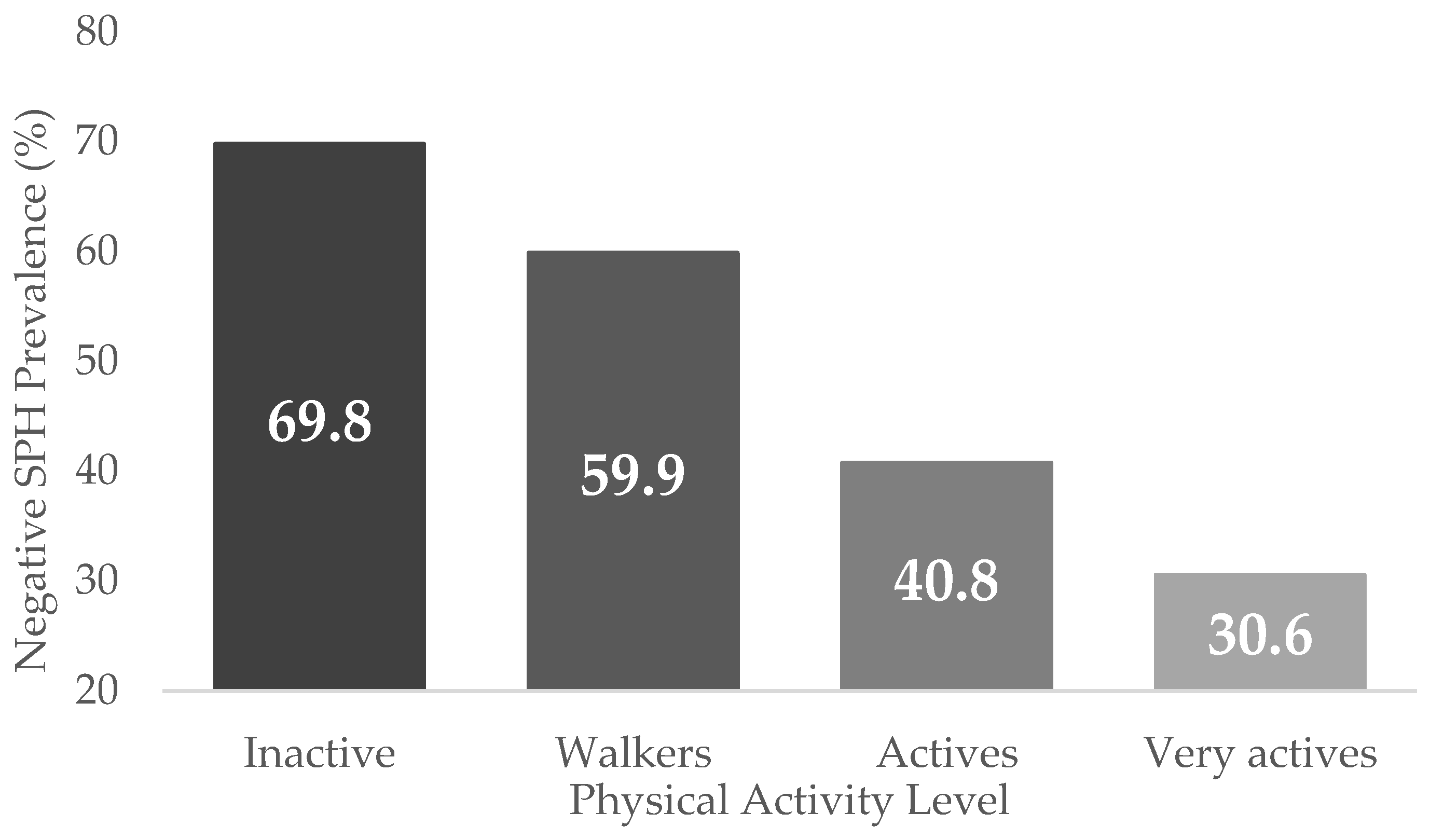
| Negative | 139 a | (69.8) | 353 a | (59.9) | 69 b | (40.8) | 15 b | (30.6) | 47.5 | 3 | <0.001 | 0.212 |
| Positive | 60 a | (30.2) | 236 a | (40.1) | 100 b | (59.2) | 34 b | (59.2) | ||||
| Variables | Total n = 1006 | Men n = 572 | Women n = 434 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mental Health | |||||||||
| PAL | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | |
| Inactives | 13.6 (6.7) | 12 (7) | <0.001 | 12.9 (6.8) | 12 (8) | <0.001 | 14.5 (6.5) | 12 (8) | p < 0.001 |
| Walkers | 11.4 (5.3) | 11 (6) | 10.4 (4.3) | 10 (5) | 12.6 (6.1) | 11 (7) | |||
| Actives | 10.0 (4.1) | 9 (5) | 9.9 (4.1) | 9 (5) | 10.2 (4.0) | 10 (5) | |||
| Very actives | 8.8 (4.1) | 7 (5) | 9.2 (4.4) | 7 (6) | 7.8 (3.2) | 6 (5) | |||
| Successful Coping | |||||||||
| PAL | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | |
| Inactives | 7.5 (2.8) | 7 (4) | <0.001 | 7.3 (2.7) | 6 (1) | <0.001 | 7.8 (2.8) | 6 (4) | p < 0.001 |
| Walkers | 6.7 (3.9) | 6 (1) | 6.3 (2.4) | 6 (0) | 7.1 (2.3) | 6 (1) | |||
| Actives | 6.1 (1.5) | 6 (0) | 6.1 (1.5) | 6 (0) | 6.1 (1.5) | 6 (1) | |||
| Very actives | 5.9 (1.3) | 6 (0) | 6.1 (1.2) | 6 (0) | 5.5 (1.5) | 6 (0) | |||
| Self-Esteem | |||||||||
| PAL | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | |
| Inactives | 3.7 (3.0) | 4 (4) | <0.001 | 3.5 (3.1) | 4 (4) | <0.001 | 3.9 (2.8) | 4 (3) | p < 0.001 |
| Walkers | 2.7 (2.5) | 2 (4) | 2.3 (2.1) | 2 (4) | 3.1 (2.8) | 3 (4) | |||
| Actives | 2.0 (2.3) | 1 (4) | 2.0 (2.3) | 1 (4) | 2.2 (2.4) | 2 (4) | |||
| Very actives | 1.6 (2.2) | 1 (3) | 1.7 (2.4) | 1 (3) | 1.1 (1.7) | 0 (2) | |||
| Stress | |||||||||
| PAL | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | p | m (sd) | mdn (IQR) | |
| Inactives | 3.5 (2.3) | 3 (3) | <0.001 | 3.1 (2.4) | 3 (4) | 0.028 | 3.9 (2.2) | 3 (2) | p < 0.001 |
| Walkers | 2.9 (2.2) | 3 (3) | 2.5 (1.9) | 3 (2) | 3.3 (2.2) | 3 (3) | |||
| Actives | 2.5 (1.8) | 3 (3) | 2.5 (1.8) | 2 (2) | 2.7 (1.8) | 3 (3) | |||
| Very actives | 1.9 (2.0) | 1 (3) | 2.0 (2.1) | 2 (3) | 1.5 (1.9) | 1 (3) | |||
| Target Variable | Rho | p |
|---|---|---|
| Mental Health | −0.220 | <0.001 |
| Successful Coping | −0.193 | <0.001 |
| Self-esteem | −0.215 | <0.001 |
