
Identifying Patients with Bicuspid Aortic Valve Disease in UK Primary Care: A Case–Control Study and Prediction Model



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design and Population
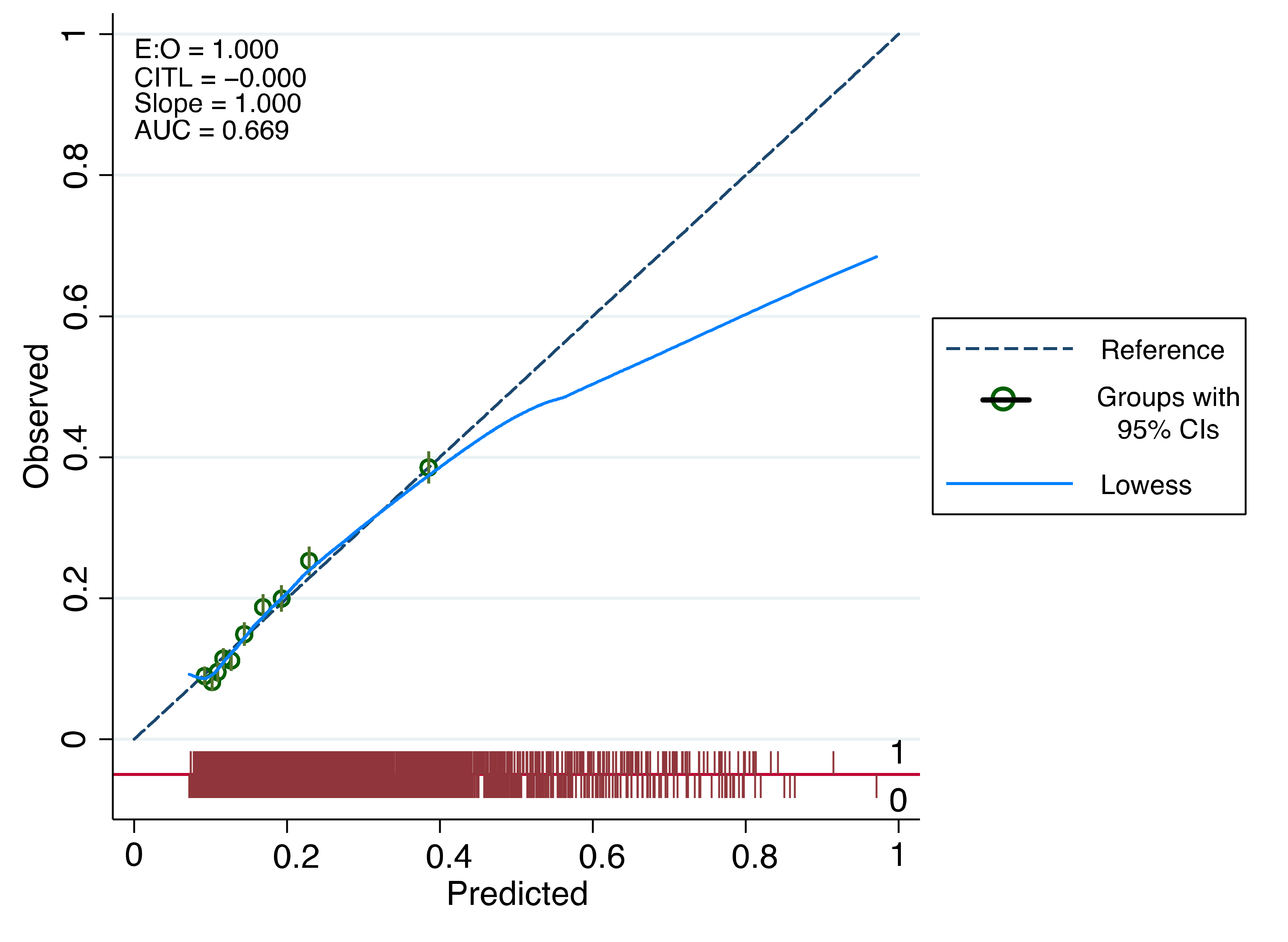
2.3. Statistical Analysis and Model Development
3. Results
3.1. Baseline Characteristics
3.2. Associated Features and Multivariate Modelling
4. Discussion
4.1. Principal Findings
4.2. Comparison with Other Literature/Studies
4.3. Clinical Implications
4.4. Strength and Limitations
4.5. Further Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galian-Gay, L.; Carro Hevia, A.; Teixido-Turà, G.; Rodríguez Palomares, J.; Gutiérrez-Moreno, L.; Maldonado, G.; Gonzàlez-Alujas, M.T.; Sao-Aviles, A.; Gallego, P.; Calvo-Iglesias, F.; et al. Familial clustering of bicuspid aortic valve and its relationship with aortic dilation in first-degree relatives. Heart 2019, 105, 603. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.K.; Bossé, Y.; Muehlschlegel, J.D.; Michelena, H.I.; Limongelli, G.; Della Corte, A.; Francesca, R.; Pluchinotta, F.R.; Russo, M.G.; Evangelista, A.; et al. A Roadmap to Investigate the Genetic Basis of Bicuspid Aortic Valve and its Complications. J. Am. Coll. Cardiol. 2014, 64, 832. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.-T.; Tribouilloy, C.; Masri, A.; Bax, J.J.; Delgado, V.; Girdauskas, E.; Evangelista, A.; Sundt, T.M.; Svensson, L.G.; Enriquez-Sarano, M.; et al. Clinical presentation and outcomes of adults with bicuspid aortic valves: 2020 update. Prog. Cardiovasc. Dis. 2020, 63, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Michelena, H.I.; Prakash, S.K.; Della Corte, A.; Bissell, M.M.; Anavekar, N.; Mathieu, P.; Bossé, Y.; Limongelli, G.; Bossone, E.; Benson, D.W.; et al. Bicuspid aortic valve: Identifying knowledge gaps and rising to the challenge from the International Bicuspid Aortic Valve Consortium (BAVCon). Circulation 2014, 129, 2691–2704. [Google Scholar] [CrossRef]
- Capoulade, R.; Schott, J.-J.; Le Tourneau, T. Familial bicuspid aortic valve disease: Should we look more closely at the valve? Heart 2019, 105, 584–586. [Google Scholar] [CrossRef]
- Arden, C.; Chambers, J.B.; Sandoe, J.; Ray, S.; Prendergast, B.; Taggart, D.; Westaby, S.; Grothier, L.; Wilson, J.; Campbell, B.; et al. Can we improve the detection of heart valve disease? Heart 2014, 100, 271. [Google Scholar] [CrossRef]
