
Proposal for a Paradigm Shift in Personalized Medicine for Patients with a Maxillary Edentulous Jaw by ENT Specialist and Dentist Cooperation


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Identification of the Possible Causal and Risk Factors for Maxillary Sinusitis after Implant Surgery with or without Sinus Augmentation
2.1. Untreated or Incompletely Managed Diabetes Mellitus and Smoking
2.2. Dental Causes such as Poor Oral Hygiene, Persistent/Recurrent Periodontitis, and Peri-Implantitis
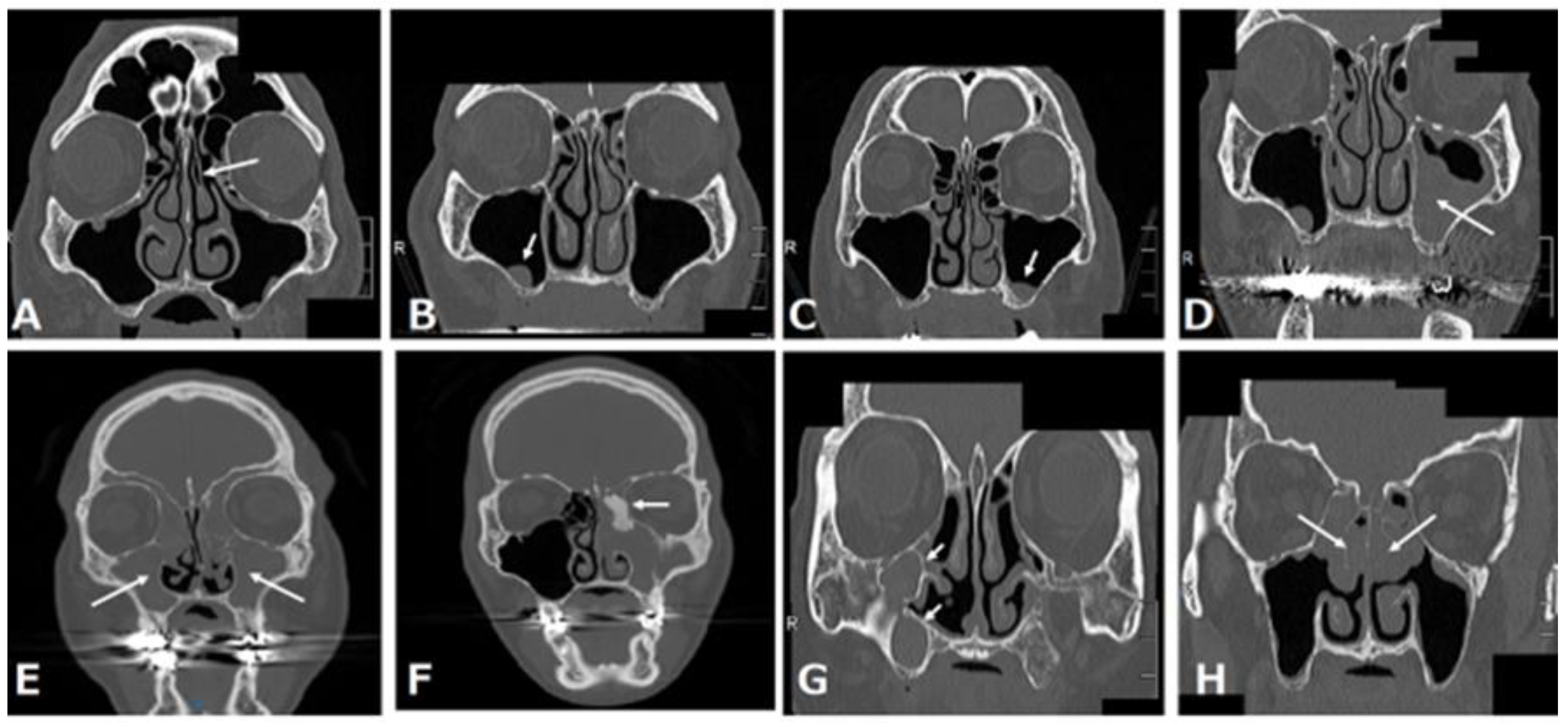
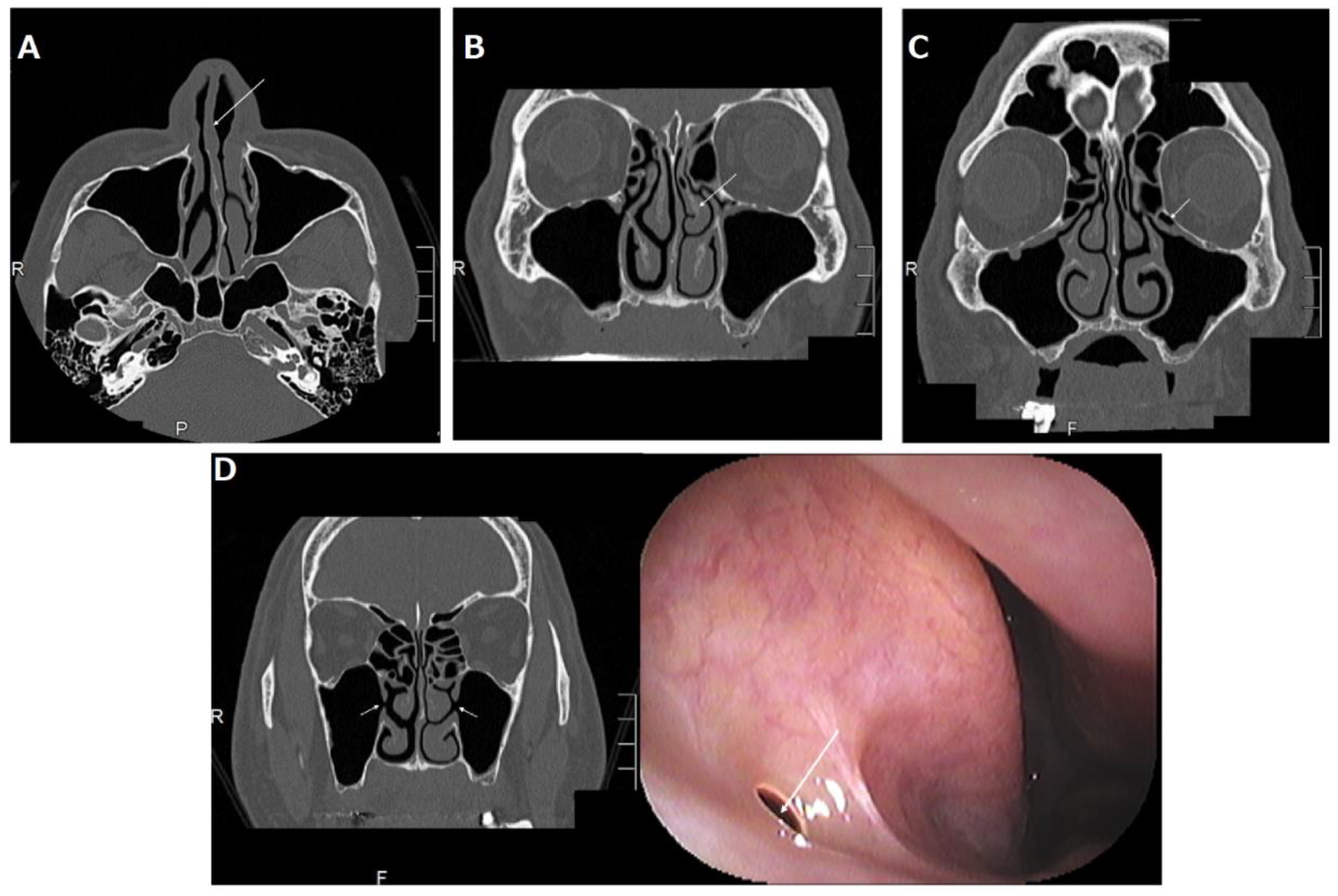
2.3. Alterations of the Anatomical Structure That Can Facilitate the Impairment of the Maxillary Sinus Drainage Pathway
2.3.1. Deviated Nasal Septum
2.3.2. Concha Bullosa or Paradoxical Middle Turbinate
2.3.3. Haller Cells
2.3.4. Accessory Ostium
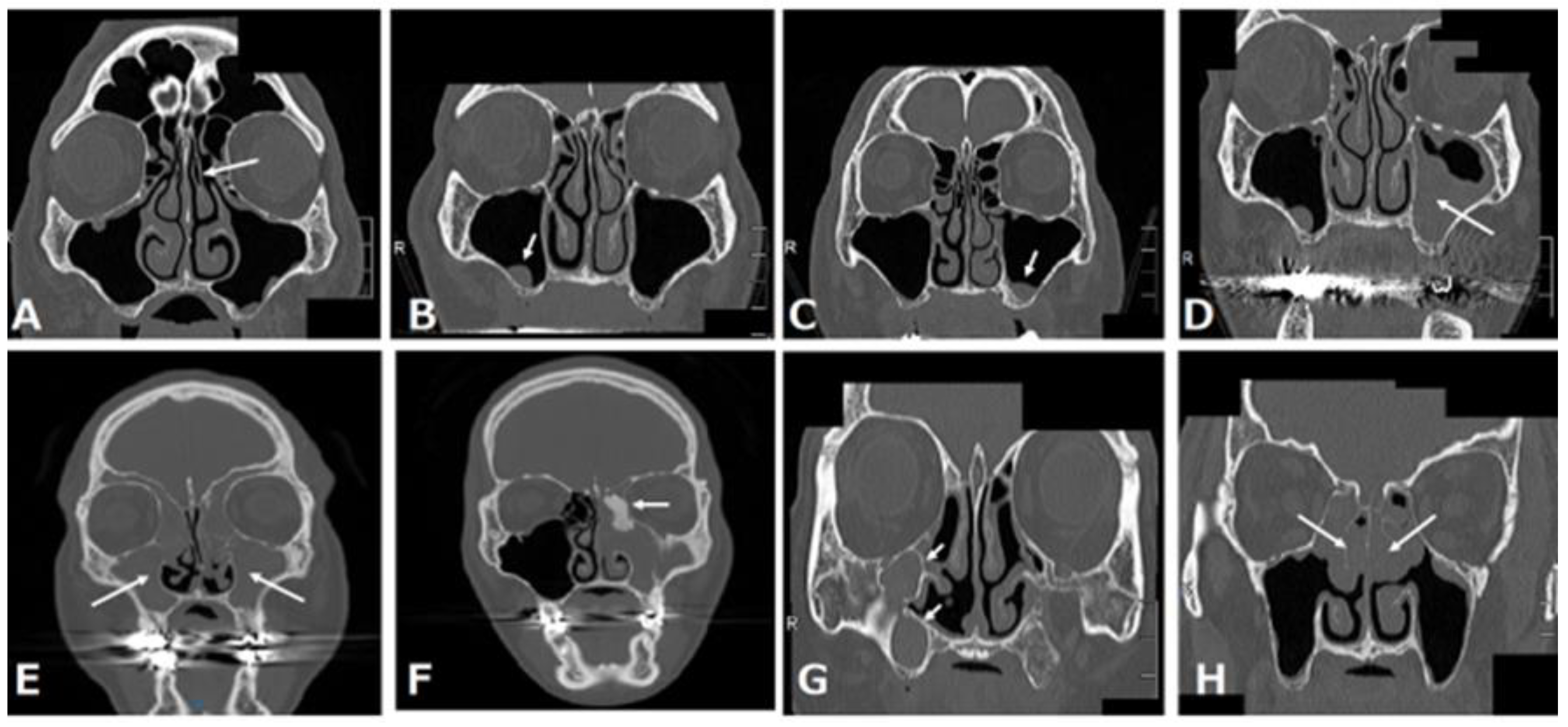
3. Common Maxillary Sinus Pathologies before Maxillary Implantation
3.1. Retention Cyst or Solitary Polyp
3.2. Mucosal Thickening in the Maxillary Sinus
3.3. Acute Rhinosinusitis
3.4. Chronic Rhinosinusitis
3.4.1. Neutrophilic Chronic Rhinosinusitis
3.4.2. Neutrophilic Chronic Rhinosinusitis with a Benign Tumor Such as Osteoma
3.4.3. Eosinophilic Chronic Rhinosinusitis (ECRS)
3.5. POMC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Romanos, G.E.; Delgado-Ruiz, R.; Sculean, A. Concepts for prevention of complications in implant therapy. Periodontol. 2000 2019, 81, 7–17. [Google Scholar]
- Law, C.; Alam, P.; Borumandi, F. Floor-of-mouth hematoma following dental implant placement: Literature Review and Case Presentation. J. Oral. Maxillofac. Surg. 2017, 75, 2340–2346. [Google Scholar]
