
Impella RP for Patients with Acute Right Ventricular Failure and Cardiogenic Shock: A Subanalysis from the IMP-IT Registry

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Patient Population and Baseline Characteristics
3.2. Procedural Characteristics
3.3. In-Hospital Outcomes
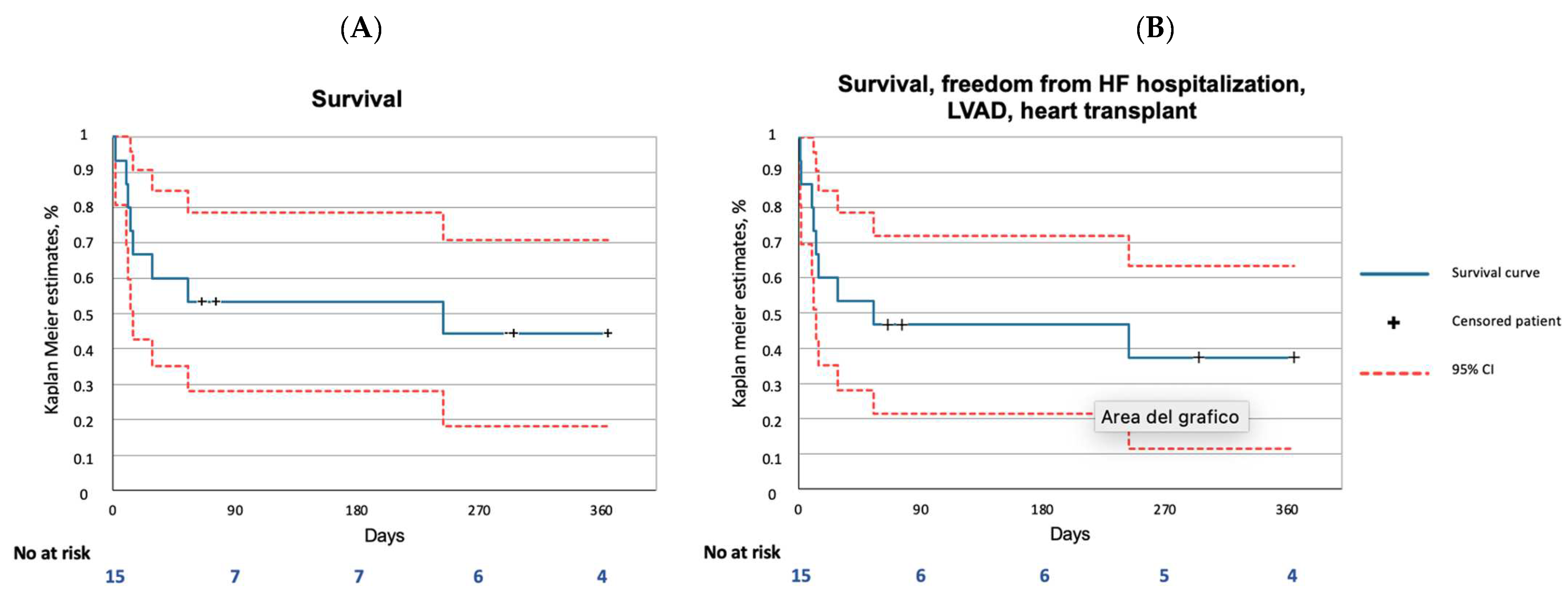
3.4. One-Year Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Description of the Impella RP Device
Appendix B. Study Endpoints and Definitions
- −
- Stroke is defined as the duration of a focal or global neurological deficit ≥24 h; or <24 h if the available neuroimaging documents a new hemorrhage or infarct or if the neurological deficit results in death.
- −
- Transient ischemic attack is defined as the duration of a focal or global neurological deficit <24 h; any variable neuroimaging does not demonstrate a new hemorrhage or infarct.
