
Anthropometric Features and Third-Fourth Degree Perineal Tears

 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
Data Analysis
3. Results
4. Discussion
Strengths and Weaknesses of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jangö, H.; Langhoff-Roos, J.; Rosthøj, S.; Saske, A. Long-term anal incontinence after obstetric anal sphincter injury-does grade of tear matter? Am. J. Obs. Gynecol. 2018, 218, 232-e1–232-e10. [Google Scholar] [CrossRef] [PubMed]
- Jha, S.; Parker, V. Risk factors for recurrent obstetric anal sphincter injury (rOASI): A systematic review and meta-analysis. Int. Urogynecol. J. 2016, 27, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Laine, K.; Gissler, M.; Pirhonen, J. Changing incidence of anal sphincter tears in four Nordic countries through the last decades. Eur. J. Obs. Gynecol. Reprod. Biol. 2009, 146, 71–75. [Google Scholar] [CrossRef]
- Peleg, D.; Kennedy, C.M.; Merrill, D.; Zlatnik, F.J. Risk of repetition of a severe perineal laceration. Obs. Gynecol. 1999, 93, 1021–1024. [Google Scholar]
- Thiagamoorthy, G.; Johnson, A.; Thakar, R.; Sultan, A.H. National survey of perineal trauma and its subsequent management in the United Kingdom. Int. Urogynecol. J. 2014, 25, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, S.; Londero, A.P.; Fruscalzo, A.; Driul, L.; Delneri, C.; Calcagno, A.; Di Benedetto, P.; Marchesoni, D. Impact of episiotomy on pelvic floor disorders and their influence on women’s wellness after the sixth month postpartum: A retrospective study. BMC. Women’s Health 2011, 11, 12. [Google Scholar] [CrossRef]
- Bertozzi, S.; Londero, A.P.; Fruscalzo, A.; Driul, L.; Marchesoni, D. Prevalence and Risk Factors for Dyspareunia and Unsatisfying Sexual Relationships in a Cohort of Primiparous and Secondiparous Women after 12 Months Postpartum. Int. J. Sex. Health 2010, 22, 47–53. [Google Scholar] [CrossRef]
- Driul, L.; Del Neri, C.; Bertozzi, S.; Londero, A.P.; Petrovec, M.M.; Di Benedetto, P.; Marchesoni, D. Prevalence of urinary incontinence and pelviperineal rehabilitation during the postpartum in a cohort of primipara and secondipara patients. Minerva Ginecol. 2009, 61, 89–95. [Google Scholar]