- Suzuki, M.; Takahashi, K.; Kato, Y.; Baba, Y. A maxillary sinusitis after sinus lift surgery. J. Dent. Oral. Disord. 2018, 4, 1100. [Google Scholar]
- Chiapasco, M.; Felisati, G.; Maccari, A.; Borloni, R.; Gatti, F.; Di Leo, F. The management of complications following displacement of oral implants in the paranasal sinuses: A multicenter clinical report and proposed treatment protocols. Int. J. Oral Maxillofac. Surg. 2009, 38, 1273–1278. [Google Scholar]
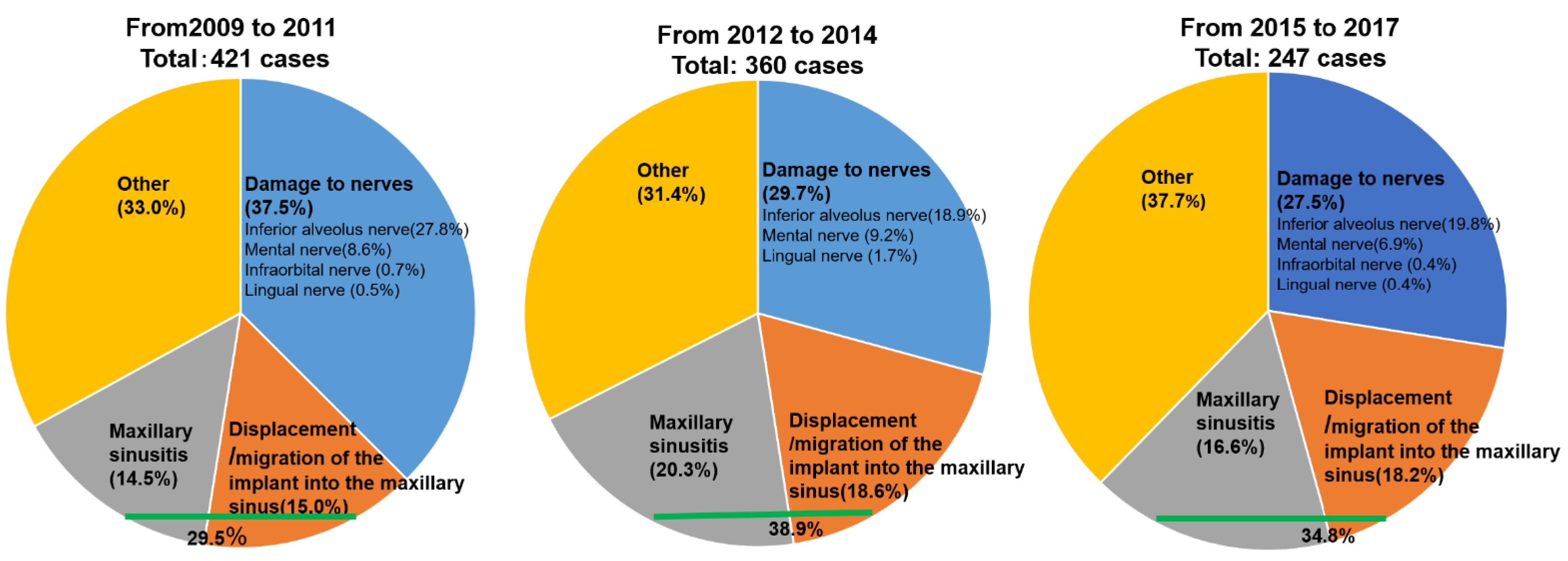
- Working Group of Trouble Investigation of The Japanese Academy of Maxillofacial Implants. Severe medical complications related dental implant surgery-The first investigative report in Japan. Jpn. J. Maxillo. Facial. Implants 2012, 11, 31–39. (In Japanese) [Google Scholar]
- Usuda, S.; Kawana, H.; Kato, T.; Kido, H.; Sato, J.; Shikimori, M.; Sekine, H.; Takahashi, T.; Fujii, T.; Yajima, Y.; et al. Severe medical complications related dental implant surgery-The second investigative report in Japan. Jpn. J. Maxillo. Facial. Implant. 2017, 16, 89–100. (In Japanese) [Google Scholar]
- Fuchigami, K.; Kawana, H.; Kato, T.; Kido, H.; Sato, J.; Shikimori, M.; Sekine, H.; Takahashi, T.; Fujii, T.; Yajima, Y.; et al. Severe medical complications relating dental implant surgery-The third investigative report in Japan. Jpn. J. Maxillo. Facial. Implant. 2020, 19, 111–121. (In Japanese) [Google Scholar]
- Nooh, N. Effect of schneiderian membrane perforation on posterior maxillary implant survival. J. Int. Oral Health. 2013, 5, 28–34. [Google Scholar]
- Monje, A.; Catena, A.; Borgnakke, W.S. Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: Systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 636–648. [Google Scholar]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar]
