
Effectiveness of Artificial Intelligence Methods in Personalized Aggression Risk Prediction within Inpatient Psychiatric Treatment Settings—A Systematic Review



Abstract
1. Introduction
2. Methodology
2.1. Problem Formulation
- What is the predictive accuracy for aggression risk prediction amongst psychiatric inpatients using artificial intelligence methods?
- What are the associated clinical variables identified in predicting aggression risk amongst psychiatric inpatients?
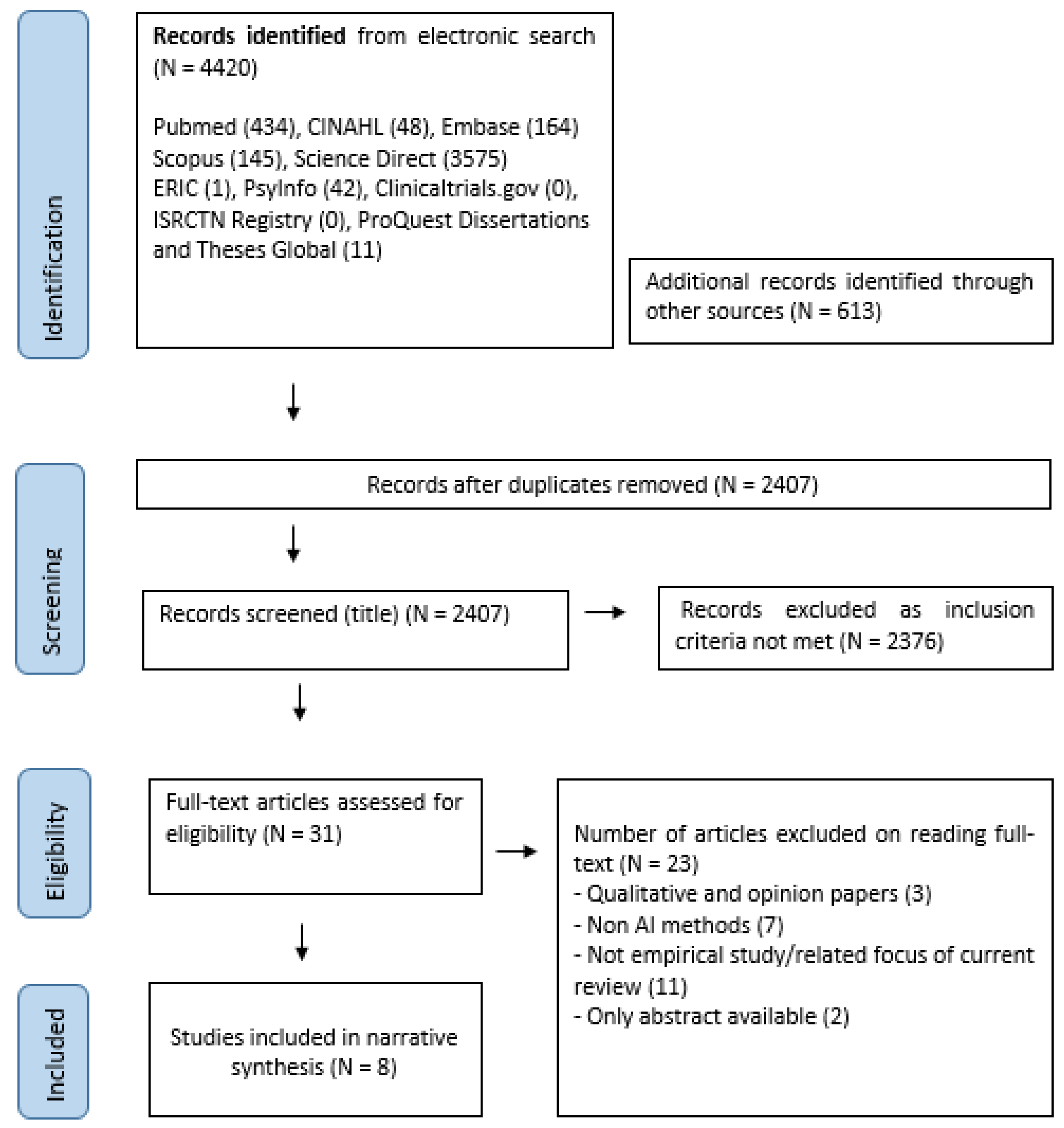
2.2. Data Collection
2.3. Evaluation (Study Selection and Quality Assessment)
2.4. Data Analysis and Interpretation
3. Results
3.1. General Features of Included Studies
3.2. Preparation of Data Points and Process in AI Modelling
3.3. Accuracy of Artificial Intelligence Methods in Predicting Aggression Risk and Relevant Variables
3.4. Relevant Clinical Variables in Predicting Aggression Risk Amongst Psychiatric Inpatients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Bias | 1. Consecutive or Random Sampling | 2. Case Control Design Avoided | 3. Prevent Inappropriate Exclusions | 4. Interpret index Results without Knowledge of the Standard Results? | 5. Pre-specified Threshold Used | 6. Appropriateness of Reference Standard in Classifying Condition? | 7. Interpretation of Reference Results without Knowledge of Standard r? | 8. Ideal Interval between Index and Reference Results? | 9. Same Reference Results for All Patients? | 10. Inclusion of All Patients in Analysis | Total Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Authors | ||||||||||||
| Goodwin et al., 2019 | + | ++ | + | + | NA | + | + | + | + | ++ | 2 | |
| Gunther et al., 2020 | + | - | + | + | NA | + | + | + | + | ++ | 1 | |
| Hofmann et al., 2022 | + | ++ | ++ | + | NA | + | + | + | ++ | ++ | 4 | |
| Menger et al., 2018 | ++ | - | ++ | + | NA | + | + | + | + | ++ | 3 | |
| Menger et al., 2019 | ++ | ++ | ++ | + | ++ | ++ | + | ++ | ++ | + | 7 | |
| Suchting et al., 2018 | ++ | - | ++ | + | NA | + | + | + | ++ | ++ | 4 | |
| Van Le et al., 2018 | ++ | + | ++ | + | ++ | ++ | + | ++ | ++ | ++ | 7 | |
| Wang et al., 2020 | + | ++ | ++ | + | ++ | + | + | + | ++ | ++ | 5 | |
| NA = not applicable; (-) = high risk; (+) = unclear risk, (++) = low risk | ||||||||||||
References
- Sariaslan, A.; Arseneault, L.; Larsson, H.; Lichtenstein, P.; Fazel, S. Risk of subjection to violence and perpetration of violence in persons with psychiatric disorders in Sweden. JAMA Psychiatry 2020, 77, 359–367. [Google Scholar] [CrossRef]
