
Generative Adversarial Networks Can Create High Quality Artificial Prostate Cancer Magnetic Resonance Images

 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Prostate MRI Images
2.2. Image Preprocessing
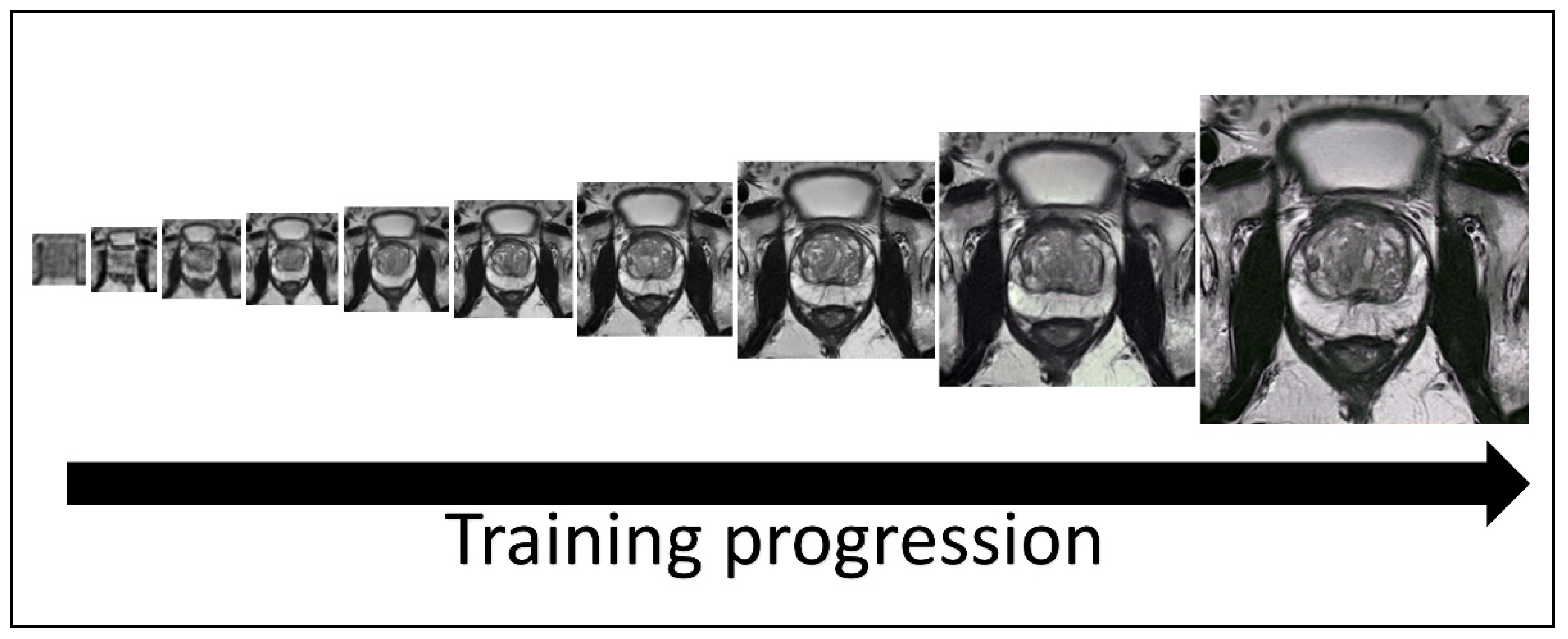
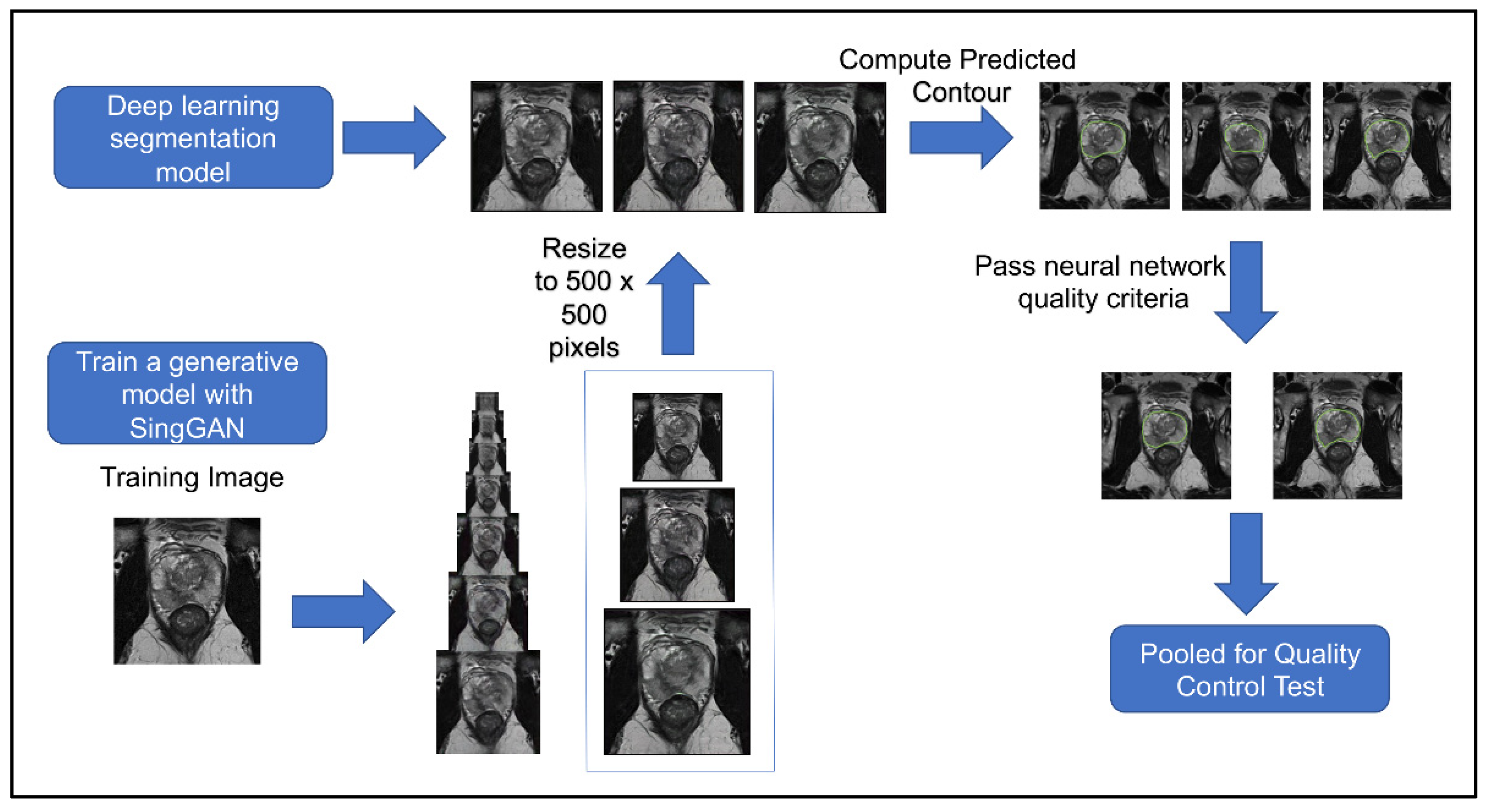
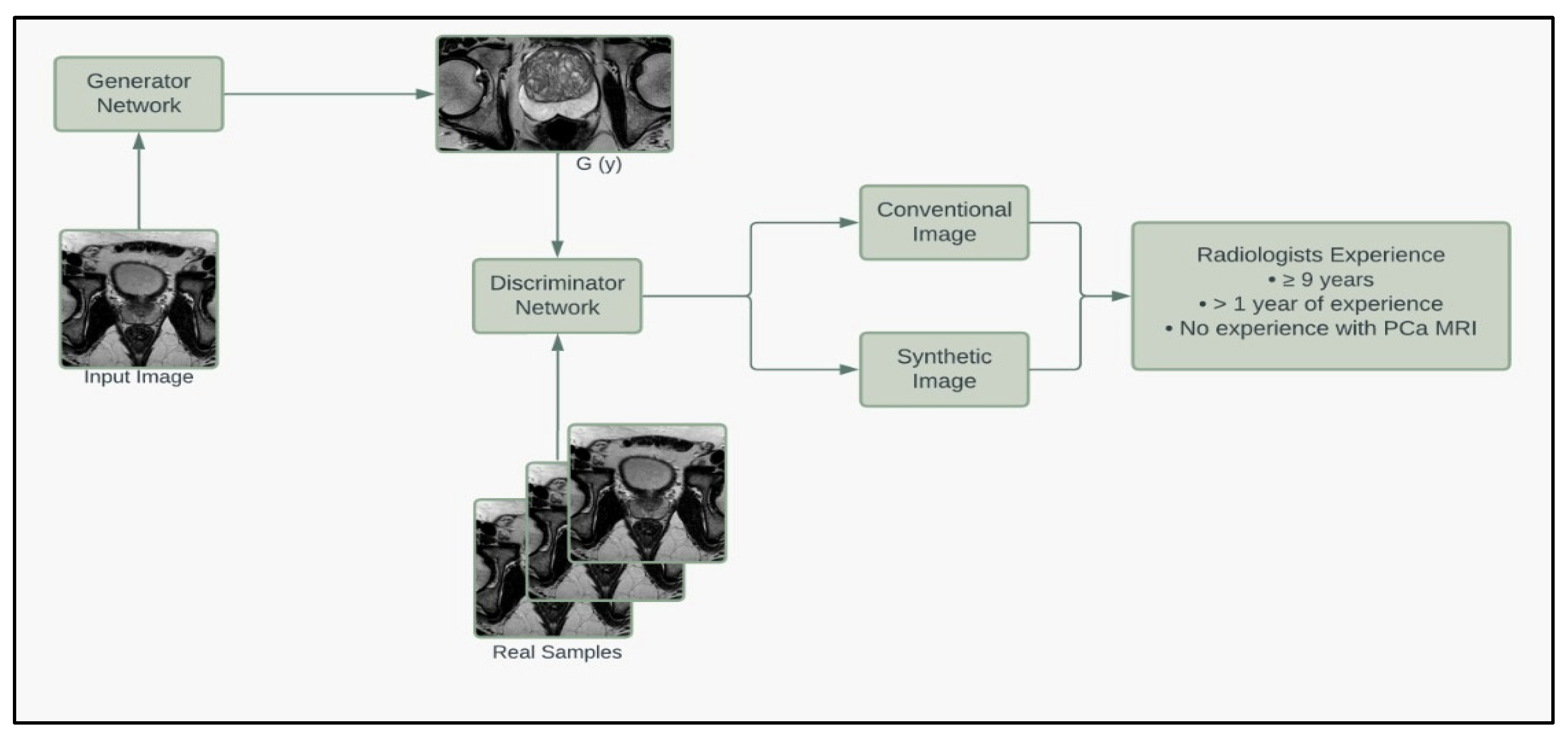
2.3. Synthetic Image Generation
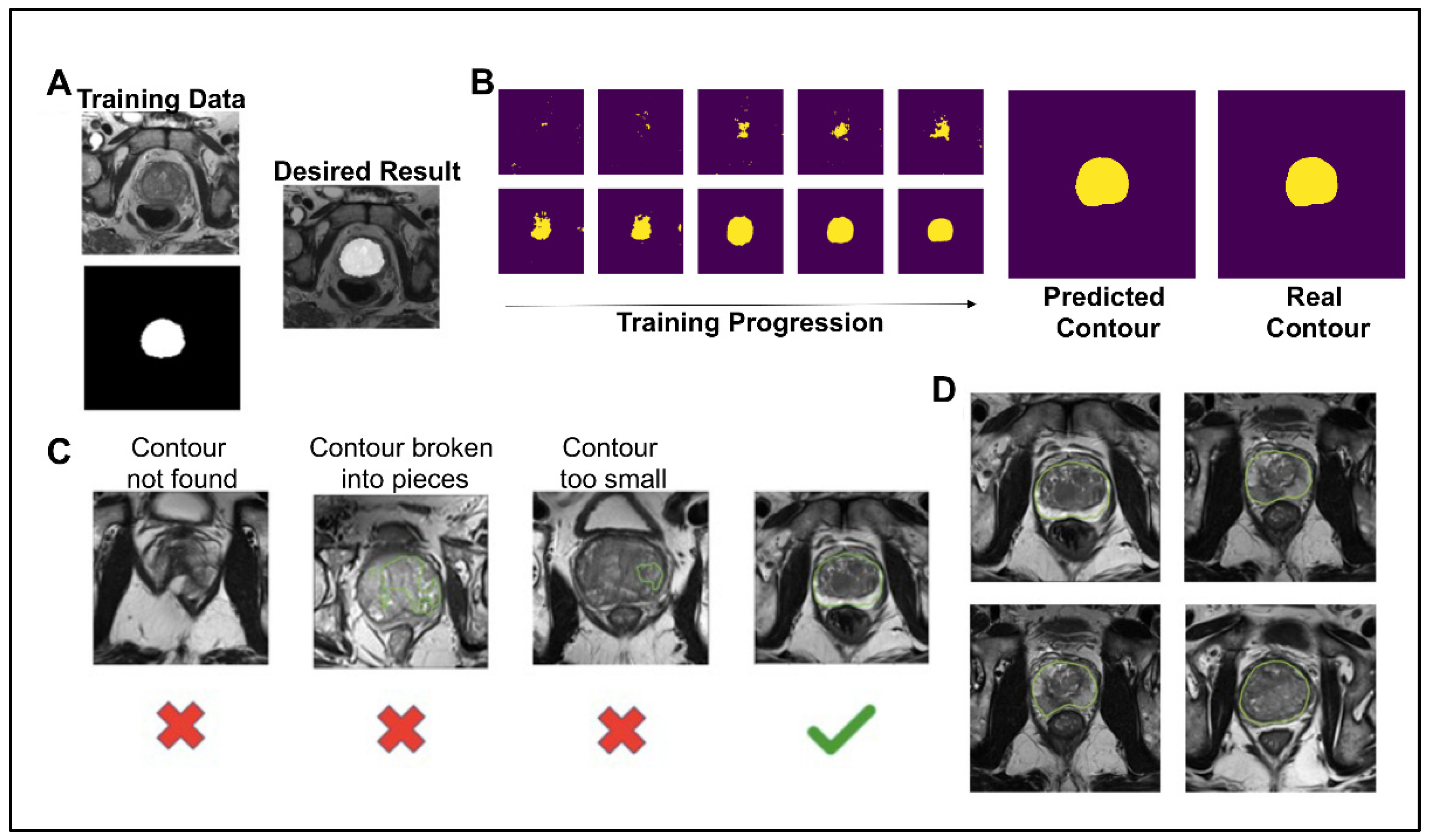
2.4. Deep Learning Image Segmentation
2.5. Quality Control Study
3. Results
3.1. Deep Learning Image Segmentation
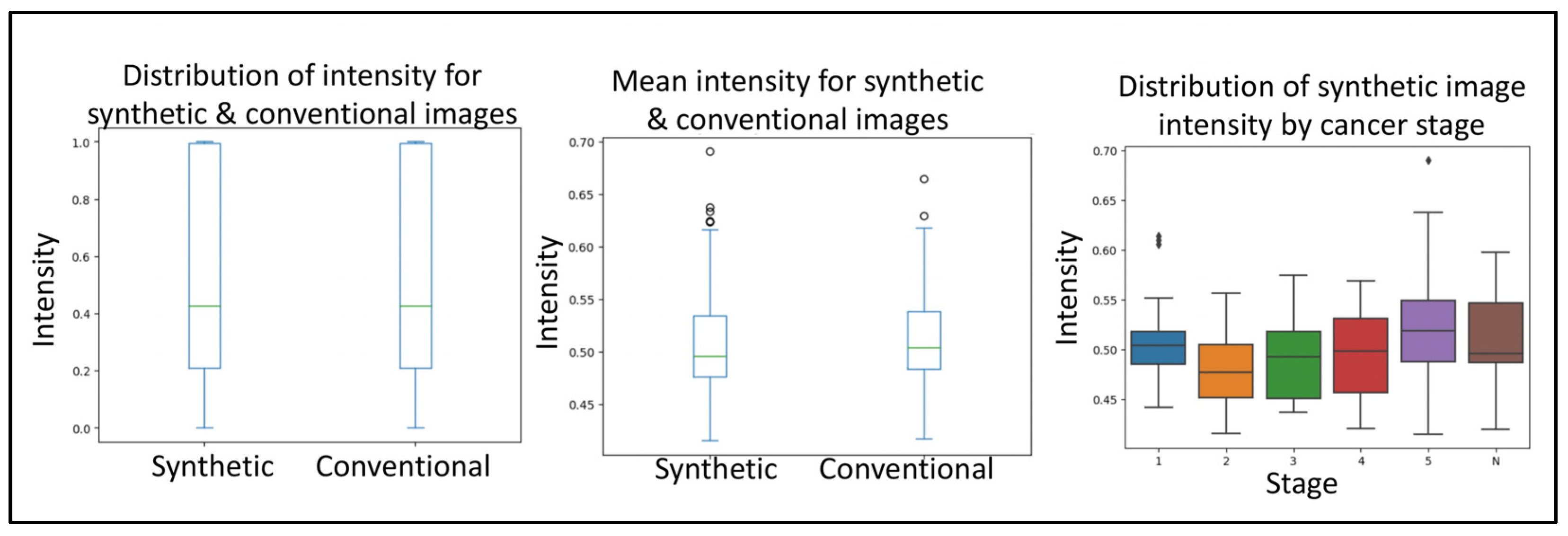
3.2. CNN Quality Control and Applicability Validation
3.3. Round 1 Quality Control Test
3.4. Round 2 Quality Control Test
3.5. Radiologist Quality Control Check
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giona, S. The Epidemiology of Prostate Cancer. In Prostate Cancer; Bott, S.R.J., Ng, K.L., Eds.; Exon Publications: Brisbane, Australia, 2021. [Google Scholar] [CrossRef]
- Sanghera, S.; Coast, J.; Martin, R.M.; Donovan, J.L.; Mohiuddin, S. Cost-effectiveness of prostate cancer screening: A systematic review of decision-analytical models. BMC Cancer 2018, 18, 84. [Google Scholar] [CrossRef] [PubMed]
