
A Systematic Review of Chest Imaging Findings in Long COVID Patients

 ,
,  and
and  on behalf of the P4O2 Consortium
on behalf of the P4O2 Consortium
Abstract
:1. Introduction
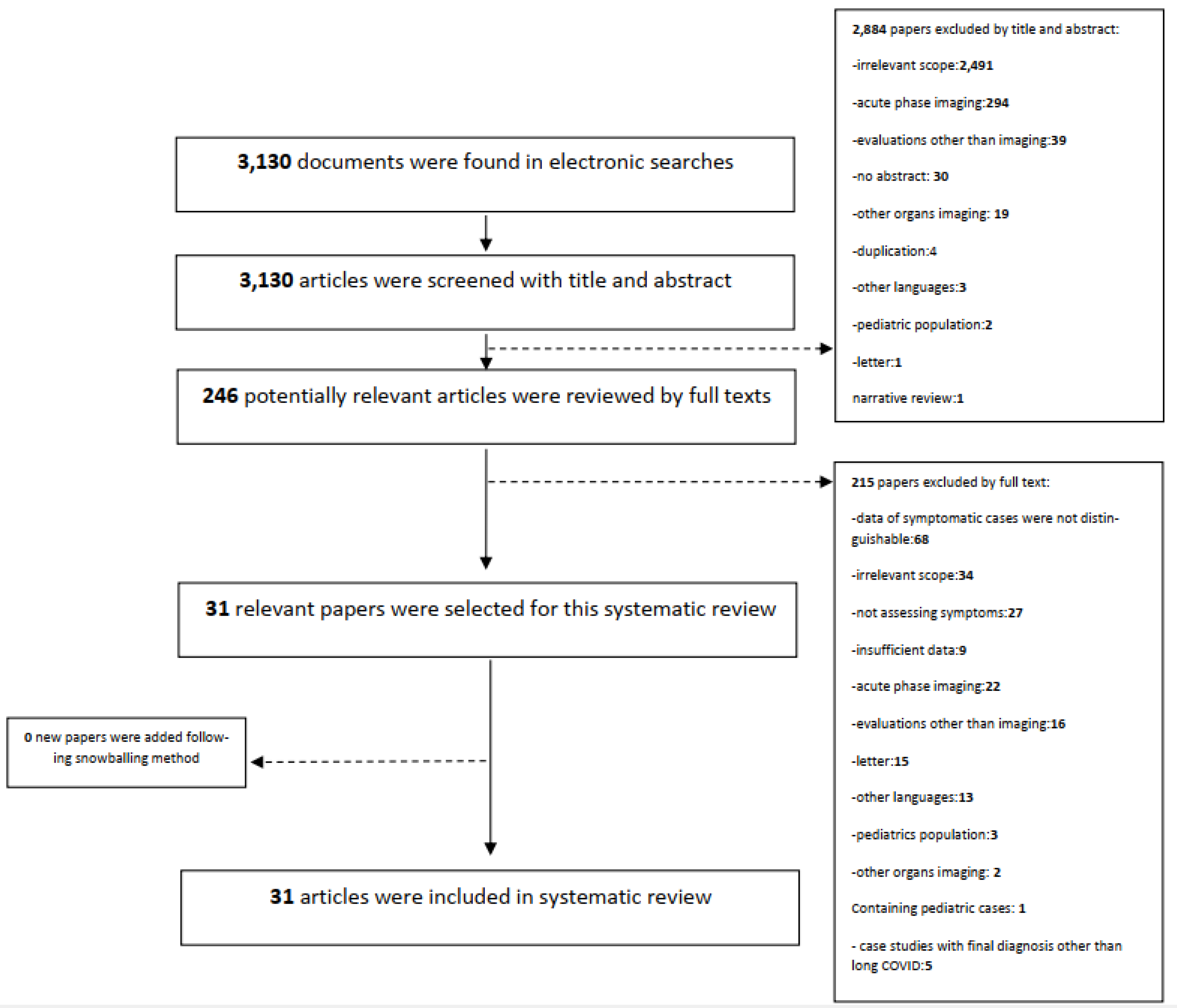
2. Methods and Materials
3. Results

{kind=link}
| First Author | Compared Modalities and Performing Days * | Imaging Modality | Imaging Finding |
|---|---|---|---|
| Sollini et al. [24] | 30 days | CT | Fibrotic change in 6 cases out of 10 population of study |
| PET | [18F]FDG lung uptake in 2 cases out of total 10 population of study | ||
| Sollini et al. [25] | 132 days | CT | bilateral lung abnormalities, as typically observed in recovered COVID-19 pneumonia, was detected in 4 cases out of 13 in the total population of study |
| PET | Mild [18F]FDG PET/CT uptake was detected in of Post-pneumonia lung abnormalities in 4 cases out of 13in the total population of study, and 2 other patients presented moderate/high [18F]FDG uptake in the lung, mediastinal lymph nodes, soft tissue, and breast tissue related to their comorbidities. | ||
| Garg et al. [28] | CT at 53 days and MRI at 55 days | CT | interlobular septal thickening, parenchymal band, Fibrotic change, bronchiectasis, bronchiolectasis, crazy-paving pattern |
| Garg et al. [28] | MRI | interlobular septal thickening, parenchymal band, Fibrotic change, bronchiectasis, bronchiolectasis, crazy-paving pattern | |
| Heiss et al. [29] | 97 days | CT | GGO, Consolidation |
| Heiss et al. [29] | MRI | GGO, Consolidation | |
| Tung-Chen et al. [30] | 56 days | CT | pleural thickening |
| Tung-Chen et al. [30] | USS | irregular pleural line in the right lateral area of the chest, which correlated with an area of pleural thickening on chest CT | |
| Tung-Chen et al. [30] | CT | GGO | |