- Anderson, C.A.; Bushman, B.J. Human aggression. Annu. Rev. Psychol. 2002, 53, 27–51. [Google Scholar] [CrossRef] [PubMed]
- di Giacomo, E.; Iozzino, L.; Ferrari, C.; Strozza, C.; Large, M.; Nielssen, O.; de Girolamo, G. Prevalence and risk factors of violence by psychiatric acute inpatients: Systematic review and meta-analysis—A 2019 update. Violence Ment. Disord. 2020, 181–202. [Google Scholar]
- Richter, D.; Berger, K. Post-traumatic stress disorder following patient assaults among staff members of mental health hospitals: A prospective longitudinal study. BMC Psychiatry 2006, 6, 15. [Google Scholar] [CrossRef]
- Bizzarri, J.V.; Piacentino, D.; Kotzalidis, G.D.; Moser, S.; Cappelletti, S.; Weissenberger, G.; Pompili, M.; Conca, A. Aggression and violence toward healthcare workers in a psychiatric service in Italy: A retrospective questionnaire-based survey. J. Nerv. Ment. Dis. 2020, 208, 299–305. [Google Scholar] [CrossRef]
- Moylan, L.; Cullinan, M. Frequency of assault and severity of injury of psychiatric nurses in relation to the nurses’ decision to restrain. J. Psychiatr. Ment. Health Nurs. 2011, 18, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Kader, N.; Elhusein, B.; Elhassan, N.M.; Alabdulla, M.; Hammoudeh, S.; Hussein, N.-R. Burnout and job satisfaction among psychiatrists in the Mental Health Service, Hamad Medical Corporation, Qatar. Asian J. Psychiatry 2021, 58, 102619. [Google Scholar] [CrossRef] [PubMed]
- Seun-Fadipe, C.T.; Akinsulore, A.A.; Oginni, O.A. Workplace violence and risk for psychiatric morbidity among health workers in a tertiary health care setting in Nigeria: Prevalence and correlates. Psychiatry Res. 2019, 272, 730–736. [Google Scholar] [CrossRef]
- Ghosh, M.; Twigg, D.; Kutzer, Y.; Towell-Barnard, A.; De Jong, G.; Dodds, M. The validity and utility of violence risk assessment tools to predict patient violence in acute care settings: An integrative literature review. Int. J. Ment. Health Nurs. 2019, 28, 1248–1267. [Google Scholar] [CrossRef] [PubMed]
- Lorettu, L.; Nivoli, A.M.; Milia, P.; Nivoli, G. Violence risk assessment in mental health. In Violence and Mental Disorders; Springer: Berlin/Heidelberg, Germany, 2020; pp. 231–252. [Google Scholar]
- Scurich, N.; Monahan, J.; John, R.S. Innumeracy and unpacking: Bridging the nomothetic/idiographic divide in violence risk assessment. Law Hum. Behav. 2012, 36, 548. [Google Scholar] [CrossRef]
