


Is Ozone a Valid Adjuvant Therapy for Periodontitis and Peri-Implantitis? A Systematic Review

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol
- P (Population): subjects with periodontal or peri-implant diseases.
- I (Intervention): gaseous, oil or water ozone treatment alone or with other interventions.
- C (Comparison): subjects treated with placebo or periodontal or peri-implant treatment without ozone.
- O (Outcome): Clinical, radiographic and inflammatory periodontal and peri-implant tissue parameters.
2.2. Search Strategy
- -
- English language on the Scopus library and on the MEDLINE/PubMed database;
- -
- Reviews, systematic reviews and metanalyses were excluded from the MEDLINE/PubMed database.
2.3. Study Selection and Eligibility Criteria
- -
- Studies published in English;
- -
- Studies with clinical and/or radiographic parameters;
- -
- Adult studies.
- -
- Studies without clinical or radiographic parameters;
- -
- Studies not published in English;
- -
- Reviews or systematic reviews;
- -
- Pediatric studies.
2.4. Data Extraction and Collection
- ∘
- First author, year of article, reference and study design;
- ∘
- Population, sample size and mean age of the study population of each study;
- ∘
- Type and regimen of gas, water or oil application used in periodontal treatment in each study;
- ∘
- Time points;
- ∘
- Clinical outcomes recorded, including clinical attachment loss (CAL), probing depth (PD), bleeding on probing (BOP), plaque index (PI) and gingival index (GI);
- ∘
- Radiographic outcomes recorded, including marginal bone levels (MBL) and cytokine profiles;
- ∘
- Conclusions.
2.5. Data Synthesis
- -
- Characterize the type and regimen of treatment performed with water or oil with ozone and make possible comparisons;
- -
- Compare the clinical radiographic results and cytokine profiles and bacteria amounts after ozone treatment (gaseous, water or oil) alone or with other treatments vs. placebo or other treatments.
2.6. Quality Assessment
3. Results
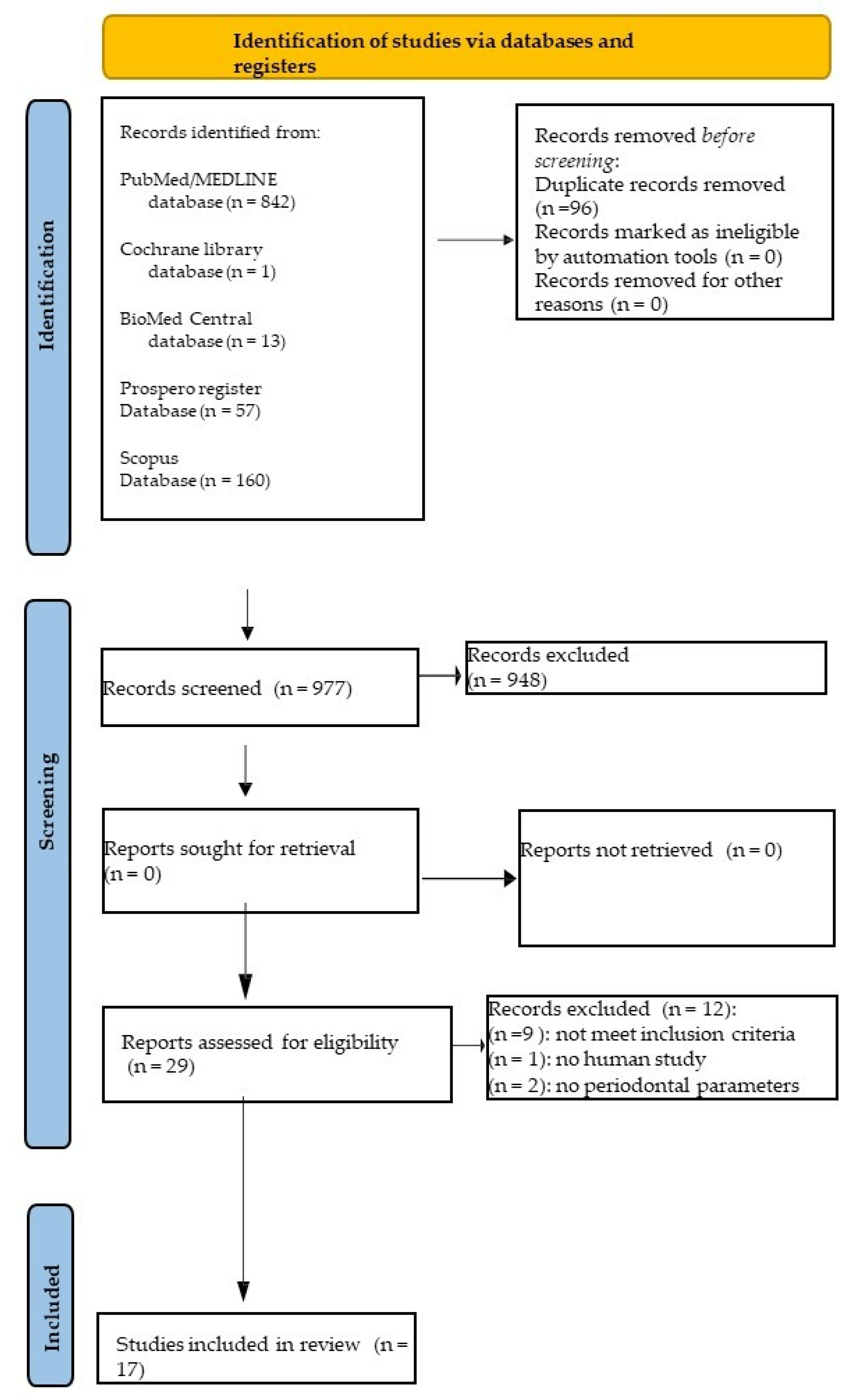
3.1. Study Selection
3.2. Study Characteristics
3.3. Data Extraction and Synthesis
3.4. Quality Assessment of the Included Studies
4. Discussion
4.1. Clinical Periodontal and Peri-Implant Parameters in Patients Treated with Gaseous Ozone
4.2. Clinical Periodontal and Peri-Implant Parameters in Patients Treated with Ozonated Water
4.3. Clinical Periodontal and Peri-Implant Parameters in Patients Treated with Ozonated Olive or Sunflower Oil
4.4. Clinical Periodontal and Peri-Implant Parameters in Patients Treated with Ozonated Gel
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bocci, V. How Does Ozone Act? How and Why Can We Avoid Ozone Toxicity? OZONE 2010, 17–26. [Google Scholar] [CrossRef]
- Solomon, S. Stratospheric Ozone Depletion: A Review of Concepts and History. Rev. Geophys. 1999, 37, 275–316. [Google Scholar] [CrossRef]
- Gupta, G.; Mansi, B. Ozone Therapy in Periodontics. J. Med. Life 2012, 5, 59–67. [Google Scholar] [PubMed]
- Bocci, V. Ozone as Janus: This Controversial Gas Can Be Either Toxic or Medically Useful. Mediat. Inflamm. 2004, 13, 3–11. [Google Scholar] [CrossRef]
- Hayes, K. Ozone: The Revolution in Dentistry. Br. Dent. J. 2005, 199, 307. [Google Scholar] [CrossRef]
- Baysan, A.; Whiley, R.A.; Lynch, E. Antimicrobial Effect of a Novel Ozone- Generating Device on Micro-Organisms Associated with Primary Root Carious Lesions in Vitro. Caries Res. 2000, 34, 498–501. [Google Scholar] [CrossRef]
- Suh, Y.; Patel, S.; Kaitlyn, R.; Gandhi, J.; Joshi, G.; Smith, N.L.; Khan, S.A. Clinical Utility of Ozone Therapy in Dental and Oral Medicine. Med. Gas Res. 2019, 9, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Nogales, C.G.; Ferrari, P.H.; Kantorovich, E.O.; Lage-Marques, J.L. Ozone Therapy in Medicine and Dentistry. J. Contemp. Dent. Pr. 2008, 9, 75–84. [Google Scholar] [CrossRef]
- Di Spirito, F.; Argentino, S.; Martuscelli, R.; Sbordone, L. Mronj Incidence After Multiple Teeth Extractions in Patients Taking Oral Bisphosphonates Without “Drug Holiday”: A Retrospective Chart Review. ORAL Implantol. 2019, 12, 105–110. [Google Scholar]
- Fortunato, L.; Amato, M.; Simeone, M.; Bennardo, F.; Barone, S.; Giudice, A. Numb Chin Syndrome: A Reflection of Malignancy or a Harbinger of MRONJ? A Multicenter Experience. J. Stomatol. Oral. Maxillofac. Surg. 2018, 119, 389–394. [Google Scholar] [CrossRef]
- Di Spirito, F.; Iandolo, A.; Amato, A.; Caggiano, M.; Raimondo, A.; Lembo, S.; Martina, S. Prevalence, Features and Degree of Association of Oral Lesions in COVID-19: A Systematic Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2022, 19, 7486. [Google Scholar] [CrossRef]
- Di Spirito, F.; Caggiano, M.; Di Palo, M.P.; Contaldo, M.; D’Ambrosio, F.; Martina, S.; Amato, A. Oral Lesions in Pediatric Subjects: SARS-CoV-2 Infection and COVID-19 Vaccination. Appl. Sci. 2022, 12, 8995. [Google Scholar] [CrossRef]
