Abstract
Many epidemiologic and clinical studies have shown significant links between the degree of sleep disturbance and severity of impairment of selective cognitive functions, including the risk of neurodegenerative diseases. However, the sleep parameters that affect cognitive function in old age are unclear. Therefore, we investigated the association between sleep parameters and cognitive function in older patients. Patients aged above 65 years who complained of sleep-disordered breathing were enrolled consecutively. The Mini-Mental-State Examination tool was used to evaluate cognitive function. Eighty patients (normal cognitive function, n = 32 and cognitive impairment, n = 42) were included in this study. Multiple linear regression and binary logistic regression analyses were performed to explain the relationship between sleep parameters and cognitive function. We found that the body mass index (BMI) was significantly lower in the cognitive impairment group than in the normal cognitive function group. Additionally, the cognitive impairment group showed significantly decreased sleep efficiency and an increased apnea index compared with normal subjects. Moreover, lower BMI, reduced sleep efficiency, and high frequency of apnea events during sleep were associated with an increased risk of cognitive impairment.
1. Introduction
Sleep patterns usually change during the course of normal aging, where a decrease in total sleep duration and efficiency, an increase in sleep fragmentation, difficulty falling asleep, a decrease in rapid-eye-movement (REM) sleep, and predominance of slow-wave sleep are some of the commonly observed sleep-related problems [1,2]. However, some of these sleep disturbances may be due to neurodegenerative processes. Specifically, the sleep–wake cycle is regulated by interactions between areas of the brain related to memory and cognitive function [3,4,5,6].
A previous study showed that various sleep problems occurred in up to 45% of patients with Alzheimer’s disease and other dementias [7]. Other studies showed that patients who have neurodegenerative disease mainly have symptoms of micro-architectural sleep alteration, nocturnal sleep fragmentation, decreased nocturnal sleep duration, and inversion of the sleep–wake cycle [8,9,10]. In particular, several studies have reported that sleep-disordered breathing (SDB), such as obstructive sleep apnea, is more common in patients with cognitive decline than in patients with normal cognitive function [11,12,13,14]. Therefore, sleep disturbance can be as stressful to patients and caregivers as the cognitive impairment itself, and is a major risk factor for early hospitalization [15]. Meanwhile, some studies have suggested that there is a bi-directional relationship between sleep disturbances and cognitive impairment [16,17]. One meta-analysis study showed that sleep disturbances such as insomnia and SDB were risk factors for dementia [18].
However, these studies have the following limitations: most of the patients’ sleep information was obtained from self-report or actigraphy, and the measurements of cognitive function were not constant. Therefore, in aiming to examine the relationship between sleep and cognitive function in old age, we consecutively enrolled older patients with SDB and compared sleep patterns between the groups with normal cognitive function and cognitive impairment using laboratory polysomnography (PSG) and Mini-Mental State Examination (MMSE) results.
2. Materials and Methods
2.1. Patients
This study was approved by the Institutional Review Board of Hallym Medical University Chuncheon Sacred Hospital (No. 2019-10-003). Patients over 60 years old who complained of SDB were consecutively and prospectively recruited at Chuncheon Sacred Hospital from October 2020 to April 2021. All participants provided written informed consent. We excluded patients who had a history of neurodegenerative disease, had undergone surgeries for sleep disorders, and had serious comorbidities (e.g., cancer, severe depression, severe cardiac or respiratory failure, severe renal or hepatic insufficiency). The patients were divided into two groups according to the results of cognitive function assessments: normal cognitive function group and cognitive impairment group.
2.2. Cognitive Outcome Measures
The MMSE is used to assess global cognitive functions [19]. MMSE scores range from 0 to 30, and the higher the score, the better the cognitive function. In this study, we used the Korean version of the Mini-Mental-State Examination (MMSE-KC), which was modified for the socio-cultural and language characteristics of the Korean population [20]. MMSE-KC scores are influenced by age, sex, and education level. Therefore, cognitive impairment is evaluated using normative scores for age, sex, and education level. Scores of 25 or higher were classified as normal results; however, scores below 24 were classified as abnormal results, indicating the possibility of cognitive impairment.