- Tsodikov, A.; Gulati, R.; de Carvalho, T.M.; Heijnsdijk, E.A.M.; Hunter-Merrill, R.A.; Mariotto, A.B.; de Koning, H.J.; Etzioni, R. Is prostate cancer different in black men? Answers from 3 natural history models. Cancer 2017, 123, 2312–2319. [Google Scholar] [CrossRef] [PubMed]
- Ellinger, J.; Alajati, A.; Kubatka, P.; Giordano, F.A.; Ritter, M.; Costigliola, V.; Golubnitschaja, O. Prostate cancer treatment costs increase more rapidly than for any other cancer-how to reverse the trend? EPMA J. 2022, 13, 1–7. [Google Scholar] [CrossRef]
- Bentley, C.; Cressman, S.; van der Hoek, K.; Arts, K.; Dancey, J.; Peacock, S. Conducting clinical trials-costs, impacts, and the value of clinical trials networks: A scoping review. Clin. Trials 2019, 16, 183–193. [Google Scholar] [CrossRef]
- Gallagher, K.M.; Christopher, E.; Cameron, A.J.; Little, S.; Innes, A.; Davis, G.; Keanie, J.; Bollina, P.; McNeill, A. Four-year outcomes from a multiparametric magnetic resonance imaging (MRI)-based active surveillance programme: PSA dynamics and serial MRI scans allow omission of protocol biopsies. BJU Int. 2019, 123, 429–438. [Google Scholar] [CrossRef]