- Di Spirito, F.; Sbordone, L.; Pilone, V.; D’Ambrosio, F. Obesity and Periodontal Disease: A Narrative Review on Current Evidence and Putative Molecular Links. TODENTJ 2019, 13, 526–536. [Google Scholar] [CrossRef]
- Cortese, A.; Caggiano, M.; Carlino, F.; Pantaleo, G. Zygomatic fractures: Technical modifications for better aesthetic and functional results in older patients. Int. J. Surg. 2016, 33 (Suppl. 1), S9–S15. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and Grading of Periodontitis: Framework and Proposal of a New Classification and Case Definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef]
- Di Spirito, F.; Schiavo, L.; Pilone, V.; Lanza, A.; Sbordone, L.; D’Ambrosio, F. Periodontal and Peri-Implant Diseases and Systemically Administered Statins: A Systematic Review. Dent. J. 2021, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Peri-Implantitis: A Narrative Review on Neurobiological, Neurobehavioral and Immune-Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Lo Giudice, R.; Amato, M.; Di Palo, M.P.; D’Ambrosio, F.; Amato, A.; Martina, S. Inflammatory, Reactive, and Hypersensitivity Lesions Potentially due to Metal Nanoparticles from Dental Implants and Supported Restorations: An Umbrella Review. Appl. Sci. 2022, 12, 11208. [Google Scholar] [CrossRef]
- Boccia, G.; Di Spirito, F.; D’Ambrosio, F.; Di Palo, M.P.; Giordano, F.; Amato, M. Local and Systemic Antibiotics in Peri-Implantitis Management: An Umbrella Review. Antibiotics 2023, 12, 114. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Chatelain, S.; Derchi, G.; Di Spirito, F.; Martuscelli, R.; Porzio, M.; Sbordone, L. Antibiotic’s Effectiveness after Erupted Tooth Extractions: A Retrospective Study. Oral. Dis. 2020, 26, 967–973. [Google Scholar] [CrossRef]
- Amato, A. Oral-Systemic Health and Disorders: Latest Advances on Oral–Gut–Lung Microbiome Axis. Appl. Sci. 2022, 12, 8213. [Google Scholar] [CrossRef]
- Di Spirito, F. Oral-Systemic Health and Disorders: Latest Prospects on Oral Antisepsis. Appl. Sci. 2022, 12, 8185. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Di Spirito, F.; Amato, A.; Caggiano, M.; Lo Giudice, R.; Martina, S. Attitudes towards Antibiotic Prescription and Antimicrobial Resistance Awareness among Italian Dentists: What Are the Milestones? Healthcare 2022, 10, 1585. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, F.; Di Spirito, F.; De Caro, F.; Lanza, A.; Passarella, D.; Sbordone, L. Adherence to Antibiotic Prescription of Dental Patients: The Other Side of the Antimicrobial Resistance. Healthcare 2022, 10, 1636. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Amato, A.; Di Palo, M.P.; Cannatà, D.; Giordano, F.; D’Ambrosio, F.; Martina, S. Periodontal Management in Periodontally Healthy Orthodontic Patients with Fixed Appliances: An Umbrella Review of Self-Care Instructions and Evidence-Based Recommendations. Dent. J. 2023, 11, 35. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The Nuts and Bolts of PROSPERO: An International Prospective Register of Systematic Reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef]
- da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Nobre, M.R.C. The PICO Strategy for the Research Question Construction and Evidence Search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Converti, I.; Grassi, F.R.; Santacroce, L.; Topi, S.; Gnoni, A.; Scacco, S.; Scarano, A.; et al. The Effect of Gaseous Ozone Therapy in Conjunction with Periodontal Treatment on Glycated Hemoglobin Level in Subjects with Type 2 Diabetes Mellitus: An Unmasked Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 5467. [Google Scholar] [CrossRef]
- Elvis, A.M.; Ekta, J.S. Ozone Therapy: A Clinical Review. J. Nat. Sci. Biol. Med. 2011, 2, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Bocci, V.; Borrelli, E.; Travagli, V.; Zanardi, I. The Ozone Paradox: Ozone Is a Strong Oxidant as Well as a Medical Drug. Med. Res. Rev. 2009, 29, 646–682. [Google Scholar] [CrossRef]
- Abreu-Villela, P.; Ferraro, M.; Rodrigues, R.R.; Ferro, D.G.; Fantoni, D.T.; Koh, I.H.J.; Gioso, M.A. Ozone Therapy in the Prevention of Dental Plaque Formation in Dogs. J. Vet. Dent. 2021, 38, 18–23. [Google Scholar] [CrossRef]
- Lio, F.; Ottria, L.; Mazzetti, V.; Leggeri, A.; Casella, S.; Arcuri, L. The Effectiveness of Subgingival Irrigant Ozone-Based as Adjuvant for Non-Surgical Periodontal Therapy in the Treatment of Chronic Periodontitis: A Review. J. Biol. Regul. Homeost. Agents 2020, 34, 27–34. [Google Scholar]
- Deepthi, R.; Bilichodmath, S. Ozone Therapy in Periodontics: A Meta-Analysis. Contemp. Clin. Dent. 2020, 11, 108–115. [Google Scholar] [CrossRef]
