
Comparison of Clinical and Imaginal Features According to the Pathological Grades of Dysplasia in Branch-Duct Intraductal Papillary Mucinous Neoplasm (BD-IPMN) for Personalized Medicine

 ,
,
Abstract
1. Introduction
2. Materials and Methods
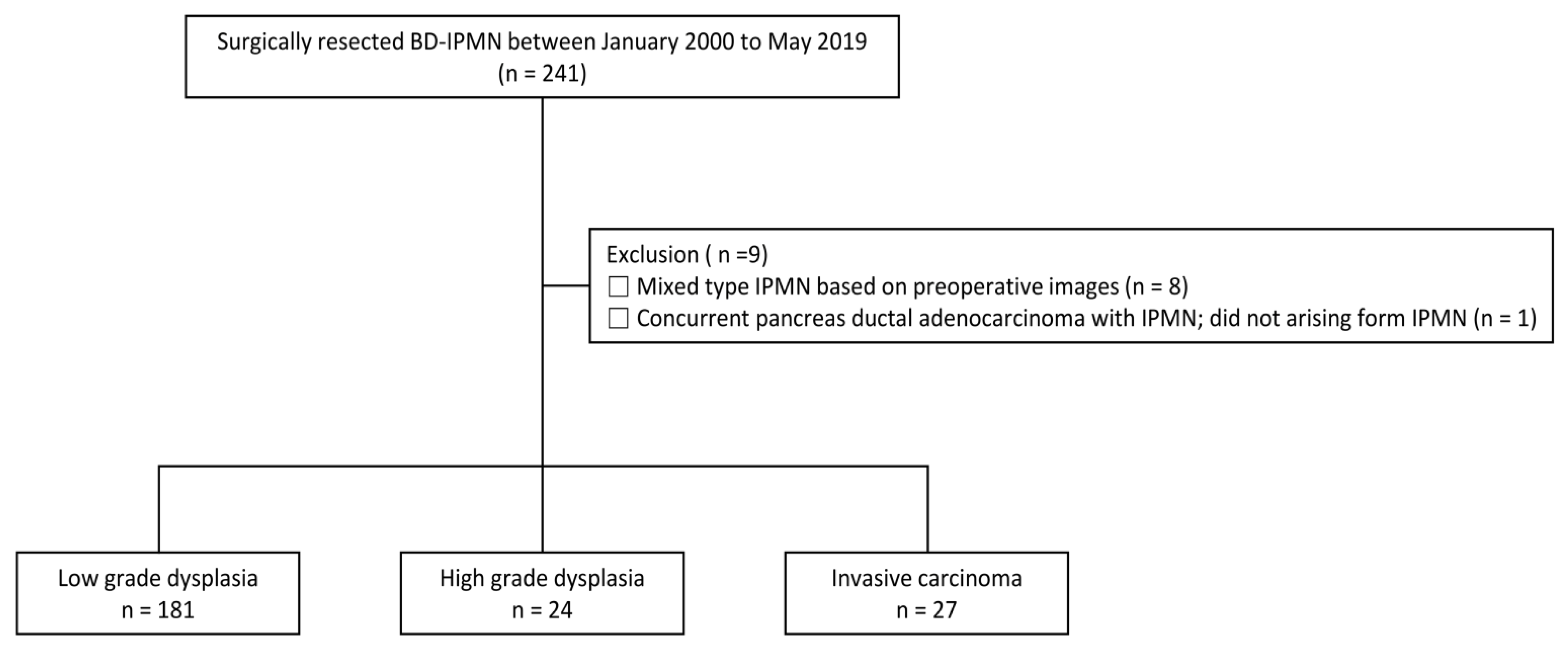
2.1. Study Design and Participants
2.2. Study Variables
2.3. Statistical Analysis
3. Results
3.1. Comparison of Baseline Characteristics
3.2. Factors That Distinguish HGD from LGD and HGD from IC
3.3. Prediction of Malignant Lesion Based on Presence or Absence of “WF” and/or “HRS”
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, T.H.; Song, T.J.; Hwang, J.-H.; Yoo, K.-S.; Lee, W.-J.; Lee, K.-H.; Dong, S.-H.; Park, C.-H.; Park, E.-T.; Moon, J.-H.; et al. Predictors of malignancy in pure branch duct type intraductal papillary mucinous neoplasm of the pancreas: A nationwide multicenter study. Pancreatology 2015, 15, 405–410. [Google Scholar] [CrossRef]
- Wada, K.; Kozarek, R.A.; Traverso, L.W. Outcomes following resection of invasive and noninvasive intraductal papillary mucinous neoplasms of the pancreas. Am. J. Surg. 2005, 189, 632–637. [Google Scholar] [CrossRef] [PubMed]
- European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms. Gut 2018, 67, 789–804. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.; Donahue, T.R.; Reber, H.A.; Hines, O.J. Pancreatic Cyst Disease. JAMA 2016, 315, 1882–1893. [Google Scholar] [CrossRef]
- Tanaka, M.; Fernández-del Castillo, C.; Kamisawa, T.; Jang, J.Y.; Levy, P.; Ohtsuka, T.; Salvia, R.; Shimizu, Y.; Tada, M.; Wolfgang, C.L. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 2017, 17, 738–753. [Google Scholar] [CrossRef]
- Vege, S.S.; Ziring, B.; Jain, R.; Moayyedi, P.; Adams, M.A.; Dorn, S.D.; Dudley-Brown, S.L.; Flamm, S.L.; Gellad, Z.F.; Gruss, C.B.; et al. American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015, 148, 819–822. [Google Scholar] [CrossRef]
- Kneuertz, P.J.; Pitt, H.A.; Bilimoria, K.Y.; Smiley, J.P.; Cohen, M.E.; Ko, C.Y.; Pawlik, T.M. Risk of Morbidity and Mortality Following Hepato-Pancreato-Biliary Surgery. J. Gastrointest. Surg. 2012, 16, 1727–1735. [Google Scholar] [CrossRef]
- Kanno, A.; Satoh, K.; Hirota, M.; Hamada, S.; Umino, J.; Itoh, H.; Masamune, A.; Asakura, T.; Shimosegawa, T. Prediction of invasive carcinoma in branch type intraductal papillary mucinous neoplasms of the pancreas. J. Gastroenterol. 2010, 45, 952–959. [Google Scholar] [CrossRef]
- Kawada, N.; Uehara, H.; Nagata, S.; Tsuchishima, M.; Tsutsumi, M.; Tomita, Y. Predictors of Malignancy in Branch Duct Intraductal Papillary Mucinous Neoplasm of the Pancreas. JOP J. Pancreas 2014, 15, 459–464. [Google Scholar] [CrossRef]
