
Impaired Humoral Immunity with Concomitant Preserved T Cell Reactivity in IBD Patients on Treatment with Infliximab 6 Month after Vaccination with the SARS-CoV-2 mRNA Vaccine BNT162b2: A Pilot Study


Abstract
:1. Introduction
2. Methods
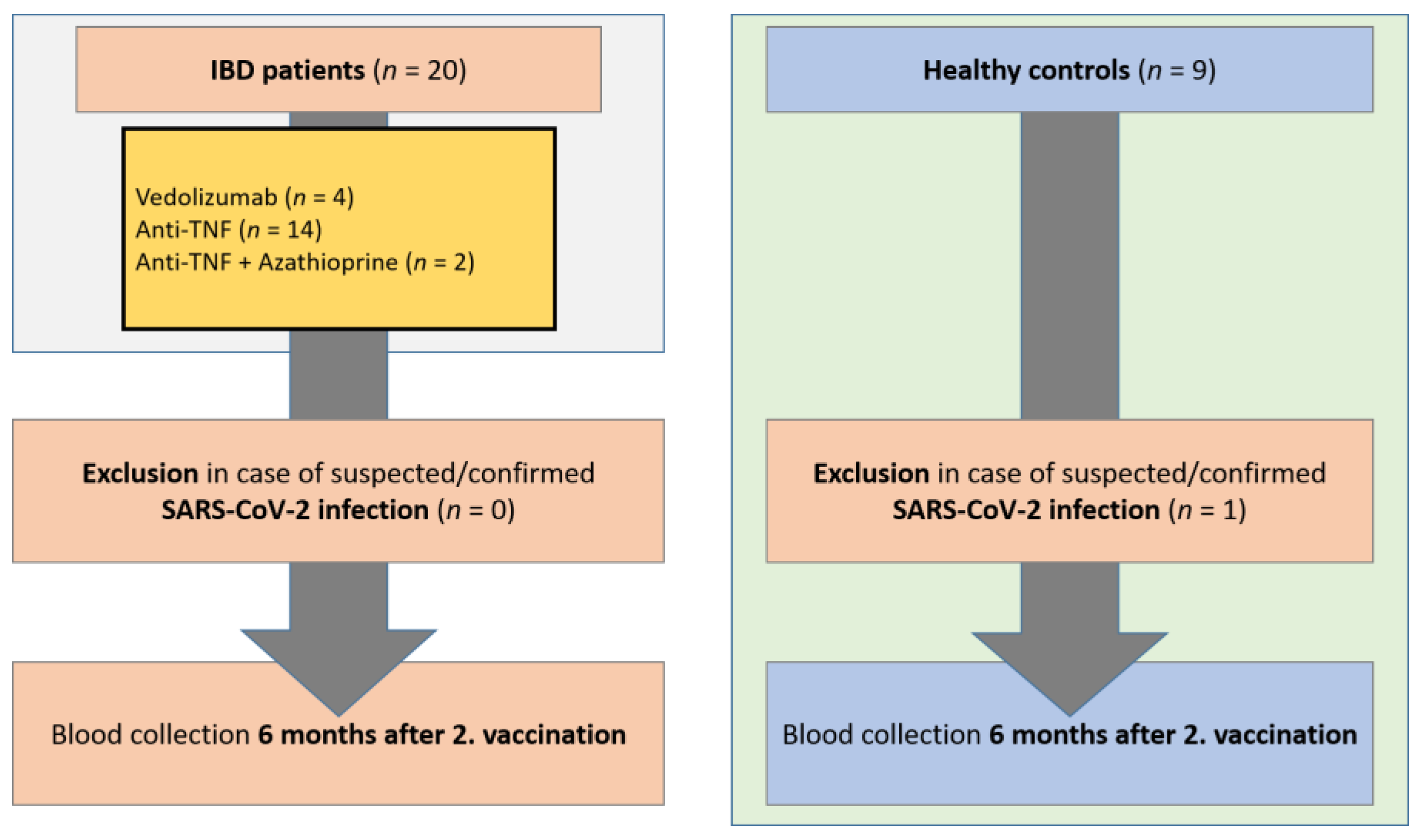
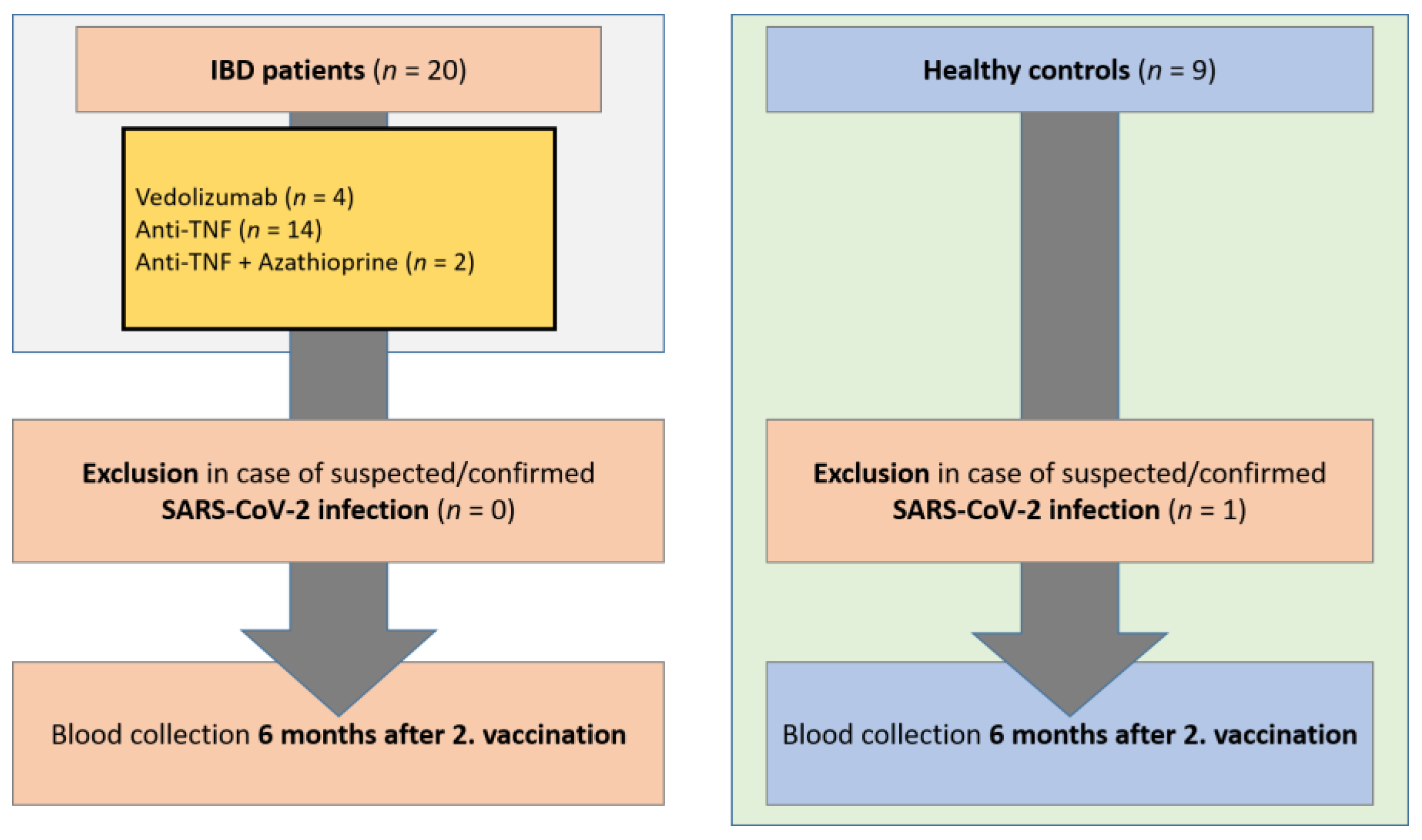
2.1. Study Subjects and Samples
2.2. Quantification of Serum Markers
2.3. SARS-CoV-2 Vaccines
2.4. Statistical Analysis
3. Results
3.1. Cohort Characteristics
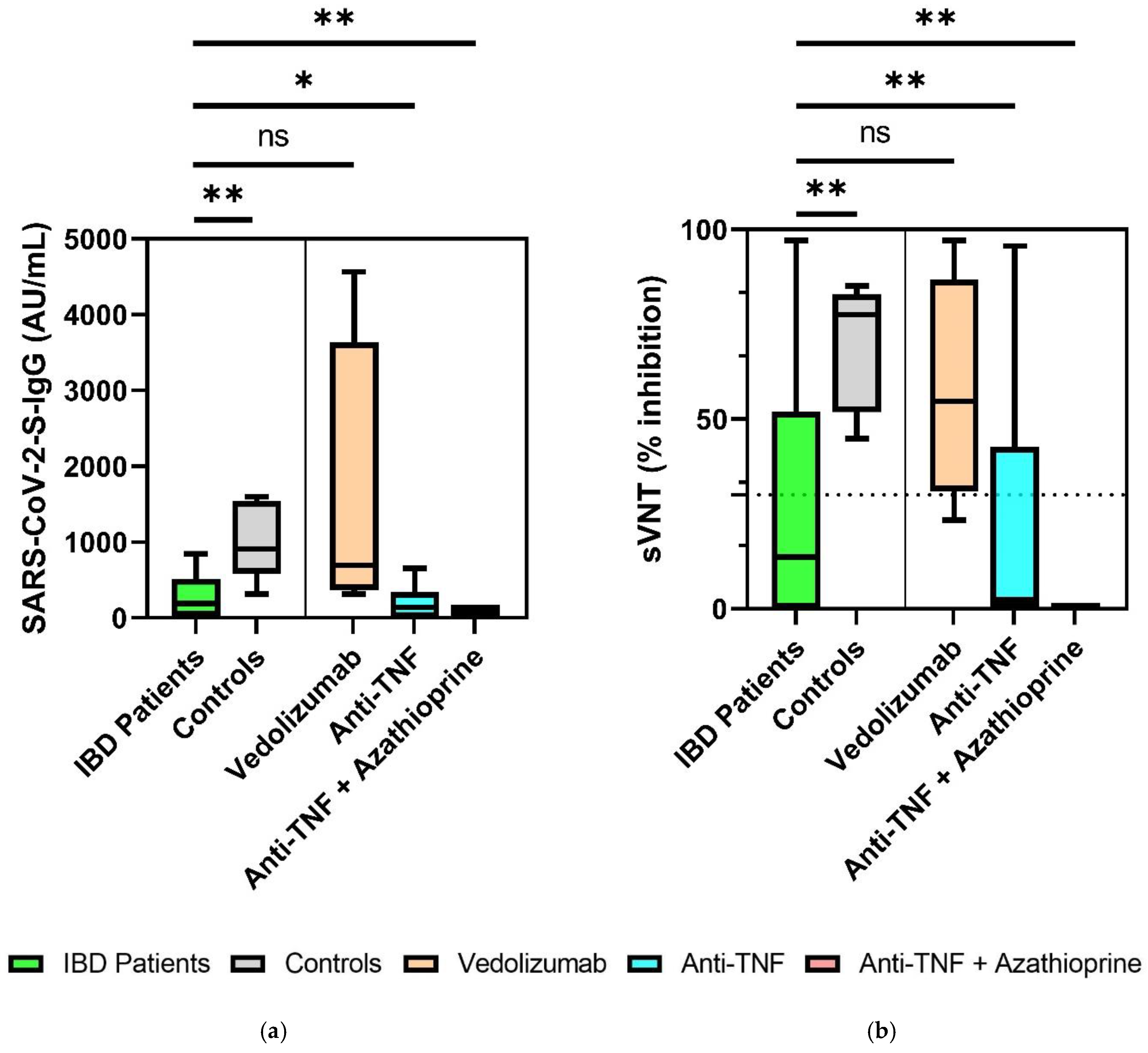
3.2. Significantly Decreased SARS-CoV-2 S-IgG and sVNT Inhibition Levels in IBD Patients 6 Months after Second Vaccination
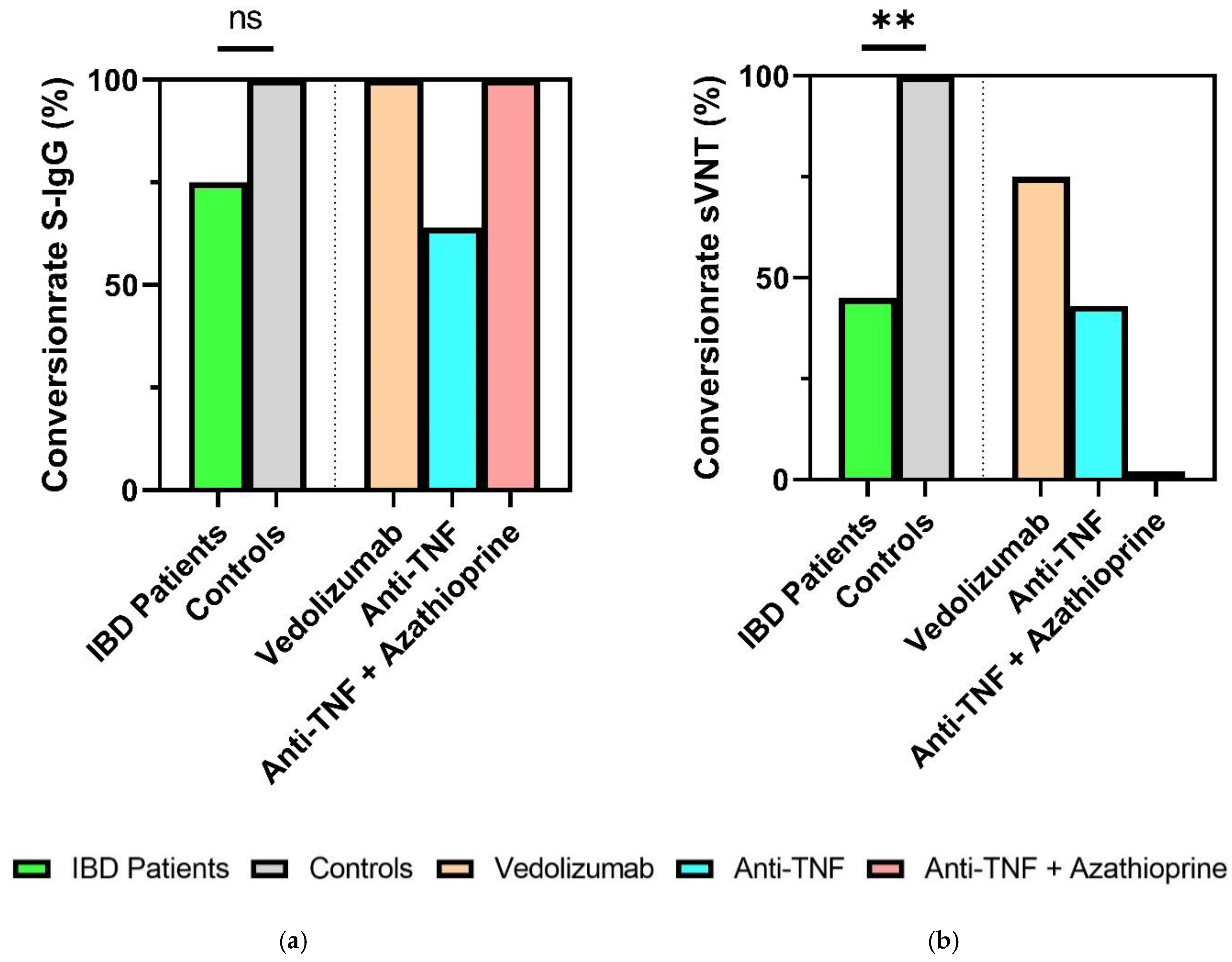
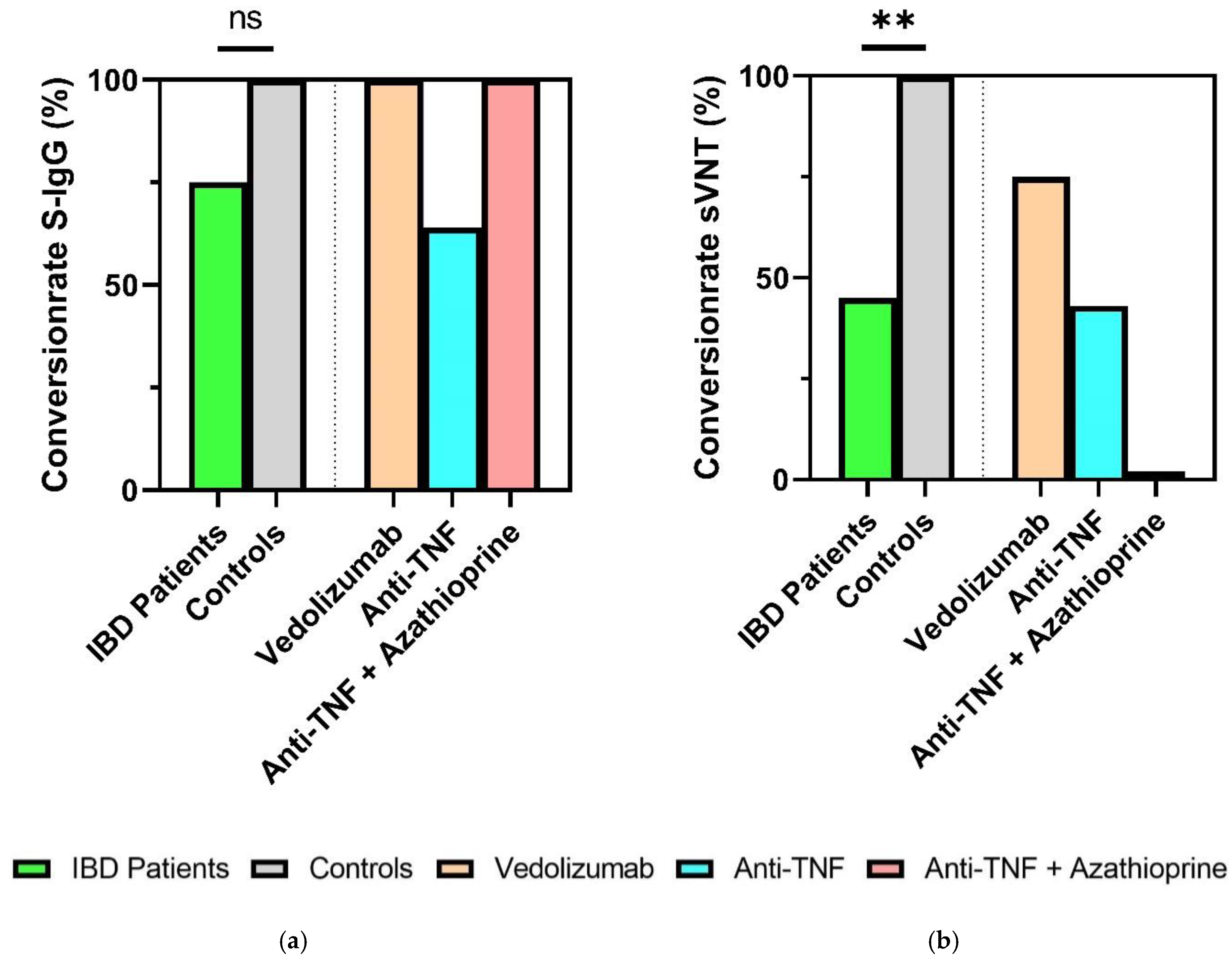
3.3. Reduced Seroconversion Rates in IBD Patients Six Months after SARS-CoV-2 mRNA-Vaccination
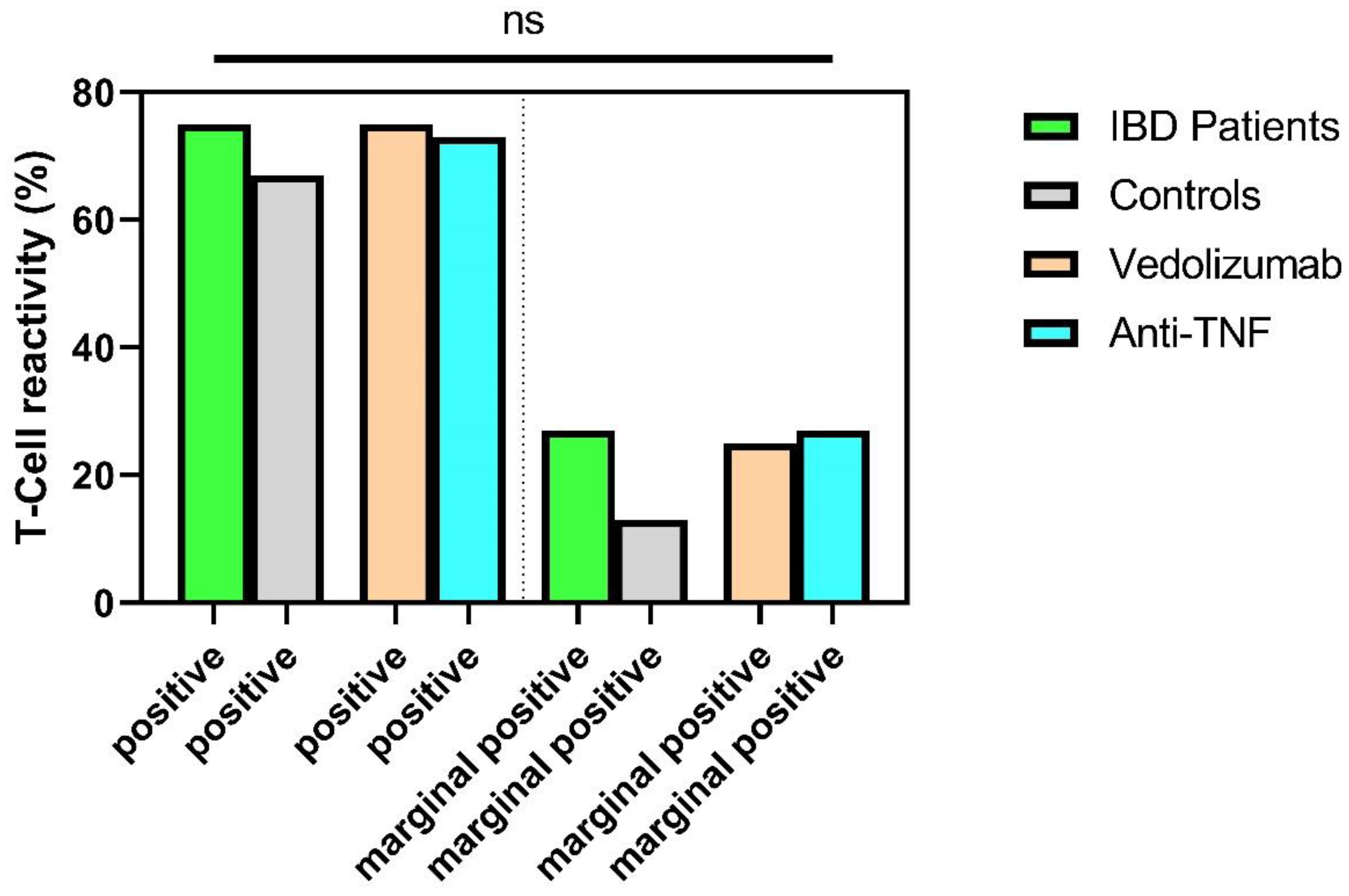
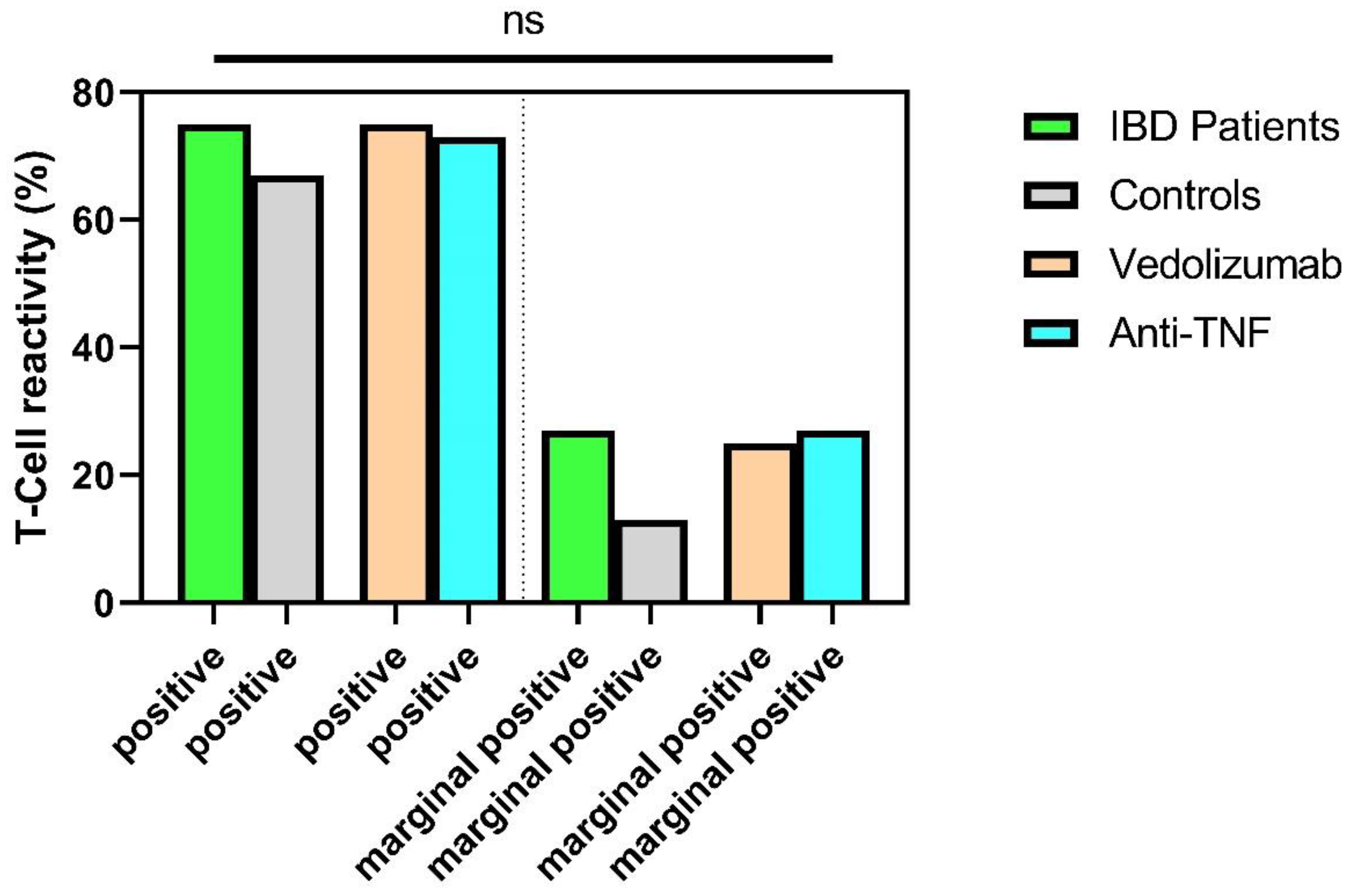
3.4. Sustained T-Cellular Reactivity in Immunosuppressed IBD Patients 6 Months after Second Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [CrossRef] [PubMed] [Green Version]
- Vollenberg, R.; Matern, P.; Nowacki, T.; Fuhrmann, V.; Padberg, J.-S.; Ochs, K.; Schütte-Nütgen, K.; Strauß, M.; Schmidt, H.; Tepasse, P.-R. Prone Position in Mechanically Ventilated COVID-19 Patients: A Multicenter Study. J. Clin. Med. 2021, 10, 1046. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Tepasse, P.-R.; Hafezi, W.; Lutz, M.; Kühn, J.; Wilms, C.; Wiewrodt, R.; Sackarnd, J.; Keller, M.; Schmidt, H.H.; Vollenberg, R. Persisting SARS-CoV-2 viraemia after rituximab therapy: Two cases with fatal outcome and a review of the literature. Br. J. Haematol. 2020, 190, 185–188. [Google Scholar] [CrossRef]