- Srikanth, A.; Sathish, M.; Sri Harsha, A.V. Application of Ozone in the Treatment of Periodontal Disease. J. Pharm. Bioallied. Sci. 2013, 5, S89–S94. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Pascadopoli, M.; Gallo, S.; Pérez-Albacete Martínez, C.; Maté Sánchez de Val, J.E.; Parisi, L.; Gariboldi, A.; Scribante, A. Ozonized Hydrogels vs. 1% Chlorhexidine Gel for the Clinical and Domiciliary Management of Peri-Implant Mucositis: A Randomized Clinical Trial. J. Clin. Med. 2023, 12, 1464. [Google Scholar] [CrossRef]
- Tonon, C.C.; Panariello, B.H.D.; Spolidorio, D.M.P.; Gossweiler, A.G.; Duarte, S. Antibiofilm Effect of Ozonized Physiological Saline Solution on Peri-Implant-Related Biofilm. J. Periodontol. 2021, 92, 1151–1162. [Google Scholar] [CrossRef] [PubMed]
- Piva, A.; Avantaggiato, P.; Candotto, V.; Pellati, A.; Moreo, G. The Use of Ozone Therapy for Treatment of Periodontal Disease: A Split-Mouth, Randomized, Controlled Clinical Trial. J. Biol. Regul. Homeost. Agents 2020, 34, 91–98. [Google Scholar]
- Moreo, G.; Mucchi, D.; Carinci, F. Efficacy Ozone Therapy in Reducing Oral Infection of Periodontal Disease: A Randomized Clinical Trial. J. Biol. Regul. Homeost. Agents 2020, 34, 31–36. [Google Scholar] [PubMed]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Topi, S.; Gnoni, A.; Dipalma, G.; Mancini, A.; Di Domenico, M.; Tartaglia, G.M.; Scarano, A.; et al. The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 985. [Google Scholar] [CrossRef]
- Seydanur Dengizek, E.; Serkan, D.; Abubekir, E.; Aysun Bay, K.; Onder, O.; Arife, C. Evaluating Clinical and Laboratory Effects of Ozone in Non-Surgical Periodontal Treatment: A Randomized Controlled Trial. J. Appl. Oral Sci. 2019, 27, e20180108. [Google Scholar] [CrossRef]
- Ranjith, A.; Niranjana, J.M.; Baiju, K.V. Adjunctive Benefit of Ozonized Water Irrigation with Mechanical Debridement in the Management of Stage III Periodontitis: A Randomized Controlled Clinical and Biochemical Study. Int. J. Dent. Hyg. 2022, 20, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Tasdemir, Z.; Oskaybas, M.N.; Alkan, A.B.; Cakmak, O. The Effects of Ozone Therapy on Periodontal Therapy: A Randomized Placebo-Controlled Clinical Trial. Oral Dis. 2019, 25, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, S.; Algan, S.; Gursoy, H.; Noyan, U.; Kuru, B.E.; Kadir, T. Evaluation of the Clinical and Antimicrobial Effects of the Er:YAG Laser or Topical Gaseous Ozone as Adjuncts to Initial Periodontal Therapy. Photomed. Laser Surg. 2013, 31, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Kshitish, D.; Laxman, V.K. The Use of Ozonated Water and 0.2% Chlorhexidine in the Treatment of Periodontitis Patients: A Clinical and Microbiologic Study. Indian J. Dent. Res. 2010, 21, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Hayakumo, S.; Arakawa, S.; Mano, Y.; Izumi, Y. Clinical and Microbiological Effects of Ozone Nano-Bubble Water Irrigation as an Adjunct to Mechanical Subgingival Debridement in Periodontitis Patients in a Randomized Controlled Trial. Clin. Oral Investig. 2013, 17, 379–388. [Google Scholar] [CrossRef]
- Nicolini, A.C.; Rotta, I.D.S.; Langa, G.P.J.; Friedrich, S.A.; Arroyo-Bonilla, D.A.; Wagner, M.C.; Weidlich, P.; Rösing, C.K.; Cavagni, J. Efficacy of Ozonated Water Mouthwash on Early Plaque Formation and Gingival Inflammation: A Randomized Controlled Crossover Clinical Trial. Clin. Oral. Investig. 2021, 25, 1337–1344. [Google Scholar] [CrossRef]
- Nardi, G.M.; Cesarano, F.; Papa, G.; Chiavistelli, L.; Ardan, R.; Jedlinski, M.; Mazur, M.; Grassi, R.; Grassi, F.R. Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6619. [Google Scholar] [CrossRef]
- Al Habashneh, R.; Alsalman, W.; Khader, Y. Ozone as an Adjunct to Conventional Nonsurgical Therapy in Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Periodontal. Res. 2015, 50, 37–43. [Google Scholar] [CrossRef]
- Patel, P.V.; Patel, A.; Kumar, S.; Holmes, J.C. Effect of Subgingival Application of Topical Ozonated Olive Oil in the Treatment of Chronic Periodontitis: A Randomized, Controlled, Double Blind, Clinical and Microbiological Study. Minerva Stomatol. 2012, 61, 381–398. [Google Scholar] [PubMed]
- Colombo, M.; Gallo, S.; Garofoli, A.; Poggio, C.; Arciola, C.R.; Scribante, A. Ozone Gel in Chronic Periodontal Disease: A Randomized Clinical Trial on the Anti-Inflammatory Effects of Ozone Application. Biology 2021, 10, 625. [Google Scholar] [CrossRef] [PubMed]
- Isler, S.C.; Unsal, B.; Soysal, F.; Ozcan, G.; Peker, E.; Karaca, I.R. The Effects of Ozone Therapy as an Adjunct to the Surgical Treatment of Peri-Implantitis. J. Periodontal Implant Sci. 2018, 48, 136–151. [Google Scholar] [CrossRef] [PubMed]
- Nambiar, S.; Malothu, S.; Karmakar, S.; Varkey, A.; Chandra, D.; Chava, V.K. Comparison of Ozonated Olive Oil and Chlorhexidine Gel as an Adjunct to Nonsurgical Periodontal Therapy for the Treatment of Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Pharm. Bioallied. Sci. 2022, 14, S94–S98. [Google Scholar] [CrossRef]