- Pergialiotis, V.; Bellos, I.; Fanaki, M.; Vrachnis, N.; Doumouchtsis, S.K. Risk factors for severe perineal trauma during childbirth: An updated meta-analysis. Eur. J. Obs. Gynecol. Reprod. Biol. 2020, 247, 94–100. [Google Scholar] [CrossRef]
- Fernando, R.; Sultan, A.; Freeman, R.; Williams, A.; Adams, E. Green-Top Guideline No. 29: The Management of Third- and Fourth-Degree Perineal Tears; Royal College of Obstetricians and Gynaecologists: London, UK, 2015. [Google Scholar]
- Jansson, M.H.; Franzén, K.; Hiyoshi, A.; Tegerstedt, G.; Dahlgren, H.; Nilsson, K. Risk factors for perineal and vaginal tears in primiparous women—The prospective POPRACT-cohort study. BMC Pregnancy Childbirth 2020, 20, 749. [Google Scholar] [CrossRef]
- Tan, A.C.C.; Mohd Yusoff, F.B.; Salleh, M.F.A.B.; Chua, A.C. What are the factors that may predict the severity of perineal tears in obstetric anal sphincter injuries and how are their outcomes? A 10-year retrospective analysis in a Southeast Asian population. Int. Urogynecol. J. 2022, 33, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, R.; Poon, L.; Cardozo, L.; Nicolaides, K. Fetomaternal BMI—A novel ultrasound predictor of obstetric anal sphincter injury. Int. Urogynecology J. 2010, 21, S300–S301. [Google Scholar]
- Khalil, M.R.; Guldberg, R.; Nørgård, B.M.; Uldbjerg, N.; Wehberg, S. Child-Mother Index: A new risk factor for selected adverse maternal birth outcomes. AJOG Glob. Rep. 2022, 2, 100090. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.A.; Brown, M.A.; Dekker, G.A.; Gatt, S.; McLintock, C.K.; McMahon, L.P.; Mangos, G.; Moore, M.P.; Muller, P.; Paech, M.; et al. Guidelines for the management of hypertensive disorders of pregnancy 2008. Aust. N. Z. J. Obs. Gynaecol. 2009, 49, 242–246. [Google Scholar] [CrossRef]
- Visentin, S.; Londero, A.P.; Camerin, M.; Grisan, E.; Cosmi, E. A possible new approach in the prediction of late gestational hypertension: The role of the fetal aortic intima-media thickness. Medicine 2017, 96, e5515. [Google Scholar] [CrossRef]