2.3. Polysomnography
Standard overnight polysomnography (PSG) was performed in the sleep laboratory of Chuncheon Sacred Hospital, using a computerized polysomnographic device (Nox-A1; Nox Medical, Reykjavik, Iceland). The sleep stage and respiratory events were scored according to the guidelines of the American Academy of Sleep Medicine [21,22]. The following sleep parameters were assessed: total sleep time (TST), sleep efficiency (TST/time in bed × 100), sleep stages (stages N1, N2, N3, and R), oxygen desaturation index (ODI), apnea index (AI), hypopnea index (HI), and apnea–hypopnea index (AHI). ODI was defined as the number of episodes of oxygen desaturation per hour of sleep, with oxygen desaturation defined as a decrease in blood oxygen saturation (SpO2) to lower than 3% below baseline. Apnea was defined using an oronasal thermal sensor when the peak signal excursions dropped by ≥90% of the pre-event baseline, lasting for more than 10 s. Hypopnea was scored when the peak signal excursions using nasal pressure dropped by ≥30% of the pre-event baseline for at least 10 s, followed by a ≥3% decrease in oxygen desaturation or accompanied by arousal. AI or HI was defined as the number of apneas or hypopneas per hour of sleep, and AHI was defined as the sum of the number of apneas and hypopneas per hour of sleep. Based on the AHI, the severity of obstructive sleep apnea (OSA) was classified as follows: no OSA, AHI < 5 per hour; mild OSA, 5 ≤ AHI < 15 per hour; moderate OSA, 15 ≤ AHI < 30 per hour; severe OSA, AHI ≥ 30 per hour.
2.4. Statistical Analysis
Numerical variables were expressed as means ± standard deviations. We used the normality test to determine whether sample data were drawn from a normally distributed population and then, Student’s t-test was used to compare demographic factors and the scores of sleep parameters (TST, sleep efficiency, AI, HI, AHI, ODI, and snoring) between the two groups. Chi-square tests were used to compare categorical variables (sex, medical history, severity of OSA). As a predictive analysis, multiple linear regression and binary logistic regression analyses were performed to determine the relationship between sleep parameters and cognitive function. The area under the receiver operating characteristic curve (AUC ROC) was calculated to assess the diagnostic performance of the variables. The AUC ROC was computed by plotting sensitivity versus 1-specificity to evaluate the ability of each variable’s score to discriminate cognitive impairment. All statistical analyses were conducted using R version 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria). p < 0.05 was considered statistically significant.
3. Results
3.1. Demographic, Cognitive Function, Sleep-Related Problem in the Study Population
Eighty patients (21 [26.2%] men and 59 [73.8%] women) were included in this study. The mean patient age was 73.1 ± 5.63 years (range, 60–85 years). The patients were divided into a group with normal cognitive function (32 patients) or a group with cognitive impairment (48 patients), according to the MMSE score. The mean MMSE score of the cognitive impairment group was 20.58 ± 2.74, and the mean MMSE score of the normal cognitive group was 26.53 ± 1.22. The baseline characteristics are summarized in Table 1. There were no significance differences in demographic variables, comorbidities, Epworth sleepiness scale scores, and sleep apnea severity; however, BMI was significantly lower in the cognitive impairment group (p < 0.001, 95% CI: 1.56–4.63).

Table 1.
Characteristics of study population.
3.2. Polysomnographic Data of Patients with and without Cognitive Impairment
We compared the sleep profiles of the two groups obtained by PSG (Table 2). The cognitive impairment group had lower TST than the normal cognitive function group (240 and 259 min, respectively), but there was no significant difference (p = 0.061). Further, the cognitive impairment group showed a significantly decreased sleep efficiency (p = 0.047) and increased AI (p = 0.038). However, there was no significant difference between the groups with regard to sleep stage architecture, AHI, ODI, and oxygen saturation.
Table 2.
Comparison of sleep profiles between normal and cognitive impairment groups.
3.3. Relationship between Sleep-Related Factor and Cognitive Function
Multiple linear regression analysis was carried out with cognitive function (MMSE score) as the dependent variable, and BMI, sleep efficiency, and AI as the independent variables, after analysis of covariance. BMI and sleep efficiency were positively related to normal cognitive function, whereas high AI was associated with reduced cognitive function (Table 3). In the binary logistic regression analysis, BMI, sleep efficiency, and AI were significantly associated with cognitive function (odds ratio [OR] = 0.746, 95% confidence interval [CI] = 0.598–0.892; OR = 1.965, 95% CI = 1.007–2.360; OR = 2.028, 95% CI = 1.076–3.531, respectively) (Table 4). AI showed the strongest relationship with cognitive function. In the ROC curve analyses, the area under the ROC curve for the prediction of cognitive impairment using BMI, sleep efficiency, and AI was 0.794, with a sensitivity of 66.7% and specificity of 85.7% (Figure 1).