- Vasthavi, C.; Babu, H.M.; Rangaraju, V.M.; Dasappa, S.; Jagadish, L.; Shivamurthy, R. Evaluation of Ozone as an Adjunct to Scaling and Root Planing in the Treatment of Chronic Periodontitis: A Randomized Clinico-Microbial Study. J. Indian Soc. Periodontol. 2020, 24, 42–46. [Google Scholar] [CrossRef]
- McKenna, D.F.; Borzabadi-Farahani, A.; Lynch, E. The Effect of Subgingival Ozone and/or Hydrogen Peroxide on the Development of Peri-Implant Mucositis: A Double-Blind Randomized Controlled Trial. Int. J. Oral Maxillofac. Implant. 2013, 28, 1483–1489. [Google Scholar] [CrossRef]
- Gandhi, K.K.; Cappetta, E.G.; Pavaskar, R. Effectiveness of the Adjunctive Use of Ozone and Chlorhexidine in Patients with Chronic Periodontitis. BDJ Open 2019, 5, 17. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Pisano, M.; Amato, A.; Iandolo, A.; Caggiano, M.; Martina, S. Periodontal and Peri-Implant Health Status in Traditional vs. Heat-Not-Burn Tobacco and Electronic Cigarettes Smokers: A Systematic Review. Dent. J. 2022, 10, 103. [Google Scholar] [CrossRef]
- Caggiano, M.; Gasparro, R.; D’Ambrosio, F.; Pisano, M.; Di Palo, M.P.; Contaldo, M. Smoking Cessation on Periodontal and Peri-Implant Health Status: A Systematic Review. Dent. J. 2022, 10, 162. [Google Scholar] [CrossRef]
- Amato, M.; Di Spirito, F.; D’Ambrosio, F.; Boccia, G.; Moccia, G.; De Caro, F. Probiotics in Periodontal and Peri-Implant Health Management: Biofilm Control, Dysbiosis Reversal, and Host Modulation. Microorganisms 2022, 10, 2289. [Google Scholar] [CrossRef]
- Sechi, L.A.; Lezcano, I.; Nunez, N.; Espim, M.; Duprè, I.; Pinna, A.; Molicotti, P.; Fadda, G.; Zanetti, S. Antibacterial Activity of Ozonized Sunflower Oil (Oleozon). J. Appl. Microbiol. 2001, 90, 279–284. [Google Scholar] [CrossRef]
- Rodrigues, K.L.; Cardoso, C.C.; Caputo, L.R.; Carvalho, J.C.T.; Fiorini, J.E.; Schneedorf, J.M. Cicatrizing and Antimicrobial Properties of an Ozonised Oil from Sunflower Seeds. Inflammopharmacology 2004, 12, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Sammartino, P.; Di Vittorio, L.; Iandolo, A.; Caggiano, M.; Roghi, M.; Muzio, L.L. Use of Diode Laser for Surgical Removal of Pyogenic Granuloma of the Lower Lip in a Pediatric Patient: A Case Report. Am. J. Case Rep. 2021, 22, e929690. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Amato, A.; Sammartino, P.; Iandolo, A.; Martina, S.; Caggiano, M. Laser Therapy in the Treatment of Peri- Implantitis: State-of-the-Art, Literature Review and Meta-Analysis. Appl. Sci. 2021, 11, 5290. [Google Scholar] [CrossRef]


{kind=link}
| Authors, Year | Reason for Exclusion |
|---|---|
| Rapone, 2020 [29] | Did not meet inclusion criteria |
| Suh, 2019 [7] | Did not meet inclusion criteria |
| Elvis, 2011 [30] | Did not meet inclusion criteria |
| Bocci, 2009 [31] | Did not meet inclusion criteria |
| Abreu-Villela, 2021 [32] | Was not a human study |
| Lio, 2020 [33] | Did not meet inclusion criteria |
| Deepthi,2020 [34] | Did not meet inclusion criteria |
| Srikanth, 2013 [35] | Did not meet inclusion criteria |
| Butera, 2023 [36] | Did not meet inclusion criteria |
| Tonon, 2021 [37] | Did not meet inclusion criteria |
| Piva, 2020 [38] | Contained no periodontal parameters |
| Moreo, 2020 [39] | Contained no periodontal parameters |
| Authors, Year of Reference Study and Design | Population, Sample Size and Mean Age | Type of Ozone Used | Time Points | Main Results |
|---|---|---|---|---|
| Rapone, 2022 [40] RCT | 45 TG (SRP + GOT) 45 CG (SRP) 51.56 ± 10.35 | Gaseous ozone | 3 months 6 months | Statistically significant difference between TG and CG in CAL (p ≤ 0.0001), PPD (p ≤ 0.0001) and BoP (p ≤ 0.0001) scores. |
| Dengizek, 2019 [41] RCT | 20 TG: SRP + 3 watts gaseous ozone 20 CG: SRP + placebo 42.4 ± 6.7 | Gaseous ozone | Baseline 1 month | PI, GI, PD and CAL scores were similar for both groups (p > 0.05). |
| McKenna, 2013 [25] RCT double blind | 80 implants divided in 4 groups G1: O2 + saline (NaCl 0.9%) G2: O2 + H2O2 (3%) G3: O3 + saline G4: O3 + H2O2 60 ± 7.7 | Gaseous ozone | Baseline 7th day 14th day 21st day | Significant differences were found among the treatments (p < 0.01) for PI (F = 16.68), GI (F = 7.86) and BoP (F = 18.42) (G3 and G4 with respect to G1 and G2). |
| Ranjith, 2022 [42] RCT triple blind | 25 TG: SRP + ozonized water irrigation 25 CG: SRP + saline irrigation | Ozonized water | Baseline 4 weeks | Ozone water irrigation resulted in significant improvement in all clinical parameters except PPD. Salivary interleukin 1 beta also reduced significantly in the test group after therapy. |