- Kessel, C.; Vollenberg, R.; Masjosthusmann, K.; Hinze, C.; Wittkowski, H.; Debaugnies, F.; Nagant, C.; Corazza, F.; Vély, F.; Kaplanski, G.; et al. Discrimination of COVID-19 from Inflammation-Induced Cytokine Storm Syndromes Using Disease-Related Blood Biomarkers. Arthritis Rheumatol. 2021, 73, 1791–1799. [Google Scholar] [CrossRef]
- Jose, R.J.; Manuel, A. COVID-19 cytokine storm: The interplay between inflammation and coagulation. Lancet Respir. Med. 2020, 8, e46–e47. [Google Scholar] [CrossRef]
- Deer, R.R.; Rock, M.A.; Vasilevsky, N.; Carmody, L.; Rando, H.; Anzalone, A.J.; Basson, M.D.; Bennett, T.D.; Bergquist, T.; Boudreau, E.A.; et al. Characterizing Long COVID: Deep Phenotype of a Complex Condition. EBioMedicine 2021, 74, 103722. [Google Scholar] [CrossRef]
- Varghese, J.; Sandmann, S.; Ochs, K.; Schrempf, I.-M.; Frömmel, C.; Dugas, M.; Schmidt, H.H.; Vollenberg, R.; Tepasse, P.-R. Persistent symptoms and lab abnormalities in patients who recovered from COVID-19. Sci. Rep. 2021, 11, 12775. [Google Scholar] [CrossRef]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the Frequency and Variety of Persistent Symptoms among Patients with COVID-19: A Systematic Review. JAMA Netw. Open 2021, 4, e2111417. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.-F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.-F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Beaugerie, L.; Rahier, J.