
Clinical Cancer and Direct-to-Consumer Genetic Test Result-Sharing Behavior: Findings from HINTS 2020


Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Genetic Test Result Sharing
2.1.2. Clinical Factors
2.1.3. Risk Perceptions
2.1.4. Cancer Beliefs
2.1.5. Genetic Self-Efficacy
2.2. Statistical Analysis
3. Results
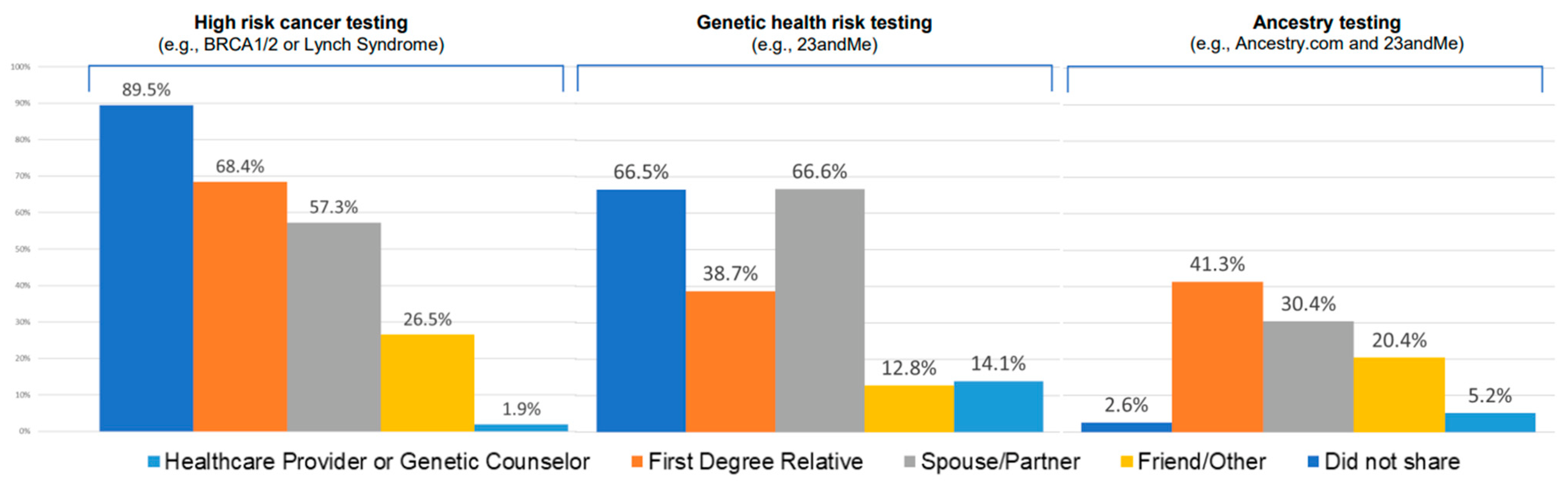
3.1. High-Risk Cancer Genetic Test Results
3.2. Genetic Health Risk Testing
3.3. Ancestry Testing
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valencia, O.M.; Samuel, S.E.; Viscusi, R.K.; Riall, T.S.; Neumayer, L.A.; Aziz, H. The Role of Genetic Testing in Patients With Breast Cancer: A Review. JAMA Surg. 2017, 152, 589–594. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.J.; Nabel, E.G. Genomics of Cardiovascular Disease. N. Engl. J. Med. 2011, 365, 2098–2109. [Google Scholar] [CrossRef] [PubMed]
- Shickh, S.; Mighton, C.; Uleryk, E.; Pechlivanoglou, P.; Bombard, Y. The clinical utility of exome and genome sequencing across clinical indications: A systematic review. Hum. Genet. 2021, 140, 1403–1416. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.C.; Dotson, W.D.; DeVore, C.S.; Bednar, E.M.; Bowen, D.J.; Ganiats, T.G.; Green, R.F.; Hurst, G.M.; Philp, A.R.; Ricker, C.N.; et al. Delivery Of Cascade Screening For Hereditary Conditions: A Scoping Review Of The Literature. Health Aff. 2018, 37, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2. 2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Turbitt, E.; Roberts, M.; A Ferrer, R.; Taber, J.M.; Lewis, K.L.; Biesecker, L.G.; Biesecker, B.B.; Klein, W.M. Intentions to share exome sequencing results with family members: Exploring spousal beliefs and attitudes. Eur. J. Hum. Genet. 2018, 26, 735–739. [Google Scholar] [CrossRef]
- Majumder, M.A.; Guerrini, C.J.; McGuire, A.L. Direct-to-Consumer Genetic Testing: Value and Risk. Annu. Rev. Med. 2021, 72, 151–166. [Google Scholar] [CrossRef]
- A, R. More than 26 Million People Have Taken an At-Home Ancestry Test. 2019. Available online: https://www.technologyreview.com/2019/02/11/103446/more-than-26-million-people-have-taken-an-at-home-ancestry-test/ (accessed on 13 May 2022).
