

The Correlation between Metformin Use and Incident Dementia in Patients with New-Onset Diabetes Mellitus: A Population-Based Study

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
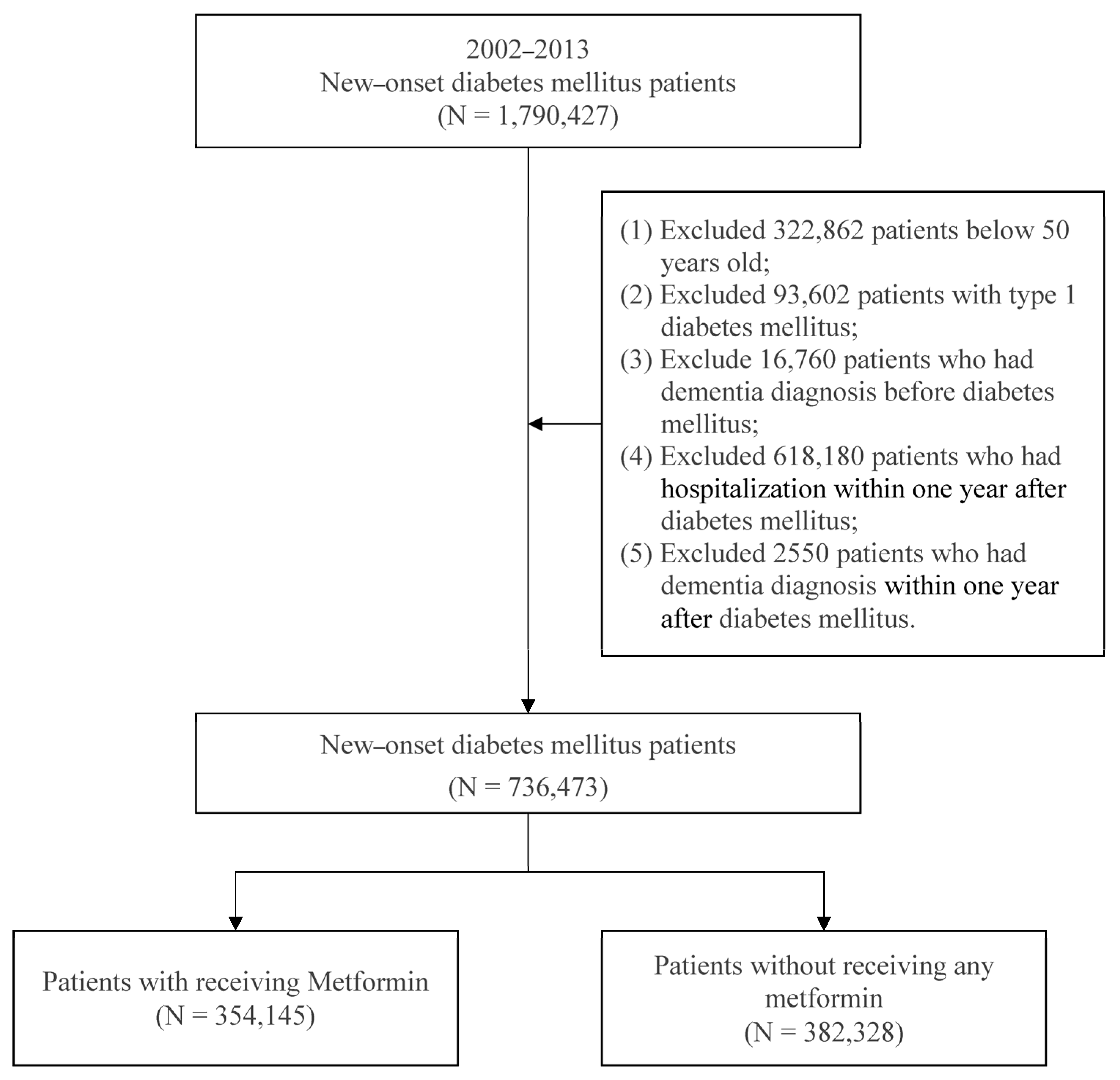
2.2. Study Subjects
2.3. Study Design
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Incident Dementia among New-Onset Patients with DM Who Used Metformin
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erkkinen, M.G.; Kim, M.O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect Biol. 2018, 10, a033118. [Google Scholar] [CrossRef] [PubMed]
- Perl, D.P. Neuropathology of Alzheimer’s disease. Mt. Sinai. J. Med. 2010, 77, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Bomfim, T.R.; Forny-Germano, L.; Sathler, L.B.; Brito-Moreira, J.; Houzel, J.C.; Decker, H.; Silverman, M.A.; Kazi, H.; Melo, H.M.; McClean, P.L.; et al. An anti-diabetes agent protects the mouse brain from defective insulin signaling caused by Alzheimer’s disease-associated Abeta oligomers. J. Clin. Investig. 2012, 122, 1339–1353. [Google Scholar] [CrossRef]
- Hiltunen, M.; Khandelwal, V.K.; Yaluri, N.; Tiilikainen, T.; Tusa, M.; Koivisto, H.; Krzisch, M.; Vepsalainen, S.; Makinen, P.; Kemppainen, S.; et al. Contribution of genetic and dietary insulin resistance to Alzheimer phenotype in APP/PS1 transgenic mice. J. Cell Mol. Med. 2012, 16, 1206–1222. [Google Scholar] [CrossRef] [PubMed]
- Talbot, K.; Wang, H.Y.; Kazi, H.; Han, L.Y.; Bakshi, K.P.; Stucky, A.; Fuino, R.L.; Kawaguchi, K.R.; Samoyedny, A.J.; Wilson, R.S.; et al. Demonstrated brain insulin resistance in Alzheimer’s disease patients is associated with IGF-1 resistance, IRS-1 dysregulation, and cognitive decline. J. Clin. Investig. 2012, 122, 1316–1338. [Google Scholar] [CrossRef]
- Ferreira, L.S.S.; Fernandes, C.S.; Vieira, M.N.N.; De Felice, F.G. Insulin Resistance in Alzheimer’s Disease. Front. Neurosci. 2018, 12, 830. [Google Scholar] [CrossRef]
- Li, X.; Song, D.; Leng, S.X. Link between type 2 diabetes and Alzheimer’s disease: From epidemiology to mechanism and treatment. Clin. Interv. Aging 2015, 10, 549–560. [Google Scholar] [CrossRef]
- Shi, Q.; Liu, S.; Fonseca, V.A.; Thethi, T.K.; Shi, L. Effect of metformin on neurodegenerative disease among elderly adult US veterans with type 2 diabetes mellitus. BMJ Open 2019, 9, e024954. [Google Scholar] [CrossRef]
- Soukas, A.A.; Hao, H.; Wu, L. Metformin as Anti-Aging Therapy: Is It for Everyone? Trends Endocrinol. Metab. 2019, 30, 745–755. [Google Scholar] [CrossRef]
- Han, J.; Li, Y.; Liu, X.; Zhou, T.; Sun, H.; Edwards, P.; Gao, H.; Yu, F.S.; Qiao, X. Metformin suppresses retinal angiogenesis and inflammation in vitro and in vivo. PLoS ONE 2018, 13, e0193031. [Google Scholar] [CrossRef]
- Ahuja, S.; Uniyal, A.; Akhtar, A.; Sah, S.P. Alpha lipoic acid and metformin alleviates experimentally induced insulin resistance and cognitive deficit by modulation of TLR2 signalling. Pharmacol. Rep. 2019, 71, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.M.; Stephenson, M.D.; de Courten, B.; Chapman, I.; Bellman, S.M.; Aromataris, E. Metformin Use Associated with Reduced Risk of Dementia in Patients with Diabetes: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2018, 65, 1225–1236. [Google Scholar] [CrossRef] [PubMed]
