
Epidemiology and Risk Factors of UTIs in Children—A Single-Center Observation
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
- Trial design
- Settings and participants
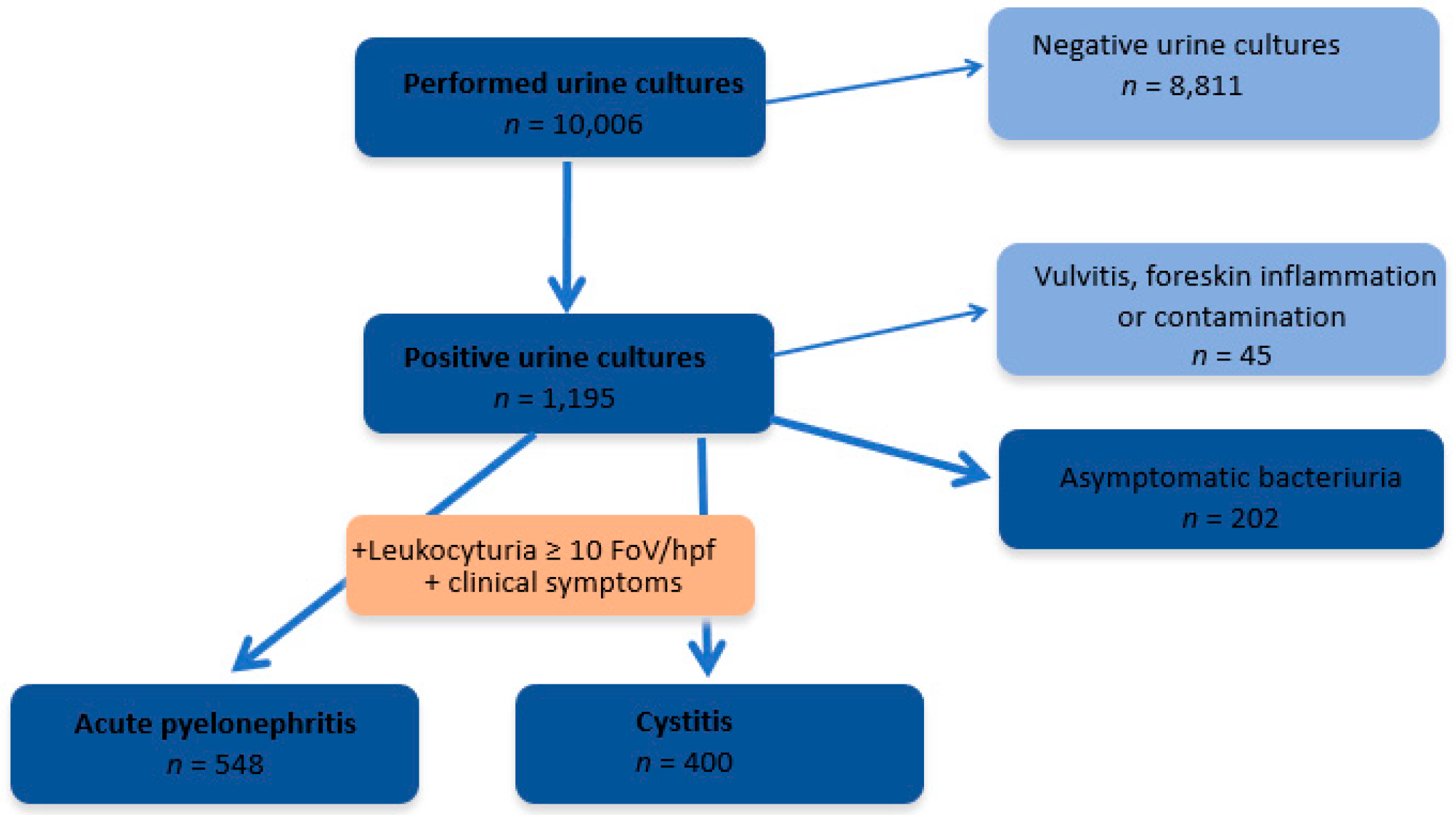
- Eligibility criteria:
- Aged from 0 to 18 years;
- Positive urine culture;
- Leukocyturia ≥10 white blood cells per high power field (WBC/hpf).