- Ramesh, T.; Igoumenou, A.; Montes, M.V.; Fazel, S. Use of risk assessment instruments to predict violence in forensic psychiatric hospitals: A systematic review and meta-analysis. Eur. Psychiatry 2018, 52, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Nielssen, O.; Paton, M.; Large, M. Clinical decisions in psychiatry should not be based on risk assessment. Australas. Psychiatry 2010, 18, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Chilla, G.S.; Yeow, L.Y.; Chew, Q.H.; Sim, K.; Prakash, K. Machine learning classification of schizophrenia patients and healthy controls using diverse neuroanatomical markers and Ensemble methods. Sci. Rep. 2022, 12, 2755. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Qian, X.; Liu, S.; Koh, A.J.; Sim, K.; Jiang, X.; Guan, C.; Zhou, J.H. Structural and diffusion MRI based schizophrenia classification using 2D pretrained and 3D naive Convolutional Neural Networks. Schizophr. Res. 2021, 243, 330–341. [Google Scholar] [CrossRef]
- Saeedi, A.; Saeedi, M.; Maghsoudi, A.; Shalbaf, A. Major depressive disorder diagnosis based on effective connectivity in EEG signals: A convolutional neural network and long short-term memory approach. Cogn. Neurodyn. 2021, 15, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Andersson, S.; Bathula, D.R.; Iliadis, S.I.; Walter, M.; Skalkidou, A. Predicting women with depressive symptoms postpartum with machine learning methods. Sci. Rep. 2021, 11, 7877. [Google Scholar] [CrossRef]
- Eder, S.J.; Steyrl, D.; Stefanczyk, M.M.; Pieniak, M.; Martínez Molina, J.; Pešout, O.; Binter, J.; Smela, P.; Scharnowski, F.; Nicholson, A.A. Predicting fear and perceived health during the COVID-19 pandemic using machine learning: A cross-national longitudinal study. PLoS ONE 2021, 16, e0247997. [Google Scholar]
- Zhou, M.; Wang, Q.; Zheng, C.; John Rush, A.; Volkow, N.D.; Xu, R. Drug repurposing for opioid use disorders: Integration of computational prediction, clinical corroboration, and mechanism of action analyses. Mol. Psychiatry 2021, 26, 5286–5296. [Google Scholar] [CrossRef]
- Large, M.; Nielssen, O. The limitations and future of violence risk assessment. World Psychiatry 2017, 16, 25. [Google Scholar] [CrossRef]
- Campbell, J.M.; Kulgar, M.; Ding, S.; Carmody, D.P.; Hakonsen, S.J.; Jadotte, Y.T.; WS, C. Diagnostic test accuracy systematic reviews. Joanna Briggs Inst. Rev. Manual. Joanna Briggs Inst. 2017. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/4687355/Chapter+9%3A+Diagnostic+test+accuracy+systematic+reviews (accessed on 1 May 2022).
- Cooper, H.M. Integrating Research: A Guide for Literature Reviews; Sage Publications, Inc: Newbury, UK, 1989. [Google Scholar]
- Joanna Briggs Institute. Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 1 March 2022).