References
- Shah, M.; Patnaik, S.; Patel, B.; Ram, P.; Garg, L.; Agarwal, M.; Agrawal, S.; Arora, S.; Patel, N.; Wald, J.; et al. Trends in mechanical circulatory support use and hospital mortality among patients with acute myocardial infarction and non-infarction related cardiogenic shock in the United States. Clin. Res. Cardiol. 2017, 107, 287–303. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, M.K.; Everett, K.D.; Gulati, G.; Brener, M.I.; Kapur, N.K. Epidemiology and management of right ventricular-predominant heart failure and shock in the cardiac intensive care unit. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Chieffo, A.; Dudek, D.; Hassager, C.; Combes, A.; Gramegna, M.; Halvorsen, S.; Huber, K.; Kunadian, V.; Maly, J.; Møller, J.E.; et al. Joint EAPCI/ACVC expert consensus document on percutaneous ventricular assist devices. EuroIntervention 2021, 17, e274–e286. [Google Scholar] [CrossRef] [PubMed]
- Garan, A.R.; Kanwar, M.; Thayer, K.L.; Whitehead, E.; Zweck, E.; Hernandez-Montfort, J.; Mahr, C.; Haywood, J.L.; Harwani, N.M.; Wencker, D.; et al. Complete Hemodynamic Profiling With Pulmonary Artery Catheters in Cardiogenic Shock Is Associated With Lower In-Hospital Mortality. JACC Heart Fail. 2020, 8, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.B.; Goldstein, J.; Milano, C.; Morris, L.D.; Kormos, R.L.; Bhama, J.; Kapur, N.K.; Bansal, A.; Garcia, J.; Baker, J.N.; et al. Benefits of a novel percutaneous ventricular assist device for right heart failure: The prospective RECOVER RIGHT study of the Impella RP device. J. Heart Lung Transplant. 2015, 34, 1549–1560. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.; Morris, D.L.; Tang, D.; Batsides, G.; Kirtane, A.; Hanson, I.; Meraj, P.; Kapur, N.K.; O’Neill, W. Outcomes of patients with right ventricular failure requiring short-term hemodynamic support with the Impella RP device. J. Heart Lung Transplant. 2018, 37, 1448–1458. [Google Scholar] [CrossRef] [PubMed]
- Aurigemma, C.; Burzotta, F.; Chieffo, A.; Briguori, C.; Piva, T.; De Marco, F.; Di Biasi, M.; Pagnotta, P.; Casu, G.; Garbo, R.; et al. Clinical Impact of Revascularization Extent in Patients Undergoing Impella-Protected PCI Enrolled in a Nationwide Registry. JACC Cardiovasc. Interv. 2021, 14, 717–719. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Masiero, G.; Burzotta, F.; Pazzanese, V.; Briguori, C.; Trani, C.; Piva, T.; De Marco, F.; Di Biasi, M.; Pagnotta, P.; et al. Timing of Impella implantation and outcomes in cardiogenic shock or high-risk percutaneous coronary revascularization. Catheter. Cardiovasc. Interv. 2021, 98, E222–E234. [Google Scholar] [CrossRef] [PubMed]
- Ancona, M.B.; Montorfano, M.; Masiero, G.; Burzotta, F.; Briguori, C.; Pagnesi, M.; Pazzanese, V.; Trani, C.; Piva, T.; De Marco, F.; et al. Device-related complications after Impella mechanical circulatory support implantation: An IMP-IT observational multicentre registry substudy. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Chieffo, A.; Ancona, M.B.; Burzotta, F.; Pazzanese, V.; Briguori, C.; Trani, C.; Piva, T.; De Marco, F.; Di Biasi, M.; Pagnotta, P.; et al. Observational multicentre registry of patients treated with IMPella mechanical circulatory support device in Italy: The IMP-IT registry. EuroIntervention 2020, 15, e1343–e1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, J.A.; Kern, M.J. Percutaneous Mechanical Support for the Failing Right Heart. Cardiol. Clin. 2012, 30, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.; Doyle, R.; Murphy, D.J.; Hunt, S.A. Right Ventricular Function in Cardiovascular Disease, Part II. Circulation 2008, 117, 1717–1731. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Randhawa, V.K.; Hoffman, K.; Bock, A.; Bhat, P.; Young, L.; Rossi, J.; Campbell, J.; Bott-Silverman, C.; Soltesz, E.G.; Tong, M.Z.; et al. Impella RP as a bridge to cardiac transplant for refractory late right ventricular failure in setting of left ventricular assist device. ESC Heart Fail. 2020, 7, 1972–1975. [Google Scholar] [CrossRef]
- Monteagudo-Vela, M.; Simon, A.; Panoulas, V. Initial experience with Impella RP in a quaternary transplant center. Artif. Organs 2020, 44, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.B.; Kann, S.H.; Veien, K.T.; Møller-Helgestad, O.K.; Dahl, J.; Rud, C.S.; Jensen, M.K.; Jensen, L.O.; Schmidt, H.; Møller, J.E. Single-centre experience with the Impella CP, 5.0 and RP in 109 consecutive patients with profound cardiogenic shock. Eur. Heart J. Acute Cardiovasc. Care 2017, 7, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Zuin, M.; Rigatelli, G.; Daggubati, R.; Nguyen, T.; Roncon, L. Impella RP in hemodynamically unstable patients with acute pulmonary embolism. J. Artif. Organs 2020, 23, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Gramegna, M.; Beneduce, A.; Bertoldi, L.F.; Pagnesi, M.; Marini, C.; Pazzanese, V.; Camici, P.G.; Chieffo, A.; Pappalardo, F. Impella RP support in refractory right ventricular failure complicating acute myocardial infarction with unsuccessful right coronary artery revascularization. Int. J. Cardiol. 2020, 302, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Josiassen, J.; Helgestad, O.K.L.; Udesen, N.L.J.; Banke, A.; Frederiksen, P.H.; Schmidt, H.; Jensen, L.O.; Hassager, C.; Møller, J.E.; Ravn, H.B. Impella RP Versus Pharmacologic Vasoactive Treatment in Profound Cardiogenic Shock due to Right Ventricular Failure. J. Cardiovasc. Transl. Res. 2021, 14, 1021–1029. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patients (n = 15) | |
|---|---|
| Age | 67.8 ± 14.4 |
| Male | 10 (66.7) |
| Hypertension | 8 (53.3) |
| Dyslipidaemia | 5 (33.3) |
| Diabetes mellitus | 3 (20.0) |
| Chronic pulmonary disease | 4 (26.7) |
| Prior myocardial infarction | 3 (20.0) |
| Previous percutaneous coronary intervention | 5 (33.3) |
| Previous coronary artery bypass graft | - |
| Chronic kidney disease * | 4 (26.7) |
| Dialysis | 2 (13.3) |
| Atrial fibrillation | 4 (26.7) |
| Prior transient ischaemic attack or stroke | 2 (13.3) |
| Peripheral artery disease | 1 (6.7) |
| Chronic heart failure | 2 (13.3) |
| Left ventricular ejection fraction, % | 32.9 ± 13.7 |
| Right ventricular dysfunction | 15 (100) |
| Out-of-hospital cardiac arrest | 2 (13.3) |
| Aetiology of cardiogenic shock | |
| ST-elevation myocardial infarction | 6 (40.0) |
| Acute myocarditis | 2 (13.3) |
| Other | 7 (46.7) |
| Haemodynamic Values | |
| Heart rate, bpm | 85.9 ± 25.0 |
| Mean arterial pressure, mmHg | 65.2 ± 11.2 |
| Laboratory values | |
| pH | 7.34 ± 0.1 |