- Orkaby, A.R.; Cho, K.; Cormack, J.; Gagnon, D.R.; Driver, J.A. Metformin vs sulfonylurea use and risk of dementia in US veterans aged >/=65 years with diabetes. Neurology 2017, 89, 1877–1885. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Wahlqvist, M.L.; Lee, M.S.; Tsai, H.N. Incidence of dementia is increased in type 2 diabetes and reduced by the use of sulfonylureas and metformin. J. Alzheimer’s Dis. 2011, 24, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Herath, P.M.; Cherbuin, N.; Eramudugolla, R.; Anstey, K.J. The Effect of Diabetes Medication on Cognitive Function: Evidence from the PATH Through Life Study. Biomed. Res. Int. 2016, 2016, 7208429. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhou, K.; Wang, R.; Liu, Y.; Kwak, Y.D.; Ma, T.; Thompson, R.C.; Zhao, Y.; Smith, L.; Gasparini, L.; et al. Antidiabetic drug metformin (GlucophageR) increases biogenesis of Alzheimer’s amyloid peptides via up-regulating BACE1 transcription. Proc. Natl. Acad. Sci. USA 2009, 106, 3907–3912. [Google Scholar] [CrossRef]
- Barini, E.; Antico, O.; Zhao, Y.; Asta, F.; Tucci, V.; Catelani, T.; Marotta, R.; Xu, H.; Gasparini, L. Metformin promotes tau aggregation and exacerbates abnormal behavior in a mouse model of tauopathy. Mol. Neurodegener. 2016, 11, 16. [Google Scholar] [CrossRef]
- Chapman, L.E.; Darling, A.L.; Brown, J.E. Association between metformin and vitamin B12 deficiency in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2016, 42, 316–327. [Google Scholar] [CrossRef]
- Imfeld, P.; Bodmer, M.; Jick, S.S.; Meier, C.R. Metformin, other antidiabetic drugs, and risk of Alzheimer’s disease: A population-based case-control study. J. Am. Geriatr. Soc. 2012, 60, 916–921. [Google Scholar] [CrossRef]
- Moore, E.M.; Mander, A.G.; Ames, D.; Kotowicz, M.A.; Carne, R.P.; Brodaty, H.; Woodward, M.; Boundy, K.; Ellis, K.A.; Bush, A.I.; et al. Increased risk of cognitive impairment in patients with diabetes is associated with metformin. Diabetes Care 2013, 36, 2981–2987. [Google Scholar] [CrossRef]
- Kuan, Y.C.; Huang, K.W.; Lin, C.L.; Hu, C.J.; Kao, C.H. Effects of metformin exposure on neurodegenerative diseases in elderly patients with type 2 diabetes mellitus. Prog. Neuropsychopharmacol. Biol. Psychiatry 2017, 79, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Picone, P.; Nuzzo, D.; Caruana, L.; Messina, E.; Barera, A.; Vasto, S.; Di Carlo, M. Metformin increases APP expression and processing via oxidative stress, mitochondrial dysfunction and NF-κB activation: Use of insulin to attenuate metformin’s effect. Biochim. Biophys. Acta 2015, 1853, 1046–1059. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, G.R.; Lakshmi, G.; Nagamani, G. Emerging links between type 2 diabetes and Alzheimer’s disease. World J. Diabetes 2015, 6, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.; Choi, D.W.; Kim, K.J.; Cho, S.Y.; Kim, H.; Kim, K.Y.; Koh, Y.; Nam, C.M.; Kim, E. Association of metformin use with Alzheimer’s disease in patients with newly diagnosed type 2 diabetes: A population-based nested case-control study. Sci. Rep. 2021, 11, 24069. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef]
- Lai, S.W.; Liao, K.F.; Lin, C.L.; Lin, C.C.; Lin, C.H. Longitudinal data of multimorbidity and polypharmacy in older adults in Taiwan from 2000 to 2013. Biomedicine 2020, 10, 1–4. [Google Scholar] [CrossRef]