| Tasdemir, 2019 [43] RCT | 18 TG: SRP + Topical GOT 18 CG: SRP + Topical GOT without starting Ozone generator 43.7 | Gaseous ozone | Baseline 3 months | PI, GI, PD, BoP and CAL were similar for both groups. All inflammatory parameters (PTX-3, Hs-CRP and IL-1) were reduced at 3-month follow-up. Only the decrease in PTX-3 levels between baseline and 3-month follow-up was statistically significant. |
| Yilmaz, 2013 [44] RCT | 10 G1: SRP + ER (YAG laser) 10 G2: SRP + topical GOT 10 G3: SRP 43 ± 5.01 (G1) 41.4 ± 8.86 (G2) 41.4 ± 4.62 (G3) | Gaseous ozone | Baseline 90th day | All treatments reduced the number of total bacteria and the proportion of obligately anaerobic microorganisms. Clinical findings, including attachment gain and PD reduction, were found to be statistically significant in favor of the SRP + Er:YAG laser group. |
| Kshitish, 2010 [45] RCT double blind | 16 G1: SRP + Ozone irrigation 16 G2: SRP + 0.2% Chlorhexidine irrigation 20–60 years (range) | Ozonated water | Baseline 7th day 18th day | A higher percentage of plaque index (12%), gingival index (29%) and bleeding index (26%) reduction was observed using ozone irrigation compared to chlorhexidine. |
| Hayakumo, 2013 [46] RCT | 11 TG: FMMD + NBW3 10 CG: FMMD + Tap Water 45.9 ± 14.8 | Ozone nano-bubble water(NBW3), tap water (WATER) | Baseline 4 weeks 8 weeks | Reduction in PPD and the clinical attachment gain after 4 and 8 weeks in the TG were significantly greater than those in the CG. TG showed statistically significant reductions in the mean total number of bacteria in subgingival plaque during the study period. |
| Nicolini, 2021 [47] RCT double blind | 21 TG: mouthwash of ozonated water 21 CG: mouthwash of bidistilled water 23.43 ± 3.63 | Ozonated water | Baseline 24h 48h 72h 96h | Plaque Free Zone Index showed no statistical difference between Test and Control groups. |
| Nardi, 2020 [48] RCT | 48 TG: SRP + mouthwashes based on ozonated olive oil 48 CG: SRP 30–60 years (range) | Ozonated Olive Oil | Baseline 14th day 1 month 6 months | A significant improvement in PI, BoP, PPD and salivary MMP-8 levels was observed in both groups. Efficacy of ozonated olive oil in decreasing MMP-8 level. Simultaneously, it slowed the decrease in the BoP index. |
| Al Habashneh, 2015 [49] RCT | 20 TG: SRP + ozonated water irrigation 21 CG: SRP + distilled water irrigation 39.7 ± 13.7 (TG) 39 ± 10.2 (CG) | Ozonated water | Baseline 3 months | Statistically significant improvement in the study parameters in both groups between T0 and T1 except for gingival index. |
| Patel, 2012 [50] RCT double blind | 20 Group A: SRP 20 Group B: SPR + topical ozonated olive oil 20 Group C: topical ozonated olive oil 20 Group D: topical chlorhexidine | Ozonated Olive Oil | Baseline 4 weeks 8 weeks | Group B resulted in a significant improvement (p < 0.001) in clinical parameters as well as microbiological parameters over the time frame and in comparison to the control groups. Group C showed a significant improvement (p < 0.001) in clinical parameters as well as microbiological parameters. There was a significant increase (p < 0.05) in dentinal hypersensitivity following OZO as an adjunct to scaling and root planing therapy. |
| Gandhi, 2019 [36] RCT double blind | 25 TG (2 Quadrants): SRP + ozonated olive oil 25 CG (2 Quadrants): SRP + chlorhexidine 30–60 years (range) | Ozonated Olive Oil | Baseline 3 months | Regarding intergroup comparison, no statistically significant differences were found between the CHX and ozonated olive oil groups regarding any of the clinical and microbiological parameters at the follow-up visit. |
| Colombo, 2021 [51] Prospective single-group and single-center RCT | 10 TG: SRP + ozone gel 10 CG: SRP + chlorhexidine gel 50.0 | Ozone gel | Baseline 1 month 3 months | The use of the ozonized gel in addition to SRP did not show significant differences compared to conventional SRP + chlorhexidine. |
| Isler, 2018 [52] RCT | 20 TG: MD + sterile saline + GOT 21 CG: MD + sterile saline 53.55 ± 8.98 | Gaseous ozone | Baseline 1 month 3 months 6 months 12 months | Treatment success was obtained in 50% of the implants in the ozone group and 36.6% of the implants in the control group. However, a statistically significant difference was not observed between the groups regarding treatment success. |
| Nambiar, 2022 [53] RCT | 30 TG: SRP + ozonated olive oil 30 CG: SRP + chlorhexidine gel 38.2 | Ozonated Olive Oil | Baseline 3 months | Three months’ posttreatment, all the parameters showed significant improvement in both groups. However, the intergroup comparison failed to be statistically significant. |
| Vasthavi, 2020 [54] RCT | 12 TG: SRP + ozonated water irrigation 12 CG: SRP + distilled water irrigation 30–65 years (range) | Ozonated water | Baseline 14th day 21st day 2 months | Significant improvement in both clinical and microbiological parameters suggests that subgingival ozonated water irrigation could be an efficient adjunct to SRP. |