-F.; Kirchgesner, J. Predicting, Preventing, and Managing Treatment-Related Complications in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2020, 18, 1324–1335.e2. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Jena, A.; Kumar-M, P.; Sharma, V.; Sebastian, S. Risk and outcomes of coronavirus disease in patients with inflammatory bowel disease: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2021, 9, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Fachgruppe COVRIIN beim Robert-Koch-Institut. Medikamentöse Therapie bei COVID-19 mit Bewertung Durch die Fachgruppe COVRIIN beim Robert Koch-Institut Stand: 2022; The Robert Koch Institute: Berlin, Germany, 2022. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Vollenberg, R.; Tepasse, P.-R.; Kühn, J.E.; Hennies, M.; Strauss, M.; Rennebaum, F.; Schomacher, T.; Boeckel, G.; Lorentzen, E.; Bokemeyer, A.; et al. Humoral Immune Response in IBD Patients Three and Six Months after Vaccination with the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2. Biomedicines 2022, 10, 171. [Google Scholar] [CrossRef]
- Chanchlani, N.; Lin, S.; Chee, D.; Hamilton, B.; Nice, R.; Arkir, Z.; Bewshea, C.; Cipriano, B.; Derikx, L.A.A.P.; Dunlop, A.; et al. Adalimumab and Infliximab Impair SARS-CoV-2 Antibody Responses: Results from a Therapeutic Drug Monitoring Study in 11 422 Biologic-Treated Patients. J. Crohns. Colitis 2022, 16, 389–397. [Google Scholar] [CrossRef]