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Roundtable on Genomics and Precision Health. The National Academies Collection: Reports Funded by National Institutes of Health, in Exploring the Current Landscape of Consumer Genomics: Proceedings of a Workshop; Beachy, S.H., Alper, J., Addie, S., Hackmann, M., Eds.; National Academies Press (US): Washington, DC, USA, 2020. [Google Scholar]
- Shah, L.L.; Daack-Hirsch, S. Family Communication About Genetic Risk of Hereditary Cardiomyopathies and Arrhythmias: An Integrative Review. J. Genet. Couns. 2018, 27, 1022–1039. [Google Scholar] [CrossRef]
- Wiseman, M.; Dancyger, C.; Michie, S. Communicating genetic risk information within families: A review. Fam. Cancer 2010, 9, 691–703. [Google Scholar] [CrossRef]
- Seymour, K.C.; Addington-Hall, J.; Lucassen, A.M.; Foster, C.L. What Facilitates or Impedes Family Communication Following Genetic Testing for Cancer Risk? A Systematic Review and Meta-Synthesis of Primary Qualitative Research. J. Genet. Couns. 2010, 19, 330–342. [Google Scholar] [CrossRef]
- McCann, S.; MacAuley, D.; Barnett, Y.; Bunting, B.; Bradley, A.; Jeffers, L.; Morrison, P.J. Family communication, genetic testing and colonoscopy screening in hereditary non-polyposis colon cancer: A qualitative study. Psycho-Oncology 2009, 18, 1208–1215. [Google Scholar] [CrossRef]
- Sobel, S.K.; Cowan, D.B. Impact of genetic testing for Huntington disease on the family system. Am. J. Med Genet. 2000, 90, 49–59. [Google Scholar] [CrossRef]
- Timmermans, S.; Stivers, T. The Spillover of Genomic Testing Results in Families: Same Variant, Different Logics. J. Health Soc. Behav. 2017, 58, 166–180. [Google Scholar] [CrossRef]
- Taber, J.M.; Chang, C.Q.; Lam, T.K.; Gillanders, E.M.; Hamilton, J.G.; Schully, S.D. Prevalence and Correlates of Receiving and Sharing High-Penetrance Cancer Genetic Test Results: Findings from the Health Information National Trends Survey. Public Health Genom. 2014, 18, 67–77. [Google Scholar] [CrossRef]
- Finney Rutten, L.J.; Blake, K.D.; Skolnick, V.G.; Davis, T.; Moser, R.P.; Hesse, B.W. Data Resource Profile: The National Cancer Institute’s Health Information National Trends Survey (HINTS). Int. J. Epidemiol. 2020, 49, 17–17j. [Google Scholar] [CrossRef]
- Rutten, L.J.F.; Davis, T.; Beckjord, E.B.; Blake, K.; Moser, R.P.; Hesse, B. Picking Up the Pace: Changes in Method and Frame for the Health Information National Trends Survey (2011–2014). J. Health Commun. 2012, 17, 979–989. [Google Scholar] [CrossRef]
- Health Information National Trends Survey 5 (HINTS 5) Cycle 4. Methodology Report. Rockville, MD: Westat. 2020. Available online: https://hints.cancer.gov/docs/methodologyreports/HINTS5_Cycle4_MethodologyReport.pdf (accessed on 1 November 2022).