- Wang, C.Y.; Wu, Y.L.; Sheu, W.H.; Tu, S.T.; Hsu, C.C.; Tai, T.Y. Accountability and utilization of diabetes care from 2005 to 2014 in Taiwan. J. Formos. Med. Assoc. 2019, 118 (Suppl. S2), S111–S121. [Google Scholar] [CrossRef]
- Grimmsmann, T.; Himmel, W. Discrepancies between prescribed and defined daily doses: A matter of patients or drug classes? Eur. J. Clin. Pharmacol. 2011, 67, 847–854. [Google Scholar] [CrossRef]
- Wellington, K. Rosiglitazone/Metformin. Drugs 2005, 65, 1581–1592. [Google Scholar] [CrossRef]
- Ferrannini, E. The target of metformin in type 2 diabetes. N. Engl. J. Med. 2014, 371, 1547–1548. [Google Scholar] [CrossRef]
- Marinangeli, C.; Didier, S.; Ahmed, T.; Caillerez, R.; Domise, M.; Laloux, C.; Begard, S.; Carrier, S.; Colin, M.; Marchetti, P.; et al. AMP-Activated Protein Kinase Is Essential for the Maintenance of Energy Levels during Synaptic Activation. iScience 2018, 9, 1–13. [Google Scholar] [CrossRef]
- Seixas da Silva, G.S.; Melo, H.M.; Lourenco, M.V.; Lyra, E.S.N.M.; de Carvalho, M.B.; Alves-Leon, S.V.; de Souza, J.M.; Klein, W.L.; da-Silva, W.S.; Ferreira, S.T.; et al. Amyloid-beta oligomers transiently inhibit AMP-activated kinase and cause metabolic defects in hippocampal neurons. J. Biol. Chem. 2017, 292, 7395–7406. [Google Scholar] [CrossRef]
- Zhao, M.; Li, X.W.; Chen, Z.; Hao, F.; Tao, S.X.; Yu, H.Y.; Cheng, R.; Liu, H. Neuro-Protective Role of Metformin in Patients with Acute Stroke and Type 2 Diabetes Mellitus via AMPK/Mammalian Target of Rapamycin (mTOR) Signaling Pathway and Oxidative Stress. Med. Sci. Monit. 2019, 25, 2186–2194. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Deng, J.; Sheng, W.; Zuo, Z. Metformin attenuates Alzheimer’s disease-like neuropathology in obese, leptin-resistant mice. Pharmacol. Biochem. Behav. 2012, 101, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, W.H.; Nunes, A.K.; Franca, M.E.; Santos, L.A.; Los, D.B.; Rocha, S.W.; Barbosa, K.P.; Rodrigues, G.B.; Peixoto, C.A. Effects of metformin on inflammation and short-term memory in streptozotocin-induced diabetic mice. Brain Res. 2016, 1644, 149–160. [Google Scholar] [CrossRef]
- Liu, Q.; Li, S.; Quan, H.; Li, J. Vitamin B12 status in metformin treated patients: Systematic review. PLoS ONE 2014, 9, e100379. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.; Mander, A.; Ames, D.; Carne, R.; Sanders, K.; Watters, D. Cognitive impairment and vitamin B12: A review. Int. Psychogeriatr. 2012, 24, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.W.; Leung, C.S.; Leung, C.P.; Cheng, J.N. Association of metformin use with vitamin B12 deficiency in the institutionalized elderly. Arch. Gerontol. Geriatr. 2018, 79, 57–62. [Google Scholar] [CrossRef]
- Huang, K.H.; Lee, C.H.; Cheng, Y.D.; Gau, S.Y.; Tsai, T.H.; Chung, N.J.; Lee, C.Y. Correlation between long-term use of metformin and incidence of NAFLD among patients with type 2 diabetes mellitus: A real-world cohort study. Front. Endocrinol. 2022, 13, 1027484. [Google Scholar] [CrossRef]
- Huang, K.H.; Chang, Y.L.; Gau, S.Y.; Tsai, T.H.; Lee, C.Y. Dose-Response Association of Metformin with Parkinson’s Disease Odds in Type 2 Diabetes Mellitus. Pharmaceutics 2022, 14, 946. [Google Scholar] [CrossRef]