- Bertozzi, S.; Londero, A.P.; Salvador, S.; Grassi, T.; Fruscalzo, A.; Driul, L.; Marchesoni, D. Influence of the couple on hypertensive disorders during pregnancy: A retrospective cohort study. Pregnancy Hypertens. 2011, 1, 156–163. [Google Scholar] [CrossRef]
- Fruscalzo, A.; Bertozzi, S.; Londero, A.P.; Biasioli, A.; Driul, L.; Kiesel, L.; Marchesoni, D. Menstrual abnormalities and predisposition to pregnancy-related hypertensive disorders: A retrospective study. Gynecol. Endocrinol. 2010, 26, 445–450. [Google Scholar] [CrossRef]
- Londero, A.P.; Bertozzi, S.; Visentin, S.; Fruscalzo, A.; Driul, L.; Marchesoni, D. High placental index and poor pregnancy outcomes: A retrospective study of 18,386 pregnancies. Gynecol. Endocrinol. 2013, 29, 666–669. [Google Scholar] [CrossRef]
- Visentin, S.; Londero, A.P.; Calanducci, M.; Grisan, E.; Bongiorno, M.C.; Marin, L.; Cosmi, E. Fetal Abdominal Aorta: Doppler and Structural Evaluation of Endothelial Function in Intrauterine Growth Restriction and Controls. Ultraschall Med. 2019, 40, 55–63. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Woo, V.G.; Hung, Y.Y.; Ritterman-Weintraub, M.L.; Painter, C.E.; Ramm, O. A Clinical Risk Model to Predict Obstetric Anal Sphincter Injuries in Laboring Patients. Female Pelvic Med. Reconstr. Surg. 2020, 26, 520–525. [Google Scholar] [CrossRef]
- Pretscher, J.; Schwenke, E.; Baier, F.; Kehl, S.; Schneider, M.; Stumpfe, F.M.; Schmid, M.; Beckmann, M.W.; Mayr, A.; Schild, R.; et al. Can Sonographic Fetal Biometry Predict Adverse Perinatal Outcome? Ultraschall Med. 2019, 40, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.; Falivene, C.; Briffa, K.; Thompson, J.; Henry, A. What is the total impact of an obstetric anal sphincter injury? An Australian retrospective study. Int. Urogynecol. J. 2020, 31, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Grobman, W.A.; Rice, M.M.; Reddy, U.M.; Tita, A.T.N.; Silver, R.M.; Mallett, G.; Hill, K.; Thom, E.A.; El-Sayed, Y.Y.; Perez-Delboy, A.; et al. Labor Induction versus Expectant Management in Low-Risk Nulliparous Women. N. Engl. J. Med. 2018, 379, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Grobman, W.A.; Caughey, A.B. Elective induction of labor at 39 weeks compared with expectant management: A meta-analysis of cohort studies. Am. J. Obs. Gynecol. 2019, 221, 304–310. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