| Tung-Chen et al. [30] | USS | a mild irregular pleural line and B-lines in the right anterior area of the chest, which correlated with ground-glass opacities on chest CT with no abnormal findings in the pleura. | |
| Tung-Chen et al. [30] | CT | fibrotic change | |
| Tung-Chen et al. [30] | USS | a marked irregular pleural line and multiple B lines, especially in the posterior inferior area of the chest, which correlated with fibrotic changes on chest CT | |
| Alhiyari et al. [32] | 130 days | CXR | air space opacity |
| Alhiyari et al. [32] | CT | GGO, bronchiectasis, interlobular septal thickening, reticulation, honeycomb-like appearance, interstitial pneumonia pattern | |
| Hamad et al. [33] | CT at 35 days and CXR at 36 days | CXR | pneumothorax, air space opacity |
| Hamad et al. [33] | CT | pleural effusion, atelectasis, pulmonary edema, cystic airspace | |
| Aesif et al. [31] | CT at 59 days and CXR at 122 days | CT | pneumothorax, Consolidation |
| Aesif et al. [31] | CXR | complete opacification, volume loss | |
| Malik et al. [34] | 42 days | CXR | Consolidation |
| Malik et al. [34] | CT | GGO, Fibrotic change, bronchiectasis, architectural distortion, linear scaring, airspace disease, COVID pneumonia |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grover, S.; Dua, D.; Sahoo, S.; Mehra, A.; Nehra, R.; Chakrabarti, S. Why all COVID-19 hospitals should have mental health professionals: The importance of mental health in a worldwide crisis! Asian J. Psychiatry 2020, 51, 102147. [Google Scholar] [CrossRef] [PubMed]
- Jara, A.; Undurraga, E.A.; González, C.; Paredes, F.; Fontecilla, T.; Jara, G.; Pizarro, A.; Acevedo, J.; Leo, K.; Leon, F.; et al. Effectiveness of an inacti-vated SARS-CoV-2 vaccine in Chile. N. Engl. J. Med. 2021, 385, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed]
- WHO. 2022. Available online: https://covid19.who.int/ (accessed on 23 December 2022).