- Chari, S.T.; Yadav, D.; Smyrk, T.C.; DiMagno, E.P.; Miller, L.J.; Raimondo, M.; Clain, J.E.; Norton, I.A.; Pearson, R.K.; Petersen, B.T.; et al. Study of recurrence after surgical resection of intraductal papillary mucinous neoplasm of the pancreas. Gastroenterology 2002, 123, 1500–1507. [Google Scholar] [CrossRef]
- Hirono, S.; Shimizu, Y.; Ohtsuka, T.; Kin, T.; Hara, K.; Kanno, A.; Koshita, S.; Hanada, K.; Kitano, M.; Inoue, H.; et al. Recurrence patterns after surgical resection of intraductal papillary mucinous neoplasm (IPMN) of the pancreas; a multicenter, retrospective study of 1074 IPMN patients by the Japan Pancreas Society. J. Gastroenterol. 2019, 55, 86–99. [Google Scholar] [CrossRef]
- Hirono, S.; Yamaue, H. Surgical strategy for intraductal papillary mucinous neoplasms of the pancreas. Surg. Today 2019, 50, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Attiyeh, M.A.; Castillo, C.F.-D.; Al Efishat, M.; Eaton, A.A.; Gönen, M.; Batts, R.; Pergolini, I.; Rezaee, N.; Lillemoe, K.D.; Ferrone, C.R.; et al. Development and Validation of a Multi-institutional Preoperative Nomogram for Predicting Grade of Dysplasia in Intraductal Papillary Mucinous Neoplasms (IPMNs) of the Pancreas. Ann. Surg. 2018, 267, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Do, R.K.G.; Katz, S.S.; Gollub, M.J.; Li, J.; LaFemina, J.; Zabor, E.C.; Moskowitz, C.S.; Klimstra, D.S.; Allen, P.J. Interobserver Agreement for Detection of Malignant Features of Intraductal Papillary Mucinous Neoplasms of the Pancreas on MDCT. Am. J. Roentgenol. 2014, 203, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Lisotti, A.; Napoleon, B.; Facciorusso, A.; Cominardi, A.; Crinò, S.F.; Brighi, N.; Gincul, R.; Kitano, M.; Yamashita, Y.; Marchegiani, G. Contrast-enhanced EUS for the characterization of mural nodules within pancreatic cystic neoplasms: Sys-tematic review and meta-analysis. Gastrointest. Endosc. 2021, 94, 881–889.e885. [Google Scholar] [CrossRef]
- Krishna, S.G.; Hart, P.A.; DeWitt, J.M.; DiMaio, C.J.; Kongkam, P.; Napoleon, B.; Othman, M.O.; Tan, D.M.Y.; Strobel, S.G.; Stanich, P.; et al. EUS-guided confocal laser endomicroscopy: Prediction of dysplasia in intraductal papillary mucinous neoplasms (with video). Gastrointest. Endosc. 2019, 91, 551–563.e5. [Google Scholar] [CrossRef]