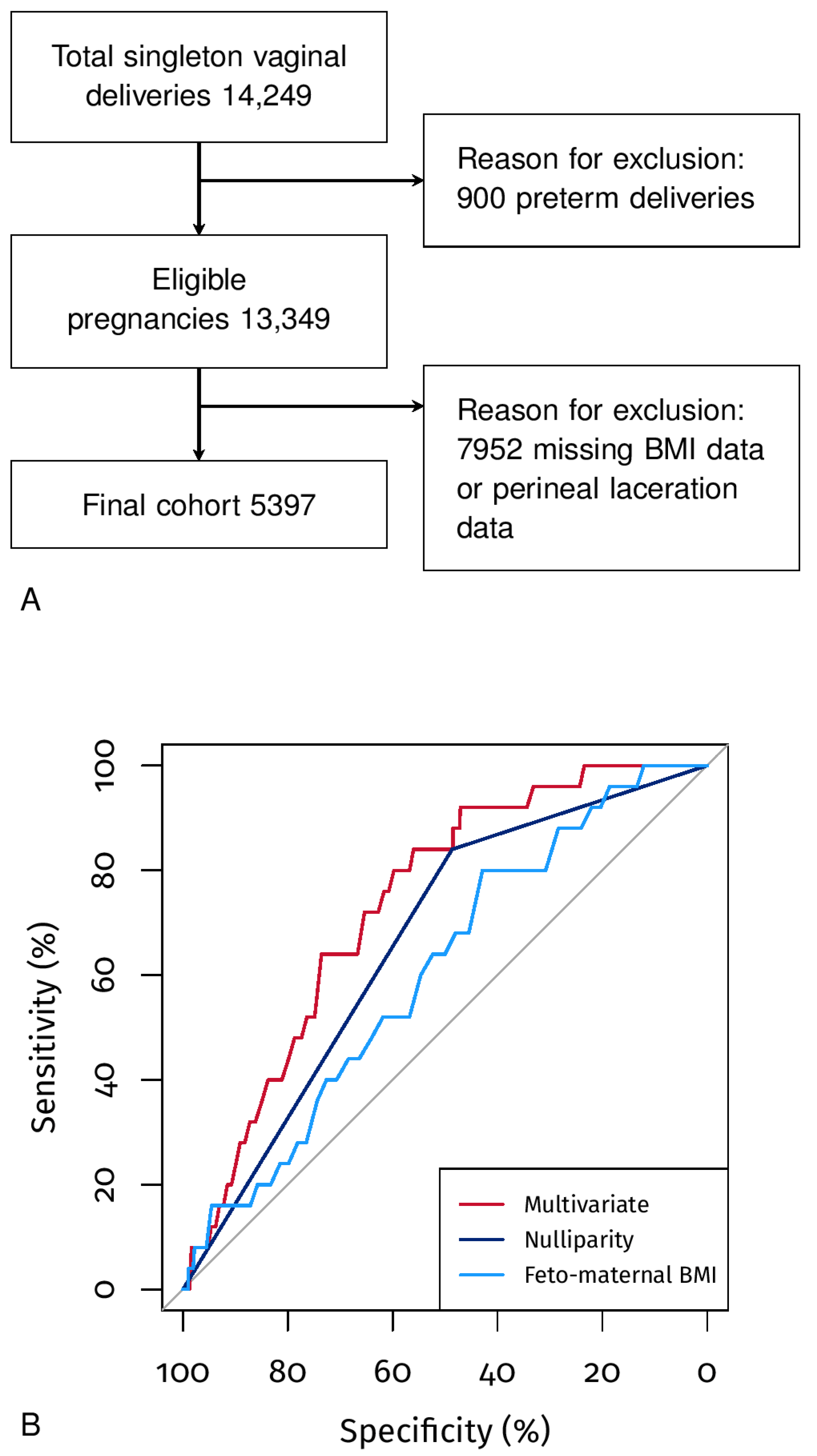
| Patient Characteristics | |
|---|---|
| Maternal age (years) | 32 (28–35) |
| Nulliparity | 51.49% (2779/5397) |
| Mother height (cm) | 165 (161–170) |
| Maternal pre-pregnancy BMI (kg/m2) | 22 (20–24) |
| Feto-maternal BMI (kg/m2) | 1.23 (1.12–1.34) |
| Gestational age at delivery (weeks) | 39 (39–40) |
| Macro-region of origin | |
| West Europe/Italy | 73% (3937/5393) |
| East Europe | 16.08% (867/5393) |
| Sub-Saharan Africa | 3.8% (205/5393) |
| Arabian countries | 3.49% (188/5393) |
| Asia | 2.48% (134/5393) |
| Other | 1.15% (62/5393) |
| HDP | 1.45% (76/5240) |
| Conception mode | |
| Spontaneous | 98.55% (5319/5397) |
| Ovulation induction/IUI | 0.43% (23/5397) |
| IVF/ICSI | 1.02% (55/5397) |
| Labor-induced/augmented | 28.66% (1504/5248) |
| Childbirth mode | |
| Spontaneous delivery | 89.09% (4808/5397) |
| Operative vaginal delivery | 10.91% (589/5397) |
| Neonatal characteristics | |
| Neonatal male sex | 49.32% (2662/5397) |
| 1st minute Apgar score | 9 (8–9) |
| 5th minute Apgar score | 9 (9–9) |
| Neonatal weight (grams) | 3375 (3110–3664) |
| Neonatal weight (MoM) | 1 (1–1) |
| Placental weight (grams) | 580 (510–655) |
| Neonatal length (cm) | 50 (49–51) |
| Neonatal head circumference (mm) | 345 (335–352) |
| SGA (<3rd centile) | 1.74% (94/5397) |
| SGA (<10th centile) | 7.93% (428/5397) |
| LGA (>90th centile) | 12.47% (673/5397) |
| LGA (>97th centile) | 4.98% (269/5397) |
| Neonatal CPR | 1.22% (66/5397) |
| NICU hospitalization | 1.04% (56/5397) |
| Controls (5372) | Perineal Tears Grade 3–4 (25) | p | |
|---|---|---|---|
| Patient characteristics | |||
| Maternal age (years) | 31.54 (±5.40) | 31.20 (±5.80) | 0.774 |
| Nulliparity | 51.34% (2758/5372) | 84.00% (21/25) | <0.05 |
| Maternal pre-pregnancy BMI (kg/m2) | 22.64 (±3.89) | 21.96 (±2.91) | 0.254 |