- Harb, J.G.; Noureldine, H.; Chedid, G.; Eldine, M.N.; Abdallah, D.A.; Chedid, N.F.; Nour-Eldine, W. SARS, MERS and COVID-19: Clinical manifestations and organ-system complications: A mini review. Pathog. Dis. 2020, 78, ftaa033. [Google Scholar] [CrossRef] [PubMed]
- Louis, T.J.; Qasem, A.; Abdelli, L.S.; Naser, S.A. Extra-Pulmonary Complications in SARS-CoV-2 Infection: A Comprehensive Multi Organ-System Review. Microorganisms 2022, 10, 153. [Google Scholar] [CrossRef]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: From an acute to chronic disease? Potential long-term health consequences. Crit. Rev. Clin. Lab. Sci. 2021, 58, 297–310. [Google Scholar] [CrossRef]
- Lancet, T. Facing up to long COVID. Lancet 2020, 396, 1861. [Google Scholar] [CrossRef]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 869–875. [Google Scholar] [CrossRef]
- Stephenson, T.; Shafran, R.; De Stavola, B.; Rojas, N.; Aiano, F.; Amin-Chowdhury, Z.; McOwat, K.; Simmons, R.; Zavala, M.; Consortium, C.; et al. Long COVID and the mental and physical health of children and young people: National matched cohort study protocol (the CLoCk study). BMJ Open 2021, 11, e052838. [Google Scholar] [CrossRef]
- Kamau, C. Risk of Debilitating Fatigue after COVID-19 Lasting Years and Implications for the UK Workforce: Evidence Report for the House of Lords Select Committee on Risk Assessment and Risk Planning; House of Lords Risk Assessment and Risk Planning Committee Publications. 2021. Available online: https://eprints.bbk.ac.uk/id/eprint/44404/ (accessed on 23 December 2022).
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Siddiqui, S.; Brightling, C.E. Pathological disease in the lung periphery after acute COVID-19. Lancet Respir. Med. 2021, 9, 1089–1090. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; CAo, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Martini, K.; Larici, A.R.; Revel, M.P.; Ghaye, B.; Sverzellati, N.; Parkar, A.P.; Snoeckx, A.; Screaton, N.; Biederer, J.; Prosch, H.; et al. COVID-19 pneumonia imaging follow-up: When and how? A proposition from ESTI and ESR. Eur. Radiol. 2022, 32, 2639–2649. [Google Scholar] [CrossRef] [PubMed]
- Nikhra, V. Living with ‘Long COVID-19’: The long-term complications and sequelae. Int. J. Clin. Virol. 2021, 5, 11–17. [Google Scholar]
- Xie, L.; Fan, B.; Xiao, Y.; Tian, Q.; Chen, L.; Zhao, H. Dynamic changes of serum SARS-coronavirus IgG, pulmonary function and radiography in patients recovering from SARS after hospital discharge. Respir. Res. 2005, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.S.; Wong, K.T.; Ko, F.W.; Tam, L.S.; Chan, D.P.; Woo, J.; Sung, J.J. The 1-year impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and quality of life in a cohort of survivors. Chest 2005, 128, 2247–2261. [Google Scholar] [CrossRef] [PubMed]
- Armange, L.; Bénézit, F.; Picard, L.; Pronier, C.; Guillot, S.; Lentz, P.A.; Carré, F.; Tattevin, P.; Revest, M. Prevalence and characteristics of persistent symptoms after non-severe COVID-19: A prospective cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2421–2425. [Google Scholar] [CrossRef]
- Bai, Y.; Xu, J.; Chen, L.; Fu, C.; Kang, Y.; Zhang, W.; Fakhri, G.E.; Gu, J.; Shao, F.; Wang, M. Inflammatory response in lungs and extrapulmonary sites detected by [18F] fluorodeoxyglucose PET/CT in convalescing COVID-19 patients tested negative for coronavirus. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2531–2542. [Google Scholar] [CrossRef]