- Facciorusso, A.; Kovacevic, B.; Yang, D.; Vilas-Boas, F.; Martínez-Moreno, B.; Stigliano, S.; Rizzatti, G.; Sacco, M.; Arevalo-Mora, M.; Villarreal-Sanchez, L.; et al. Predictors of adverse events after endoscopic ultrasound-guided through-the-needle biopsy of pancreatic cysts: A recursive partitioning analysis. Endoscopy 2022, 54, 1158–1168. [Google Scholar] [CrossRef]
- Blackham, A.U.; Doepker, M.P.; Centeno, B.A.; Springett, G.; Pimiento, J.M.; Malafa, M.; Hodul, P.J. Patterns of recurrence and long-term outcomes in patients who underwent pancreatectomy for intraductal papillary mucinous neoplasms with high grade dysplasia: Implications for surveillance and future management guidelines. Hpb 2017, 19, 603–610. [Google Scholar] [CrossRef]
- Majumder, S.; Philip, N.A.; Nagpal, S.J.S.; Takahashi, N.; Mara, K.C.; Kendrick, M.L.; Smyrk, T.C.; Zhang, L.; Levy, M.J.; Gleeson, F.C.; et al. High-Grade Dysplasia in Resected Main-Duct Intraductal Papillary Mucinous Neoplasm (MD-IPMN) is Associated with an Increased Risk of Subsequent Pancreatic Cancer. Am. J. Gastroenterol. 2018, 114, 524–529. [Google Scholar] [CrossRef]
- Jang, J.-Y.; Park, T.; Lee, S.; Kim, Y.; Lee, S.Y.; Kim, S.-W.; Kim, S.-C.; Song, K.-B.; Yamamoto, M.; Hatori, T.; et al. Proposed Nomogram Predicting the Individual Risk of Malignancy in the Patients With Branch Duct Type Intraductal Papillary Mucinous Neoplasms of the Pancreas. Ann. Surg. 2017, 266, 1062–1068. [Google Scholar] [CrossRef]
- Uehara, H.; Ishikawa, O.; Katayama, K.; Kawada, N.; Ikezawa, K.; Fukutake, N.; Takakura, R.; Takano, Y.; Tanaka, S.; Takenaka, A. Size of mural nodule as an indicator of surgery for branch duct intraductal papillary mucinous neoplasm of the pancreas during follow-up. J. Gastroenterol. 2010, 46, 657–663. [Google Scholar] [CrossRef]
- Maitra, A.; Fukushima, N.; Takaori, K.; Hruban, R.H. Precursors to Invasive Pancreatic Cancer. Adv. Anat. Pathol. 2005, 12, 81–91. [Google Scholar] [CrossRef]
- Jan, I.-S.; Chang, M.-C.; Yang, C.-Y.; Tien, Y.-W.; Jeng, Y.-M.; Wu, C.-H.; Chen, B.-B.; Chang, Y.-T. Validation of Indications for Surgery of European Evidence-Based Guidelines for Patients with Pancreatic Intraductal Papillary Mucinous Neoplasms. J. Gastrointest. Surg. 2019, 24, 2536–2543. [Google Scholar] [CrossRef]
- Wilson, G.C.; Maithel, S.K.; Bentrem, D.; Abbott, D.E.; Weber, S.; Cho, C.; Martin, R.C.; Scoggins, C.R.; Kim, H.J.; Merchant, N.B.; et al. Are the Current Guidelines for the Surgical Management of Intraductal Papillary Mucinous Neoplasms of the Pancreas Adequate? A Multi-Institutional Study. J. Am. Coll. Surg. 2017, 224, 461–469. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | LGD (n = 181) | HGD (n = 24) | IC (n = 27) | p-Value *,** |
|---|---|---|---|---|