- Orlandi, R.R. A systematic analysis of septal deviation associated with rhinosinusitis. Laryngoscope 2010, 120, 1687–1695. [Google Scholar]
- Fadda, G.L.; Rosso, S.; Aversa, S.; Petrelli, A.; Ondolo, C.; Succo, G. Multiparametric statistical correlations between paranasal sinus anatomic variations and chronic rhinosinusitis. Acta. Otorhinolaryngol. Ital. 2012, 32, 244–251. [Google Scholar]
- Bani-Ata, M.; Aleshawi, A.; Khatatbeh, A.; Al-Domaidat, D.; Alnussair, B.; Al-Shawaqfeh, R.; Allouh, M. Accessory maxillary ostia: Prevalence of an anatomical variant and association with chronic sinusitis. Int. J. Gen. Med. 2020, 8, 163–168. [Google Scholar]
- Lee, J.W.; Yoo, J.Y.; Paek, S.J.; Park, W.J.; Choi, E.J.; Choi, M.G.; Kwon, K.H. Correlations between anatomic variations of maxillary sinus ostium and postoperative complication after sinus lifting. J. Korean Assoc. Oral Maxillofac. Surg. 2016, 42, 278–283. [Google Scholar]
- Akbulut, A.; Dilaver, E. Correlation between prevelance of Haller cells and postoperative maxillary sinusitis after sinus lifting procedure. Br. J. Oral. Maxillofac. Surg. 2019, 57, 473–476. [Google Scholar]
- Suzuki-Yamazaki, M.; Takahashi, K.; Takada, S.; Kato, Y.; Baba, Y. A successful treatment regimen for the prevention of sinusitis after maxillary sinus floor elevation surgery in a high-risk case. Case Rep. Otolaryngol. 2020, 2020, 6869805. [Google Scholar]
- Kim, J.S.; Choi, S.M.; Yoon, J.H.; Lee, E.J.; Yoon, J.; Kwon, S.H.; Yeo, C.D.; Ryu, J.S.; Lee, J.H.; You, Y.S.; et al. What affects postoperative sinusitis and implant failure after dental implant: A meta-analysis. Otolaryngol. Head Neck Surg. 2019, 160, 974–984. [Google Scholar]