- Stewart, K.F.J.; Wesselius, A.; Schreurs, M.A.C.; Schols, A.M.W.J.; Zeegers, M.P. Behavioural changes, sharing behaviour and psychological responses after receiving direct-to-consumer genetic test results: A systematic review and meta-analysis. J. Community Genet. 2017, 9, 1–18. [Google Scholar] [CrossRef]
- Finn, K.S.; Pacyna, J.E.; Tsou, C.; Samadder, N.J.; Sharp, R.R. Factors that Influence Intent to Share Genetic Information Related to Cancer Risk with Family Members. J. Heal. Commun. 2021, 26, 545–552. [Google Scholar] [CrossRef]
- Hunt, K.; Ford, G.; Harkins, L.; Wyke, S. Are Women More Ready to Consult than Men? Gender Differences in Family Practitioner Consultation for Common Chronic Conditions. J. Health Serv. Res. Policy 1999, 4, 96–100. [Google Scholar] [CrossRef]
- Ready, K.; Arun, B.K.; Schmeler, K.M.; Uyei, A.; Litton, J.K.; Lu, K.H.; Sun, C.C.; Peterson, S.K. Communication of BRCA1 and BRCA2 genetic test results to health care providers following genetic testing at a tertiary care center. Fam. Cancer 2011, 10, 673–679. [Google Scholar] [CrossRef]
- Vadaparampil, S.T.; Malo, T.; de la Cruz, C.; Christie, J. Do Breast Cancer Patients Tested in the Oncology Care Setting Share BRCA Mutation Results with Family Members and Health Care Providers? J. Cancer Epidemiol. 2012, 2012, 498062. [Google Scholar] [CrossRef] [PubMed]
- Triantafillidis, J.K.; Vagianos, C.; Gikas, A.; Korontzi, M.; Papalois, A. Screening for colorectal cancer: The role of the primary care physician. Eur. J. Gastroenterol. Hepatol. 2017, 29, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Peterson, E.B.; Ostroff, J.S.; DuHamel, K.N.; D’Agostino, T.A.; Hernandez, M.; Canzona, M.R.; Bylund, C.L. Impact of provider-patient communication on cancer screening adherence: A systematic review. Prev. Med. 2016, 93, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Makhnoon, S.; Maki, K.G.; Yu, R.; Peterson, S.K.; Shete, S. Are beliefs about the importance of genetics for cancer prevention and early detection associated with high risk cancer genetic testing in the U.S. Population? Prev. Med. Rep. 2022, 27, 101781. [Google Scholar] [CrossRef]
- Tandy-Connor, S.; Guiltinan, J.; Krempely, K.; LaDuca, H.; Reineke, P.; Gutierrez, S.; Gray, P.; Davis, B.T. False-positive results released by direct-to-consumer genetic tests highlight the importance of clinical confirmation testing for appropriate patient care. Genet. Med. 2018, 20, 1515–1521. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Category | Total | Sharing with HCP/GC | Sharing with FDR | ||||
|---|---|---|---|---|---|---|---|---|
| N (wtd%) | Shared n (wtd%) | Did Not Share n (wtd%) | p-Value | Shared n (wtd%) | Did Not Share n (wtd%) | p | ||
| Sociodemographic factors | ||||||||
| Age, y | Mean, SD | NA | 50.1, 2.2 | 59.1, 2.3 | 0.018 | 49.8, 2.9 | 53.7, 3.7 | 0.422 |
| Sex | Male | 7 (11.7) | 4 (9.9) | 3 (27.69) | 0.075 | 3 (7.15) | 4 (21.89) | 0.161 |
| Female | 56 (88.3) | 47 (90.1) | 9 (72.31) | 39 (92.85) | 17 (78.11) | |||
| Income | Less than $20,000 | 7 (11.1) | 5 (11.2) | 2 (9.71) | NA | 5 (7.51) | 2 (19.64) | 0.876 |