Table 3.
Result of multiple linear regression analysis of the contribution of other variables on cognitive function.
Table 4.
Determinants of cognitive impairment on binary logistic regression analysis results.
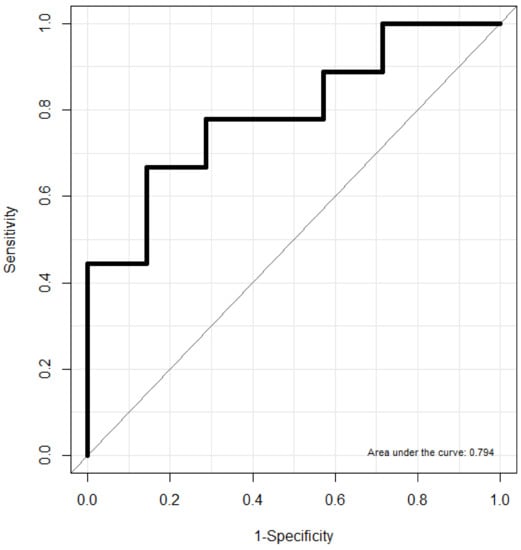
Figure 1.
Receiver operating characteristic curve (ROC) for prediction of cognitive impairment using BMI, sleep efficiency and apnea index.
4. Discussion
As people age, their sleep patterns naturally change and cognitive function declines. An estimated 25% of the older population experiences sleep problems, and 45% of patients with cognitive impairment have been reported to experience sleep disturbance [7,23]. Sleep disturbances in patients with cognitive impairment are qualitatively similar to those in older people but much more severe [9,24]. Several studies have been conducted from various perspectives to determine the relationship between sleep and cognition. In these studies, patients with cognitive impairment showed increased wakefulness after sleep onset and increased sleep latency, but reduced TST, sleep efficiency, and REM sleep [1,8,25]. To our knowledge, this study is the first to investigate the effect of sleep disturbance on cognitive function in old age using objective parameters. BMI, among demographic factors, and sleep efficiency and AI, among sleep parameters, were significantly associated with cognitive function. Interestingly, BMI and sleep efficiency were significantly lower in patients with cognitive impairment, and as the AI score increased, the tendency to developing cognitive decline also increased.
Previous studies have reported that short sleep duration and reduced sleep quality in patients with cognitive decline are associated with an increase in amyloid-β accumulation, one of the well-known risk factors of Alzheimer’s disease [26,27]. A functional imaging study using positron emission tomography showed a correlation between short sleep duration (or poor sleep quality) and high amyloid-β burden in 70 healthy older subjects [27]. Other studies reported that 40–70% of the patients with Alzheimer’s disease showed an AHI of 5 or higher and were at a higher risk of SDB than healthy older subjects [28,29]. Additionally, other studies showed that high AHI and hypoxemia were related to low global cognitive function [30,31,32]. Consistent with the results of these studies, we found that patients with cognitive impairment experienced significantly more apnea events during sleep, with lower sleep efficiency than patients with normal cognitive function.
Cognitive decline caused by SDB did not have an equal effect on all cognitive domains, and in particular, vigilance, executive functions, and memory domains were related [33]. Increased sleep fragmentation and hypoxia are two mechanisms by which SDB can impair cognition. An animal study showed that hypoxia was associated with an increase in neuronal apoptosis and hippocampal atrophy via oxidative stress and inflammatory pathways [34,35]. Other studies showed that exposure to hypoxia increased the levels of key components of AD, such as amyloid-β, amyloid plaques in the brain, and tau phosphorylation [36,37]. Similarly, in one study with a cognitive healthy APOE-ε4 negative adult, intermittent hypoxia was associated with an increase in the levels of phosphorylated tau, total tau, and amyloid-β in the cerebrospinal fluid [38]. Meanwhile, in neuroimaging studies, patients with obstructive sleep apnea showed decreased white matter integrity and grey matter volume in areas related to memory and execution function compared with healthy control [39,40]; in a large neuroimaging study of more than 800 older adults, SDB showed a strong association with longitudinal white matter changes, suggesting that the SDB increased the risk of cognitive impairment via changes in the white matter caused by vascular disease [41].