- Giotakis, E.I.; Weber, R.K. Cysts of the maxillary sinus: A literature review. Int. Forum Allergy Rhinol. 2013, 3, 766–771. [Google Scholar]
- Anitua, E.; Alkhraisat, M.H.; Torre, A.; Eguia, A. Are mucous retention cysts and pseudocysts in the maxillary sinus a risk factor for dental implants? A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, e276–e283. [Google Scholar]
- Chan, H.L.; Wang, H.L. Sinus pathology and anatomy in relation to complications in lateral window sinus augmentation. Implant. Dent. 2011, 20, 406–412. [Google Scholar]
- Chen, Y.W.; Lee, F.Y.; Chang, P.H.; Huang, C.C.; Fu, C.H.; Huang, C.C.; Lee, T.J. A paradigm for evaluation and management of the maxillary sinus before dental implantation. Laryngoscope 2018, 128, 1261–1267. [Google Scholar]
- Kwah, J.H.; Peters, A.T. Nasal polyps and rhinosinusitis. Allergy Asthma Proc. 2019, 40, 380–384. [Google Scholar]
- El-Anwar, M.W.; Eesa, M.; Mansour, W.; Zake, L.G.; Hendawy, E. Analysis of ear, nose and throat Manifestations in COVID-19 Patients. Int. Arch. Otorhinolaryngol. 2021, 25, 343–348. [Google Scholar]
- Tobita, T.; Nakamura, M.; Ueno, T.; Sano, K. Sinus augmentation surgery after endoscopic sinus surgery for the treatment of chronic maxillary sinusitis: A case report. Implant Dent. 2011, 20, 337–340. [Google Scholar]
- Strek, P.; Zagólski, O.; Składzień, J.; Kurzyński, M.; Dyduch, G. Osteomas of the paranasal sinuses: Surgical treatment options. Med. Sci. Monit. 2007, 13, 244–250. [Google Scholar]
- Haruna, S.; Otori, N.; Yanagi, K.; Moriyama, H. Eosinophilic sinusitis. Oto-Rhino-Laryngol. 2001, 44, 195–201. (In Japanese) [Google Scholar]
- Takahashi, K.; Yamazaki, K.; Suzuki-Yamazaki, M.; Ito, H.; Baba, Y. Different management for patients with two types of chronic rhinosinusitis for their oral implant therapy. Adv. Dent. Oral Health 2021, 14, 555894. [Google Scholar]