| $20,000 to less than $35,000 | 5 (3.9) | 4 (3.7) | 1 (5.72) | 2 (3.60) | 3 (4.52) | |||
| $35,000 to less than $50,000 | 4 (10.0) | 4 (10.8) | NA | 3 (9.35) | 1 (11.48) | |||
| $50,000 to less than $75,000 | 13 (33.7) | 9 (32.1) | 4 (54.34) | 8 (34.63) | 5 (31.64) | |||
| $75,000 or more | 31 (41.3) | 28 (42.2) | 3 (30.22) | 23 (44.92) | 8 (32.71) | |||
| Education | ≤High school | 34 (77.0) | 30 (80.1) | 4 (46.62) | 0.036 | 22 (77.17) | 12 (76.77) | 0.978 |
| >High school | 27 (23.0) | 20 (19.9) | 7 (53.38) | 19 (22.83) | 8 (23.23) | |||
| Race/Ethnicity | Non-Hispanic White | 48 (91.7) | 39 (91.3) | 9 (95.29) | NA | 34 (93.68) | 14 (86.53) | NA |
| Non-Hispanic Black | 3 (2.6) | 2 (2.3) | 1 (4.71) | 1 (0.61) | 2 (7.55) | |||
| Hispanic/Latino | 5 (4.8) | 5 (5.3) | NA | 3 (4.33) | 2 (5.92) | |||
| Non-Hispanic other | 1 (1.0) | 1 (1.1) | NA | 1 (1.38) | NA | |||
| Health Insurance | Insured | 61 (100) | 50 (90.3) | 11 (9.74) | NA | 41 (69.09) | 20 (30.91) | NA |
| Uninsured | 0 (0) | (0.00) | (0.00) | 0 (0.00) | (0.00) | |||
| Zip code | Urban | 56 (81.8) | 45 (80.14) | 11 (96.95) | 0.023 | 38 (83.54) | 18 (77.83) | 0.768 |
| Rural | 7 (18.2) | 6 (19.86) | 1 (3.05) | 4 (16.46) | 3 (22.17) | |||
| Clinical factors | ||||||||
| Family history of cancer | Yes | 57 (94.0) | 47 (94.11) | 10 (92.68) | 0.824 | 38 (98.38) | 19 (84.02) | <0.001 |
| No | 6 (6.0) | 4 (5.89) | 2 (7.32) | 4 (1.62) | 2 (15.98) | |||
| Personal history of cancer | Yes | 23 (79.7) | 19 (92.78) | 4 (29.46) | <0.0001 | 16 (82.50) | 7 (71.58) | 0.512 |
| No | 12 (20.3) | 5 (7.22) | 7 (70.54) | 8 (17.50) | 4 (28.42) | |||
| Psychological factors | ||||||||
| Cancer worry | Not at all or Slightly | 7 (8.8) | 4 (7.43) | 3 (20.24) | 0.1936 | 3 (7.35) | 4 (11.89) | 0.198 |
| Somewhat | 19 (33.0) | 18 (36.33) | 1 (5.75) | 13 (25.25) | 6 (49.38) | |||
| Extremely or Moderately | 35 (58.2) | 27 (56.25) | 8 (74.01) | 25 (67.40) | 10 (38.73) | |||
| Perceived genetic susceptibility | A little or Not at all | 60 (95.4) | 48 (94.85) | 12 (100.00) | NA | 39 (93.29) | 21 (100.00) | NA |
| A lot or Somewhat | 3 (4.6) | 3 (5.15) | NA | 3 (6.71) | NA | |||
| Importance of genetics for cancer prevention | A little or Not at all | 58 (92.5) | 47 (93.64) | 11 (81.82) | 0.019 | 40 (92.97) | 18 (91.36) | 0.719 |
| A lot or Somewhat | 4 (7.5) | 3 (6.36) | 1 (18.18) | 2 (7.03) | 2 (8.64) | |||
| Importance of genetics for early detection of cancer | A little or Not at all | 61 (97.6) | 49 (97.29) | 12 (100.00) | NA | 42 (100.00) | 19 (92.06) | NA |
| A lot or Somewhat | 2 (2.4) | 2 (2.71) | NA | NA | 2 (7.94) | |||
| Fatalistic belief | A little or Not at all | 43 (72.8) | 36 (73.27) | 7 (68.99) | 0.83 | 28 (66.09) | 15 (86.94) | 0.131 |
| A lot or Somewhat | 18 (27.2) | 13 (26.73) | 5 (31.01) | 13 (33.91) | 5 (13.06) | |||
| Prevention not possible | Strongly/Somewhat disagree | 10 (21.1) | 8 (22.48) | 2 (10.01) | 0.339 | 6 (12.20) | 4 (39.94) | 0.083 |
| Strongly/Somewhat agree | 51 (78.9) | 41 (77.52) | 10 (89.99) | 35 (87.80) | 16 (60.06) | |||
| Too many recommendations | Strongly/Somewhat disagree | 41 (73.0) | 33 (73.41) | 8 (70.00) | 0.862 | 29 (71.59) | 12 (76.09) | 0.767 |