- Kam, J.; Yuminaga, Y.; Krelle, M.; Gavin, D.; Koschel, S.; Aluwihare, K.; Sutherland, T.; Skinner, S.; Brennan, J.; Wong, L.M.; et al. Evaluation of the accuracy of multiparametric MRI for predicting prostate cancer pathology and tumour staging in the real world: An multicentre study. BJU Int. 2019, 124, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Chlap, P.; Min, H.; Vandenberg, N.; Dowling, J.; Holloway, L.; Haworth, A. A review of medical image data augmentation techniques for deep learning applications. J. Med. Imaging Radiat. Oncol. 2021, 65, 545–563. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lee, C.H.; Chia, D.; Lin, Z.; Huang, W.; Tan, C.H. Machine Learning in Prostate MRI for Prostate Cancer: Current Status and Future Opportunities. Diagnostics 2022, 12, 289. [Google Scholar] [CrossRef]
- Hansen, N.; Patruno, G.; Wadhwa, K.; Gaziev, G.; Miano, R.; Barrett, T.; Gnanapragasam, V.; Doble, A.; Warren, A.; Bratt, O.; et al. Magnetic Resonance and Ultrasound Image Fusion Supported Transperineal Prostate Biopsy Using the Ginsburg Protocol: Technique, Learning Points, and Biopsy Results. Eur. Urol. 2016, 70, 332–340. [Google Scholar] [CrossRef]