- Exclusion criteria:
- Patients whose parents or legal guardians did not consent to the use of the child’s data for scientific research upon admission to the hospital.
- Methods
- ≥2 infections in the upper urinary tract in one year or;
- A total of 1 UTI in the upper urinary tract and ≥1 infection in the lower urinary tract in one year or;
- Statistical analysis
3. Results
3.1. Clinical and Laboratory Manifestations
3.2. Risk Factors
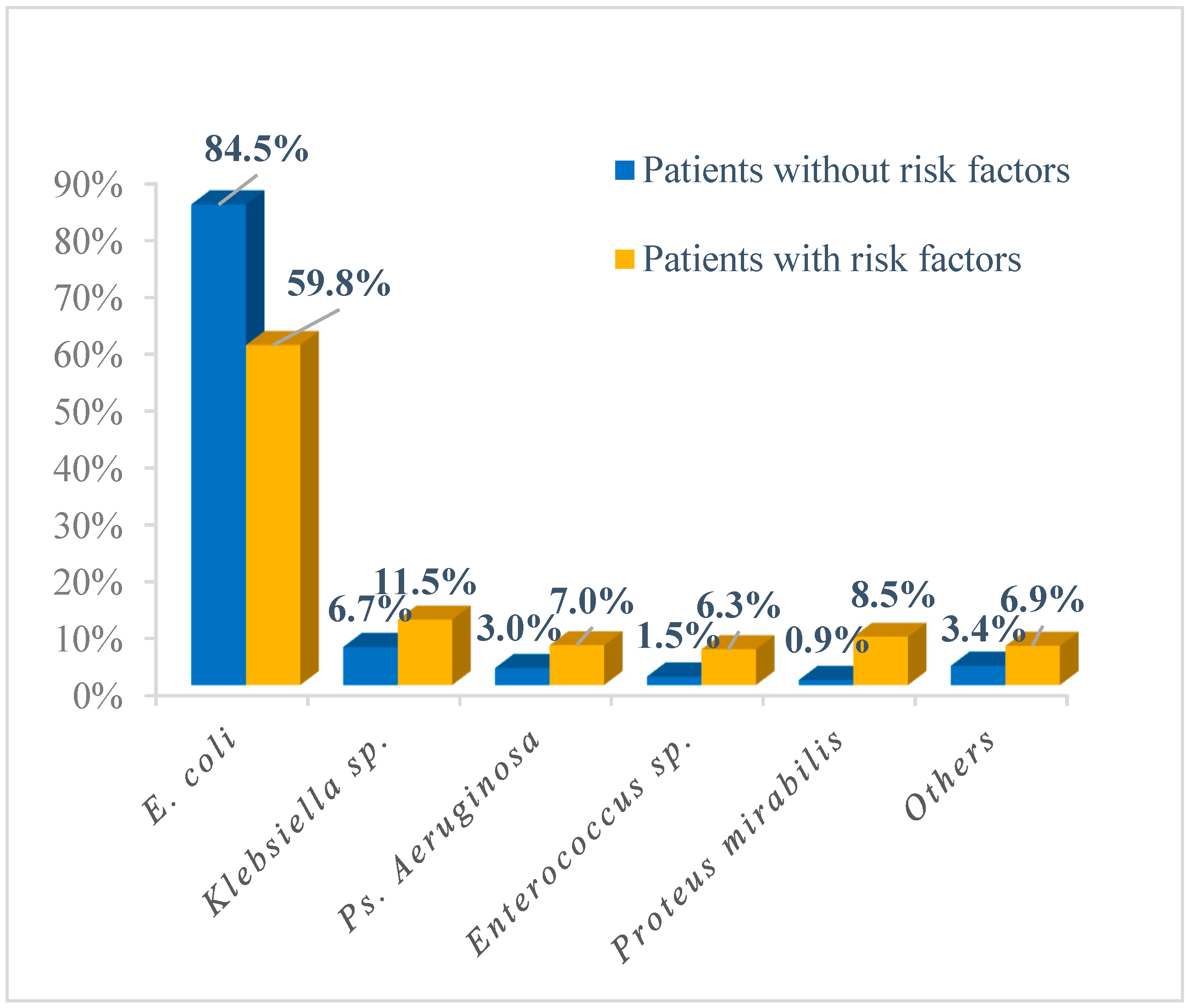
3.3. Etiology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tullus, K.; Shaikh, N. Urinary tract infections in children. Lancet 2020, 395, 1659–1668. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.; Dogan, H.S.; Hoebeke, P.; Kočvara, R.; Nijman, R.J.; Radmayr, C.; Tekgül, S.; European Association of Urology; European Society for Pediatric Urology. Urinary tract infections in children: EAU/ESPU guidelines. Eur. Urol. 2015, 67, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Morone, N.E.; Bost, J.E.; Farrell, M.H. Prevalence of urinary tract infection in childhood: A meta-analysis. Pediatr. Infect. Dis. J. 2008, 27, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.C.; Wong, A.H.C.; Leung, A.A.M.; Hon, K.L. Urinary Tract Infection in Children. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Atay, N.; Gökceoğlu, A.U. Evaluation of urinalysis and urine culture in children with first-time urinary tract infection. Turk. J. Urol. 2021, 47, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Schlager, T.A. Urinary Tract Infections in Infants and Children. Microbiol Spectr. 2016, 4. [Google Scholar] [CrossRef]