- Cesarone, M.R.; Hu, S.; Belcaro, G.; Cornelli, U.; Feragalli, B.; Corsi, M.; Bombardelli, E.; Cotellese, R.; Hosoi, M.; Rosenkvist, L. Pycno-genol®-Centellicum® supplementation improves lung fibrosis and Post-COVID-19 lung healing. Minerva Med. 2021, 113, 135–140. [Google Scholar] [PubMed]
- Gaspardone, C.; Meloni, C.; Preda, A.; Romagnolo, D.; Brugliera, L.; Castellazzi, P.; Tettamanti, A.; Conte, C.; Secchi, A.; Maranta, F.; et al. Lung ultra-sound in COVID-19 a role beyond the acute phase? J. Ultrasound Med. 2021, 40, 503–511. [Google Scholar] [CrossRef]
- Rinaldo, R.F.; Mondoni, M.; Parazzini, E.M.; Baccelli, A.; Pitari, F.; Brambilla, E.; Luraschi, S.; Balbi, M.; Guazzi, M.; Di Marco, F.; et al. Severity does not impact on exercise capacity in COVID-19 survivors. Respir. Med. 2021, 187, 106577. [Google Scholar] [CrossRef]
- Sollini, M.; Ciccarelli, M.; Cecconi, M.; Aghemo, A.; Morelli, P.; Gelardi, F.; Chiti, A. Vasculitis changes in COVID-19 survivors with persistent symptoms: An [18F]FDG-PET/CT study. Eur. J. Nucl. Med. 2021, 48, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Morbelli, S.; Ciccarelli, M.; Cecconi, M.; Aghemo, A.; Morelli, P.; Chiola, S.; Gelardi, F.; Chiti, A. Long COVID hallmarks on [18F]FDG-PET/CT: A case-control study. Eur. J. Nucl. Med. 2021, 48, 3187–3197. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Xi, X.; Min, X.; Feng, Z.; Li, B.; Cai, W.; Fan, C.; Wang, L.; Xia, L. Long-term chest CT follow-up in COVID-19 Survivors: 102–361 days after onset. Ann. Transl. Med. 2021, 9, 1231. [Google Scholar] [CrossRef] [PubMed]
- Miwa, M.; Nakajima, M.; Kaszynski, R.H.; Hamada, S.; Ando, H.; Nakano, T.; Shirokawa, M.; Goto, H. Abnormal pulmonary function and imaging studies in critical COVID-19 survivors at 100 days after the onset of symptoms. Respir. Investig. 2021, 59, 614–621. [Google Scholar] [CrossRef]
- Garg, M.; Prabhakar, N.; Dhooria, S.; Lamichhane, S. Magnetic resonance imaging (MRI) chest in post-COVID-19 pneumonia. Lung India 2021, 38, 498. [Google Scholar] [CrossRef]
- Heiss, R.; Grodzki, D.M.; Horger, W.; Uder, M.; Nagel, A.M.; Bickelhaupt, S. High-performance low field MRI enables visualization of persistent pulmonary damage after COVID-19. Magn. Reson. Imaging 2020, 76, 49–51. [Google Scholar] [CrossRef]
- Tung-Chen, Y.; De Gracia, M.M.; Parra-Gordo, M.L.; Díez-Tascón, A.; Agudo-Fernández, S.; Ossaba-Vélez, S. Usefulness of Lung Ultrasound Follow-up in Patients Who Have Recovered from Coronavirus Disease 2019. J. Ultrasound Med. 2021, 40, 1971–1974. [Google Scholar] [CrossRef]
- Aesif, S.W.; Bribriesco, A.C.; Yadav, R.; Nugent, S.L.; Zubkus, D.; Tan, C.D.; Mehta, A.C.; Mukhopadhyay, S. Pulmonary Pathology of COVID-19 Following 8 Weeks to 4 Months of Severe Disease: A Report of Three Cases, Including One With Bilateral Lung Transplantation. Am. J. Clin. Pathol. 2021, 155, 506–514. [Google Scholar] [CrossRef]
- Alhiyari, M.A.; Ata, F.; Alghizzawi, M.I.; Bilal, A.B.I.; Abdulhadi, A.S.; Yousaf, Z. Post COVID-19 fibrosis, an emerging complicationof SARS-CoV-2 infection. IDCases 2021, 23, e01041. [Google Scholar] [CrossRef]
- Hamad, A.-M.M.; El-Saka, H.A. Post COVID-19 large pneumatocele: Clinical and pathological perspectives. Interact. Cardiovasc. Thorac. Surg. 2021, 33, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Malik, B.; Abdelazeem, B.; Ghatol, A. Pulmonary Fibrosis after COVID-19 Pneumonia. Cureus 2021, 13, e13923. [Google Scholar] [CrossRef] [PubMed]