- Funakawa, T.; Kawanabe, H.; Usami, A.; Takahashi, K.; Kato, Y.; Baba, Y. The importance of early detection for postoperative maxillary cyst before dental implantation: A case report. Int. J. Surg. Case Rep. 2021, 86, 106370. [Google Scholar]
- Kim, S.W.; Lee, I.H.; Kim, S.W.; Kim, D.H. Points to consider before the insertion of maxillary implants: The otolaryngologist’s perspective. J. Periodontal. Implant. Sci. 2019, 49, 346–354. [Google Scholar]
- Pignataro, L.; Mantovani, M.; Torretta, S.; Felisati, G.; Sambataro, G. ENT assessment in the integrated management of candidate for (maxillary) sinus lift. Acta. Otorhinolaryngol. Ital. 2008, 28, 110–119. [Google Scholar]
- Stella, J.P.; Warner, M.R. Sinus slot technique for simplification and improved orientation of zygomaticus dental implants: A technical note. Int. J. Oral Maxillofac. Implant. 2000, 15, 889–893. [Google Scholar]
- Tan, V.Y.J.; Zhang, E.Z.Y.; Daniel, D.; Sadovoy, A.; Teo, N.W.Y.; Kiong, K.L.; Toh, S.T.; Yuen, H.W. Respiratory droplet generation and dispersal during nasoendoscopy and upper respiratory swab testing. Head Neck 2020, 42, 2779–2781. [Google Scholar]
- Al-Haj, Husain, A.; Döbelin, Q.; Giacomelli-Hiestand, B.; Wiedemeier, D.B.; Stadlinger, B.; Valdec, S. Diagnostic Accuracy of Cystic Lesions Using a Pre-Programmed Low-Dose and Standard-Dose Dental Cone-Beam Computed Tomography Protocol: An Ex Vivo Comparison Study. Sensors 2021, 21, 7402. [Google Scholar]
- Al-Haj, Husain, A.; Sekerci, E.; Schönegg, D.; Bosshard, F.A.; Stadlinger, B.; Winklhofer, S.; Piccirelli, M.; Valdec, S. Dental MRI of Oral Soft-Tissue Tumors-Optimized Use of Black Bone MRI Sequences and a 15-Channel Mandibular Coil. J. Imaging 2022, 8, 146. [Google Scholar]