| Periodontal Clinical and Radiographic Parameters | Author, Year of Reference Study and Design | Main Results | Considerations |
|---|---|---|---|
| CAL | Dengizek, 2019 [41] RCT | The levels of CAL were similar for both groups (p > 0.05). | No statistically significant difference between the groups. |
| CAL | Tasdemir, 2019 [43] RCT | The levels of CAL were similar for both groups. | No significant differences between the two groups at baseline or 3 months (p > 0.05). |
| CAL CAL | Rapone, 2022 [40] RCT Isler, 2018 [52] RCT | At 3 months, a statistically significant difference between groups was observed from baseline in the CAL (p ≤ 0.0001). At 12 months postoperatively, significant differences were observed in the CAL values for both groups compared to baseline (p < 0.001). | There were significant CAL differences among the groups. There were no statistically significant differences in the CAL values between the groups. |
| BOP | McKenna, 2013 [36] RCT double blind | Significant differences were seen among the treatments (p < 0.01) regarding bleeding. | O3 + NaCl and O3 + H2O2 were equally the most effective treatments, whereas O2 + NaCl was the least effective in controlling the bleeding around implants. |
| BOP | Rapone, 2022 [40] RCT | At 3 months, a statistically significant difference in the BOP (p ≤ 0.0001) was observed between the groups. | SRP + ozone therapy improved BOP compared with SRP alone. |
| BOP | Tasdemir, 2019 [43] RCT | Significant decreases in percentage of BOP were determined in both groups after periodontal treatment. | No significant differences between the two groups at baseline or 3 months (p > 0.05). |
| PPD | Tasdemir, 2019 [43] RCT | Significant decreases in PD were determined in both groups after periodontal treatment. | No significant differences between the two groups at baseline or 3 months (p > 0.05). |
| PPD | Yilmaz, 2013 [44] RCT | Statistically significant differences were detected in favor of Group 1 in the double comparisons of Group 1–Group 2, Group 1–Group 3 and Group 2–Group 3 (p = 0.002; p = 0.09; and p = 0.365, respectively). | SRP + Er:YAG laser was more effective in PPD reduction compared to SRP + ozone or SRP only. |
| PPD | Rapone, 2022 [40] RCT | At 3 months, a statistically significant difference in the PPD (p ≤ 0.0001) was observed between the groups. | SRP + ozone therapy improved PPD compared to SRP only. |
| PI | Dengizek, 2019 [41] RCT | PI score was similar for both groups (p > 0.05). | No statistically significant difference between both groups. |
| PI | McKenna, 2013 [55] RCT double blind | Significant differences were seen among the treatments (p < 0.01) for plaque (F = 16.68). | In order of increasing effectiveness, we observed O2 + NaCl, O2 + H2O2, O3 + NaCl, and O3 + H2O2. O3 with or without H2O2 can reduce the development of peri-implant mucositis. |
| PI | Tasdemir, 2019 [43] RCT | Similar decreases in PI indicators of oral hygiene were observed on both sides. | This finding is not surprising since oral hygiene motivations were repeated after all sessions. |
| GI | Dengizek, 2019 [41] RCT | GI score was similar for both groups (p > 0.05). | No statistically significant difference between both groups. |
| GI | McKenna, 2013 [55] RCT double blind | Significant differences were seen among the treatments (p < 0.01) regarding gingival index (F = 7.86). | In order of increasing effectiveness, we observed O2 + NaCl, O2 + H2O2, O3 + NaCl, and O3 + H2O2. O3 with or without H2O2 can reduce the development Of peri-implant mucositis. |
| PD | Isler, 2018 [52] RCT | A significant difference was only detected in the PD values between the groups at the 3-month follow- up period in favor of the ozone group (p < 0.05). | At 12 months postoperatively, significant differences were observed in the PD values for both groups compared to baseline (p < 0.001). |
| Periodontal Clinical and Radiographic Parameters | Author, Year of Reference Study and Design | Main Results | Considerations |
|---|---|---|---|
| CAL | Ranjith, 2022 [42] RCT triple blind | The mean clinical attachment gain in moderate and deep pockets was significantly greater in the test group (p < 0.01). | Significant clinical attachment gain may be indicative of better tissue regeneration with the use of ozone therapy compared to saline. |
| BOP | Kshitish, 2010 [45] RCT double blind | A higher percentage of bleeding index (26%) reduction was observed using ozone irrigation compared to chlorhexidine. | Ozone may be considered an alternative management strategy due to its powerful ability to inactivate microorganisms. |
