
Building Capacity for Implementation Science in Precision Health and Society: Development of a Course for Professional and Graduate Students in Pharmacy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Course Description
- 1.
- Define implementation science.
- 2.
- Define precision health.
- 3.
- Summarize common challenges to the implementation of precision health in pharmacy practice.
- 4.
- Identify and describe implementation science frameworks, models, and theories that can be used to promote implementation of precision health in pharmacy practice.
- 5.
- Apply an implementation science framework, model, or theory to guide how one would tackle an implementation challenge.
- 6.
- Define and describe how implementation strategies can be employed to translate precision health into practice.
- 7.
- Select implementation strategies to overcome an implementation challenge in precision health research or pharmacy practice.
- 8.
- Describe the types of study design that are commonly used by implementation scientists.
- 9.
- List and define implementation science outcomes that can be measured to evaluate implementation.
- 10.
- Select which implementation outcomes could be measured to better understand the implementation of precision health in pharmacy practice.
- 11.
- Apply implementation science principles to a challenge in pharmacy practice or research.
- 12.
- Use implementation science to solve practice problems and/or to answer research questions.
2.2. Grading
2.3. Course Evaluation Metrics
3. Results
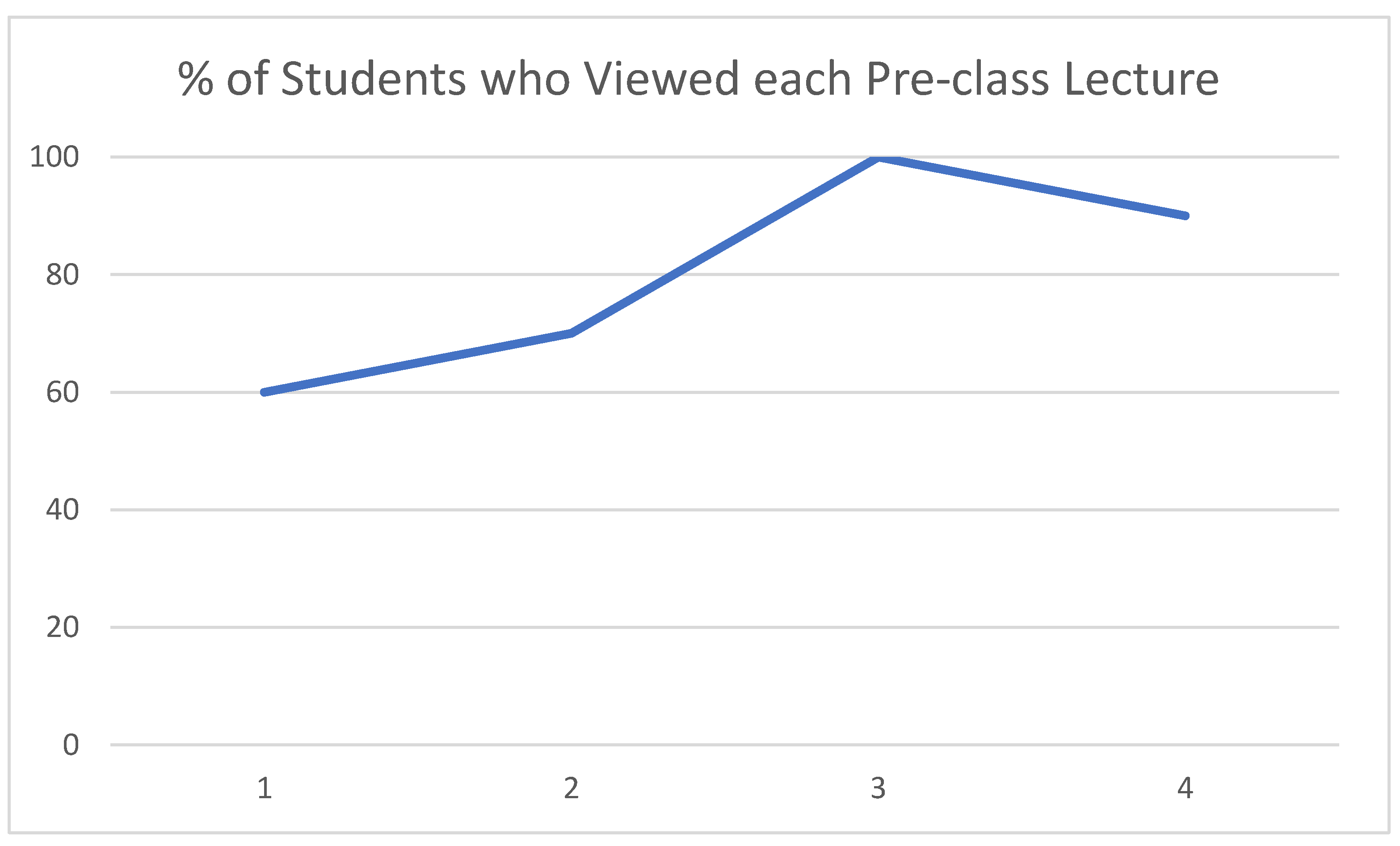
3.1. Engagement
3.2. Learning
3.3. Process

{kind=link}
| Evaluation Item [never, 1, to always, 5] | Overall | Section 1 | Section 2 | p | |||
|---|---|---|---|---|---|---|---|
| n = 17 | n = 10 | n = 7 | |||||
| Mean | Median | Mean | Median | Mean | Median | ||
| This course was well organized. | 4.71 | 5.00 | 4.60 | 5.00 | 4.86 | 5.00 | 0.57 |
| The in-class activities/exercises contributed to my learning. | 4.35 | 4.00 | 4.30 | 4.50 | 4.43 | 4.00 | 0.70 |
| The assessments were clearly connected to the course outcomes. | 4.50 | 5.00 | 4.30 | 5.00 | 4.83 | 5.00 | 0.26 |
| This course challenged me to think deeply about the subject matter. | 4.12 | 4.00 | 3.80 | 4.00 | 4.57 | 5.00 | 0.046 |
| Overall rating [poor, 1, to excellent, 5] | 3.59 | 4.00 | 3.50 | 4.00 | 3.71 | 4.00 | 0.57 |
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allen, C.G.; Fohner, A.E.; Landry, L.; Paul, J.; Smith, S.G.; Turbitt, E.; Roberts, M.C. Early career investigators and precision public health. Lancet Lond. Engl. 2019, 394, 382–383. [Google Scholar] [CrossRef]
- Allen, C.G.; Fohner, A.E.; Landry, L.; Paul, J.L.; Smith, S.G.; Turbitt, E.; Roberts, M.C. Perspectives from Early Career Investigators Who Are “Staying in the Game” of Precision Public Health Research. Am. J. Public Health 2019, 109, 1186–1187. [Google Scholar] [CrossRef] [PubMed]
- Seaton, T.L. Dissemination and implementation sciences in pharmacy: A call to action for professional organizations. Res. Soc. Adm. Pharm. 2017, 13, 902–904. [Google Scholar] [CrossRef] [PubMed]
- Curran, G.M.; Shoemaker, S.J. Advancing pharmacy practice through implementation science. Res. Soc. Adm. Pharm. 2017, 13, 889–891. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.C.; Fohner, A.E.; Landry, L.; Olstad, D.L.; Smit, A.K.; Turbitt, E.; Allen, C.G. Advancing precision public health using human genomics: Examples from the field and future research opportunities. Genome Med. 2021, 13, 97. [Google Scholar] [CrossRef] [PubMed]
- Persky, A.M.; McLaughlin, J.E. The Flipped Classroom—From Theory to Practice in Health Professional Education. Am. J. Pharm. Educ. 2017, 81, 118. [Google Scholar] [CrossRef] [PubMed]