- Fletcher, P.; De Santis, M.; Ippoliti, S.; Orecchia, L.; Charlesworth, P.; Barrett, T.; Kastner, C. Vector Prostate Biopsy: A Novel Magnetic Resonance Imaging/Ultrasound Image Fusion Transperineal Biopsy Technique Using Electromagnetic Needle Tracking Under Local Anaesthesia. Eur. Urol. 2023, 83, 249–256. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.; van Ginneken, B.; Sanchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed]
- Stoyanova, R.; Chinea, F.; Kwon, D.; Reis, I.M.; Tschudi, Y.; Parra, N.A.; Breto, A.L.; Padgett, K.R.; Dal Pra, A.; Abramowitz, M.C.; et al. An Automated Multiparametric MRI Quantitative Imaging Prostate Habitat Risk Scoring System for Defining External Beam Radiation Therapy Boost Volumes. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.W.; Platts-Mills, T.F. Understanding commonly encountered limitations in clinical research: An emergency medicine resident’s perspective. Ann. Emerg. Med. 2012, 59, 425–431.e411. [Google Scholar] [CrossRef]
- Tataru, O.S.; Vartolomei, M.D.; Rassweiler, J.J.; Virgil, O.; Lucarelli, G.; Porpiglia, F.; Amparore, D.; Manfredi, M.; Carrieri, G.; Falagario, U.; et al. Artificial Intelligence and Machine Learning in Prostate Cancer Patient Management-Current Trends and Future Perspectives. Diagnostics 2021, 11, 354. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.B.; Liu, C.; Ye, J.; Chang, L.F.; Xu, Q.; Shi, B.W.; Liu, L.L.; Yin, Y.L.; Shi, B.B. A comparison between deep learning convolutional neural networks and radiologists in the differentiation of benign and malignant thyroid nodules on CT images. Endokrynol. Pol. 2021, 72, 217–225. [Google Scholar] [CrossRef]
- Yu, B.; Wang, Y.; Wang, L.; Shen, D.; Zhou, L. Medical Image Synthesis via Deep Learning. Adv. Exp. Med. Biol. 2020, 1213, 23–44. [Google Scholar] [CrossRef]
- Zhao, L.; Liang, M.; Wu, P.Y.; Yang, Y.; Zhang, H.; Zhao, X. A preliminary study of synthetic magnetic resonance imaging in rectal cancer: Imaging quality and preoperative assessment. Insights Imaging 2021, 12, 120. [Google Scholar] [CrossRef]