- Simões e Silva, A.C.; Oliveira, E.A. Update on the approach of urinary tract infection in childhood. J. Pediatr. 2015, 91 (Suppl. 1), S2–S10. [Google Scholar] [CrossRef]
- Edlin, R.S.; Shapiro, D.J.; Hersh, A.L.; Copp, H.L. Antibiotic resistance patterns of outpatient pediatric urinary tract infections. J. Urol. 2013, 190, 222–227. [Google Scholar] [CrossRef]
- Shaikh, N.; Shope, T.R.; Hoberman, A.; Vigliotti, A.; Kurs-Lasky, M.; Martin, J.M. Association Between Uropathogen and Pyuria. Pediatrics 2016, 138, e20160087. [Google Scholar] [CrossRef]
- Keren, R.; Shaikh, N.; Pohl, H.; Gravens-Mueller, L.; Ivanova, A.; Zaoutis, L.; Patel, M.; deBerardinis, R.; Parker, A.; Bhatnagar, S.; et al. Risk Factors for Recurrent Urinary Tract Infection and Renal Scarring. Pediatrics 2015, 136, e13–e21. [Google Scholar] [CrossRef]
- Pérez, R.P.; Ortega, M.J.C.; Álvarez, J.A.; Baquero-Artigao, F.; Rico, J.C.S.; Zúñiga, R.V.; Campos, L.M.; Gallego, B.C.; Fernández, A.J.C.; Calvo, C.; et al. Recommendations on the diagnosis and treatment of urinary tract infection. An. Pediatr. 2019, 90, 400.e1–400.e9. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence: Clinical Guidelines; Urinary tract infection in under 16s: Diagnosis and management; National Institute for Health and Care Excellence: London, UK, 2022; Available online: https://www.nice.org.uk/guidance/ng224/chapter/Recommendations-for-research (accessed on 9 January 2023).