| PPD | Ranjith, 2022 [42] RCT triple blind | Ozone water irrigation resulted in significant reduction in pocket depth in deep pockets (p = 0.01) and the number of sites with a pocket depth ≥ 4 mm with bleeding on probing. | PPD reduction was statistically significant for deep pockets (>7 mm) and for pockets with depth ≥ 4 mm with bleeding on probing. |
| PPD | Hayakumo, 2013 [46] RCT | There were statistically significant improvements in the full-mouth mean PPD in both groups from baseline to 4 weeks and 8 weeks. The differences in the full-mouth mean PPD were not statistically significant at each follow-up visit. | The reductions in mean PPD from baseline to 4 and 8 weeks in the NBW3 group were significantly greater than those in the water group. |
| PI | Kshitish, 2010 [45] RCT double blind | A higher percentage of plaque index (12%) reduction was observed using ozone irrigation compared to chlorhexidine. | Ozone may be considered an alternative management strategy due to its powerful ability to inactivate microorganisms. |
| PI | Nicolini, 2021 [47] RCT double blind | Both groups presented a very similar pattern of plaque formation according to the Plaque Free Zone Index at all time points. | No statistically significant differences among the groups. |
| GI | Al Habashneh, 2015 [49] RCT | The decrease sin gingival indexes were comparable in the two treatment groups. | Ozonated water irrigation as an adjunctive therapy to SRP produced no statistically significant benefit compared to SRP with distilled water irrigation. |
| GI | Kshitish, 2010 [45] RCT double blind | A higher percentage of gingival index (29%) reduction was observed using ozone irrigation compared to chlorhexidine. | Ozone may be considered an alternative management strategy due to its powerful ability to inactivate microorganisms. |
| IL-1b | Ranjith, 2022 [42] RCT triple blind | Reduction in salivary IL1 β was noticed 1 month after ozone water irrigation. | Salivary interleukin 1 beta reduced significantly in the test group after therapy. |
| PI | Vasthavi, 2020 [54] RCT | The mean PI scores of TG at the baseline and after 2 months were 2.505 ± 0.318 and 1.416 ± 0.372, respectively, showing a statistically significant difference (p < 0.001). | The mean difference in scores between the groups was not statistically significant. |
| GI | Vasthavi, 2020 [54] RCT | The mean GI scores of TG at the baseline and after 2 months were 2.569 ± 0.336 and 1.512 ± 0.406, respectively, showing a statistically significant difference (p < 0.001). | The mean difference in scores between the groups was statistically significant. |
| PPD | Vasthavi, 2020 [54] RCT | The mean PPD scores of TG at the baseline and after 2 months were 6.833 ± 1.193 and 4.500 ± 0.797, respectively, showing a statistically significant difference (p < 0.001). | The mean difference in scores between the groups was statistically significant. |
| Periodontal Clinical and Radiographic Parameters | Author, Year of Reference Study and Design | Main Results | Considerations |
|---|---|---|---|
| BOP BOP BOP | Patel, 2012 [50] RCT double blind Nardi, 2020 [48] RCT Nambiar, 2022 [53] RCT | The adjunctive use of the OZO with SRP resulted in a significant improvement (p < 0.001) in BOP. A significant improvement in BoP was observed in both groups. There was a non-statistically significant reduction in both groups, but not between the two groups. | Ozonate olive oil + SRP improved BOP. The ozonated olive oil mouthwash slowed the decrease in BoP index at the beginning of treatment. No differences between ozone olive oil + SRP and clorexidine group + SRP. |
| PPD PPD PPD PI | Nardi, 2020 [48] RCT Patel, 2012 [50] RCT double blind Nambiar, 2022 [53] RCT Patel, 2012 [50] RCT double blind | Groups showed significantly different variances regarding PPD (p < 0.001 in Levene’s test). The adjunctive use of the OZO with SRP resulted in a significant improvement (p < 0.001) in PPD. There was a non-statistically significant reduction in both groups, but not between the two groups. The adjunctive use of the OZO with SRP resulted in a significant improvement (p < 0.001) in PI. | PPD decreased both in the study and control group with no statistical significance. Ozonate olive oil + SRP improved PPD. No differences between ozone olive oil + SRP and clorexidine group + SRP. Ozonate olive oil + SRP improved PI. |
| PI | Nardi, 2020 [48] RCT | A significant improvement in PI was observed in both groups. | Ozonated olive oil slowed the decrease in PI index at the beginning of treatment (at T1). |
| MMP-8 | Nardi, 2020 [48] RCT | This study showed the efficacy of ozonated olive oil in decreasing MMP-8 levels. | SRP + ozonated oil led to a significant and faster reduction in saliva MMP-8 concentrations in patients with periodontitis. |