- Michelena, H.I.; Desjardins, V.A.; Avierinos, J.F.; Russo, A.; Nkomo, V.T.; Sundt, T.M.; Pellikka, P.A.; Tajik, A.J.; Enriquez-Sarano, M. Natural history of asymptomatic patients with normally functioning or minimally dysfunctional bicuspid aortic valve in the community. Circulation 2008, 117, 2776–2784. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Herrett, E.; Gallagher, A.M.; Bhaskaran, K.; Forbes, H.; Mathur, R.; van Staa, T.; Smeeth, L. Data Resource Profile: Clinical Practice Research Datalink (CPRD). Int. J. Epidemiol. 2015, 44, 827–836. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Marshall, A.; Altman, D.G.; Holder, R.L.; Royston, P. Combining estimates of interest in prognostic modelling studies after multiple imputation: Current practice and guidelines. BMC Med. Res. Methodol. 2009, 9, 57. [Google Scholar] [CrossRef]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef]
- Liu, X. Classification accuracy and cut point selection. Statist. Med. 2012, 31, 2676–2686. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multiple Prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Tither, K. NHS Diagnostic Waiting Times and Activity Data; Government Statistical Service (GSS): Leeds, UK, 2017. [Google Scholar]
- Masri, A.; Svensson, L.G.; Griffin, B.P.; Desai, M.Y. Contemporary natural history of bicuspid aortic valve disease: A systematic review. Heart 2017, 103, 1323–1330. [Google Scholar] [CrossRef]
- Stortecky, S.; Buellesfeld, L.; Wenaweser, P.; Heg, D.; Pilgrim, T.; Khattab Ahmed, A.; Gloekler, S.; Huber, C.; Nietlispach, F.; Meier, B.; et al. Atrial Fibrillation and Aortic Stenosis. Circ. Cardiovasc. Interv. 2013, 6, 77–84. [Google Scholar] [CrossRef]
- Brignole, M.; Moya, A.; De Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martin, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef]
- Lee, S.Y.; Shim, C.Y.; Hong, G.-R.; Cho, I.J.; Chang, H.-J.; Ha, J.-W.; Chung, N. Determinants and Prognostic Significance of Symptomatic Status in Patients with Moderately Dysfunctional Bicuspid Aortic Valves. PLoS ONE 2017, 12, e0169285. [Google Scholar] [CrossRef]