- Carmeli, G.; Artzi, Z.; Kozlovsky, A.; Segev, Y.; Landsberg, R. Antral computerized tomography pre-operative evaluation: Relationship between mucosal thickening and maxillary sinus function. Clin. Oral Implant. Res. 2011, 22, 78–82. [Google Scholar]
- Shanbhag, S.; Karnik, P.; Shirke, P.; Shanbhag, V. Cone-beam computed tomographic analysis of sinus membrane thickness, ostium patency, and residual ridge heights in the posterior maxilla: Implications for sinus floor elevation. Clin. Oral Implant. Res. 2014, 25, 755–760. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baba, Y.; Kato, Y.; Takahashi, K. Proposal for a Paradigm Shift in Personalized Medicine for Patients with a Maxillary Edentulous Jaw by ENT Specialist and Dentist Cooperation. J. Pers. Med. 2022, 12, 1289. https://doi.org/10.3390/jpm12081289
Baba Y, Kato Y, Takahashi K. Proposal for a Paradigm Shift in Personalized Medicine for Patients with a Maxillary Edentulous Jaw by ENT Specialist and Dentist Cooperation. Journal of Personalized Medicine. 2022; 12(8):1289. https://doi.org/10.3390/jpm12081289
Chicago/Turabian StyleBaba, Yuh, Yasumasa Kato, and Keiso Takahashi. 2022. "Proposal for a Paradigm Shift in Personalized Medicine for Patients with a Maxillary Edentulous Jaw by ENT Specialist and Dentist Cooperation" Journal of Personalized Medicine 12, no. 8: 1289. https://doi.org/10.3390/jpm12081289
APA StyleBaba, Y., Kato, Y., & Takahashi, K. (2022). Proposal for a Paradigm Shift in Personalized Medicine for Patients with a Maxillary Edentulous Jaw by ENT Specialist and Dentist Cooperation. Journal of Personalized Medicine, 12(8), 1289. https://doi.org/10.3390/jpm12081289