| Age, years † | 63 (57–69) | 67 (55–71) | 65 (56–72) | 0.768 * 0.948 ** |
| Sex, male | 126 (69.6) | 8 (33.3) | 16 (59.3) | 0.000 * 0.064 ** |
| BMI † | 24 (22–26) | 25 (23–26) | 24 (22–25) | 0.715 * 0.148 ** |
| DM | 36 (19.9) | 7 (29.2) | 8 (29.6) | 0.294 * 0.971 ** |
| New-onset DM | 9 (5.0) | 1 (4.2) | 4 (14.8) | 1.000 * 0.354 ** |
| Weight loss | 5 (2.8) | 0 (0.0) | 0 (0.0) | 1.000 * |
| CA 19-9, U/mL † | 11 (7–19) | 13 (7–21) | 39 (6–296) | 0.792 * 0.132 ** |
| CEA, ng/mL † | 1.6 (1.0–2.5) | 1.3 (1.0–1.8) | 1.5 (1.1–2.3) | 0.304 * 0.389 ** |
| Location, head, neck, and uncinate | 112 (61.9) | 18 (75) | 22 (81.5) | 0.210 * 0.574 ** |
| Multifocal | 53 (29.3) | 8 (33.3) | 7 (25.9) | 0.683 * 0.562 ** |
| Size based on images, cm † | 3.0 (2.3–4.0) | 3.5 (3.0–4.5) | 3.2 (2.4–4.5) | 0.159 * 0.524 ** |
| High-risk stigmata (HRS) | ||||
| Obstructive jaundice with cystic lesion | 2 (1.1) | 1 (4.2) | 10 (37.0) | 0.313 * 0.004 ** |
| Solid component or enhancing mural nodule ≥ 5 mm | 14 (7.7) | 9 (37.5) | 15 (55.6) | 0.000 * 0.197 ** |
| Solid component or enhancing mural nodule ≥ 10 mm | 7 (3.9) | 8 (33.3) | 12 (44.4) | 0.000 * 0.417 ** |
| Main pancreatic duct ≥ 10 mm | 0 (0.0) | 1 (4.2) | 2 (7.4) | 0.117 * 1.000 ** |
| Worrisome features (WF) | ||||
| Pancreatitis | 14 (7.7) | 2 (8.3) | 3 (11.1) | 1.000 * 1.000 ** |
| Cyst ≥ 3 cm | 108 (59.7) | 19 (79.2) | 17 (63.0) | 0.065 * 0.205 ** |
| Enhancing mural nodule < 5 mm | 4 (2.2) | 0 (0.0) | 0 (0.0) | 1.000 * |
| Thickened (>2 mm)/enhancing cyst walls | 9 (5.0) | 5 (20.8) | 6 (22.2) | 0.014 * 0.904 ** |
| Main-duct size 5–9 mm | 38 (21.0) | 6 (25.0) | 4 (14.8) | 0.653 * 0.485 ** |
| Abrupt change in duct caliber | 0 (0.0) | 0 (0.0) | 1 (3.7) | 1.000 ** |
| Lymphadenopathy | 2 (1.1) | 0 (0.0) | 3 (11.1) | 1.000 * 0.238 ** |
| Cystic growth rate ≥ 5 mm/2 years | 34 (18.8) | 3 (12.5) | 3 (11.1) | 0.580 * 1.000 ** |
| Increased serum CA 19-9 (≥37 U/mL) | 14 (8.0) | 2 (8.3) | 14 (51.9) | 1.000 * 0.001 ** |
| Features on EUS (n = 93) | 69 | 16 | 8 | 1.000 * 0.015 ** |
| Definite mural nodule(s) ≥ 5 mm | 21 (30.4) | 5 (31.3) | 6 (75) | |
| Suspicious for main-duct involvement | 4 (5.8) | 0 (0.0) | 1 (12.5) | |
| Cytology on FNA (n = 45) | 27 | 13 | 5 | 0.013 * 0.268 ** |
| Low cellularity (inadequate) | 6 (22.2) | 2 (15.3) | 0 (0.0) | |
| Negative | 15 (55.6) | 4 (30.8) | 0 (0.0) | |
| Atypical cell | 5 (18.5) | 1 (7.7) | 2 (40.0) | |
| Suspicious or positive for malignancy | 1 (3.7) | 6 (46.2) | 3 (60.0) |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| p-Value * | OR | 95% CI | p-Value * | |