- Kappelman, M.D.; Weaver, K.N.; Boccieri, M.; Firestine, A.; Zhang, X.; Long, M.D. Humoral Immune Response to Messenger RNA COVID-19 Vaccines Among Patients with Inflammatory Bowel Disease. Gastroenterology 2021, 161, 1340–1343.e2. [Google Scholar] [CrossRef]
- Kennedy, N.A.; Goodhand, J.R.; Bewshea, C.; Nice, R.; Chee, D.; Lin, S.; Chanchlani, N.; Butterworth, J.; Cooney, R.; Croft, N.M.; et al. Anti-SARS-CoV-2 antibody responses are attenuated in patients with IBD treated with infliximab. Gut 2021, 70, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Melmed, G.Y.; Botwin, G.J.; Sobhani, K.; Li, D.; Prostko, J.; Figueiredo, J.; Cheng, S.; Braun, J.; McGovern, D.P.B. Antibody Responses After SARS-CoV-2 mRNA Vaccination in Adults with Inflammatory Bowel Disease. Ann. Intern. Med. 2021, 174, 1768–1770. [Google Scholar] [CrossRef] [PubMed]
- Pozdnyakova, V.; Botwin, G.J.; Sobhani, K.; Prostko, J.; Braun, J.; McGovern, D.P.B.; Melmed, G.Y.; Appel, K.; Banty, A.; Feldman, E.; et al. Decreased Antibody Responses to Ad26.COV2.S Relative to SARS-CoV-2 mRNA Vaccines in Patients With Inflammatory Bowel Disease. Gastroenterology 2021, 161, 2041–2043.e1. [Google Scholar] [CrossRef] [PubMed]
- Reuken, P.A.; Andreas, N.; Grunert, P.C.; Glöckner, S.; Kamradt, T.; Stallmach, A. T Cell Response After SARS-CoV-2 Vaccination in Immunocompromised Patients with Inflammatory Bowel Disease. J. Crohns. Colitis 2022, 16, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Spencer, E.A.; Klang, E.; Dolinger, M.; Pittman, N.; Dubinsky, M.C. Seroconversion Following SARS-CoV-2 Infection or Vaccination in Pediatric IBD Patients. Inflamm. Bowel Dis. 2021, 27, 1862–1864. [Google Scholar] [CrossRef] [PubMed]