Our study had several strengths. First, the patients were recruited consecutively and prospectively. Second, we used laboratory PSG, which is the gold standard for diagnosing obstructive sleep apnea. We were able to evaluate sleep patterns and apnea-hypopnea events during sleep more accurately than previous studies that used actigraphy or home PSG. However, this study also has certain limitations. First, we used the MMSE to evaluate cognitive function. However, it is a relatively simple assessment for cognitive function. To confirm the impact of sleep disturbance on a specific cognitive domain, more detailed and specific cognitive function assessments are required. Second, some demographic factors closely related to cognitive function, such as household income and educational level, were not controlled [42]. Therefore, our findings might have entailed confounding biases. Future studies with larger sample sizes are needed to clarify the relationship between sleep parameters and cognitive function.
5. Conclusions
BMI and sleep efficiency positively correlate with cognitive function, but AHI scores are negatively associated with cognitive function in old age. Therefore, clinicians should pay attention to early detection of cognitive impairment when treating older patients with SDB who show low sleep efficiency and a high frequency of apnea events.
Author Contributions
Study conception, D.-K.K. and C.Y.L.; study design, I.H.L. and D.-K.K.; data acquisition, B.C.L.; data analysis, D.-K.K. and C.Y.L.; data interpretation, I.H.L., B.C.L. and D.-K.K.; manuscript preparation, D.-K.K. and C.Y.L.; review of the final manuscript, all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a grant from the Bio and Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (grant number NRF-2021R1C1C1005746).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Hallym Medical University Chuncheon Sacred Hospital (No. 2019-10-003).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and/or analyzed in the present study are not publicly available but are available from the corresponding author upon reasonable request.
Acknowledgments
We want to express our gratitude to all members of the division of Big Data and Artificial Intelligence at Hallym University College of Medicine.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bliwise, D.L. Sleep in Normal aging and dementia. Sleep 1993, 16, 40–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooke, J.R.; Ancoli-Israel, S. Normal and abnormal sleep in the elderly. Handb. Clin. Neurol. 2011, 98, 653–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canto, C.B.; Onuki, Y.; Bruinsma, B.; van der Werf, Y.D.; De Zeeuw, C.I. The sleeping cerebellum. Trends Neurosci. 2017, 40, 309–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branger, P.; Arenaza-Urquijo, E.M.; Tomadesso, C.; Mézenge, F.; André, C.; de Flores, R.; Mutlu, J.; de La Sayette, V.; Eustache, F.; Chételat, G.; et al. Relationships between sleep quality and brain volume, metabolism, and amyloid deposition in late adulthood. Neurobiol. Aging 2016, 41, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Zhong, G.; Naismith, S.L.; Rogers, N.L.; Lewis, S.J. Sleep-wake disturbances in common neurodegenerative diseases: A closer look at selected aspects of the neural circuitry. J. Neurol. Sci. 2011, 307, 9–14. [Google Scholar] [CrossRef]
- Diekelmann, S.; Born, J. The Memory Function of Sleep. Nat. Rev. Neurosci. 2010, 11, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.; Lynch, C.A.; Walsh, C.; Coen, R.; Coakley, D.; Lawlor, B.A. Sleep disturbance in mild to moderate alzheimer’s disease. Sleep Med. 2005, 6, 347–352. [Google Scholar] [CrossRef]
- Bliwise, D.L. Sleep disorders in Alzheimer’s disease and other dementias. Clin. Cornerstone 2004, 6 (Suppl. 1A), S16–S28. [Google Scholar] [CrossRef]