| Sex, male | 0.001 | 0.21 | 0.07–0.66 | 0.004 |
| Solid component or enhancing mural nodule ≥ 5 mm | 0.001 | 9.29 | 3.63–54.12 | <0.000 |
| Thickened/enhancing cyst walls | 0.029 | 6.95 | 1.68–33.13 | 0.008 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| p-Value * | OR | 95% CI | p-Value * | |
| Obstructive jaundice with cystic lesion | 0.009 | |||
| Increased serum CA 19-9 (≥37 U/mL) | 0.002 | 12.59 | 1.81–87.44 | 0.006 |
| Patients with No “HRS” | LGD/HGD, N | OR | 95% CI | p-Value |
|---|---|---|---|---|
| No WF (Ref) | 34/0 | |||
| 1 WF | 79/7 | 6.51 | 0.23–186.07 | 0.421 |
| 2 WF | 40/4 | 7.67 | 0.25–236.85 | 0.366 |
| ≥3 WF | 12/4 | 24.85 | 0.77–806.70 | 0.077 |
| Patients with “HRS” | ||||
| 1 HRS only or with one or more WF (Ref) | 16/7 | |||
| >1 HRS | 0/2 | 11.00 | 0.14–869.37 | 0.438 |
| Patients with No “HRS” | HGD/IC, N | OR | 95% CI | p-Value |
|---|---|---|---|---|
| No WF | 0/0 | |||
| 1 WF (Ref) | 7/4 | |||
| 2 WF | 4/3 | 1.31 | 0.14–12.02 | 1.000 |
| ≥3 WF | 4/1 | 0.44 | 0.03–7.74 | 1.000 |
| Patients with “HRS” | ||||
| 1 HRS only or with one or more WF (Ref) | 7/12 | |||
| >1 HRS | 2/7 | 2.04 | 0.25–16.50 | 0.888 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Na, J.E.; Park, J.K.; Lee, J.K.; Park, J.K.; Lee, K.H.; Lee, K.T. Comparison of Clinical and Imaginal Features According to the Pathological Grades of Dysplasia in Branch-Duct Intraductal Papillary Mucinous Neoplasm (BD-IPMN) for Personalized Medicine. J. Pers. Med. 2023, 13, 149. https://doi.org/10.3390/jpm13010149
Na JE, Park JK, Lee JK, Park JK, Lee KH, Lee KT. Comparison of Clinical and Imaginal Features According to the Pathological Grades of Dysplasia in Branch-Duct Intraductal Papillary Mucinous Neoplasm (BD-IPMN) for Personalized Medicine. Journal of Personalized Medicine. 2023; 13(1):149. https://doi.org/10.3390/jpm13010149
Chicago/Turabian StyleNa, Ji Eun, Jae Keun Park, Jong Kyun Lee, Joo Kyung Park, Kwang Hyuck Lee, and Kyu Taek Lee. 2023. "Comparison of Clinical and Imaginal Features According to the Pathological Grades of Dysplasia in Branch-Duct Intraductal Papillary Mucinous Neoplasm (BD-IPMN) for Personalized Medicine" Journal of Personalized Medicine 13, no. 1: 149. https://doi.org/10.3390/jpm13010149
APA StyleNa, J. E., Park, J. K., Lee, J. K., Park, J. K., Lee, K. H., & Lee, K. T. (2023). Comparison of Clinical and Imaginal Features According to the Pathological Grades of Dysplasia in Branch-Duct Intraductal Papillary Mucinous Neoplasm (BD-IPMN) for Personalized Medicine. Journal of Personalized Medicine, 13(1), 149. https://doi.org/10.3390/jpm13010149