| Feto-maternal BMI (kg/m2) | 1.23 (±0.17) | 1.29 (±0.15) | <0.05 |
| Conception mode | |||
| Spontaneous | 98.57% (5295/5372) | 96.00% (24/25) | 0.283 |
| Ovulation induction/IUI | 0.43% (23/5372) | 0.00% (0/25) | 0.743 |
| IVF/ICSI | 1.01% (54/5372) | 4.00% (1/25) | 0.137 |
| Gestational age at delivery (weeks) | 39.00 (39.00–40.00) | 40.00 (39.00–41.00) | 0.071 |
| Macro-region of origin | |||
| West Europe/Italy | 73.03% (3921/5369) | 66.67% (16/24) | 0.492 |
| East Europe | 16.07% (863/5369) | 16.67% (4/24) | 1.000 |
| Sub-Saharan Africa | 3.78% (203/5369) | 8.33% (2/24) | 0.231 |
| Arabian countries | 3.48% (187/5369) | 4.17% (1/24) | 0.574 |
| Asia | 2.48% (133/5369) | 4.17% (1/24) | 0.454 |
| Other | 1.15% (62/5369) | 0.00% (0/24) | 1.000 |
| HDP | 1.41% (76/5372) | 0.00% (0/25) | 1.000 |
| Labor induction/augmentation | 28.61% (1495/5225) | 39.13% (9/23) | 0.266 |
| Vaginal operative delivery | 10.87% (584/5372) | 20.00% (5/25) | 0.144 |
| Neonatal characteristics | |||
| Neonatal male sex | 49.26% (2646/5372) | 64.00% (16/25) | 0.141 |
| 1st minute Apgar score | 9.00 (8.00–9.00) | 9.00 (8.00–9.00) | 0.658 |
| 5th minute Apgar score | 9.00 (9.00–9.00) | 9.00 (9.00–10.00) | 0.387 |
| Neonatal weight (grams) | 3375.00 (3106.00–3664.25) | 3515.00 (3380.00–3650.00) | 0.072 |
| Neonatal weight (MoM) | 1.01 (0.93–1.09) | 1.03 (0.98–1.07) | 0.383 |
| Placental weight (grams) | 580.00 (510.00–655.00) | 600.00 (535.00–641.00) | 0.642 |
| Neonatal length (cm) | 50.00 (49.00–51.00) | 50.00 (50.00–51.00) | 0.539 |
| Neonatal head circumference (mm) | 345.00 (335.00–352.00) | 349.00 (343.00–350.00) | 0.107 |
| SGA (<3rd centile) | 1.75% (94/5372) | 0.00% (0/25) | 1.000 |
| SGA (<10th centile) | 7.97% (428/5372) | 0.00% (0/25) | 0.258 |
| LGA (>90th centile) | 12.49% (671/5372) | 8.00% (2/25) | 0.761 |
| LGA (>97th centile) | 4.97% (267/5372) | 8.00% (2/25) | 0.356 |
| Neonatal CPR | 1.21% (65/5372) | 4.00% (1/25) | 0.265 |
| NICU hospitalization | 1.02% (55/5372) | 4.00% (1/25) | 0.230 |
| OR (CI.95) | p | AUC (CI.95) | |
|---|---|---|---|
| Nulliparity | 4.98 (1.71–14.52) | <0.05 | 66.33% (58.97–73.69) |