- Subcommittee on Urinary Tract Infection; Roberts, K.B. Reaffirmation of AAP Clinical Practice Guideline: The Diagnosis and Management of the Initial Urinary Tract Infection in Febrile Infants and Young Children 2–24 Months of Age. Pediatrics 2016, 138, e20163026. [Google Scholar]
- Ammenti, A.; Alberici, I.; Brugnara, M.; Chimenz, R.; Guarino, S.; La Manna, A.; La Scola, C.; Maringhini, S.; Marra, G.; Materassi, M.; et al. Updated Italian recommendations for the diagnosis, treatment and follow-up of the first febrile urinary tract infection in young children. Acta Paediatr. 2020, 109, 236–247. [Google Scholar] [CrossRef]
- Robinson, J.L.; Finlay, J.C.; Lang, M.E.; Bortolussi, R. Urinary tract infections in infants and children: Diagnosis and management. Paediatr. Child Health 2014, 19, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Ziółkowska, H.B.-C.I.; Grenda, R.; Musiał, K.; Ogarek, I.; Szczepańska, M.; Zachwieja, J. Żurowska A Zalecenia Polskiego Towarzystwa Nefrologii Dziecięcej (PTNFD) dotyczące postępowania z dzieckiem z zespołem nerczycowym. Forum Nefrol. 2015, 8, 238–256. [Google Scholar]
- Stephens, G.M.; Akers, S.; Nguyen, H.; Woxland, H. Evaluation and management of urinary tract infections in the school-aged child. Prim. Care 2015, 42, 33–41. [Google Scholar] [CrossRef]
- Larcombe, J. Urinary tract infection in children. Am. Fam. Phys. 2010, 82, 1252–1256. [Google Scholar]
- Karmazyn, B.K.; Alazraki, A.L.; Anupindi, S.A.; Dempsey, M.E.; Dillman, J.R.; Dorfman, S.R.; Garber, M.D.; Moore, S.G.; Peters, C.A.; Rice, H.E.; et al. ACR Appropriateness Criteria® Urinary Tract Infection-Child. J. Am. Coll. Radiol. 2017, 14, S362–S371. [Google Scholar] [CrossRef]
- Korbel, L.; Howell, M.; Spencer, J.D. The clinical diagnosis and management of urinary tract infections in children and adolescents. Paediatr. Int. Child Health 2017, 37, 273–279. [Google Scholar] [CrossRef]
- Clark, C.J.; Kennedy, W.A., 2nd; Shortliffe, L.D. Urinary tract infection in children: When to worry. Urol. Clin. N. Am. 2010, 37, 229–241. [Google Scholar] [CrossRef]
- Chang, S.L.; Shortliffe, L.D. Pediatric urinary tract infections. Pediatr. Clin. N. Am. 2006, 53, 379–400. [Google Scholar] [CrossRef] [PubMed]
- Zorc, J.J.; Kiddoo, D.A.; Shaw, K.N. Diagnosis and management of pediatric urinary tract infections. Clin. Microbiol. Rev. 2005, 18, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Balighian, E.; Burke, M. Urinary Tract Infections in Children. Pediatr. Rev. 2018, 39, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Copp, H.L. Work-up of Pediatric Urinary Tract Infection. Urol. Clin. N. Am. 2015, 42, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Jackson, E.C. Urinary tract infections in children: Knowledge updates and a salute to the future. Pediatr. Rev. 2015, 36, 153–164. [Google Scholar] [CrossRef]
- Chen, L.; Baker, M.D. Racial and ethnic differences in the rates of urinary tract infections in febrile infants in the emergency department. Pediatr. Emerg. Care 2006, 22, 485–487. [Google Scholar] [CrossRef]
- Morello, W.; La Scola, C.; Alberici, I.; Montini, G. Acute pyelonephritis in children. Pediatr. Nephrol. 2016, 31, 1253–1265. [Google Scholar] [CrossRef]