- Khattar, D.; Khaliq, F.; Vaney, N.; Madhu, S.V. Is Metformin-Induced Vitamin B12 Deficiency Responsible for Cognitive Decline in Type 2 Diabetes? Indian J. Psychol. Med. 2016, 38, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.H.; Ko, S.H.; Ahn, Y.B.; Song, K.H.; Han, K.D.; Park, Y.M.; Ko, S.H.; Kim, H.S. Association of vitamin B12 deficiency and metformin use in patients with type 2 diabetes. J. Korean Med. Sci. 2014, 29, 965–972. [Google Scholar] [CrossRef]
- Alharbi, T.J.; Tourkmani, A.M.; Abdelhay, O.; Alkhashan, H.I.; Al-Asmari, A.K.; Bin Rsheed, A.M.; Abuhaimed, S.N.; Mohammed, N.; AlRasheed, A.N.; AlHarbi, N.G. The association of metformin use with vitamin B12 deficiency and peripheral neuropathy in Saudi individuals with type 2 diabetes mellitus. PLoS ONE 2018, 13, e0204420. [Google Scholar] [CrossRef] [PubMed]
- Damiao, C.P.; Rodrigues, A.O.; Pinheiro, M.F.; Cruz, R.A.F.; Cardoso, G.P.; Taboada, G.F.; Lima, G.A. Prevalence of vitamin B12 deficiency in type 2 diabetic patients using metformin: A cross-sectional study. Sao Paulo Med. J. 2016, 134, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Kickstein, E.; Krauss, S.; Thornhill, P.; Rutschow, D.; Zeller, R.; Sharkey, J.; Williamson, R.; Fuchs, M.; Kohler, A.; Glossmann, H.; et al. Biguanide metformin acts on tau phosphorylation via mTOR/protein phosphatase 2A (PP2A) signaling. Proc. Natl. Acad. Sci. USA 2010, 107, 21830–21835. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, D.K.; Ismail, C.A.; Ghareeb, D.A. Differential metformin dose-dependent effects on cognition in rats: Role of Akt. Psychopharmacology 2016, 233, 2513–2524. [Google Scholar] [CrossRef]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Boyko, E.J.; et al. Diabetes complications severity index and risk of mortality, hospitalization, and healthcare utilization. Am. J. Manag. Care 2008, 14, 15–23. [Google Scholar]
- Chang, H.Y.; Weiner, J.P.; Richards, T.M.; Bleich, S.N.; Segal, J.B. Validating the adapted Diabetes Complications Severity Index in claims data. Am. J. Manag. Care 2012, 18, 721–726. [Google Scholar]
- Chiu, W.C.; Ho, W.C.; Liao, D.L.; Lin, M.H.; Chiu, C.C.; Su, Y.P.; Chen, P.C.; Health Data Analysis in Taiwan Research Group. Progress of Diabetic Severity and Risk of Dementia. J. Clin. Endocrinol. Metab. 2015, 100, 2899–2908. [Google Scholar] [CrossRef]
- LoGiudice, D.; Watson, R. Dementia in older people: An update. Intern. Med. J. 2014, 44, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Reinstatler, L.; Qi, Y.P.; Williamson, R.S.; Garn, J.V.; Oakley, G.P., Jr. Association of biochemical B(1)(2) deficiency with metformin therapy and vitamin B(1)(2) supplements: The National Health and Nutrition Examination Survey, 1999–2006. Diabetes Care 2012, 35, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F. Is depression a risk factor for dementia or cognitive decline? A review. Gerontology 2000, 46, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.D.; Katon, W.J.; Lovato, L.C.; Miller, M.E.; Murray, A.M.; Horowitz, K.R.; Bryan, R.N.; Gerstein, H.C.; Marcovina, S.; Akpunonu, B.E.; et al. Association of depression with accelerated cognitive decline among patients with type 2 diabetes in the ACCORD-MIND trial. JAMA Psychiatry 2013, 70, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Santabarbara, J.; Lipnicki, D.M.; Olaya, B.; Villagrasa, B.; Bueno-Notivol, J.; Nuez, L.; Lopez-Anton, R.; Gracia-Garcia, P. Does Anxiety Increase the Risk of All-Cause Dementia? An Updated Meta-Analysis of Prospective Cohort Studies. J. Clin. Med. 2020, 9, 1791. [Google Scholar] [CrossRef]