| Stress | −0.160 | <0.001 |
| 1. Have you been able to concentrate well on what you were doing? | −0.125 | <0.001 |
| 2. Have your worries caused you to lose sleep? | −0.104 | 0.001 |
| 3. Did you feel that you were playing a useful role in life? | −0.191 | <0.001 |
| 4. Did you feel able to make decisions? | −0.137 | <0.001 |
| 5. Have you felt constantly overwhelmed and under stress? | −0.150 | <0.001 |
| 6. Have you had the feeling that you cannot overcome your difficulties? | −0.220 | <0.001 |
| 7. Have you been able to enjoy your normal daily activities? | −0.203 | <0.001 |
| 8. Have you been able to cope adequately with your problems? | −0.162 | <0.001 |
| 9. Have you felt unhappy or depressed? | −0.162 | <0.001 |
| 10. Have you lost confidence in yourself? | −0.160 | <0.001 |
| 11. Have you thought of yourself as a worthless person? | −0.180 | <0.001 |
| 12. Do you feel reasonably happy considering all the circumstances? | −0.176 | <0.001 |
| Target Variable | Correlations | p |
|---|---|---|
| Mental Health | −0.234 | <0.001 |
| Successful Coping | −0.189 | <0.001 |
| Self-esteem | −0.230 | <0.001 |
| Stress | −0.189 | <0.001 |
| 1. Have you been able to concentrate well on what you were doing? | −0.189 | <0.001 |
| 2. Have your worries caused you to lose sleep? | −0.179 | <0.001 |
| 3. Did you feel that you were playing a useful role in life? | −0.151 | <0.001 |
| 4. Did you feel able to make decisions? | −0.164 | <0.001 |
| 5. Have you felt constantly overwhelmed and under stress? | −0.193 | <0.001 |
| 6. Have you had the feeling that you cannot overcome your difficulties? | −0.192 | <0.001 |
| 7. Have you been able to enjoy your normal daily activities? | −0.188 | <0.001 |
| 8. Have you been able to cope adequately with your problems? | −0.204 | <0.001 |
| 9. Have you felt unhappy or depressed? | −0.228 | <0.001 |
| 10. Have you lost confidence in yourself? | −0.204 | <0.001 |
| 11. Have you thought of yourself as a worthless person? | −0.150 | <0.001 |
| 12. Do you feel reasonably happy considering all the circumstances? | −0.193 | <0.001 |
| B | SE | Wald | df | Sig | Exp(B) | 95% CI for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Inactive | 29.898 | 3 | 0.000 | |||||