- Hudson, A.; Romao, R.L.P.; MacLellan, D. Urinary tract infection in children. CMAJ 2017, 189, E608. [Google Scholar] [CrossRef]
- Roberts, K.B. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef]
- Hanna-Wakim, R.H.; Ghanem, S.T.; El Helou, M.W.; Khafaja, S.A.; Shaker, R.A.; Hassan, S.A.; Saad, R.K.; Hedari, C.P.; Khinkarly, R.W.; Hajar, F.M.; et al. Epidemiology and characteristics of urinary tract infections in children and adolescents. Front. Cell. Infect. Microbiol. 2015, 5, 45. [Google Scholar] [CrossRef]
- Krawczyk, B.; Wysocka, M.; Michalik, M.; Gołębiewska, J. Urinary Tract Infections Caused by K. pneumoniae in Kidney Transplant Recipients-Epidemiology, Virulence and Antibiotic Resistance. Front. Cell. Infect. Microbiol. 2022, 12, 861374. [Google Scholar] [CrossRef] [PubMed]
- Stamm, W.E.; Norrby, S.R. Urinary tract infections: Disease panorama and challenges. J. Infect. Dis. 2001, 183 (Suppl. 1), S1–S4. [Google Scholar] [CrossRef] [PubMed]
- Mohkam, M. Novel Urinary Biomarkers for Diagnosis of Acute Pyelonephritis in Children. Iran. J. Kidney Dis. 2020, 14, 1–7. [Google Scholar]
- Bitsori, M.; Maraki, S.; Koukouraki, S.; Galanakis, E. Pseudomonas aeruginosa urinary tract infection in children: Risk factors and outcomes. J. Urol. 2012, 187, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Temple-Smith, M.; Sanci, L. Urinary tract infections in children: An overview of diagnosis and management. BMJ Paediatr. Open 2019, 3, e000487. [Google Scholar] [CrossRef]
- Ammenti, A.; Cataldi, L.; Chimenz, R.; Fanos, V.; La Manna, A.; Marra, G.; Materassi, M.; Pecile, P.; Pennesi, M.; Pisanello, L.; et al. Febrile urinary tract infections in young children: Recommendations for the diagnosis, treatment and follow-up. Acta Paediatr. 2012, 101, 451–457. [Google Scholar] [CrossRef]
- Alberici, I.; La Manna, A.; Pennesi, M.; Starc, M.; Scozzola, F.; Nicolini, G.; Toffolo, A.; Marra, G.; Chimenz, R.; Sica, F.; et al. First urinary tract infections in children: The role of the risk factors proposed by the Italian recommendations. Acta Paediatr. 2019, 108, 544–550. [Google Scholar] [CrossRef]
- Montini, G.; Rigon, L.; Zucchetta, P.; Fregonese, F.; Toffolo, A.; Gobber, D.; Cecchin, D.; Pavanello, L.; Molinari, P.P.; Maschio, F.; et al. Prophylaxis after first febrile urinary tract infection in children? A multicenter, randomized, controlled, noninferiority trial. Pediatrics 2008, 122, 1064–1071. [Google Scholar] [CrossRef]
- Edwards, A.; Peters, C.A. Managing vesicoureteral reflux in children: Making sense of all the data. F1000Res 2019, 8, F1000 Faculty Rev-29. [Google Scholar] [CrossRef]
- Capozza, N.; Gulia, C.; Heidari Bateni, Z.; Zangari, A.; Gigli, S.; Briganti, V.; Tursini, S.; Koh, C.J.; Gaffi, M.; Baldassarra, S.; et al. Vesicoureteral reflux in infants: What do we know about the gender prevalence by age? Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5321–5329. [Google Scholar]
- Mattoo, T.K.; Carpenter, M.A.; Moxey-Mims, M.; Chesney, R.W. The RIVUR trial: A factual interpretation of our data. Pediatr. Nephrol. 2015, 30, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Morris, B.J.; Wiswell, T.E. Circumcision and lifetime risk of urinary tract infection: A systematic review and meta-analysis. J. Urol. 2013, 189, 2118–2124. [Google Scholar] [CrossRef] [PubMed]