- Kazuhiro, K.; Werner, R.A.; Toriumi, F.; Javadi, M.S.; Pomper, M.G.; Solnes, L.B.; Verde, F.; Higuchi, T.; Rowe, S.P. Generative Adversarial Networks for the Creation of Realistic Artificial Brain Magnetic Resonance Images. Tomography 2018, 4, 159–163. [Google Scholar] [CrossRef]
- Armato, S.G., 3rd; Huisman, H.; Drukker, K.; Hadjiiski, L.; Kirby, J.S.; Petrick, N.; Redmond, G.; Giger, M.L.; Cha, K.; Mamonov, A.; et al. PROSTATEx Challenges for computerized classification of prostate lesions from multiparametric magnetic resonance images. J. Med. Imaging 2018, 5, 044501. [Google Scholar] [CrossRef]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Shaham, T.R.; Dekel, T.; Michaeli, T. SinGAN: Learning a Generative Model from a Single Natural Image. In Proceedings of the 2019 IEEE/CVF International Conference on Computer Vision (ICCV), Seoul, Republic of Korea, 27 October–2 November 2019; pp. 4569–4579. [Google Scholar] [CrossRef]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative Adversarial Networks. Commun. Acm. 2020, 63, 139–144. [Google Scholar] [CrossRef]