- Garvey, C.J.; Hanlon, R. Computed tomography in clinical practice. Bmj 2002, 324, 1077–1080. [Google Scholar] [CrossRef] [PubMed]
- Moro, F.; Beneduce, G.; Buonsenso, D.; Landolfo, C.; Mascilini, F.; Scambia, G.; Testa, A.C. Lung ultrasound in COVID-19 pregnancies: A literature review. Sechenov. Med. J. 2021, 12, 26–34. [Google Scholar] [CrossRef]
- Peixoto, A.O.; Costa, R.M.; Uzun, R.; Fraga, A.D.M.A.; Ribeiro, J.D.; Marson, F.L. Applicability of lung ultra-sound in COVID-19 diagnosis and evaluation of the disease progression: A systematic review. Pulmonology 2021, 27, 529–562. [Google Scholar] [CrossRef]
- Caiulo, V.A.; Gargani, L.; Caiulo, S.; Fisicaro, A.; Moramarco, F.; Latini, G.; Picano, E.; Mele, G. Lung ultrasound characteristics of community-acquired pneumonia in hospitalized children. Pediatr. Pulmonol. 2013, 48, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, G.; De Michele, L.; De Ceglie, M.; Pierucci, P.; Mirabile, A.; Vita, M.; Palmieri, V.O.; Carpagnano, G.E.; Scardapane, A.; D’Agostino, C. Lung ultrasonography for long-term follow-up of COVID-19 survivors compared to chest CT scan. Respir. Med. 2021, 181, 106384. [Google Scholar] [CrossRef]
- Dehbozorgi, A.; Mousavi-Roknabadi, R.S.; Hosseini-Marvast, S.R.; Sharifi, M.; Sadegh, R.; Farahmand, F.; Damghani, F. Correction to: Diagnosing Skull fracture in children with closed head injury using point-of-care ultrasound vs computed tomography scan. Eur. J. Pediatr. 2020, 180, 485–486. [Google Scholar] [CrossRef]
- Kubota, R.; Yamada, S.; Kubota, K.; Ishiwata, K.; Tamahashi, N.; Ido, T. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: High accumulation in macrophages and granulation tissues studied by microautoradiography. J. Nucl. Med. 1992, 33, 1972–1980. [Google Scholar]
- Geboes, K. From inflammation to lesion. Acta Gastro-Enterol. Belg. 1994, 57, 273–284. [Google Scholar]
- Pezzotti, W. Chest X-ray interpretation: Not just black and white. Nursing2020 2014, 44, 40–47. [Google Scholar] [CrossRef]
- Retson, T.A.; Hasenstab, K.A.; Kligerman, S.J.; Jacobs, K.E.; Yen, A.C.; Brouha, S.S.; Hahn, L.D.; Hsiao, A. Reader perceptions and impact of AI on CT assessment of air trapping. Radiol. Artif. Intell. 2021, 4, e210160. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.L.; Villacreses, R.; Nagpal, P.; Guo, J.; Pezzulo, A.A.; Thurman, A.L.; Hamzeh, N.Y.; Blount, R.J.; Fortis, S.; Hoffman, E.A.; et al. Small airways disease is a post-acute sequelae of SARS-CoV-2 infection. medRxiv 2021. [Google Scholar] [CrossRef]
- Cho, J.L.; Villacreses, R.; Nagpal, P.; Guo, J.; Pezzulo, A.A.; Thurman, A.L.; Hamzeh, N.Y.; Blount, R.J.; Fortis, S.; Hoffman, E.A.; et al. Quantitative chest CT assessment of small airways disease in post-acute SARS-CoV-2 infection. Radiology 2022, 304, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Goldberg-Stein, S.; Chernyak, V. Adding value in radiology reporting. J. Am. Coll. Radiol. 2019, 16, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.V.; McInnes, M.; Jacob, B.; Kumar, D.; Soman, D.K.; Subair, H.S.V.; Mahajan, P.S.; Shah, M.A.H.; Sabawi, M.A.S.; Al-Heidous, M. Diagnostic accuracy and inter-observer agreement with the CO-RADS lexicon for CT chest reporting in COVID-19. Emerg. Radiol. 2021, 28, 1045–1054. [Google Scholar] [CrossRef]
- Scelfo, C.; Fontana, M.; Casalini, E.; Menzella, F.; Piro, R.; Zerbini, A.; Spaggiari, L.; Ghidorsi, L.; Ghidoni, G.; Facciolongo, N.C. A dangerous conse-quence of the recent pandemic: Early lung fibrosis following Covid-19 pneumonia—Case reports. Ther. Clin. Risk Manag. 2020, 16, 1039. [Google Scholar] [CrossRef] [PubMed]