- Vitiello, M.V.; Prinz, P.N. Alzheimer’s disease. Sleep and sleep/wake patterns. Clin. Geriatr. Med. 1989, 5, 289–299. [Google Scholar] [CrossRef]
- Volicer, L.; Harper, D.G.; Manning, B.C.; Goldstein, R.; Satlin, A. Sundowning and circadian rhythms in Alzheimer’s disease. Am. J. Psychiatry 2001, 158, 704–711. [Google Scholar] [CrossRef]
- Gaeta, A.M.; Benítez, I.D.; Jorge, C.; Torres, G.; Dakterzada, F.; Minguez, O.; Huerto, R.; Pujol, M.; Carnes, A.; Dalmases, M.; et al. Prevalence of obstructive sleep apnea in Alzheimer’s disease patients. J. Neurol. 2020, 267, 1012–1022. [Google Scholar] [CrossRef] [PubMed]
- Yusop, C.Y.C.; Mohamad, I.; Mohammad, W.M.Z.W.; Abdullah, B. Cognitive function among obstructive sleep apnea patients in North East Malaysia. J. Natl. Med. Assoc. 2017, 109, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.L.; Gao, B.; Han, T.; Xiang, B.Y.; Liu, X. Moderate-to-severe obstructive sleep apnea and cognitive function impairment in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 1813–1822. [Google Scholar] [CrossRef] [PubMed]
- Harmell, A.L.; Neikrug, A.B.; Palmer, B.W.; Avanzino, J.A.; Liu, L.; Maglione, J.E.; Natarajan, L.; Corey-Bloom, J.; Loredo, J.S.; Ancoli-Israel, S. Obstructive sleep apnea and cognition in Parkinson’s disease. Sleep Med. 2016, 21, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollak, C.P.; Perlick, D.; Linsner, J.P.; Wenston, J.; Hsieh, F. Sleep problems in the community elderly as predictors of death and nursing home placement. J. Community Health 1990, 15, 123–135. [Google Scholar] [CrossRef]
- Wang, C.; Holtzman, D.M. Bidirectional relationship between sleep and Alzheimer’s disease: Role of amyloid, tau, and other factors. Neuropsychopharmacology 2020, 45, 104–120. [Google Scholar] [CrossRef]
- Ju, Y.E.; Lucey, B.P.; Holtzman, D.M. Sleep and Alzheimer disease pathology—A bidirectional relationship. Nat. Rev. Neurol. 2014, 10, 115–119. [Google Scholar] [CrossRef]
- Shi, L.; Chen, S.J.; Ma, M.Y.; Bao, Y.P.; Han, Y.; Wang, Y.M.; Shi, J.; Vitiello, M.V.; Lu, L. Sleep Disturbances Increase the Risk of Dementia: A Systematic Review and Meta-analysis. Sleep Med. Rev. 2018, 40, 4–16. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. ‘Mini-mental state’. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, K.U.; Lee, D.Y.; Kim, K.W.; Jhoo, J.H.; Kim, J.H.; Lee, K.H.; Kim, S.Y.; Han, S.H.; Woo, J.I. Development of the Korean Version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet (CERAD-K): Clinical and neuropsychological assessment batteries. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, P47–P53. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Updates for 2017 (Version 2.4). J. Clin. Sleep Med. 2017, 13, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Wolkove, N.; Elkholy, O.; Baltzan, M.; Palayew, M. Sleep and aging: 1. Sleep disorders commonly found in older people. Can. Med. Assoc. J. 2007, 176, 1299–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benca, R.M.; Obermeyer, W.H.; Thisted, R.A.; Gillin, J.C. Sleep and psychiatric disorders. a meta-analysis. Arch. Gen. Psychiatry 1992, 49, 651–668; discussion 669–670. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, T.; Yaffe, K.; Ancoli-Israel, S.; Schneider, J.L.; Cauley, J.A.; Hillier, T.A.; Fink, H.A.; Stone, K.L. Study of osteoporotic fractures group. poor sleep is associated with impaired cognitive function in older women: The study of osteoporotic fractures. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 405–410. [Google Scholar] [CrossRef] [Green Version]
- Ju, Y.E.; McLeland, J.S.; Toedebusch, C.D.; Xiong, C.; Fagan, A.M.; Duntley, S.P.; Morris, J.C.; Holtzman, D.M. Sleep quality and preclinical Alzheimer disease. JAMA Neurol. 2013, 70, 587–593. [Google Scholar] [CrossRef]