- Caglic, I.; Sushentsev, N.; Gnanapragasam, V.J.; Sala, E.; Shaida, N.; Koo, B.C.; Kozlov, V.; Warren, A.Y.; Kastner, C.; Barrett, T. MRI-derived PRECISE scores for predicting pathologically-confirmed radiological progression in prostate cancer patients on active surveillance. Eur. Radiol. 2021, 31, 2696–2705. [Google Scholar] [CrossRef] [PubMed]
- Lovegrove, C.E.; Matanhelia, M.; Randeva, J.; Eldred-Evans, D.; Tam, H.; Miah, S.; Winkler, M.; Ahmed, H.U.; Shah, T.T. Prostate imaging features that indicate benign or malignant pathology on biopsy. Transl. Urol. 2018, 7, S420–S435. [Google Scholar] [CrossRef]
- Zavala-Romero, O.; Breto, A.L.; Xu, I.R.; Chang, Y.C.; Gautney, N.; Dal Pra, A.; Abramowitz, M.C.; Pollack, A.; Stoyanova, R. Segmentation of prostate and prostate zones using deep learning: A multi-MRI vendor analysis. Strahlenther. Onkol. 2020, 196, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.M.; Gimelshein, N.; Antiga, L.; et al. PyTorch: An Imperative Style, High-Performance Deep Learning Library. Adv. Neur. 2019, 32, 8026–8037. [Google Scholar]
- Eppel, S. Available online: https://github.com/sagieppel/Train-Semantic-Segmentation-Net-with-Pytorch-In-50-Lines-Of-Code (accessed on 20 January 2022).