- Suchting, R.; Green, C.E.; Glazier, S.M.; Lane, S.D. A data science approach to predicting patient aggressive events in a psychiatric hospital. Psychiatry Res. 2018, 268, 217–222. [Google Scholar] [CrossRef]
- Van Le, D.; Montgomery, J.; Kirkby, K.C.; Scanlan, J. Risk prediction using natural language processing of electronic mental health records in an inpatient forensic psychiatry setting. J. Biomed. Inform. 2018, 86, 49–58. [Google Scholar]
- Menger, V.; Spruit, M.; Van Est, R.; Nap, E.; Scheepers, F. Machine learning approach to inpatient violence risk assessment using routinely collected clinical notes in electronic health records. JAMA Netw. Open 2019, 2, e196709. [Google Scholar] [CrossRef]
- Menger, V.; Scheepers, F.; Spruit, M. Comparing deep learning and classical machine learning approaches for predicting inpatient violence incidents from clinical text. Appl. Sci. 2018, 8, 981. [Google Scholar] [CrossRef]
- Wang, K.Z.; Bani-Fatemi, A.; Adanty, C.; Harripaul, R.; Griffiths, J.; Kolla, N.; Gerretsen, P.; Graff, A.; De Luca, V. Prediction of physical violence in schizophrenia with machine learning algorithms. Psychiatry Res. 2020, 289, 112960. [Google Scholar] [CrossRef]
- Günther, M.P.; Kirchebner, J.; Lau, S. Identifying direct coercion in a high risk subgroup of offender patients with schizophrenia via machine learning algorithms. Front. Psychiatry 2020, 11, 415. [Google Scholar] [CrossRef]
- Hofmann, L.A.; Lau, S.; Kirchebner, J. Advantages of Machine Learning in Forensic Psychiatric Research—Uncovering the Complexities of Aggressive Behavior in Schizophrenia. Appl. Sci. 2022, 12, 819. [Google Scholar] [CrossRef]
- Goodwin, M.S.; Mazefsky, C.A.; Ioannidis, S.; Erdogmus, D.; Siegel, M. Predicting aggression to others in youth with autism using a wearable biosensor. Autism. Res. 2019, 12, 1286–1296. [Google Scholar] [CrossRef]
- Dietterich, T. Overfitting and undercomputing in machine learning. ACM Comput. Surv. 1995, 27, 326–327. [Google Scholar] [CrossRef]
- Kumar, R.; Indrayan, A. Receiver operating characteristic (ROC) curve for medical researchers. Indian Pediatrics 2011, 48, 277–287. [Google Scholar] [CrossRef]
- Hosmer Jr, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013; Volume 398, pp. 153–225. [Google Scholar]
- Passos, I.C.; Mwangi, B.; Cao, B.; Hamilton, J.E.; Wu, M.-J.; Zhang, X.Y.; Zunta-Soares, G.B.; Quevedo, J.; Kauer-Sant’Anna, M.; Kapczinski, F. Identifying a clinical signature of suicidality among patients with mood disorders: A pilot study using a machine learning approach. Journal of affective disorders 2016, 193, 109–116. [Google Scholar] [CrossRef]
- Rajkomar, A.; Oren, E.; Chen, K.; Dai, A.M.; Hajaj, N.; Hardt, M.; Liu, P.J.; Liu, X.; Marcus, J.; Sun, M. Scalable and accurate deep learning with electronic health records. NPJ Digit. Med. 2018, 1, 18. [Google Scholar] [CrossRef] [PubMed]
- Micciolo, R.; Bianconi, G.; Canal, L.; Clerici, M.; Ferla, M.T.; Giugni, C.; Iozzino, L.; Sbravati, G.; Tura, G.B.; Vita, A.; et al. Young age and the risk of violent behaviour in people with severe mental disorders: Prospective, multicentre study. BJPsych Open 2021, 8, e1. [Google Scholar] [CrossRef]
- Rueve, M.E.; Welton, R.S. Violence and mental illness. Psychiatry 2008, 5, 34–48. [Google Scholar] [PubMed]
- Tasmim, S.; Kolla, N.J.; Dada, O.; Bani-Fatemi, A.; De Luca, V. Correlation between violence and antipsychotic dosage in schizophrenia: A secondary analysis of the clinical antipsychotic trials for intervention effectiveness (CATIE) dataset. Pharmacopsychiatry 2019, 52, 217–221. [Google Scholar] [CrossRef]
- Swanson, J.W.; Swartz, M.S.; Van Dorn, R.A.; Elbogen, E.B.; Wagner, H.R.; Rosenheck, R.A.; Stroup, T.S.; McEvoy, J.P.; Lieberman, J.A. A national study of violent behavior in persons with schizophrenia. Arch. Gen. Psychiatry 2006, 63, 490–499. [Google Scholar] [CrossRef] [PubMed]