- Spira, A.P.; Gamaldo, A.A.; An, Y.; Wu, M.N.; Simonsick, E.M.; Bilgel, M.; Zhou, Y.; Wong, D.F.; Ferrucci, L.; Resnick, S.M. Self-reported sleep and β-Amyloid deposition in community-dwelling older adults. JAMA Neurol. 2013, 70, 1537–1543. [Google Scholar] [CrossRef] [Green Version]
- Ancoli-Israel, S.; Klauber, M.R.; Butters, N.; Parker, L.; Kripke, D.F. Dementia in Institutionalized elderly: Relation to sleep apnea. J. Am. Geriatr. Soc. 1991, 39, 258–263. [Google Scholar] [CrossRef]
- Hoch, C.C.; Reynolds, C.F., III; Kupfer, D.J.; Houck, P.R.; Berman, S.R.; Stack, J.A. Sleep-disordered breathing in normal and pathologic aging. J. Clin. Psychiatry 1986, 47, 499–503. [Google Scholar]
- Cohen-Zion, M.; Stepnowsky, C.; Marler; Shochat, T.; Kripke, D.F.; Ancoli-Israel, S. Changes in cognitive function associated with sleep disordered breathing in older people. J. Am. Geriatr. Soc. 2001, 49, 1622–1627. [Google Scholar] [CrossRef]
- Spira, A.P.; Blackwell, T.; Stone, K.L.; Redline, S.; Cauley, J.A.; Ancoli-Israel, S.; Yaffe, K. Sleep-disordered breathing and cognition in older women. J. Am. Geriatr. Soc. 2008, 56, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.S.; Sforza, E.; Roche, F.; Barthélémy, J.C.; Thomas-Anterion, C.; PROOF Study Group. Sleep breathing disorders and cognitive function in the elderly: An 8-year follow-up study. The Proof-Synapse Cohort. Sleep 2015, 38, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, M.E.; Aloia, M.S. Sleep-disordered breathing and cognition in older adults. Curr. Neurol. Neurosci. Rep. 2012, 12, 537–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gozal, D.; Row, B.W.; Kheirandish, L.; Liu, R.; Guo, S.Z.; Qiang, F.; Brittian, K.R. Increased susceptibility to intermittent hypoxia in aging rats: Changes in proteasomal activity, neuronal apoptosis and spatial function. J. Neurochem. 2003, 86, 1545–1552. [Google Scholar] [CrossRef] [Green Version]
- Nair, D.; Dayyat, E.A.; Zhang, S.X.; Wang, Y.; Gozal, D. Intermittent hypoxia-induced cognitive deficits are mediated by NADPH oxidase activity in a murine model of sleep apnea. PLoS ONE 2011, 6, e19847. [Google Scholar] [CrossRef]
- Li, L.; Zhang, X.; Yang, D.; Luo, G.; Chen, S.; Le, W. Hypoxia increases abeta generation by altering beta- and gamma-cleavage of APP. Neurobiol. Aging 2009, 30, 1091–1098. [Google Scholar] [CrossRef]
- Gao, L.; Tian, S.; Gao, H.; Xu, Y. Hypoxia increases Aβ-induced Tau phosphorylation by calpain and promotes behavioral consequences in AD transgenic mice. J. Mol. Neurosci. 2013, 51, 138–147. [Google Scholar] [CrossRef]
- Osorio, R.S.; Ayappa, I.; Mantua, J.; Gumb, T.; Varga, A.; Mooney, A.M.; Burschtin, O.E.; Taxin, Z.; During, E.; Spector, N.; et al. Interaction between sleep-disordered breathing and apolipoprotein E genotype on cerebrospinal fluid biomarkers for Alzheimer’s disease in cognitively normal elderly individuals. Neurobiol. Aging 2014, 35, 1318–1324. [Google Scholar] [CrossRef] [Green Version]
- Macey, P.M.; Kumar, R.; Woo, M.A.; Valladares, E.M.; Yan-Go, F.L.; Harper, R.M. Brain Structural Changes in Obstructive Sleep Apnea. Sleep 2008, 31, 967–977. [Google Scholar]
- Joo, E.Y.; Tae, W.S.; Lee, M.J.; Kang, J.W.; Park, H.S.; Lee, J.Y.; Suh, M.; Hong, S.B. Reduced Brain Gray Matter Concentration in Patients with Obstructive Sleep Apnea Syndrome. Sleep 2010, 33, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Robbins, J.; Redline, S.; Ervin, A.; Walsleben, J.A.; Ding, J.; Nieto, F.J. Associations of Sleep-disordered breathing and cerebral changes on MRI. J. Clin. Sleep Med. 2005, 1, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caamaño-Isorna, F.; Corral, M.; Montes-Martínez, A.; Takkouche, B. Education and dementia: A meta-analytic study. Neuroepidemiology 2006, 26, 226–232. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).