- Rahimi, K.; Mohseni, H.; Kiran, A.; Tran, J.; Nazarzadeh, M.; Rahimian, F.; Woodward, M.; Dwyer, T.; MacMahon, S.; Otto, C.M. Elevated blood pressure and risk of aortic valve disease: A cohort analysis of 5.4 million UK adults. Eur. Heart J. 2018, 39, 3596–3603. [Google Scholar] [CrossRef]
- Koenraadt, W.M.C.; Tokmaji, G.; DeRuiter, M.C.; Vliegen, H.W.; Scholte, A.J.H.A.; Siebelink, H.M.J.; Gittenberger-de Groot, A.C.; de Graaf, M.A.; Wolterbeek, R.; Mulder, B.J.; et al. Coronary anatomy as related to bicuspid aortic valve morphology. Heart 2016, 102, 943. [Google Scholar] [CrossRef]
- NICE. Atrial fibrillation: Diagnosis and Management|NICE Guideline NG196; NICE: London, UK, 2021. [Google Scholar]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. ESC Scientific Document Group, 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery [EACTS]: The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology [ESC] Developed with the special contribution of the European Heart Rhythm Association [EHRA] of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Raviele, A.; Giada, F.; Bergfeldt, L.; Blanc, J.J.; Blomstrom-Lundqvist, C.; Mont, L.; Morgan, J.M.; Raatikainen, M.J.P.; Steinbeck, G.; Viskin, S.; et al. Management of patients with palpitations: A position paper from the European Heart Rhythm Association. EP Eur. 2011, 13, 920–934. [Google Scholar] [CrossRef]
- Excellence. NIfHaC. Transient Loss of Consciousness [‘Blackouts’] in over 16s|[NICE Guideline CG109]|NICE. 2010. Available online: https://www.nice.org.uk/guidance/cg109/evidence (accessed on 5 March 2022).
- NICE. Hypertension in Adults: Diagnosis and Management|Guidance NG136|NICE; NICE: London, UK, 2019. [Google Scholar]
- NICE. Suspected Cancer: Recognition and Referral. Guidance NG12; NICE: London, UK, 2015. [Google Scholar]
- Draper, J.; Subbiah, S.; Bailey, R.; Chambers, J.B. Murmur clinic: Validation of a new model for detecting heart valve disease. Heart 2019, 105, 56. [Google Scholar] [CrossRef]
- Hillebrand, M.; Koschyk, D.; Ter Hark, P.; Schuler, H.; Rybczynski, M.; Berger, J.; Gulati, A.; Bernhardt, A.M.; Detter, C.; Girdauskas, E.; et al. Diagnostic accuracy study of routine echocardiography for bicuspid aortic valve: A retrospective study and meta-analysis. Cardiovasc. Diagn. Ther. 2017, 7, 367–379. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Cases BAV n = 2898 (16.67) | Controls n = 14,487 (83.33) | ||||