- d’Ettorre, G.; Pellicani, V. Workplace violence toward mental healthcare workers employed in psychiatric wards. Saf. Health Work. 2017, 8, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Nielssen, O.; Large, M. Rates of homicide during the first episode of psychosis and after treatment: A systematic review and meta-analysis. Schizophr. Bull. 2010, 36, 702–712. [Google Scholar] [CrossRef] [PubMed]
- Odawara, T.; Narita, H.; Yamada, Y.; Fujita, J.; Yamada, T.; Hirayasu, Y. Use of restraint in a general hospital psychiatric unit in Japan. Psychiatry Clin. Neurosci. 2005, 59, 605–609. [Google Scholar] [CrossRef]
- Draine, J.; Salzer, M.S.; Culhane, D.P.; Hadley, T.R. Role of social disadvantage in crime, joblessness, and homelessness among persons with serious mental illness. Psychiatric Serv. 2002, 53, 565–573. [Google Scholar] [CrossRef]
- Klassen, D.; O’Connor, W.A. A prospective study of predictors of violence in adult male mental health admissions. Law Hum. Behav. 1988, 12, 143–158. [Google Scholar] [CrossRef]
- Spidel, A.; Lecomte, T.; Greaves, C.; Sahlstrom, K.; Yuille, J.C. Early psychosis and aggression: Predictors and prevalence of violent behaviour amongst individuals with early onset psychosis. Int. J. Law Psychiatry 2010, 33, 171–176. [Google Scholar] [CrossRef]
- Jovanovic, N.; Kudumija Slijepcevic, M.; Podlesek, A. Personality traits in suicidal and homicidal subjects with schizophrenia. J. Forensic Psychiatry Psychol. 2019, 30, 76–88. [Google Scholar] [CrossRef]
- Stanton, B.; Baldwin, R.M.; Rachuba, L. A quarter century of violence in the United States: An epidemiologic assessment. Psychiatr. Clin. North Am. 1997, 20, 269–282. [Google Scholar] [CrossRef]
- Kirchebner, J.; Sonnweber, M.; Nater, U.M.; Günther, M.; Lau, S. Stress, Schizophrenia, and Violence: A Machine Learning Approach. J. Interpers. Violence 2022, 37, 602–622. [Google Scholar] [CrossRef]
- Ntounas, P.; Katsouli, A.; Efstathiou, V.; Pappas, D.; Chatzimanolis, P.; Touloumis, C.; Papageorgiou, C.; Douzenis, A. Comparative study of aggression–dangerousness on patients with paranoid schizophrenia: Focus on demographic data, PANSS, drug use and aggressiveness. Int. J. Law Psychiatry 2018, 60, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Fisher, H.L.; Craig, T.K.; Fearon, P.; Morgan, K.; Dazzan, P.; Lappin, J.; Hutchinson, G.; Doody, G.A.; Jones, P.B.; McGuffin, P. Reliability and comparability of psychosis patients’ retrospective reports of childhood abuse. Schizophr. Bull. 2011, 37, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Heinrichs, R.W.; Sam, E.P. Schizophrenia and crime: How predictable are charges, convictions and violence? Int. J. Ment. Health Addict. 2012, 10, 122–131. [Google Scholar] [CrossRef]
- Bartels, S.J.; Drake, R.E.; Wallach, M.A.; Freeman, D.H. Characteristic hostility in schizophrenic outpatients. Schizophr. Bull. 1991, 17, 163–171. [Google Scholar] [CrossRef]
- Fischer, S.N.; Shinn, M.; Shrout, P.; Tsemberis, S. Homelessness, mental illness, and criminal activity: Examining patterns over time. Am. J. Community Psychol. 2008, 42, 251–265. [Google Scholar] [CrossRef]
- Fryer, M.A.; Beech, M.; Byrne, G.J. Seclusion use with children and adolescents: An Australian experience. Aust. New Zealand J. Psychiatry 2004, 38, 26–33. [Google Scholar] [CrossRef]
- Green, K.; Browne, K.; Chou, S. The relationship between childhood maltreatment and violence to others in individuals with psychosis: A systematic review and meta-analysis. Trauma Violence Abus. 2019, 20, 358–373. [Google Scholar] [CrossRef] [PubMed]
- Mossman, D. Assessing predictions of violence: Being accurate about accuracy. J. Consult. Clin. Psychol. 1994, 62, 783. [Google Scholar] [CrossRef] [PubMed]
- Elbogen, E.B.; Johnson, S.C. The intricate link between violence and mental disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch. Gen. Psychiatry 2009, 66, 152–161. [Google Scholar] [CrossRef]