| Sub-Saharan Africa | 2.31 (0.54–9.91) | 0.258 | 52.28% (46.62–57.93) |
| Mother height (cm) | 0.98 (0.92–1.05) | 0.618 | 46.49% (35.31–57.67) |
| Pre-pregnancy BMI (kg/m2) | 0.95 (0.84–1.07) | 0.380 | 53.57% (42.83–64.31) |
| Pre-pregnancy weight (kg) | 0.98 (0.94–1.02) | 0.279 | 55.59% (45.88–65.31) |
| Feto-maternal BMI (kg/m2) | 5.37 (1.09–26.42) | <0.05 | 60.72% (50.64–70.81) |
| Neonatal weight (grams) | 1.00 (1.00–1.00) | 0.092 | 60.42% (51.73–69.11) |
| LGA (>97th centile) | 1.77 (0.41–7.58) | 0.443 | 51.79% (45.90–57.69) |
| Gestational age at delivery (weeks) | 1.39 (0.96–2.03) | 0.084 | 60.12% (48.23–72.00) |
| Neonatal head circumference (mm) | 1.02 (1.00–1.04) | 0.106 | 59.31% (49.54–69.07) |
| Vaginal operative delivery | 2.05 (0.77–5.48) | 0.153 | 54.56% (46.55–62.58) |
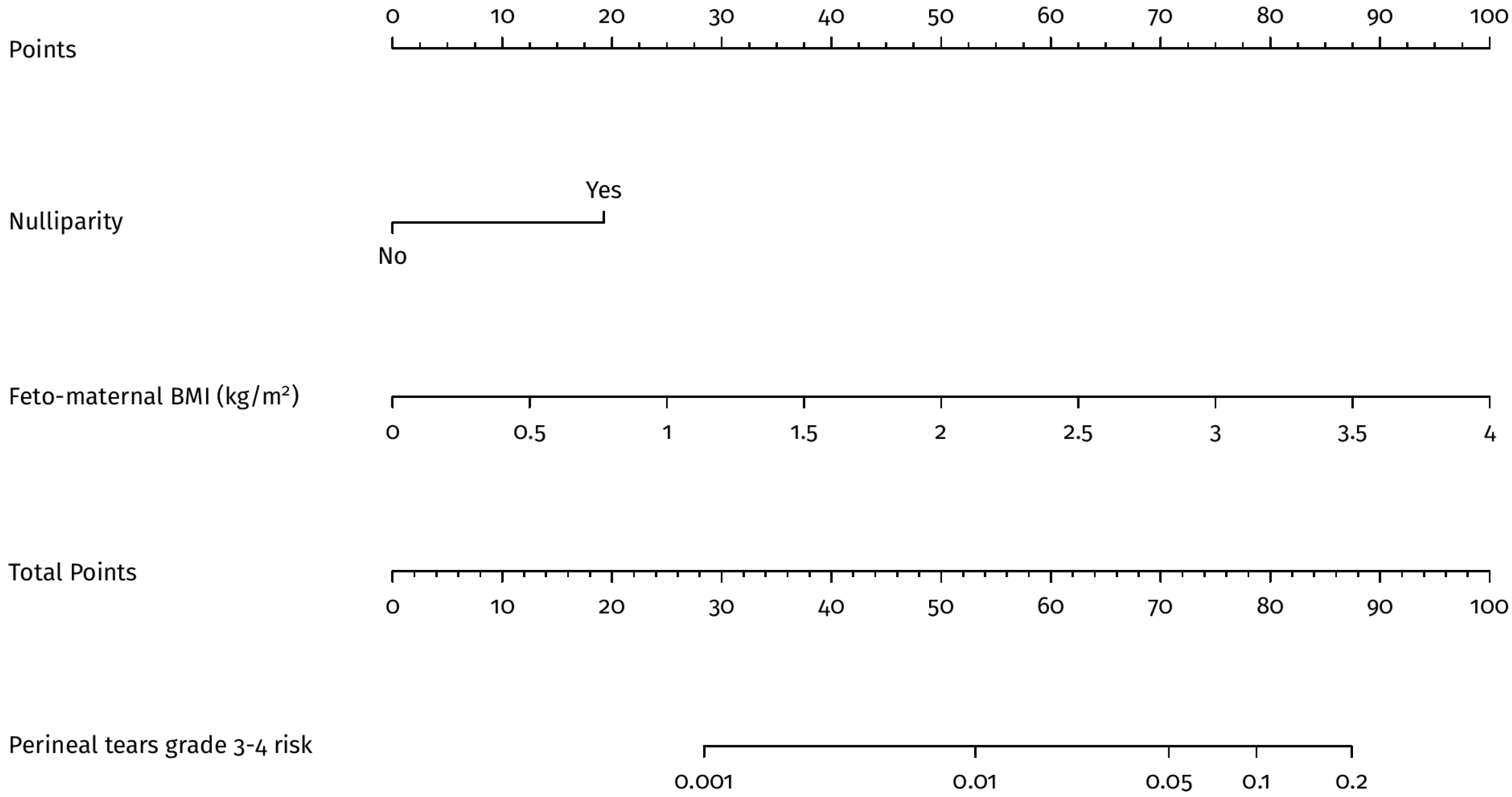
| Multivariate model (*) | 73.54% (65.65–81.42) | ||
| Nulliparity | 6.05 (2.00–18.35) | <0.05 | |
| Feto-maternal BMI (kg/m2) | 10.36 (2.12–50.6) | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fruscalzo, A.; Novak, A.; Somma, C.; Xholli, A.; Michelerio, V.; Prefumo, F.; Londero, A.P.; Cagnacci, A. Anthropometric Features and Third-Fourth Degree Perineal Tears. J. Pers. Med. 2023, 13, 545. https://doi.org/10.3390/jpm13030545
Fruscalzo A, Novak A, Somma C, Xholli A, Michelerio V, Prefumo F, Londero AP, Cagnacci A. Anthropometric Features and Third-Fourth Degree Perineal Tears. Journal of Personalized Medicine. 2023; 13(3):545. https://doi.org/10.3390/jpm13030545
Chicago/Turabian StyleFruscalzo, Arrigo, Alice Novak, Camilla Somma, Anjeza Xholli, Virginia Michelerio, Federico Prefumo, Ambrogio P. Londero, and Angelo Cagnacci. 2023. "Anthropometric Features and Third-Fourth Degree Perineal Tears" Journal of Personalized Medicine 13, no. 3: 545. https://doi.org/10.3390/jpm13030545
APA StyleFruscalzo, A., Novak, A., Somma, C., Xholli, A., Michelerio, V., Prefumo, F., Londero, A. P., & Cagnacci, A. (2023). Anthropometric Features and Third-Fourth Degree Perineal Tears. Journal of Personalized Medicine, 13(3), 545. https://doi.org/10.3390/jpm13030545