- Lago, V.C.; Prudente, R.A.; Luzia, D.A.; Franco, E.T.; Cezare, T.J.; Peralta, A.; Ferreira, E.V.M.; Albuquerque, A.L.P.; Okoshi, M.P.; Baldi, B.G.; et al. Persistent interstitial lung abnormalities in post-COVID-19 patients: A case series. J. Venom. Anim. Toxins Incl. Trop. Dis. 2021, 27, e20200157. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.K.; Kumar, S.; Sahay, N. Post-COVID-19 pulmonary fibrosis: A case series and review of literature. J. Fam. Med. Prim. Care 2021, 10, 2028–2031. [Google Scholar] [CrossRef]
- Singh, A.K.; Kumar, O.P.; Bansal, P.; Margekar, S.L.; Aggarwal, R.; Ghotekar, L.R.; Gupta, A. Post-COVID interstitial lung disease—The looming epidemic. J. Assoc. Physicians India 2021, 69, 11–12. [Google Scholar]
- Abdelnour, L.H.; Abdalla, M.E. Progression of CXR features on a COVID-19 survivor. Idcases 2020, 21, e00834. [Google Scholar] [CrossRef]
- Betelli, M.; De Stefano, F.; Tedeschi, A. Late worsening of COVID-19 pneumonia: Successful treatment with ruxolitinib and steroid. Eur. J. Case Rep. Intern. Med. 2020, 7, 001938. [Google Scholar]
- Horii, T.; Fujioka, T.; Takahashi, M.; Mori, M.; Tsuchiya, J.; Yamaga, E.; Yamada, H.; Kimura, M.; Kishino, M.; Tateishi, U. Late-onset pneumothorax in a COVID-19 patient treated with ventilation and ECMO: A case report and literature review. Radiol. Case Rep. 2020, 15, 2560–2564. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zhou, J.; Zhao, J. Recurrent pneumonia in a patient with new coronavirus infection after discharge from hospital for insufficient antibody production: A case report. BMC Infect. Dis. 2020, 20, 500. [Google Scholar] [CrossRef]
- Aissaoui, H.; Eskenazi, A.; Suteau, V.; Adenis, A.; Alsibai, K.D. Case Report: Potential Role of Corticosteroids in the Management of Post-COVID-19 Pneumonia. Front. Med. 2021, 8, 686806. [Google Scholar] [CrossRef] [PubMed]
- Dayco, J.S.; El-Reda, Z.; Sumbal, N.; Alhusain, R.; Raheem, S. Perpetually Positive: Post-COVID Interstitial Lung Disease in an Immunocompromised Patient With Diffuse Large B-cell Lymphoma. J. Investig. Med. High Impact Case Rep. 2021, 9, 23247096211041207. [Google Scholar] [CrossRef]
- Liu, F.; Cai, Z.B.; Huang, J.S.; Niu, H.Y.; Yu, W.Y.; Zhang, Y.; Yan, T.-B.; Chen, C.; Liu, Y.; Xu, A.-F. Repeated COVID-19 relapse during post-discharge surveillance with viral shedding lasting for 67 days in a recovered patient infected with SARS-CoV-2. J. Microbiol. Immunol. Infect. 2021, 54, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Mazzolini, M.; Monari, M.; Angeletti, G.; Dalpiaz, G.; Rocca, A. Fatal pulmonary fibrosis complicating COVID-19 infection in preexistent emphysema. Radiol. Case Rep. 2020, 16, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Mitrani, M.I.; Bellio, M.A.; Meglin, A.; Khan, A.; Xu, X.; Haskell, G.; Arango, A.; Shapiro, G.C. Treatment of a COVID-19 long hauler with an amniotic fluid-derived extracellular vesicle biologic. Respir. Med. Case Rep. 2021, 34, 101502. [Google Scholar] [CrossRef] [PubMed]
- Susanto, A.D.; Triyoga, P.A.; Isbaniah, F.; Fairuz, A.; Cendikiawan, H.; Zaron, F.; Aryanti, I.; Irbah, S.N.; Hidayat, M. Lung Fibrosis Sequelae After Recovery from COVID-19 Infection. J. Infect. Dev. Ctries. 2021, 15, 360–365. [Google Scholar] [CrossRef]