- Tepasse, P.-R.; Vollenberg, R.; Nowacki, T.M. Vaccination against SARS-CoV-2 in Patients with Inflammatory Bowel Diseases: Where Do We Stand? Life 2021, 11, 1220. [Google Scholar] [CrossRef]
- Wong, S.-Y.; Dixon, R.; Martinez Pazos, V.; Gnjatic, S.; Colombel, J.-F.; Cadwell, K. Serologic Response to Messenger RNA Coronavirus Disease 2019 Vaccines in Inflammatory Bowel Disease Patients Receiving Biologic Therapies. Gastroenterology 2021, 161, 715–718.e4. [Google Scholar] [CrossRef]
- von Rhein, C.; Scholz, T.; Henss, L.; Kronstein-Wiedemann, R.; Schwarz, T.; Rodionov, R.N.; Corman, V.M.; Tonn, T.; Schnierle, B.S. Comparison of potency assays to assess SARS-CoV-2 neutralizing antibody capacity in COVID-19 convalescent plasma. J. Virol. Methods 2021, 288, 114031. [Google Scholar] [CrossRef]
- Schwarz, T.; Tober-Lau, P.; Hillus, D.; Helbig, E.T.; Lippert, L.J.; Thibeault, C.; Koch, W.; Landgraf, I.; Michel, J.; Bergfeld, L.; et al. Delayed Antibody and T-Cell Response to BNT162b2 Vaccination in the Elderly, Germany. Emerg. Infect. Dis. 2021, 27, 2174–2178. [Google Scholar] [CrossRef]
- Hillus, D.; Schwarz, T.; Tober-Lau, P.; Vanshylla, K.; Hastor, H.; Thibeault, C.; Jentzsch, S.; Helbig, E.T.; Lippert, L.J.; Tscheak, P.; et al. Safety, reactogenicity, and immunogenicity of homologous and heterologous prime-boost immunisation with ChAdOx1 nCoV-19 and BNT162b2: A prospective cohort study. Lancet Respir. Med. 2021, 9, 1255–1265. [Google Scholar] [CrossRef]