- Megged, O.; Koriat, Y. The prevalence of vesicoureteral reflux in infants with first urinary tract infection following circumcision is similar to infants with UTI not the following circumcision. Int. Urol. Nephrol. 2020, 52, 417–422. [Google Scholar] [CrossRef]
- Singh-Grewal, D.; Macdessi, J.; Craig, J. Circumcision for the prevention of urinary tract infection in boys: A systematic review of randomised trials and observational studies. Arch. Dis. Child 2005, 90, 853–858. [Google Scholar] [CrossRef]
- Bulum, B.; Özçakar, Z.B.; Kavaz, A.; Hüseynova, M.; Ekim, M.; Yalçinkaya, F. Lower urinary tract dysfunction is frequently seen in urinary tract infections in children and is often associated with reduced quality of life. Acta Paediatr. 2014, 103, e454–e458. [Google Scholar] [CrossRef] [PubMed]
- Tekgul, S.; Stein, R.; Bogaert, G.; Undre, S.; Nijman, R.J.M.; Quaedackers, J.; ‘t Hoen, L.; Kocvara, R.; Silay, M.S.; Radmayr, C.; et al. EAU-ESPU guidelines recommendations for daytime lower urinary tract conditions in children. Eur. J. Pediatr. 2020, 179, 1069–1077. [Google Scholar] [CrossRef]
- Koff, S.A.; Wagner, T.T.; Jayanthi, V.R. The relationship among dysfunctional elimination syndromes, primary vesicoureteral reflux and urinary tract infections in children. J. Urol. 1998, 160 Pt 2, 1019–1022. [Google Scholar] [CrossRef] [PubMed]
- Maternik, M.; Krzeminska, K.; Zurowska, A. The management of childhood urinary incontinence. Pediatr. Nephrol. 2015, 30, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Robson, W.L.; Leung, A.K.; Van Howe, R. Primary and secondary nocturnal enuresis: Similarities in presentation. Pediatrics 2005, 115, 956–959. [Google Scholar] [CrossRef]
- Gondim, R.; Azevedo, R.; Braga, A.; Veiga, M.L.; Barroso, U., Jr. Risk factors for urinary tract infection in children with urinary urgency. Int. Braz. J. Urol. 2018, 44, 378–383. [Google Scholar] [CrossRef]
- Shaikh, N.; Hoberman, A.; Keren, R.; Gotman, N.; Docimo, S.G.; Mathews, R.; Bhatnagar, S.; Ivanova, A.; Mattoo, T.K.; Moxey-Mims, M.; et al. Recurrent Urinary Tract Infections in Children with Bladder and Bowel Dysfunction. Pediatrics 2016, 137, e20152982. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall n = 948 | APN n = 548 | CYS n = 400 | APN vs. CYS p | |
|---|---|---|---|---|
| Girls, Boys, n | 531; 417 | 331; 217 | 200; 200 | 0.00014 * |
| Age at the onset of the UTI (months) (median (IQR) | 12.0 (5.0–48.0) girls: 17 (7–65) boys: 7 (3–28) | 10 (4–25) | 23.5 (5–84.5) | <0.0001 * |
| Age category (n, %) | ||||
| 0–2 years, n (%) girls, n (%) | 611 (64.4%) 304 (49.8%) | 410 (43.2%) 228 (55.6%) | 201 (21.2%) 76 (37.8%) | <0.0001 * |
| 0–1 year girls, n (%) | 486 212 (43.6%) | 318 157 (49.4%) | 168 55 (32.7%) | |
| >2–7 years, n (%) girls, n (%) | 196 (20.7%) 135 (68.9%) | 97 75 (77.3%) | 99 60 (60.6%) | |
| >7 years, n (%) girls, n (%) | 141 (14.9%) 92 (65.3%) | 41 28 (68.3%) | 100 64 (64.0%) | |
| Clinical presentation (n, %) | ||||
| Fever ≥ 38° | 601 (63.4%) | 548 (100%) | 53 (13.2%) | <0.0001 * |
| Loss of appetite | 170 (17.9%) | 124 (22.6%) | 46 (11.5%) | <0.0001 * |
| Abdominal pain | 135 (14.2%) | 80 (14.6%) | 55 (13.8%) | 0.7120 |