- Elbogen, E.B.; Swanson, J.W.; Swartz, M.S.; Van Dorn, R. Family representative payeeship and violence risk in severe mental illness. Law Hum. Behav. 2005, 29, 563–574. [Google Scholar] [CrossRef]
- Kamphuis, J.; Dijk, D.-J.; Spreen, M.; Lancel, M. The relation between poor sleep, impulsivity and aggression in forensic psychiatric patients. Physiol. Behav. 2014, 123, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Witt, K.; Hawton, K.; Fazel, S. The relationship between suicide and violence in schizophrenia: Analysis of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) dataset. Schizophr. Res. 2014, 154, 61–67. [Google Scholar] [CrossRef]
- Ben-Zeev, D.; Scherer, E.A.; Brian, R.M.; Mistler, L.A.; Campbell, A.T.; Wang, R. Use of multimodal technology to identify digital correlates of violence among inpatients with serious mental illness: A pilot study. Psychiatr. Serv. 2017, 68, 1088–1092. [Google Scholar] [CrossRef] [PubMed]
- Gordon, V.; Egan, V. What self-report impulsivity measure best postdicts criminal convictions and prison breaches of discipline? Psychol. Crime Law 2011, 17, 305–318. [Google Scholar] [CrossRef]
- Witt, K.; Van Dorn, R.; Fazel, S. Risk factors for violence in psychosis: Systematic review and meta-regression analysis of 110 studies. PLoS ONE 2013, 8, e55942. [Google Scholar]
- Sun, L.; Han, X.; Wang, K.; Xu, C.; Song, Z.; Zhang, J.; Cao, D.; Tan, L.; Chen, F.; Wu, S. Candidate symptomatic markers for predicting violence in schizophrenia: A cross-sectional study of 7711 patients in a Chinese population. Asian J. Psychiatry 2021, 59, 102645. [Google Scholar] [CrossRef]
- Arango, C.; Barba, A.C.; González-Salvador, T.; Ordonez, A.C. Violence in inpatients with schizophrenia: A prospective study. Schizophr. Bull. 1999, 25, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Dib, J.E.; Yaacoub, H.E.; Ikdais, W.H.; Atallah, E.; Merheb, T.J.; Ajaltouni, J.; Akkari, M.; Mourad, M.; Nasr, M.E.; Hachem, D. Rapid tranquillisation in a psychiatric emergency hospital in Lebanon: TREC-Lebanon–a pragmatic randomised controlled trial of intramuscular haloperidol and promethazine v. intramuscular haloperidol, promethazine and chlorpromazine. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, A.; Fenger, M.; Østergaard, S.; Nielbo, K.; Mors, O. Predicting mechanical restraint of psychiatric inpatients by applying machine learning on electronic health data. Acta Psychiatr. Scand. 2019, 140, 147–157. [Google Scholar] [CrossRef]
- Susser, E.; Lovell, A.; Conover, S. Unravelling the causes of homelessness–and of its association with mental illness. In Epidemiology and the Prevention of Mental Disorders; Routledge: London, UK, 2021; pp. 228–239. [Google Scholar]
- Varshney, M.; Mahapatra, A.; Krishnan, V.; Gupta, R.; Deb, K.S. Violence and mental illness: What is the true story? J. Epidemiol. Community Health 2016, 70, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Choe, J.Y.; Teplin, L.A.; Abram, K.M. Perpetration of violence, violent victimization, and severe mental illness: Balancing public health concerns. Psychiatr. Serv. 2008, 59, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Swanson, J.W.; Swartz, M.S.; Essock, S.M.; Osher, F.C.; Wagner, H.R.; Goodman, L.A.; Rosenberg, S.D.; Meador, K.G. The social–environmental context of violent behavior in persons treated for severe mental illness. Am. J. Public Health 2002, 92, 1523–1531. [Google Scholar] [CrossRef]
- Chandra, I.S.; Kumar, K.L.; Reddy, M.P.; Reddy, C.M.P.K. Attitudes toward medication and reasons for non-compliance in patients with schizophrenia. Indian J. Psychol. Med. 2014, 36, 294–298. [Google Scholar] [CrossRef]
- Müller, V.C. Ethics of Artificial Intelligence and Robotics. Available online: https://plato.stanford.edu/archives/sum2021/entries/ethics-ai (accessed on 31 July 2022).