- Knopman, D.S. Dementia and cerebrovascular disease. Mayo Clin. Proc. 2006, 81, 223–230. [Google Scholar] [CrossRef]
- Wang, Y.; Li, X.; Wei, B.; Tung, T.H.; Tao, P.; Chien, C.W. Association between Chronic Obstructive Pulmonary Disease and Dementia: Systematic Review and Meta-Analysis of Cohort Studies. Dement. Geriatr. Cogn. Dis. Extra 2019, 9, 250–259. [Google Scholar] [CrossRef]
- Barnes, P.J. The cytokine network in asthma and chronic obstructive pulmonary disease. J. Clin. Investig. 2008, 118, 3546–3556. [Google Scholar] [CrossRef]
- Torres-Sanchez, I.; Rodriguez-Alzueta, E.; Cabrera-Martos, I.; Lopez-Torres, I.; Moreno-Ramirez, M.P.; Valenza, M.C. Cognitive impairment in COPD: A systematic review. J. Bras. Pneumol. 2015, 41, 182–190. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total | Metformin | |||||
|---|---|---|---|---|---|---|---|
| Non-Users | Users | p-Value | |||||
| N | % | N | % | N | % | ||
| Total | 736,473 | 100.00 | 354,145 | 51.36 | 382,328 | 48.64 | |
| Gender | |||||||
| Female | 378,225 | 51.36 | 187,099 | 52.83 | 191,126 | 49.99 | <0.001 |
| Male | 358,248 | 48.64 | 167,046 | 47.17 | 191,202 | 50.01 | |
| Age (year) (Mean ± SD) | 62.03 ± 8.76 | 62.90 ± 9.06 | 61.22 ± 8.39 | <0.001 | |||
| 50–64 | 475,964 | 64.63 | 215,283 | 60.79 | 260,681 | 68.18 | |
| 65–74 | 181,583 | 24.66 | 92,699 | 26.18 | 88,884 | 23.25 | |
| 75+ | 78,926 | 10.72 | 46,163 | 13.04 | 32,763 | 8.57 | |
| Income level (NTD) a | <0.001 | ||||||
| ≤21,000 | 381,282 | 51.77 | 187,444 | 52.93 | 193,838 | 50.70 | |
| 21,001–33,000 | 174,995 | 23.76 | 78,427 | 22.15 | 96,568 | 25.26 | |
| ≥33,001 | 180,196 | 24.47 | 88,274 | 24.93 | 91,922 | 24.04 | |
| Urbanization | <0.001 | ||||||
| Level 1 | 203,376 | 27.61 | 103,603 | 29.25 | 99,773 | 26.10 | |
| Level 2 | 238,177 | 32.34 | 113,779 | 32.13 | 124,398 | 32.54 | |
| Level 3 | 114,530 | 15.55 | 52,472 | 14.82 | 62,058 | 16.23 | |
| Level 4 | 103,176 | 14.01 | 48,606 | 13.72 | 54,570 | 14.27 | |
| Level 5 | 17,291 | 2.35 | 8405 | 2.37 | 8886 | 2.32 | |
| Level 6 | 31,369 | 4.26 | 14,398 | 4.07 | 16,971 | 4.44 | |
| Level 7 | 28,554 | 3.88 | 12,882 | 3.64 | 15,672 | 4.10 | |
| DCSI score b | <0.001 | ||||||
| 0 | 447,130 | 60.71 | 211,227 | 59.64 | 235,903 | 61.70 | |
| 1 | 157,532 | 21.39 | 75,610 | 21.35 | 81,922 | 21.43 | |
| 2+ | 131,811 | 17.90 | 67,308 | 19.01 | 64,503 | 16.87 | |
| Hypertension | <0.001 | ||||||
| No | 404,777 | 54.96 | 189,444 | 53.49 | 215,333 | 56.32 | |
| Yes | 331,696 | 45.04 | 164,701 | 46.51 | 166,995 | 43.68 | |
| Hyperlipidemia | <0.001 | ||||||
| No | 579,453 | 78.68 | 265,968 | 75.10 | 313,485 | 81.99 | |
| Yes | 157,020 | 21.32 | 88,177 | 24.90 | 68,843 | 18.01 | |
| Hyperuricemia | <0.001 | ||||||
| No | 730,080 | 99.13 | 350,573 | 98.99 | 379,507 | 99.26 | |
| Yes | 6393 | 0.87 | 3572 | 1.01 | 2821 | 0.74 | |
| Cerebrovascular disease | <0.001 | ||||||
| No | 699,849 | 95.03 | 334,521 | 94.46 | 365,328 | 95.55 | |
| Yes | 36,624 | 4.97 | 19,624 | 5.54 | 17,000 | 4.45 | |
| Coronary artery disease | <0.001 | ||||||
| No | 672,668 | 91.34 | 320,226 | 90.42 | 352,442 | 92.18 | |
| Yes | 63,805 | 8.66 | 33,919 | 9.58 | 29,886 | 7.82 | |
| Arrhythmia | <0.001 | ||||||
| No | 705,090 | 95.74 | 337,005 | 95.16 | 368,085 | 96.27 | |
| Yes | 31,383 | 4.26 | 17,140 | 4.84 | 14,243 | 3.73 | |
| Heart failure | <0.001 | ||||||