- Frey, S.; Chowdhury, R.; Connolly, C.M.; Werbel, W.A.; Segev, D.L.; Parian, A.M. Antibody Response Six Months after SARS-CoV-2 mRNA Vaccination in Patients with Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Caldera, F.; Knutson, K.L.; Saha, S.; Wald, A.; Phan, H.S.; Chun, K.; Grimes, I.; Lutz, M.; Hayney, M.S.; Farraye, F.A. Humoral Immunogenicity of mRNA COVID-19 Vaccines Among Patients with Inflammatory Bowel Disease and Healthy Controls. Am. J. Gastroenterol. 2022, 117, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Cerna, K.; Duricova, D.; Lukas, M.; Machkova, N.; Hruba, V.; Mitrova, K.; Kubickova, K.; Kostrejova, M.; Teplan, V.; Vasatko, M.; et al. Anti-SARS-CoV-2 Vaccination and Antibody Response in Patients with Inflammatory Bowel Disease on Immune-modifying Therapy: Prospective Single-Tertiary Study. Inflamm. Bowel Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Doherty, J.; Morain, N.O.; Stack, R.; Girod, P.; Tosetto, M.; Inzitiari, R.; Sheridan, J.; Cullen, G.; Mc Dermott, E.; Buckley, M.; et al. Reduced serological response to COVID-19 vaccines in patients with IBD is further diminished by TNF inhibitor therapy; Early results of the VARIATION study (VAriability in Response in IBD Against SARS-COV-2 ImmunisatiON). J. Crohns. Colitis 2022. [Google Scholar] [CrossRef]
- Alexander, J.L.; Kennedy, N.A.; Ibraheim, H.; Anandabaskaran, S.; Saifuddin, A.; Castro Seoane, R.; Liu, Z.; Nice, R.; Bewshea, C.; D’Mello, A.; et al. COVID-19 vaccine-induced antibody responses in immunosuppressed patients with inflammatory bowel disease (VIP): A multicentre, prospective, case-control study. Lancet Gastroenterol. Hepatol. 2022, 7, 342–352. [Google Scholar] [CrossRef]