| Authors/Year Country/Setting | Patients/ Health Records | Variables Measured | Measure | Main Findings |
|---|---|---|---|---|
| Goodwin et al., 2019 United States Inpatient setting | Autism spectrum disorder, aged 6–17 years old (n = 20) | Wearable wrist biosensor, E4, which measures heart rate, heart rate variability, sweat glands autonomic innervation, and changes in sympathetic nervous system arousal. | Nil | Data were evaluated in cycles of 15 seconds. Aggressive behaviors could be predicted 1 min before they happened, with 3 min of prior biosensor information. |
| Günther et al., 2020 Switzerland University Hospital of Psychiatry Inpatient Setting | Schizophrenia, with offence history (n = 358) | Data obtained from physical records, including psychiatric assessments, treatments and reports from legal documents. | Symptoms were measured with close adoption of Positive and Negative Symptoms Scale, classifying symptoms as present or not. | 569 variables narrowed down to 10 predictor variables: aggression threat, actual aggression, prior direct coercive methods, poor impulse control, uncooperativeness, hostility, Haloperidol prescription, higher PANSS scores, higher antipsychotic dosage and unfavorable legal prognosis. |
| Hofmann et al., 2022 Switzerland University Hospital of Psychiatry Zurich Inpatient Setting | Schizophrenia spectrum disorder (n = 352) | Data obtained from physical records including demographic data, social data, childhood and youth history, psychiatric history, criminal history, forensic data, circumstances of current hospitalization and psychopathological symptoms. | Symptoms were measured with the adopted Positive and Negative Symptoms Scale, classifying whether symptoms were absent, partially present or substantially present. | 507 probable variables narrowed down to 10 predictor variables: complaints about staff, adverse behaviors towards patients, antisocial behaviors, breaking of ward rules, time at high dependency, higher PANSS score, and adapted PANSS scores for hostility, tension, uncooperativeness and poor impulse control. |
| Menger et al., 2018 Netherlands University Medical Center Utrecht, Inpatient Setting | Electronic health records (n = 1,015,931) | Data from electronic health records written by psychiatrists or nurses in free text format. Psychiatrists’ notes included patient history and treatment. Nurses’ notes included patients’ well-being and activities. | Nil | Classical models like Naïve Bayes and Decision Trees did not achieve equivalent performance with other algorithms, likely due to their simplicity and inability to detect complex patterns. |
| Menger et al., 2019 Netherlands Inpatient Setting | Electronic health records of patients with psychotic disorders, mood disorders, personality disorders, substance-related disorders Site 1 (n = 2209 patients) Site 2 (n = 3253 patients) | Data from electronic health records of patients who were admitted. Notes were from 4 weeks prior to patients’ admission up to the initial 24 h of admission. The free text data were converted to numerical form using paragraph2vec algorithm. | Staff Observation Aggression Scale-Revised | Internal validation: Site 1: AUC = 0.80, specificity = 0.94, sensitivity = 0.33 Site 2: AUC = 0.76, specificity = 0.95, sensitivity = 0.34 External validation: Site 1: AUC = 0.72, specificity = 0.93, sensitivity = 0.25 Site 2: AUC = 0.64, specificity = 0.93, sensitivity = 0.13 |
| Suchting et al., 2018 United States Harris County Psychiatric Center, Inpatient setting | Electronic health records (n = 29,841) | Data from electronic health records, including demographic data, psychosocial assessment, childhood, education, military and work history, medical and psychiatric history, substance use and treatment, abuse, and financial and living situation. | Affective Disorders Rating Scale | 328 probable variables narrowed down to 20 predictor variables: homelessness, forensic assault history, abuse history (witnessed and perpetrated), younger age, aggressive history, lower educational levels, having suicidal ideation upon admission, underwent special education, depressive history, problematic work history, no children, poor sleep, family history of suicide, single, impaired mental state, risk issues, financial difficulties and no prior work history. |