- Zhu, M.; Chen, D.; Zhu, Y.; Xiong, X.; Ding, Y.; Guo, F.; Zhu, M.; Zhou, J. Long-term sero-positivity for IgG, sequelae of respiratory symptoms, and abundance of malformed sperms in a patient recovered from severe COVID-19. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Boehm, A.; Luger, A.K.; Schmitz, K.; Cima, K.; Patscheider, D.H.; Augustin, F.; Jakob, L.M.; Obermayer, A.; Weiss, G.; Stoiber, W.; et al. A spark of hope: Histopathological and functional recovery after critical COVID-19. Infection 2021, 50, 263–267. [Google Scholar] [CrossRef] [PubMed]

| First Author/Group of Articles | All Study Participants | Long-COVID Patients Who Underwent Imaging | Imaging Modality | Mean Age | Male | Study Design |
|---|---|---|---|---|---|---|
| Original articles | 761 | 309 | CT, USS, CXR, MRI | 59.7 | 147 (61%) | Cohort/Case-control |
| Armange et al. [19] | 214 | 23 | CT | 44 | 5(21.7%) | Cohort |
| Bai et al. [20] | 7 | 4 | CT | 62.75 | 2 (50%) | Case-control |
| Cesarone et al. [21] | 18 | 18 | CXR | 56.9 | 10(55.5%) | Cohort |
| Gaspardone et al. [22] | 70 | 70 | USS | 68 | 48 (68.5%) | Cohort |
| Rinaldo et al. [23] | 75 | 68 | CT | NM | NM | Cohort |
| Sollini et al. [24] | 101 | 10 | CT & PET | 58 | 7 (70%) | Cohort |
| Sollini et al. [25] | 13 | 13 | CT & PET | 54 | 8 (61.5%) | Case-control |
| Yin et al. [26] | 337 | 91 | CT | 58.68 | 57 (62.6%) | Cohort |
| Miwa et al. [27] * | 17 | 12 | CT | 63.25 | 10 (83.3%) | Cohort |
| Case reports/series | 33 | 33 | CT, USS, CXR | 57.5 | 23 (71%) | Case report/case series |
| Category of Abnormality | Frequency (N) | Specified Abnormality | Frequency (N) |
|---|---|---|---|
| Interstitial (fibrotic) abnormalities | 105 | Reticulation | 78 |
| Architectural distortion | 2 | ||
| Honeycomb-like appearance | 2 | ||
| Linear scarring | 1 | ||
| Fibrotic change | 14 | ||
| Parenchymal band | 2 | ||
| Fibrous stripe | 3 | ||
| Scissural deformation | 1 | ||
| Interstitial thickening | 2 | ||
| Interlobular septal thickening | 2 | ||
| Pulmonary edema | 8 | ||
| Interstitial pneumonia pattern | 1 | ||
| Pleural abnormalities | 7 | Pneumothorax | 4 |
| Pleural effusion | 6 | ||
| Hemopneumothorax | 1 | ||
| Pleural thickening | 1 | ||
| Airway abnormalities | 28 | Bronchiectasis | 4 |
| Bronchiolectasis | 25 | ||
| Other parenchymal abnormalities | 112 | Ground-glass opacity | 93 |
| Consolidation | 22 | ||
| Complete opacification | 1 | ||
| Airspace opacity | 4 | ||
| Reticular opacity | 5 | ||
| Aeriation | 1 | ||
| Volume loss of lung lobe | 7 | ||
| Emphysematous changes | 4 | ||
| Atelectasis | 1 | ||
| Crazy paving pattern | 16 |
| First Author | Evaluation Setting | Evaluation Time (days) | Imaging Modality | Imaging Finding | Positive FU Imaging | Negative FU Imaging | Category Interstitial (Fibrotic) | Category Pleural | Category Airway | Category Other Parenchymal |
|---|---|---|---|---|---|---|---|---|---|---|
| Armange et al. [19] | Follow-up Assessment | 42 | CT | GGO | 4 | 19 | 0 | 0 | 0 | 4 |
| Bai et al. [20] | Follow-up assessment | 40 | CT | Consolidation, fibrous stripe | 4 | 0 | 3 | 0 | 0 | 1 |
| Cesarone et al. [21] | Follow-up assessment | 60 | CXR | pulmonary edema | 7 | 11 | 7 | 0 | 0 | 0 |
| Gaspardone et al. [22] * | prolonged hsp. | 43 | USS | NA | NA | NA | NA | NA | NA | NA |
| Rinaldo et al. [23] | Follow-up assessment | 111 | CT | NM | 43 | 25 | NA | NA | NA | NA |
| Sollini et al. [24] | Follow-up assessment | 30 | CT, PET | Fibrotic change | 6 | 4 | 6 | 0 | 0 | 0 |