|---|---|---|---|---|---|
| Male | Female | Male | Female | ||
| n (%) | 1792 (61.84) | 1106 (38.16) | 8811 (60.82) | 5676 (39.18) | |
| Age at diagnosis * | Mean (s.d) | 41.28 (16.46) | 41.82 (17.11) | 41.28 (16.46) | 41.38 (16.86) |
| Median | 39.67 | 38.85 | 39.67 | 38.24 | |
| Range | 16.02, 90.84 | 16.00, 90.37 | 16.02, 90.84 | 16.02, 90.4 | |
| IQR | 27.19, 53.88 | 27.51, 53.78 | 27.19, 53.88 | 27.27, 53.01 | |
| BMI (kg/m2) | Median (IQR) | 25.35 (22.7, 27.9) | 24.2 (21.8, 27.5) | 25 (22.6, 28.1) | 24 (21.4, 27.4) |
| Smoking status | Smoker n (%) | 371 (20.70) | 174 (15.73) | 1892 (21.47) | 919 (16.19) |
| Non-smoker n (%) | 1045 (58.31) | 750 (67.81) | 3751 (42.57) | 3008 (53.00) | |
| Ex-smoker n (%) | 155 (8.65) | 86 (7.78) | 636 (7.22) | 428 (7.54) | |
| No data n (%) | 221 (12.33) | 96 (8.68) | 2532 (28.74) | 1321 (23.27) | |
| Ethnicity | White n (%) | 777 (43.36) | 469 (42.41) | 2457 (27.89) | 1601 (28.21) |
| Non-White/unknown n (%) | 1015 (56.64) | 637 (57.59) | 6354 (72.11) | 4075 (71.79) | |
| Age Categories | Number | No Preceding Complications * n (%) | No Preceding Complications or CVD+ n (%) | CAD Dx before n (%) | CHF Dx before n (%) | Endocarditis Dx before n (%) | Stroke Dx before n (%) |
|---|---|---|---|---|---|---|---|
| <25 | 566 | 526 (93%) | 517 (91%) | 1 (0.18) | 1 (0.18) | 1 (0.18) | 0 |
| 25–49 | 1463 | 1271 (87%) | 1189 (81%) | 12 (0.82) | 8 (0.55) | 11 (0.75) | 9 (0.62) |
| 50–74 | 779 | 582 (75%) | 423 (54%) | 80 (10.27) | 15 (1.93) | 4 (0.51) | 17 (2.18) |
| >=75 | 90 | 57 (63%) | 42 (47%) | 14 (15.56) | 7 (7.78) | 0 | 2 (2.22) |
| Clinical Variable | Odds Ratio [95% CI] | p-Value | Coefficient [95% CI] |
|---|---|---|---|
| Diagnosis of hypertension | 1.72 [1.48 to 2.00] | 0.000 | 0.543 [0.391 to 0.695] |
| Diagnosis of atrial fibrillation [AF] | 2.25 [1.60 to 3.16] | 0.000 | 0.810 [0.470 to 1.15] |
| Diagnosis of palpitations | 2.86 [2.32 to 3.51] | 0.000 | 1.05. [0.843 to 1.26] |
| Diagnosis of dizziness | 1.22 [1.01 to 1.47] | 0.039 | 0.198 [0.010 to 0.386] |
| Ethnicity White/non-White | 1.35 [1.29 to 1.41] | 0.000 | 0.301 [0.259 to 0.343] |
| Log mean pulse3,3 | 0.000 | −1.38 [−1.98 to −0.788] 0.742 [0.410 to 1.07] | |
| Beta-blocker category | |||
| Intermittent beta-blocker use (Longest gap between prescriptions > 90 but <180 days) | 2.05 [1.75 to 2.41] | 0.000 | 0.717 [0.558 to 0.878] |