| No | 722,542 | 98.11 | 347,017 | 97.99 | 375,525 | 98.22 | |
| Yes | 13,931 | 1.89 | 7128 | 2.01 | 6803 | 1.78 | |
| Anxiety | <0.001 | ||||||
| No | 663,384 | 90.08 | 314,858 | 88.91 | 348,526 | 91.16 | |
| Yes | 73,089 | 9.92 | 39,287 | 11.09 | 33,802 | 8.84 | |
| Depression | <0.001 | ||||||
| No | 732,707 | 99.49 | 352,120 | 99.43 | 380,587 | 99.54 | |
| Yes | 3766 | 0.51 | 2025 | 0.57 | 1741 | 0.46 | |
| COPD b | <0.001 | ||||||
| No | 692,329 | 94.01 | 330,362 | 93.28 | 361,967 | 94.67 | |
| Yes | 44,144 | 5.99 | 23,783 | 6.72 | 20,361 | 5.33 | |
| Chronic kidney disease | <0.001 | ||||||
| No | 730,618 | 99.20 | 349,812 | 98.78 | 380,806 | 99.60 | |
| Yes | 5855 | 0.80 | 4333 | 1.22 | 1522 | 0.40 | |
| Obesity | 0.012 | ||||||
| No | 733,254 | 99.56 | 352,668 | 99.58 | 380,586 | 99.54 | |
| Yes | 3219 | 0.44 | 1477 | 0.42 | 1742 | 0.46 | |
| Alcoholism | 0.950 | ||||||
| No | 736,037 | 99.94 | 353,936 | 99.94 | 382,101 | 99.94 | |
| Yes | 436 | 0.06 | 209 | 0.06 | 227 | 0.06 | |
| Variables | Three-Year Follow-Up of Incident Dementia | |||||||
|---|---|---|---|---|---|---|---|---|
| Events | Model 1 | Model 2 | ||||||
| N | % | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Total | 7590 | 1.03 | ||||||
| cDDD of metformin use | ||||||||
| Non-users | 4245 | 1.20 | 1 | |||||
| DDD < 300 | 3312 | 0.88 | 0.92 | 0.88–0.96 | <0.001 | - | - | - |
| DDD 300–500 | 30 | 0.59 | 0.80 | 0.56–1.15 | 0.235 | - | - | - |
| DDD 500+ | 3 | 1.28 | 1.48 | 0.48–4.60 | 0.496 | - | - | - |
| Intensity of metformin use | ||||||||
| Non-users | 4245 | 1.20 | 1 | |||||
| <10 | 2526 | 0.91 | - | - | - | 0.92 | 0.87–0.97 | <0.001 |
| 10~25 | 786 | 0.78 | - | - | - | 0.92 | 0.85–1.00 | 0.037 |
| 25+ | 33 | 0.62 | - | - | - | 0.84 | 0.60–1.18 | 0.317 |
| Gender | ||||||||
| Female | 4115 | 1.09 | 1 | 1 | ||||
| Male | 3475 | 0.97 | 0.94 | 0.90–0.98 | 0.006 | 0.94 | 0.90–0.98 | 0.006 |
| Age (year) | ||||||||
| 50–64 | 1145 | 0.24 | 1 | 1 | ||||
| 65–74 | 2981 | 1.64 | 6.27 | 5.85–6.72 | <0.001 | 6.27 | 5.85–6.72 | <0.001 |
| 75+ | 3464 | 4.39 | 15.94 | 14.86–17.09 | <0.001 | 15.94 | 14.86–17.09 | <0.001 |
| Income level (NTD) a | ||||||||
| ≤21,000 | 4884 | 1.28 | 1 | 1 | ||||
| 21,001–33,000 | 1402 | 0.80 | 0.90 | 0.85–0.96 | <0.001 | 0.90 | 0.85–0.96 | <0.001 |
| ≥33,001 | 1304 | 0.72 | 0.91 | 0.86–0.97 | 0.005 | 0.91 | 0.86–0.97 | 0.005 |
| Urbanization | ||||||||
| Level 1 | 1907 | 0.94 | 1 | 1 | ||||
| Level 2 | 2182 | 0.92 | 0.98 | 0.92–1.04 | 0.430 | 0.98 | 0.92–1.04 | 0.429 |
| Level 3 | 1147 | 1.00 | 0.98 | 0.91–1.06 | 0.586 | 0.98 | 0.91–1.05 | 0.584 |
| Level 4 | 1251 | 1.21 | 1.00 | 0.93–1.08 | 0.909 | 1.00 | 0.93–1.08 | 0.911 |
| Level 5 | 281 | 1.63 | 1.07 | 0.95–1.22 | 0.280 | 1.07 | 0.95–1.22 | 0.279 |
| Level 6 | 458 | 1.46 | 1.07 | 0.97–1.19 | 0.202 | 1.07 | 0.97–1.19 | 0.202 |
| Level 7 | 364 | 1.27 | 0.99 | 0.89–1.11 | 0.883 | 0.99 | 0.89–1.11 | 0.884 |
| DCSI score b | ||||||||
| 0 | 3382 | 0.76 | 1 | 1 | ||||
| 1 | 1595 | 1.01 | 1.06 | 1.00–1.13 | 0.059 | 1.06 | 1.00–1.13 | 0.059 |
| 2+ | 2613 | 1.98 | 1.44 | 1.35–1.53 | <0.001 | 1.44 | 1.35–1.53 | <0.001 |
| Hypertension | ||||||||
| No | 3239 | 0.80 | 1 | 1 | ||||
| Yes | 4351 | 1.31 | 0.98 | 0.94–1.03 | 0.529 | 0.98 | 0.94–1.03 | 0.529 |
| Hyperlipidemia | ||||||||
| No | 5976 | 1.03 | 1 | 1 | ||||
| Yes | 1614 | 1.03 | 0.89 | 0.84–0.94 | <0.001 | 0.89 | 0.84–0.94 | <0.001 |