| Serum lactate, mmol/L | 5.1 ± 3.9 |
| Haemoglobin, g/dL | 12.2 ± 2.0 |
| Serum creatinine, mg/dL | 2.1 ± 1.2 |
| Other Concomitant pVAD | Patients (n = 15) |
|---|---|
| Isolated Impella RP | 9 (60.0) |
| Impella RP + left-side Impella (BiPELLA) | 6 (40.0) |
| Impella 2.5 | 2 (13.3) |
| Impella CP | 4 (26.7) |
| Impella 5.0 | - |
| Intra-aortic balloon pump | 7 (46.7) |
| Inotropes | 7 (46.7) |
| Mechanical ventilation | 13 (86.7) |
| Duration of Impella support, hours | 156.0 ± 92.1 |
| Length of mechanical ventilation, hours | 96 (48–252) |
| Intensive care length of stay, days | 15 (10–27) |
| Patients (n = 8) | |
|---|---|
| Coronary angiography performed | 8 (53.3) |
| PCI performed | 5 (33.3) |
| Left main disease | 1 (6.7) |
| Left anterior descending artery disease | 3 (20.0) |
| Left circumflex disease | 3 (20.0) |
| Right coronary artery disease | 6 (40.0) |
| Number of diseased vessels | 1.1 ± 1.2 |
| Three-vessel disease | 2 (13.3) |
| Patients (n = 15) | |
|---|---|
| Death | 7 (46.7) |
| Life-threatening or severe bleeding | - |
| Number of red blood cell transfusions | 8.79 ± 9.6 |
| Device-related complications | |
| Access-site bleeding | - |
| Haemolysis | 4 (26.6) |
| Limb ischaemia | 3 (20.0) |
| Sepsis | 9 (60.0) |
| Acute kidney injury * | 10 (66.7) |
| Need for renal replacement therapy | 7 (46.7) |
| Escalation therapy | 2 (13.3) |
| LVEF at discharge, % | 35.8 ± 17.7 |
| Patients (n = 15) | |
|---|---|
| All-cause death | 8 (53.33) |
| Cardiac death | 8 (53.3) |
| Hospitalisation for heart failure | - |
| Myocardial infarction | - |
| Stroke | 2 (13.3) |
| LVAD or heart transplant | 1 (6.7) |
| Death, hospitalization for heart failure, LVAD or heart transplant | 9 (60.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botti, G.; Gramegna, M.; Burzotta, F.; Masiero, G.; Briguori, C.; Trani, C.; Napodano, M.; Scandroglio, A.M.; Montorfano, M.; Tarantini, G.; et al. Impella RP for Patients with Acute Right Ventricular Failure and Cardiogenic Shock: A Subanalysis from the IMP-IT Registry. J. Pers. Med. 2022, 12, 1481. https://doi.org/10.3390/jpm12091481
Botti G, Gramegna M, Burzotta F, Masiero G, Briguori C, Trani C, Napodano M, Scandroglio AM, Montorfano M, Tarantini G, et al. Impella RP for Patients with Acute Right Ventricular Failure and Cardiogenic Shock: A Subanalysis from the IMP-IT Registry. Journal of Personalized Medicine. 2022; 12(9):1481. https://doi.org/10.3390/jpm12091481
Chicago/Turabian StyleBotti, Giulia, Mario Gramegna, Francesco Burzotta, Giulia Masiero, Carlo Briguori, Carlo Trani, Massimo Napodano, Anna Mara Scandroglio, Matteo Montorfano, Giuseppe Tarantini, and et al. 2022. "Impella RP for Patients with Acute Right Ventricular Failure and Cardiogenic Shock: A Subanalysis from the IMP-IT Registry" Journal of Personalized Medicine 12, no. 9: 1481. https://doi.org/10.3390/jpm12091481
APA StyleBotti, G., Gramegna, M., Burzotta, F., Masiero, G., Briguori, C., Trani, C., Napodano, M., Scandroglio, A. M., Montorfano, M., Tarantini, G., & Chieffo, A., on behalf of IMP IT Investigators. (2022). Impella RP for Patients with Acute Right Ventricular Failure and Cardiogenic Shock: A Subanalysis from the IMP-IT Registry. Journal of Personalized Medicine, 12(9), 1481. https://doi.org/10.3390/jpm12091481