| Intermittent beta-blocker use (Longest gap between prescriptions > 180 days) | 2.23 [1.79 to 2.79] | 0.000 | 0.804 [0.581 to 1.03] |
| Continuous beta-blocker use (No gap between prescriptions longer than 90 days) | 1.71 [0.927 to 3.17] | 0.086 | 0.539 [−0.759 to 1.15] |
| Diagnoses before BAV Diagnosis n (%) (Unless Otherwise Stated) | Cases | Controls | p Value (chi2) (* = t Test) | Time before Diagnosis (Days) Median [IQR] | First Dx > 90 Days before BAV Dx (%) |
|---|---|---|---|---|---|
| n = 2898 | n = 14,487 | ||||
| Cardiovascular | |||||
| Systolic BP (mean [SD]) | 127.4 [18.6] | 125.7 [18.6] | <0.001 * | ||
| Diastolic BP (mean [SD]) | 76.3 [11.0] | 76.2 [11.43] | 0.7 * | ||
| Diagnosis of hypertension | 337 [11.6] | 727 [5.02] | <0.001 | 1232 [351–2547] | 85 |
| Pulse (mean [SD]) | 74.9 [14.85] | 76.83 [13.37] | 0.03 * | ||
| Diagnosis of tachycardia | 34 [1.17] | 44 [0.30] | <0.001 | 1147 [34–5423] | 74 |
| Diagnosis of bradycardia | 10 [0.35] | 22 [0.15] | 0.027 | 1830 [172–2475] | 80 |
| Tachycardia on pulse (mean >100) | 22 [0.76] | 52 [0.36] | <0.001 | ||
| Bradycardia on pulse (mean < 60) | 56 [1.93] | 70 [0.48] | <0.001 | ||
| Diagnosis of aortic aneurysm/dissection | 18 [0.62] | 11 [0.08] | <0.001 | 265 [47–1274] | 72 |
| Diagnosis of endocarditis | 16 [0.55] | 1 [0.01] | <0.001 | 954 [193–3893] | 88 |
| Diagnosis of tricuspid valve disease | 6 [0.21] | 7 [0.05] | 0.004 | 1341 [1113–2749] | 100 |
| Diagnosis of mitral valve disease | 61 [2.10] | 18 [0.12] | <0.001 | 398 [132–1431] | 82 |
| Diagnosis of pulmonary valve disease | 18 [0.62] | 9 [0.06] | <0.001 | 1325 [255–1571] | 94 |
| Diagnosis of palpitations | 192 [6.63] | 258 [1.78] | <0.001 | 655 [163–1756] | 81 |
| Diagnosis of heart failure | 31 [1.07] | 52 [0.36] | <0.001 | 246 [58–946] | 65 |
| Diagnosis of coronary arterial disease | 107 [3.69] | 231 [1.59] | <0.001 | 731 [85–1866] | 73 |
| Diagnosis of atrial fibrillation (AF) | 81 [2.80] | 86 [0.59] | <0.001 | 419 [108–1187] | 79 |
| Neurological | |||||
| Diagnosis of stroke/TIA | 28 [0.97] | 72 [0.50] | 0.002 | 888 [142–4899] | 93 |
| Diagnosis of epilepsy | 29 [1.00] | 95 [0.66] | 0.044 | 839 [186–2701] | 83 |
| Diagnosis of migraine | 27 [0.93] | 63 [0.43] | <0.001 | 1015 [290–3005] | 96 |