- DeLozier, S.J.; Rhodes, M.G. Flipped Classrooms: A Review of Key Ideas and Recommendations for Practice. Educ. Psychol. Rev. 2017, 29, 141–151. [Google Scholar] [CrossRef]
- Angelo, T.A.; Cross, K.P. Classroom Assessment Techniques: A Handbook for College Teachers, 2nd ed.; Wiley: Hoboken, NJ, USA, 1993. [Google Scholar]
- Chair, G.K.; Bacci, J.L.; Chui, M.A.; Farley, J.; Gannett, P.M.; Holstad, S.G.; Livet, M.; Farrell, D. Implementation Science to Advance Practice and Curricular Transformation: Report of the 2019-2020 AACP Research and Graduate Affairs Committee. Am. J. Pharm. Educ. 2020, 84, ajpe848204. [Google Scholar] [CrossRef] [PubMed]
- Garza, K.B.; Abebe, E.; Bacci, J.L.; Kunda, N.K.; Lor, K.B.; Rickles, N.; Shankar, N.; Farrell, D. Building Implementation Science Capacity in Academic Pharmacy: Report of the 2020-2021 AACP Research and Graduate Affairs Committee. Am. J. Pharm. Educ. 2021, 85, 8718. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, R.; Mosnier, J.; Reed, K.; Powell, B.J.; Schenck, A.P. Building capacity for Public Health 3.0: Introducing implementation science into an MPH curriculum. Implement. Sci. 2019, 14, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estabrooks, P.A.; Brownson, R.C.; Pronk, N.P. Dissemination and Implementation Science for Public Health Professionals: An Overview and Call to Action. Prev. Chronic. Dis. 2018, 15, E162. [Google Scholar] [CrossRef] [PubMed]
- McNett, M.; Masciola, R.; Sievert, D.; Tucker, S. Advancing Evidence-Based Practice Through Implementation Science: Critical Contributions of Doctor of Nursing Practice- and Doctor of Philosophy-Prepared Nurses. Worldviews Evid. Based Nurs. 2021, 18, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Boehm, L.M.; Stolldorf, D.P.; Jeffery, A.D. Implementation Science Training and Resources for Nurses and Nurse Scientists. J. Nurs. Scholarsh. 2020, 52, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Bertram, R.M.; Choi, S.-W.; Elsen, M. Integrating Implementation Science and Evidence-Based Practice into Academic and Field Curricula. J. Soc. Work Educ. 2018, 54, S20–S30. [Google Scholar] [CrossRef]

| Strengths | Exemplar Quotes |
|---|---|
| Structure: guest speakers (n = 11) | The course brought in a lot of experts in the field to talk about their research and experience in the field. They brought in new points of view that kept the class changing. |
| Foundational nature (n = 5) | The course introduced implementation science, a fresh area to me, and the research methods introduced in class could help me conduct research on pharmacy practice/health service. |
| Structure: introduction to new material to application (n = 2) | I really liked how the course was structured, especially with the focus on foundational topics at the beginning, and then transitioning to application of those topics later in the course. |
| Structure: class cases (n = 10) | I feel like I learned a lot in this class. Some of the concepts are still a little abstract to me but I think I have built a foundation on what is implementation science. I like the in class cases as they allowed me to really put in the work and understand the class materials in a more applicable way. |
| Structure: pre-course materials (n = 8) | I appreciate that the course introduced us to various health science disciplines so that we could understand how implementation science informs research across different disciplines. I also found the pre–class modules to be helpful in teaching me important foundational concepts prior to class. |
| Structure: pre-course materials (quizzes) (n = 1) | …the quizzes at the end of each video are good ways to check my knowledge. |
| Structure: QA (n = 2) | I liked the group discussions on the various topics. |