- Shehab, M.; Alrashed, F.; Alfadhli, A.; Alotaibi, K.; Alsahli, A.; Mohammad, H.; Cherian, P.; Al-Khairi, I.; Alphonse Thanaraj, T.; Channanath, A.; et al. Serological Response to BNT162b2 and ChAdOx1 nCoV-19 Vaccines in Patients with Inflammatory Bowel Disease on Biologic Therapies. Vaccines 2021, 9, 1471. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.A.; Lin, S.; Goodhand, J.R.; Chanchlani, N.; Hamilton, B.; Bewshea, C.; Nice, R.; Chee, D.; Cummings, F., Jr.; Fraser, A.; et al. Infliximab is associated with attenuated immunogenicity to BNT162b2 and ChAdOx1 nCoV-19 SARS-CoV-2 vaccines in patients with IBD. Gut 2021, 70, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Classen, J.M.; Muzalyova, A.; Nagl, S.; Fleischmann, C.; Ebigbo, A.; Römmele, C.; Messmann, H.; Schnoy, E. Antibody response to SARS-CoV-2 vaccination in patients with inflammatory bowel disease—results of a single-center cohort study in a tertiary hospital in Germany. Dig. Dis. 2021. [Google Scholar] [CrossRef]
- Shehab, M.; Abu-Farha, M.; Alrashed, F.; Alfadhli, A.; Alotaibi, K.; Alsahli, A.; Alphonse Thanaraj, T.; Channanath, A.; Ali, H.; Abubaker, J.; et al. Immunogenicity of BNT162b2 Vaccine in Patients with Inflammatory Bowel Disease on Infliximab Combination Therapy: A Multicenter Prospective Study. J. Clin. Med. 2021, 10, 5362. [Google Scholar] [CrossRef]