| Strongly/Somewhat agree | 20 (27.0) | 16 (26.59) | 4 (30.00) | 12 (28.41) | 8 (23.91) | |||
| Self-efficacy | Strongly/Somewhat disagree | 52 (83.2) | 41 (82.90) | 11 (85.33) | 0.882 | 35 (85.32) | 17 (78.63) | 0.671 |
| Strongly/Somewhat agree | 9 (16.8) | 8 (17.10) | 1 (14.67) | 6 (14.68) | 3 (21.37) | |||
| Desire to know about mutation status | A little or Not at all | 57 (88.7) | 45 (87.49) | 12 (100.00) | NA | 41 (94.22) | 16 (75.67) | 0.204 |
| A lot or Somewhat | 5 (11.3) | 5 (12.51) | NA | 1 (5.78) | 4 (24.33) | |||
| Variable | Shared Result with HCP/GC (n = 51, 90.2%) | Shared Result with FDR (n = 42, 69.3%) | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Race/ethnicity | ||||||
| Non-Hispanic White | ref | - | - | ref | - | - |
| Other | 4.987 | 0.24–102.56 | 0.291 | 0.476 | 0.03–6.64 | 0.574 |
| Sex | ||||||
| Male | ref | - | - | ref | - | - |
| Female | 9.322 | 1.93–45.08 | 0.006 | 1.252 | 0.03–59.51 | 0.907 |
| Family history of cancer | ||||||
| No/Not sure | ref | - | - | ref | - | - |
| Yes | 3.71 | 0.07–186.33 | 0.504 | 6.194 | 0.31–293.37 | 0.347 |
| Personal history of cancer | ||||||
| No cancer history | Ref | - | - | ref | - | - |
| Yes | 0.025 | 0.01–0.09 | <0.0001 | 1.917 | 0.34–10.79 | 0.453 |
| Income | ||||||
| Less than $50,000 | ref | - | - | ref | - | - |
| More than $50,000 | 0.981 | 0.14–7.01 | 0.984 | 1.297 | 0.04–38.35 | 0.878 |
| Variable | Categories | Sharing with HCP/GC | Sharing with FDR | ||||
|---|---|---|---|---|---|---|---|
| Shared | Did Not Share | p-Value | Shared | Did Not Share | p-Value | ||
| Age. y | Mean, SD | 50.1, 2.2 | 59.1, 2.3 | 0.005 * | 49.8, 2.9 | 53.7, 3.7 | 0.43 * |
| n (wtd%) | n (wtd%) | n (wtd%) | n (wtd%) | ||||
| Sex | Male | 4 (9.0) | 3 (2.7) | 0.29 ^ | 3 (4.95) | 4 (6.73) | 0.19 ^ |
| Female | 47 (81.2) | 9 (7.1) | 39 (64.32) | 17 (24.00) | |||
| Income | Less than $20,000 | 5 (10.1) | 2 (0.72) | NA ^ | 5 (10.10) | 2 (0.72) | 0.80 ^ |
| $20,000 to less than $35,000 | 4 (3.4) | 1 (0.42) | 4 (3.35) | 1 (0.42) | |||
| $35,000 to less than $50,000 | 4 (9.7) | 0 (0) | 4 (9.73) | 0 (0) | |||
| $50,000 to less than $75,000 | 9 (28.9) | 4 (4.01) | 9 (28.89) | 4 (4.01) | |||
| $75,000 or more | 28 (38.0) | 3 (2.23) | 28 (38.03) | 3 (2.23) | |||
| Education | Less than high school | 2 (6.2) | 1 (0.30) | NA ^ | 2 (4.30) | 1 (2.17) | 0.99 ^ |
| 12 years/Completed high school | 9 (19.6) | 0 (0) | 6 (13.73) | 3 (5.83) | |||
| College graduate or higher | 19 (46.5) | 3 (3.97) | 14 (34.94) | 8 (15.50) | |||
| Some college | 20 (17.9) | 7 (4.89) | 19 (15.67) | 8 (7.11) | |||
| Race/Ethnicity | Non-Hispanic White | 39 (82.8) | 9 (8.92) | NA ^ | 34 (67.47) | 14 (24.21) | NA ^ |
| Non-Hispanic Black | 2 (2.1) | 1 (0.44) | 1 (0.44) | 2 (2.11) | |||
| Hispanic/Latino | 5 (4.8) | 0 (0) | 3 (3.12) | 2 (1.66) | |||
| Non-Hispanic Asian | 1 (1.0) | 0 (0) | 1 (0.99) | 0 (0) | |||
| Non-Hispanic other | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| Health Insurance | Insured | 50 (90.3) | 11 (9.74) | NA ^ | 41 (69.09) | 20 (30.91) | NA ^ |