| PPD GI | Gandhi, 2019 [56] RCT double blind Patel, 2012 [50] RCT double blind | No significant difference was found in the efficacy of ozonated olive oil and CHX in improving the PD. The adjunctive use of the OZO with SRP resulted in a significant improvement (p < 0.001) in GI. | No statistically significant differences were found between the CHX and ozonated olive oil groups regarding any of the clinical parameters at the follow-up visit. Ozonate olive oil + SRP improved GI. |
| CAL CAL CAL | Gandhi, 2019 [56] RCT double blind Nambiar, 2022 [53] RCT Patel, 2012 [50] RCT double blind | No significant difference was found in the efficacy of ozonated olive oil and CHX in improving clinical attachment levels. There was a non-statistically significant reduction in both groups, but not between the two groups. The adjunctive use of the OZO with SRP resulted in a significant improvement (p < 0.001) in CAL. | No statistically significant differences were found between the CHX and ozonated olive oil groups regarding any of the clinical and microbiological parameters at the follow-up visit. No differences between ozone olive oil + SRP and clorexidine group + SRP. Ozonate olive oil + SRP improved CAL. |
| Periodontal Clinical and Radiographic Parameters | Author, Year of Reference and Study Design | Main Results | Considerations |
|---|---|---|---|
| CAL | Colombo, 2021 [51] Prospective single-group and single-center RCT | Significant intragroup differences were found between each time point for the sites treated with SRP plus chlorhexidine (p < 0.05), whereas for ozone, a significant improvement was found at T1 but not at T2. | A significant intergroup difference was found between the sites at T2 (p < 0.05). |
| BOP | Colombo, 2021 [51] Prospective single-group and single-center RCT | Significant intragroup differences were found between each time point for both groups. | Significant intergroup differences were found between the sites (p > 0.05). |
| PPD | Colombo, 2021 [51] Prospective single-group and single-center RCT | Significant intragroup differences were found between each time point for both groups. | Significant intergroup differences were found between the sites (p > 0.05). |
| Studies | Bias due to Confounding | Bias in Selection of Participants | Bias in Measurement Classification of Interventions | Bias due to Deviations from Intended Interventions | Bias due to Missing Data | Bias in Measurement of Outcomes | Bias due to Selection of the Reported Result |
|---|---|---|---|---|---|---|---|
| Rapone, 2022 [40] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Dengizek, 2019 [41] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| McKenna, 2013 [55] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Ranjith, 2022 [42] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Nambiar, 2022 [53] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Vasthavi, 2020 [54] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Yilmaz, 2013 [43] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Yilmaz, 2013 [44] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Kshitish, 2010 [45] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Hayakumo, 2013 [46] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Nicolini, 2021 [47] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Nardi, 2020 [48] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Al Abashneh, 2015 [49] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Patel, 2012 [50] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Gandhi, 2019 [56] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Colombo, 2021 [51] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Isler, 2018 [52] | Y/PY/ PN/N | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI | Y/PY/ PN/N/NI |
| Risk of bias judgements | MODERATE | SERIOUS | LOW | LOW | LOW | MODERATE | LOW |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D′Ambrosio, F.; Caggiano, M.; Acerra, A.; Pisano, M.; Giordano, F. Is Ozone a Valid Adjuvant Therapy for Periodontitis and Peri-Implantitis? A Systematic Review. J. Pers. Med. 2023, 13, 646. https://doi.org/10.3390/jpm13040646
D′Ambrosio F, Caggiano M, Acerra A, Pisano M, Giordano F. Is Ozone a Valid Adjuvant Therapy for Periodontitis and Peri-Implantitis? A Systematic Review. Journal of Personalized Medicine. 2023; 13(4):646. https://doi.org/10.3390/jpm13040646
Chicago/Turabian StyleD′Ambrosio, Francesco, Mario Caggiano, Alfonso Acerra, Massimo Pisano, and Francesco Giordano. 2023. "Is Ozone a Valid Adjuvant Therapy for Periodontitis and Peri-Implantitis? A Systematic Review" Journal of Personalized Medicine 13, no. 4: 646. https://doi.org/10.3390/jpm13040646
APA StyleD′Ambrosio, F., Caggiano, M., Acerra, A., Pisano, M., & Giordano, F. (2023). Is Ozone a Valid Adjuvant Therapy for Periodontitis and Peri-Implantitis? A Systematic Review. Journal of Personalized Medicine, 13(4), 646. https://doi.org/10.3390/jpm13040646