| Sollini et al. [25] | Follow-up assessment | 132 | CT, PET | in 4 out of 13 long COVID patients, CT images demonstrated bilateral lung abnormalities—as typically observed in recovered COVID-19 pneumonia—presenting mild [18F]FDG uptake, 2 patients presented moderate/high [18F]FDG uptake in the lung, mediastinal lymph nodes, soft tissue, and breast tissue related to their comorbidities. | 6 | 7 | NA | NA | NA | NA |
| Yin et al. [26] | Follow-up assessment | 203 | CT | GGO, Consolidation, bronchiectasis, crazy-paving pattern, reticulation | NM | NM | 76 | 7 | 22 | 68 |
| Miwa et al. [27] | Follow-up assessment | 100 | CT | GGO, Consolidation | 12 | 0 | 0 | 0 | 0 | 12 |
| Total | --- | 90 | CT/PET/USS | --- | 82 | 66 | 85 | 7 | 22 | 85 |
| Evaluation Setting | Study Design | Positive FU Imaging | Interstitial (Fibrotic) Abnormalities | Pleural Abnormalities | Airway Abnormalities | Other Parenchymal Abnormalities |
|---|---|---|---|---|---|---|
| Follow-up evaluation | Cohort/Case-control/Case-report/Case-series | 91/157 (57.9%) | 95/167 (56.9%) | 7/167 (4.2%) | 24/167 (14.4%) | 94/167(56.3%) |
| Re-admission | Case-report/Case-series | 10/10 (100%) | 3/10 (25.0%) | 4/10 (25.0%) | 1/10 (8.3%) | 8/10 (75.0%) |
| Prolonged hospitalization | Case-report/Case-series | 14/14 (100%) | 7/13 (53.8%) | 3/13 (23.1%) | 3/13 (23.1%) | 10/13 (76.9%) |
| First Author | Positive FU Imaging | Negative FU Imaging | Category Interstitial (Fibrotic) Abnormalities | Category Pleural Abnormalities | Category Airway Abnormalities | Category Other Parenchymal Abnormalities |
|---|---|---|---|---|---|---|
| Armange et al. [19] | 4 | 19 | 0 | 0 | 0 | 4 |
| Bai et al. [20] | 4 | 0 | 3 | 0 | 0 | 1 |
| Cesarone et al. [21] | 7 | 11 | 7 | 0 | 0 | 0 |
| Rinaldo et al. [23] | 43 | 25 | NA | NA | NA | NA |
| Sollini et al. [24] | 6 | 4 | 6 | 0 | 0 | 0 |
| Sollin et al. [25] | 6 | 7 | NA | NA | NA | NA |
| Yin et al. [26] | NM | NM | 76 | 0 | 22 | 68 |
| Miwa et al. [27] | 12 | 0 | 0 | 0 | 0 | 12 |
| Total | 82/148 (55.4%) | 66/148 (44.6%) | 92/158 (58.2%) | 0/158 (0.0%) | 22/158 (14.0%) | 85/158 (53.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazdar, S.; Kwee, A.K.A.L.; Houweling, L.; de Wit-van Wijck, Y.; Mohamed Hoesein, F.A.A.; Downward, G.S.; Nossent, E.J.; Maitland-van der Zee, A.H., on behalf of the P4O2 Consortium. A Systematic Review of Chest Imaging Findings in Long COVID Patients. J. Pers. Med. 2023, 13, 282. https://doi.org/10.3390/jpm13020282
Bazdar S, Kwee AKAL, Houweling L, de Wit-van Wijck Y, Mohamed Hoesein FAA, Downward GS, Nossent EJ, Maitland-van der Zee AH on behalf of the P4O2 Consortium. A Systematic Review of Chest Imaging Findings in Long COVID Patients. Journal of Personalized Medicine. 2023; 13(2):282. https://doi.org/10.3390/jpm13020282
Chicago/Turabian StyleBazdar, Somayeh, Anastasia K. A. L. Kwee, Laura Houweling, Yolanda de Wit-van Wijck, Firdaus A. A. Mohamed Hoesein, George S. Downward, Esther J. Nossent, and Anke H. Maitland-van der Zee on behalf of the P4O2 Consortium. 2023. "A Systematic Review of Chest Imaging Findings in Long COVID Patients" Journal of Personalized Medicine 13, no. 2: 282. https://doi.org/10.3390/jpm13020282
APA StyleBazdar, S., Kwee, A. K. A. L., Houweling, L., de Wit-van Wijck, Y., Mohamed Hoesein, F. A. A., Downward, G. S., Nossent, E. J., & Maitland-van der Zee, A. H., on behalf of the P4O2 Consortium. (2023). A Systematic Review of Chest Imaging Findings in Long COVID Patients. Journal of Personalized Medicine, 13(2), 282. https://doi.org/10.3390/jpm13020282