| Van Le et al., 2018 Australia Wilfred Lopes Centre, forensic inpatient | Electronic Health Records (n = 220,000) | Electronic health records of time-sequenced narrative records illustrating observations and comments about each patient. Terms were extracted using different dictionaries: symptom, sentiment and frequency. | Dynamic Appraisal of Situational Aggression (DASA) Historical Clinical Risk Management-20 (HCR-20) Short-Term Assessment of Risk and Treatability (START) | DASA: Support Vector Machine and Logistic Model Tree produced the best models with all three dictionaries. Support Vector Machine had accuracy = 0.77, and LMT had accuracy = 0.75. Best prediction of DASA scores weas from the examination of sentiment language, accuracy 0.56–0.77. HCR-20: Algorithms performed better for symptoms rather than frequency dictionary. START dataset: Root Mean Square Error of 6.29–14.92, and deemed non-reliable. |
| Wang et al., 2020 Canada Centre for Addiction and Mental Health, Inpatient setting | Schizophrenia spectrum disorder (n = 275) | Data from electronic health records, including demographic data, psychiatric history, lifetime alcohol and drug use, suicidal behaviors, personality, experiences of abuse or neglect, family history of mental disorders and suicide. | Modified Overt Aggression Scale Columbia- Suicide Severity Rating Scale Childhood Trauma Questionnaire NEO Five Factor Inventory | Predictors of aggression that were significant included older age (p < 0.001), increased hospitalizations (p < 0.001), lower agreeableness (p = 0.015) and previous history of physical neglect (p = 0.042). Predictors of non-aggression included immigration after 18 years old (p = 0.033) and family history of mood disorders (p = 0.048). |
| Authors | Machine Learning Models | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Logistic Regression | Support Vendor Machine | GLM | Random Forest | GBM | K-Nearest Neigbour | Decision Tree | Naive Bayes | J48 | Others | NN | RNN | CNN | |
| Goodwin et al., 2019 | Global: * 0.71 PD: ** 0.84 | ||||||||||||
| Günther et al., 2020 | ** 0.85 | ** 0.84 | ** 0.86 | ** 0.84 | ** 0.80 | * 0.79 | ** 0.85 | ||||||
| Hofmann et al., 2022 | ** 0.85 | ** 0.87 | ** 0.83 | ** 0.85 | ** 0.80 | ** 0.85 | |||||||
| Menger et al., 2018 | +BB: * 0.76 +BTI: * 0.76 +WE: * 0.76 +DE: * 0.77 | +BB: * 0.73 +BTI: * 0.72 +WE: 0.69 +DE: 0.67 | +BB: 0.69 +BTI: * 0.70 +WE: * 0.70 +DE: 0.69 | +BB: * 0.73 +BTI: * 0.72 +WE: * 0.75 +DE: * 0.75 | +BB: * 0.77 +BTI: * 0.75 +WE: 0.65 +DE: * 0.79 | +BB: * 0.73 +BTI: * 0.72 +WE: 0.68 +DE: * 0.76 | |||||||
| Menger et al., 2019 | Internal validation: * 0.76–** 0.80 External validation: 0.64–* 0.72 | ||||||||||||
| Suchting et al., 2018 | * 0.78 | * 0.74 | * 0.78 | * 0.71 | |||||||||
| # Van Le et al., 2018 | +ST: 0.69 +SY: 0.64 +F: 0.61 | +ST: * 0.74 +SY: * 0.70 +F: 0.69 | Bagging +ST: 0.70 +SY: 0.68 +F: 0.69 | +ST: * 0.75 +SY: * 0.70 +F: * 0.73 | +ST: 0.68 +SY: 0.68 +F: 0.59 | Jrip +ST: 0.64 +SY: 0.65 +F: 0.63 | |||||||
| Wang et al., 2020 | 0.64 | 0.64 | ^ 0.63 | 0.63 RBF = 0.62 | 0.64 for Lasso and Elastic net | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tay, J.L.; Li, Z.; Sim, K. Effectiveness of Artificial Intelligence Methods in Personalized Aggression Risk Prediction within Inpatient Psychiatric Treatment Settings—A Systematic Review. J. Pers. Med. 2022, 12, 1470. https://doi.org/10.3390/jpm12091470
Tay JL, Li Z, Sim K. Effectiveness of Artificial Intelligence Methods in Personalized Aggression Risk Prediction within Inpatient Psychiatric Treatment Settings—A Systematic Review. Journal of Personalized Medicine. 2022; 12(9):1470. https://doi.org/10.3390/jpm12091470
Chicago/Turabian StyleTay, Jing Ling, Ziqiang Li, and Kang Sim. 2022. "Effectiveness of Artificial Intelligence Methods in Personalized Aggression Risk Prediction within Inpatient Psychiatric Treatment Settings—A Systematic Review" Journal of Personalized Medicine 12, no. 9: 1470. https://doi.org/10.3390/jpm12091470
APA StyleTay, J. L., Li, Z., & Sim, K. (2022). Effectiveness of Artificial Intelligence Methods in Personalized Aggression Risk Prediction within Inpatient Psychiatric Treatment Settings—A Systematic Review. Journal of Personalized Medicine, 12(9), 1470. https://doi.org/10.3390/jpm12091470