| Diagnosis of dizziness | 187 [6.45] | 538 [3.71] | <0.001 | 1420 [374–2943] | 90 |
| Diagnosis of collapse | 116 [4.00] | 312 [2.15] | <0.001 | 855 [152–2304] | 83 |
| Beta-blocker use | |||||
| Not taking | 2427 [83.75] | 13,649 [94.2] | |||
| Intermittent use (90–180-day gap in prescription issue after initiation) | 306 [10.56] | 558 [3.85] | |||
| Intermittent use (>180-day gap in prescription issue after initiation) | 148 [5.11] | 247 [1.70] | |||
| Continuous use (<90-day gap in prescription issue since initiation) | 17 [0.59] | 33 [0.22] | <0.001 |
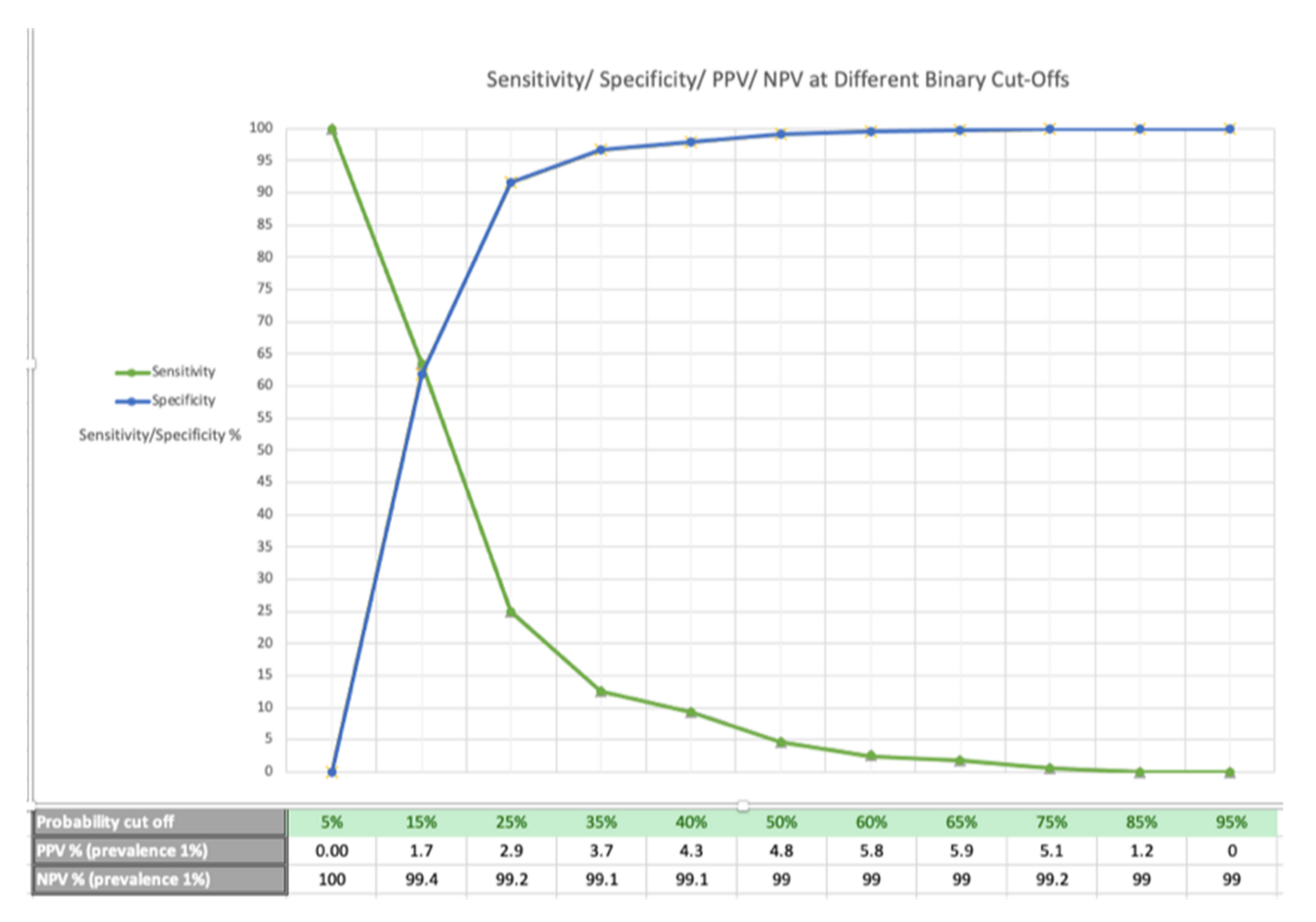
| Probability Cut-Off | 5% | 15% | 25% | 35% | 50% | 65% | 75% | 85% | 95% |
|---|---|---|---|---|---|---|---|---|---|
| PPV % (prevalence 0.5%) | 0 | 0.8 | 1.5 | 1.9 | 2.4 | 3 | 2.6 | 0.6 | 0 |
| NPV % (prevalence 0.5%) | 100 | 99.7 | 99.6 | 99.5 | 99.5 | 99.5 | 99.5 | 99.5 | 99.5 |
| PPV % (prevalence 1%) | 0 | 1.7 | 2.9 | 3.7 | 4.8 | 5.9 | 5.1 | 1.2 | 0 |
| NPV % (prevalence 1%) | 100 | 99.4 | 99.2 | 99.1 | 99.0 | 99.0 | 99.2 | 99.0 | 99.0 |
| PPV % (prevalence 2%) | 0 | 3.3 | 5.7 | 7.2 | 9.2 | 11.3 | 9.7 | 2.5 | 0 |
| NPV % (prevalence 2%) | 100 | 98.8 | 98.4 | 98.2 | 98.1 | 98.0 | 98.0 | 98.0 | 98.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, W.; Akyea, R.K.; Weng, S.; Kai, J.; Qureshi, N. Identifying Patients with Bicuspid Aortic Valve Disease in UK Primary Care: A Case–Control Study and Prediction Model. J. Pers. Med. 2022, 12, 1290. https://doi.org/10.3390/jpm12081290
Evans W, Akyea RK, Weng S, Kai J, Qureshi N. Identifying Patients with Bicuspid Aortic Valve Disease in UK Primary Care: A Case–Control Study and Prediction Model. Journal of Personalized Medicine. 2022; 12(8):1290. https://doi.org/10.3390/jpm12081290
Chicago/Turabian StyleEvans, William, Ralph Kwame Akyea, Stephen Weng, Joe Kai, and Nadeem Qureshi. 2022. "Identifying Patients with Bicuspid Aortic Valve Disease in UK Primary Care: A Case–Control Study and Prediction Model" Journal of Personalized Medicine 12, no. 8: 1290. https://doi.org/10.3390/jpm12081290
APA StyleEvans, W., Akyea, R. K., Weng, S., Kai, J., & Qureshi, N. (2022). Identifying Patients with Bicuspid Aortic Valve Disease in UK Primary Care: A Case–Control Study and Prediction Model. Journal of Personalized Medicine, 12(8), 1290. https://doi.org/10.3390/jpm12081290