| Hyperuricemia | ||||||||
| No | 7509 | 1.03 | 1 | 1 | ||||
| Yes | 81 | 1.27 | 1.05 | 0.84–1.30 | 0.692 | 1.05 | 0.84–1.30 | 0.693 |
| Cerebrovascular disease | ||||||||
| No | 6500 | 0.93 | 1 | 1 | ||||
| Yes | 1090 | 2.98 | 1.53 | 1.42–1.64 | <0.001 | 1.53 | 1.42–1.64 | <0.001 |
| Coronary artery disease | ||||||||
| No | 6535 | 0.97 | 1 | 1 | ||||
| Yes | 1055 | 1.65 | 0.91 | 0.84–0.97 | 0.007 | 0.91 | 0.84–0.97 | 0.007 |
| Arrhythmia | ||||||||
| No | 7014 | 0.99 | 1 | 1 | ||||
| Yes | 576 | 1.84 | 1.01 | 0.93–1.11 | 0.785 | 1.01 | 0.93–1.11 | 0.784 |
| Heart failure | ||||||||
| No | 7253 | 1.00 | 1 | 1 | ||||
| Yes | 337 | 2.42 | 0.95 | 0.85–1.07 | 0.379 | 0.95 | 0.85–1.07 | 0.379 |
| Anxiety | ||||||||
| No | 6331 | 0.95 | 1 | 1 | ||||
| Yes | 1259 | 1.72 | 1.50 | 1.41–1.59 | <0.001 | 1.50 | 1.41–1.59 | <0.001 |
| Depression | ||||||||
| No | 7496 | 1.02 | 1 | 1 | ||||
| Yes | 94 | 2.50 | 1.76 | 1.43–2.16 | <0.001 | 1.76 | 1.43–2.16 | <0.001 |
| COPD b | ||||||||
| No | 6723 | 0.97 | 1 | 1 | ||||
| Yes | 867 | 1.96 | 1.11 | 1.03–1.20 | 0.004 | 1.11 | 1.03–1.20 | 0.004 |
| Chronic kidney disease | ||||||||
| No | 7455 | 1.02 | 1 | 1 | ||||
| Yes | 135 | 2.31 | 0.99 | 0.83–1.18 | 0.927 | 0.99 | 0.83–1.18 | 0.927 |
| Obesity | ||||||||
| No | 7573 | 1.03 | 1 | 1 | ||||
| Yes | 17 | 0.53 | 0.75 | 0.47–1.21 | 0.237 | 0.75 | 0.47–1.21 | 0.238 |
| Alcoholism | ||||||||
| No | 7583 | 1.03 | 1 | 1 | ||||
| Yes | 7 | 1.61 | 2.47 | 1.18–5.20 | 0.017 | 2.47 | 1.18–5.19 | 0.017 |
| Variables | Five-Year Follow-Up of Incident Dementia | |||||||
|---|---|---|---|---|---|---|---|---|
| Events | Model 1 | Model 2 | ||||||
| N | % | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Total | 15,989 | 2.17 | ||||||
| cDDD of metformin use | ||||||||
| Non-users | 8801 | 2.49 | 1 | |||||
| DDD < 300 | 7111 | 1.89 | 0.94 | 0.91–0.97 | <0.001 | - | - | - |
| DDD 300–500 | 70 | 1.37 | 0.88 | 0.70–1.12 | 0.304 | - | - | - |
| DDD 500+ | 7 | 2.98 | 1.61 | 0.77–3.38 | 0.207 | - | - | - |
| Intensity of metformin use | ||||||||
| Non-users | 8801 | 2.49 | 1 | |||||
| <10 | 5409 | 1.96 | - | - | - | 0.94 | 0.91–0.97 | <0.001 |
| 10~25 | 1702 | 1.70 | - | - | - | 0.95 | 0.90–1.00 | 0.035 |
| 25+ | 77 | 1.44 | - | - | - | 0.92 | 0.74–1.15 | 0.477 |
| Gender | ||||||||
| Female | 8811 | 2.33 | 1 | 1 | ||||
| Male | 7178 | 2.00 | 0.90 | 0.88–0.93 | <0.001 | 0.90 | 0.88–0.93 | <0.001 |
| Age (year) | ||||||||
| 50–64 | 2657 | 0.56 | 1 | 1 | ||||
| 65–74 | 6487 | 3.57 | 5.88 | 5.62–6.16 | <0.001 | 5.88 | 5.62–6.16 | <0.001 |
| 75+ | 6845 | 8.67 | 13.92 | 13.28–14.59 | <0.001 | 13.92 | 13.28–14.60 | <0.001 |
| Income level (NTD) a | ||||||||
| ≤21,000 | 10,557 | 2.77 | 1 | 1 | ||||
| 21,001–33,000 | 2692 | 1.54 | 0.78 | 0.75–0.82 | <0.001 | 0.78 | 0.75–0.82 | <0.001 |
| ≥33,001 | 2740 | 1.52 | 0.87 | 0.84–0.91 | <0.001 | 0.87 | 0.84–0.91 | <0.001 |
| Urbanization | ||||||||
| Level 1 | 3915 | 1.93 | 1 | 1 | ||||
| Level 2 | 4633 | 1.95 | 1.01 | 0.97–1.05 | 0.731 | 1.01 | 0.97–1.05 | 0.733 |
| Level 3 | 2397 | 2.09 | 1.00 | 0.95–1.05 | 0.997 | 1.00 | 0.95–1.05 | 0.994 |
| Level 4 | 2720 | 2.64 | 1.07 | 1.02–1.13 | 0.006 | 1.07 | 1.02–1.13 | 0.007 |
| Level 5 | 572 | 3.31 | 1.08 | 0.99–1.18 | 0.091 | 1.08 | 0.99–1.18 | 0.090 |
| Level 6 | 972 | 3.10 | 1.12 | 1.04–1.20 | 0.003 | 1.12 | 1.04–1.20 | 0.003 |