| Structure: course-long project (n = 1) | I like how we worked on the project throughout the course of the semester. It made it very valuable to continue learning and applying knowledge. |
| Weaknesses | |
| Order of concepts: frameworks later (n = 5) | I think some of the course information could have been re–ordered to make the material easier to understand. I think leading with the more abstract principals like frameworks before discussing how they’re applied can be confusing. |
| Linking IS concepts (n = 1) | ...the course did not do a good job of linking the different topics together until later in the semester so a majority of the time I was a little lost. |
| Linking guest speaker content to pre-class material (n = 3) | Hard to apply the guest speaker information into the context of the class. |
| Preparation of guest speakers (n = 1) | I felt like some of the presenters who came in were not really prepared to present |
| IS terminology (n = 3) | Sometimes I knew what words I was supposed to use in the class, but I had no idea what that meant in practice. |
| PowerPoints for pre-class videos available (n = 2) | I would have liked the lecture slides from the pre–class videos to be available on sakai. |
| Pre-class self quiz banks (n = 2) | For the first 3–4 quizzes, the pre–class material did not give feedback on the assessment. [Block 1] |
| Shorter class period (n = 2) | I felt like the length of the class period partially hindered learning. It was difficult to stay engaged for the full 2.5 h. |
| Make course a full semester (n = 1) | I think having this course throughout a full semester would help because this is a very broad subject and can be very specialized, so it’s hard to learn in a few weeks. |
| More discussion of cases (n = 1) | I would like more case discussion and more deep explanations about the research methods, especially the qualitative research. |
| More practice before cases (n = 1) | Some of the in–class exercises felt abstract… maybe because we had just learned the material. |
| Move pharmacy-specific guest lectures to beginning (n = 1) | I think it might be beneficial for students if the guest lectures in the beginning of the course are more focused to the intersection between implementation science and pharmacists. |
| No need for longer guest speaker seminars at end of Block 1 (n = 1) | The long [guest] lectures in the last 3 weeks didn’t help much. |
| Move cases and speakers to second half of block (n = 1) | think that the course needs to focus on learning the basics for the first half of the semester then bring in the case reports and guest speakers. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roberts, M.C.; McLaughlin, J.E. Building Capacity for Implementation Science in Precision Health and Society: Development of a Course for Professional and Graduate Students in Pharmacy. J. Pers. Med. 2022, 12, 1499. https://doi.org/10.3390/jpm12091499
Roberts MC, McLaughlin JE. Building Capacity for Implementation Science in Precision Health and Society: Development of a Course for Professional and Graduate Students in Pharmacy. Journal of Personalized Medicine. 2022; 12(9):1499. https://doi.org/10.3390/jpm12091499
Chicago/Turabian StyleRoberts, Megan C., and Jacqueline E. McLaughlin. 2022. "Building Capacity for Implementation Science in Precision Health and Society: Development of a Course for Professional and Graduate Students in Pharmacy" Journal of Personalized Medicine 12, no. 9: 1499. https://doi.org/10.3390/jpm12091499
APA StyleRoberts, M. C., & McLaughlin, J. E. (2022). Building Capacity for Implementation Science in Precision Health and Society: Development of a Course for Professional and Graduate Students in Pharmacy. Journal of Personalized Medicine, 12(9), 1499. https://doi.org/10.3390/jpm12091499