- Arita, Y.; Akita, H.; Fujiwara, H.; Hashimoto, M.; Shigeta, K.; Kwee, T.C.; Yoshida, S.; Kosaka, T.; Okuda, S.; Oya, M.; et al. Synthetic magnetic resonance imaging for primary prostate cancer evaluation: Diagnostic potential of a non-contrast-enhanced bi-parametric approach enhanced with relaxometry measurements. Eur. J. Radiol. Open 2022, 9, 100403. [Google Scholar] [CrossRef]
- Khan, Z.; Yahya, N.; Alsaih, K.; Ali, S.S.A.; Meriaudeau, F. Evaluation of Deep Neural Networks for Semantic Segmentation of Prostate in T2W MRI. Sensors 2020, 20, 3183. [Google Scholar] [CrossRef]
- Sunoqrot, M.R.S.; Selnaes, K.M.; Sandsmark, E.; Nketiah, G.A.; Zavala-Romero, O.; Stoyanova, R.; Bathen, T.F.; Elschot, M. A Quality Control System for Automated Prostate Segmentation on T2-Weighted MRI. Diagnostics 2020, 10, 714. [Google Scholar] [CrossRef]
- Ghai, S.; Haider, M.A. Multiparametric-MRI in diagnosis of prostate cancer. Indian J. Urol. 2015, 31, 194–201. [Google Scholar] [CrossRef]
- Hu, S.; Lei, B.; Wang, S.; Wang, Y.; Feng, Z.; Shen, Y. Bidirectional Mapping Generative Adversarial Networks for Brain MR to PET Synthesis. IEEE Trans. Med. Imaging 2022, 41, 145–157. [Google Scholar] [CrossRef]
- Keeble, C.; Baxter, P.D.; Gislason-Lee, A.J.; Treadgold, L.A.; Davies, A.G. Methods for the analysis of ordinal response data in medical image quality assessment. Br. J. Radiol. 2016, 89, 20160094. [Google Scholar] [CrossRef] [PubMed]
- Karimi, D.; Nir, G.; Fazli, L.; Black, P.C.; Goldenberg, L.; Salcudean, S.E. Deep Learning-Based Gleason Grading of Prostate Cancer From Histopathology Images-Role of Multiscale Decision Aggregation and Data Augmentation. IEEE J. Biomed. Health 2020, 24, 1413–1426. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Round 1 | Round 2 | |||||
|---|---|---|---|---|---|---|
| Amount Conventional | 25 | 26 | ||||
| Amount Synthetic | 35 | 34 | ||||
| Experience Level | 10 Years | 1 Year | No Experience | 10 Years | 1 Year | No Experience |
| % Correct | 62 | 55 | 53 | 67 | 58 | 50 |
| % FP | 46 | 46 | 54 | 25 | 35 | 47 |
| % FN | 33 | 44 | 42 | 40 | 47 | 54 |
| % Concordance | 67 | 57 | 42 | 80 | 60 | 30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, I.R.L.; Van Booven, D.J.; Goberdhan, S.; Breto, A.; Porto, J.; Alhusseini, M.; Algohary, A.; Stoyanova, R.; Punnen, S.; Mahne, A.; et al. Generative Adversarial Networks Can Create High Quality Artificial Prostate Cancer Magnetic Resonance Images. J. Pers. Med. 2023, 13, 547. https://doi.org/10.3390/jpm13030547
Xu IRL, Van Booven DJ, Goberdhan S, Breto A, Porto J, Alhusseini M, Algohary A, Stoyanova R, Punnen S, Mahne A, et al. Generative Adversarial Networks Can Create High Quality Artificial Prostate Cancer Magnetic Resonance Images. Journal of Personalized Medicine. 2023; 13(3):547. https://doi.org/10.3390/jpm13030547
Chicago/Turabian StyleXu, Isaac R. L., Derek J. Van Booven, Sankalp Goberdhan, Adrian Breto, Joao Porto, Mohammad Alhusseini, Ahmad Algohary, Radka Stoyanova, Sanoj Punnen, Anton Mahne, and et al. 2023. "Generative Adversarial Networks Can Create High Quality Artificial Prostate Cancer Magnetic Resonance Images" Journal of Personalized Medicine 13, no. 3: 547. https://doi.org/10.3390/jpm13030547
APA StyleXu, I. R. L., Van Booven, D. J., Goberdhan, S., Breto, A., Porto, J., Alhusseini, M., Algohary, A., Stoyanova, R., Punnen, S., Mahne, A., & Arora, H. (2023). Generative Adversarial Networks Can Create High Quality Artificial Prostate Cancer Magnetic Resonance Images. Journal of Personalized Medicine, 13(3), 547. https://doi.org/10.3390/jpm13030547