| Level 7 | 780 | 2.73 | 1.05 | 0.97–1.13 | 0.264 | 1.05 | 0.97–1.13 | 0.263 |
| DCSI score b | ||||||||
| 0 | 7311 | 1.64 | 1 | 1 | ||||
| 1 | 3510 | 2.23 | 1.09 | 1.04–1.13 | <0.001 | 1.09 | 1.04–1.13 | <0.001 |
| 2+ | 5168 | 3.92 | 1.38 | 1.32–1.44 | <0.001 | 1.38 | 1.32–1.44 | <0.001 |
| Hypertension | ||||||||
| No | 6976 | 1.72 | 1 | 1 | ||||
| Yes | 9013 | 2.72 | 0.97 | 0.94–1.01 | 0.112 | 0.97 | 0.94–1.01 | 0.112 |
| Hyperlipidemia | ||||||||
| No | 12,577 | 2.17 | 1 | 1 | ||||
| Yes | 3412 | 2.17 | 0.91 | 0.87–0.94 | <0.001 | 0.91 | 0.87–0.94 | <0.001 |
| Hyperuricemia | ||||||||
| No | 15,821 | 2.17 | 1 | 1 | ||||
| Yes | 168 | 2.63 | 1.05 | 0.91–1.23 | 0.498 | 1.05 | 0.91–1.23 | 0.499 |
| Cerebrovascular disease | ||||||||
| No | 13,905 | 1.99 | 1 | 1 | ||||
| Yes | 2084 | 5.69 | 1.45 | 1.38–1.52 | <0.001 | 1.45 | 1.38–1.52 | <0.001 |
| Coronary artery disease | ||||||||
| No | 13,744 | 2.04 | 1 | 1 | ||||
| Yes | 2245 | 3.52 | 0.95 | 0.91–1.00 | 0.049 | 0.95 | 0.91–1.00 | 0.049 |
| Arrhythmia | ||||||||
| No | 14,787 | 2.10 | 1 | 1 | ||||
| Yes | 1202 | 3.83 | 1.05 | 0.99–1.11 | 0.129 | 1.05 | 0.99–1.11 | 0.129 |
| Heart failure | ||||||||
| No | 15,331 | 2.12 | 1 | 1 | ||||
| Yes | 658 | 4.72 | 0.93 | 0.85–1.01 | 0.071 | 0.93 | 0.85–1.01 | 0.071 |
| Anxiety | ||||||||
| No | 13,457 | 2.03 | 1 | 1 | ||||
| Yes | 2532 | 3.46 | 1.44 | 1.38–1.50 | <0.001 | 1.44 | 1.38–1.50 | <0.001 |
| Depression | ||||||||
| No | 15,820 | 2.16 | 1 | 1 | ||||
| Yes | 169 | 4.49 | 1.58 | 1.35–1.84 | <0.001 | 1.58 | 1.35–1.84 | <0.001 |
| COPD b | ||||||||
| No | 14,266 | 2.06 | 1 | 1 | ||||
| Yes | 1723 | 3.90 | 1.08 | 1.02–1.13 | 0.004 | 1.08 | 1.02–1.13 | 0.004 |
| Chronic kidney disease | ||||||||
| No | 15,745 | 2.16 | 1 | 1 | ||||
| Yes | 244 | 4.17 | 0.92 | 0.81–1.05 | 0.194 | 0.92 | 0.81–1.05 | 0.195 |
| Obesity | ||||||||
| No | 15,943 | 2.17 | 1 | 1 | ||||
| Yes | 46 | 1.43 | 0.94 | 0.71–1.26 | 0.699 | 0.95 | 0.71–1.26 | 0.701 |
| Alcoholism | ||||||||
| No | 15,979 | 2.17 | 1 | 1 | ||||
| Yes | 10 | 2.29 | 1.69 | 0.91–3.14 | 0.098 | 1.69 | 0.91–3.14 | 0.098 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, K.-H.; Tsai, Y.-F.; Lee, C.B.; Gau, S.-Y.; Tsai, T.-H.; Chung, N.-J.; Lee, C.-Y. The Correlation between Metformin Use and Incident Dementia in Patients with New-Onset Diabetes Mellitus: A Population-Based Study. J. Pers. Med. 2023, 13, 738. https://doi.org/10.3390/jpm13050738
Huang K-H, Tsai Y-F, Lee CB, Gau S-Y, Tsai T-H, Chung N-J, Lee C-Y. The Correlation between Metformin Use and Incident Dementia in Patients with New-Onset Diabetes Mellitus: A Population-Based Study. Journal of Personalized Medicine. 2023; 13(5):738. https://doi.org/10.3390/jpm13050738
Chicago/Turabian StyleHuang, Kuang-Hua, Ya-Fang Tsai, Chiachi Bonnie Lee, Shuo-Yan Gau, Tung-Han Tsai, Ning-Jen Chung, and Chien-Ying Lee. 2023. "The Correlation between Metformin Use and Incident Dementia in Patients with New-Onset Diabetes Mellitus: A Population-Based Study" Journal of Personalized Medicine 13, no. 5: 738. https://doi.org/10.3390/jpm13050738
APA StyleHuang, K.-H., Tsai, Y.-F., Lee, C. B., Gau, S.-Y., Tsai, T.-H., Chung, N.-J., & Lee, C.-Y. (2023). The Correlation between Metformin Use and Incident Dementia in Patients with New-Onset Diabetes Mellitus: A Population-Based Study. Journal of Personalized Medicine, 13(5), 738. https://doi.org/10.3390/jpm13050738