| Uninsured | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| Zip code | Urban | 45 (72.3) | 11 (9.49) | 0.13 ^ | 38 (57.87) | 18 (23.92) | 0.78 ^ |
| Rural | 6 (17.9) | 1 (0.30) | 4 (11.40) | 3 (6.81) | |||
| Variable | Categories | Sharing with HCP/GC | Sharing with FDR | ||||
|---|---|---|---|---|---|---|---|
| Shared | Did Not Share | p-Value | Shared | Did Not Share | p-Value | ||
| Age, y | Mean, SD | 49.0, 5.1 | 52.1, 1.4 | 0.56 * | 50.8, 1.6 | 57.0, 2.4 | 0.05 * |
| n (wtd%) | n (wtd%) | n (wtd%) | n (wtd%) | ||||
| Sex | Male | 4 (1.38) | 127 (45.42) | 0.51 ^ | 96 (36.46) | 35 (10.34) | 0.43 ^ |
| Female | 9 (2.79) | 157 (50.41) | 129 (43.87) | 37 (9.33) | |||
| Income | Less than $20,000 | 2 (0.28) | 14 (5.98) | NA ^ | 12 (4.37) | 4 (1.89) | 0.90 ^ |
| $20,000 to less than $35,000 | 3 (0.34) | 16 (6.12) | 15 (4.74) | 4 (1.72) | |||
| $35,000 to less than $50,000 | 1 (0.20) | 40 (12.37) | 31 (10.05) | 10 (2.52) | |||
| $50,000 to less than $75,000 | 3 (1.29) | 51 (15.75) | 39 (13.23) | 15 (3.80) | |||
| $75,000 or more | 4 (2.07) | 142 (52.90) | 114 (45.89) | 32 (9.08) | |||
| Education | Less than high school | 0 (0) | 1 (0.16) | NA ^ | 0 (0) | 1 (0.16) | NA ^ |
| 12 years/Completed high school | 1 (0.66) | 32 (16.28) | 24 (13.44) | 9 (3.51) | |||
| College graduate or higher | 7 (1.65) | 171 (40.63) | 136 (35.25) | 42 (7.03) | |||
| Some college | 5 (1.86) | 77 (38.37) | 62 (31.25) | 20 (8.98) | |||
| Race/Ethnicity | Non-Hispanic White | 8 (2.86) | 208 (80.94) | NA ^ | 169 (68.60) | 47 (15.20) | 0.19 ^ |
| Non-Hispanic Black | 2 (0.40) | 26 (5.43) | 21 (4.82) | 7 (1.01) | |||
| Hispanic/Latino | 2 (0.91) | 25 (5.28) | 20 (5.56) | 7 (0.63) | |||
| Non-Hispanic Asian | 1 (0.06) | 6 (1.81) | 3 (0.66) | 4 (1.22) | |||
| Non-Hispanic other | 0 (0) | 9 (2.31) | 4 (0.48) | 5 (1.83) | |||
| Health Insurance | Insured | 13 (4.17) | 278 (94.04) | NA ^ | 221 (78.68) | 70 (19.54) | 0.53 ^ |
| Uninsured | 0 (0) | 4 (1.79) | 2 (1.62) | 2 (0.17) | |||
| Zip code | Urban | 12 (2.98) | 257 (83.05) | 0.56 ^ | 205 (69.38) | 64 (16.64) | 0.82 ^ |
| Rural | 1 (1.19) | 27 (12.78) | 20 (10.94) | 8 (3.03) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makhnoon, S.; Yu, R.; Peterson, S.K.; Shete, S. Clinical Cancer and Direct-to-Consumer Genetic Test Result-Sharing Behavior: Findings from HINTS 2020. J. Pers. Med. 2023, 13, 18. https://doi.org/10.3390/jpm13010018
Makhnoon S, Yu R, Peterson SK, Shete S. Clinical Cancer and Direct-to-Consumer Genetic Test Result-Sharing Behavior: Findings from HINTS 2020. Journal of Personalized Medicine. 2023; 13(1):18. https://doi.org/10.3390/jpm13010018
Chicago/Turabian StyleMakhnoon, Sukh, Robert Yu, Susan K Peterson, and Sanjay Shete. 2023. "Clinical Cancer and Direct-to-Consumer Genetic Test Result-Sharing Behavior: Findings from HINTS 2020" Journal of Personalized Medicine 13, no. 1: 18. https://doi.org/10.3390/jpm13010018
APA StyleMakhnoon, S., Yu, R., Peterson, S. K., & Shete, S. (2023). Clinical Cancer and Direct-to-Consumer Genetic Test Result-Sharing Behavior: Findings from HINTS 2020. Journal of Personalized Medicine, 13(1), 18. https://doi.org/10.3390/jpm13010018