| Walker | −0.320 | 0.191 | 2.793 | 1 | 0.095 | 0.726 | 0.499 | 1.057 |
| Active | −1.021 | 0.235 | 18.921 | 1 | 0.000 | 0.360 * | 0.228 | 0.571 |
| Very active | −1.411 | 0.370 | 14.569 | 1 | 0.000 | 0.244 * | 0.118 | 0.503 |
| Sex (male) | −0.552 | 0.143 | 14.980 | 1 | 0.000 | 0.576 * | 0.435 | 0.762 |
| PSS | −0.026 | 0.009 | 8.521 | 1 | 0.004 | 0.975 * | 0.958 | 0.992 |
| IMC | 0.049 | 0.014 | 11.977 | 1 | 0.001 | 1.050 * | 1.021 | 1.079 |
| Age | 0.021 | 0.008 | 7.733 | 1 | 0.005 | 1.022 * | 1.006 | 1.037 |
| Constant | −0.398 | 0.736 | 0.292 | 1 | 0.589 | 0.672 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denche-Zamorano, A.; Pisà-Canyelles, J.; Barrios-Fernandez, S.; Pastor-Cisneros, R.; Adsuar, J.C.; Garcia-Gordillo, M.A.; Pereira-Payo, D.; Mendoza-Muñoz, M. Is Psychological Distress Associated with Self-Perceived Health, Perceived Social Support and Physical Activity Level in Spanish Adults with Diabetes? J. Pers. Med. 2023, 13, 739. https://doi.org/10.3390/jpm13050739
Denche-Zamorano A, Pisà-Canyelles J, Barrios-Fernandez S, Pastor-Cisneros R, Adsuar JC, Garcia-Gordillo MA, Pereira-Payo D, Mendoza-Muñoz M. Is Psychological Distress Associated with Self-Perceived Health, Perceived Social Support and Physical Activity Level in Spanish Adults with Diabetes? Journal of Personalized Medicine. 2023; 13(5):739. https://doi.org/10.3390/jpm13050739
Chicago/Turabian StyleDenche-Zamorano, Angel, Jofre Pisà-Canyelles, Sabina Barrios-Fernandez, Raquel Pastor-Cisneros, José C. Adsuar, Miguel Angel Garcia-Gordillo, Damián Pereira-Payo, and María Mendoza-Muñoz. 2023. "Is Psychological Distress Associated with Self-Perceived Health, Perceived Social Support and Physical Activity Level in Spanish Adults with Diabetes?" Journal of Personalized Medicine 13, no. 5: 739. https://doi.org/10.3390/jpm13050739
APA StyleDenche-Zamorano, A., Pisà-Canyelles, J., Barrios-Fernandez, S., Pastor-Cisneros, R., Adsuar, J. C., Garcia-Gordillo, M. A., Pereira-Payo, D., & Mendoza-Muñoz, M. (2023). Is Psychological Distress Associated with Self-Perceived Health, Perceived Social Support and Physical Activity Level in Spanish Adults with Diabetes? Journal of Personalized Medicine, 13(5), 739. https://doi.org/10.3390/jpm13050739