| Dysuria | 107 (11.3%) | 48 (8.76%) | 59 (14.8%) | 0.0040 * |
| Loose stools | 107 (11.3%) | 69 (12.6%) | 38 (9.5%) | 0.1374 |
| Vomiting | 107 (11.2%) | 91 (16.6%) | 16 (4%) | <0.001 * |
| Lethargy | 64 (6.7%) | 47 (8.6%) | 17 (4.4%) | 0.0087 * |
| Positive Goldflam’s symptom | 33 (3.5%) | 33 (6%) | - | ** |
| Haematuria | 15 (1.6%) | 4 (0.7%) | 11 (2.8%) | 0.0138 * |
| Seizures | 10 (1.1%) | 9 (1.6%) | 1 (0.25%) | 0.0382 * |
| Laboratory data (median, IQR) | ||||
| WBC (×103/μL) | 17.6 (14.3–19.8) | 17.3 (12.5–22.1) | 11.21 (8.4–14.7) | <0.0001 * |
| Neutrophils (%) | 51.2 (35.0–65.3) | 55.85 (43.8–67.8) | 40.6 (26.8–57.0) | <0.0001 * |
| CRP (mg/dL) | 3.85 (0.9–8.3) | 6.95 (3.8–15.3) | 0.85 (0.5–2.1) | <0.0001 * |
| Children with UTIs | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patients | Overall | APN | CYS | p | 0–2 years | >2–7 years | >7 years | |||
| n | 948 | 548 | 400 | 611 | 196 | 141 | ||||
| APN 410 | CYS 201 | APN 97 | CYS 99 | APN 41 | CYS 100 | |||||
| Risk factors, n (%) girls, n | 442 (46.6%) 225 | 195 (35.6%) 117 | 247 (61.7%) 108 | <0.0001 * | 202 | 138 | 102 | |||
| CAKUT, n (%) girls, n | 248 (26.2%) 108 | 123 (22.4%) 67 | 125 (31.2%) 41 | 0.0023 * | 159 (26.0%) | 58 (29.6%) | 31 (22.0%) | |||
| Neurogenic bladder, n (%) girls, n | 54 (5.7%) 24 | 10 (1.8%) 6 | 44 (11.0%) 26 | <0.0001 * | 5 (0.8%) | 20 (10.2%) | 29 (20.6%) | |||
| Constipation, n (%) girls, n | 53 (5.6%) 33 | 34 (6.2%) 16 | 29 (7.2%) 17 | 0.0575 | 17 (2.8%) | 21 (10.7%) | 15 (10.6%) | |||
| Bladder dysfunction, n (%) girls, n | 45 (4.7%) 25 | 19 (3.5%) 14 | 26 (6.5%) 11 | 0.0301 * | 15 (2.4%) | 21 (10.7%) | 9 (6.4%) | |||
| Immunosuppressive drugs, n (%) girls, n | 21 (2.2%) 17 | 9 (1.6%) 8 | 12 (3.0%) 9 | 0.3698 | 1 (0.2%) | 12 (6.1%) | 8 (5.7%) | |||
| Urolithiasis, n (%) girls, n | 11 (1.2%) 7 | 5 (0.9%) 4 | 6 (1.5%) 3 | 0.3610 | 4 (0.6%) | 5 (2.5%) | 2 (1.4%) | |||
| Diabetes mellitus, n (%) girls, n | 10 (1.0%) 7 | 5 (0.9%) 3 | 5 (1.2%) 4 | 0.6153 | 1 (0.2%) | 1 (0.5%) | 8 (5.7%) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daniel, M.; Szymanik-Grzelak, H.; Sierdziński, J.; Podsiadły, E.; Kowalewska-Młot, M.; Pańczyk-Tomaszewska, M. Epidemiology and Risk Factors of UTIs in Children—A Single-Center Observation. J. Pers. Med. 2023, 13, 138. https://doi.org/10.3390/jpm13010138
Daniel M, Szymanik-Grzelak H, Sierdziński J, Podsiadły E, Kowalewska-Młot M, Pańczyk-Tomaszewska M. Epidemiology and Risk Factors of UTIs in Children—A Single-Center Observation. Journal of Personalized Medicine. 2023; 13(1):138. https://doi.org/10.3390/jpm13010138
Chicago/Turabian StyleDaniel, Maria, Hanna Szymanik-Grzelak, Janusz Sierdziński, Edyta Podsiadły, Magdalena Kowalewska-Młot, and Małgorzata Pańczyk-Tomaszewska. 2023. "Epidemiology and Risk Factors of UTIs in Children—A Single-Center Observation" Journal of Personalized Medicine 13, no. 1: 138. https://doi.org/10.3390/jpm13010138
APA StyleDaniel, M., Szymanik-Grzelak, H., Sierdziński, J., Podsiadły, E., Kowalewska-Młot, M., & Pańczyk-Tomaszewska, M. (2023). Epidemiology and Risk Factors of UTIs in Children—A Single-Center Observation. Journal of Personalized Medicine, 13(1), 138. https://doi.org/10.3390/jpm13010138