- Wörns, M.A.; Teufel, A.; Kanzler, S.; Shrestha, A.; Victor, A.; Otto, G.; Lohse, A.W.; Galle, P.R.; Höhler, T. Incidence of HAV and HBV infections and vaccination rates in patients with autoimmune liver diseases. Am. J. Gastroenterol. 2008, 103, 138–146. [Google Scholar] [CrossRef]
- Lin, S.; Kennedy, N.A.; Saifuddin, A.; Sandoval, D.M.; Reynolds, C.J.; Seoane, R.C.; Kottoor, S.H.; Pieper, F.P.; Lin, K.-M.; Butler, D.K.; et al. Antibody decay, T cell immunity and breakthrough infections following two SARS-CoV-2 vaccine doses in inflammatory bowel disease patients treated with infliximab and vedolizumab. Nat. Commun. 2022, 13, 1379. [Google Scholar] [CrossRef]
- Kapetanovic, M.C.; Saxne, T.; Nilsson, J.-A.; Geborek, P. Influenza vaccination as model for testing immune modulation induced by anti-TNF and methotrexate therapy in rheumatoid arthritis patients. Rheumatology 2007, 46, 608–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapetanovic, M.C.; Saxne, T.; Sjöholm, A.; Truedsson, L.; Jönsson, G.; Geborek, P. Influence of methotrexate, TNF blockers and prednisolone on antibody responses to pneumococcal polysaccharide vaccine in patients with rheumatoid arthritis. Rheumatology 2006, 45, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Andrade, P.; Santos-Antunes, J.; Rodrigues, S.; Lopes, S.; Macedo, G. Treatment with infliximab or azathioprine negatively impact the efficacy of hepatitis B vaccine in inflammatory bowel disease patients. J. Gastroenterol. Hepatol. 2015, 30, 1591–1595. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.A.; Haraoui, B.; Kumar, D.; Marshall, J.K.; Bissonnette, R.; Bitton, A.; Bressler, B.; Gooderham, M.; Ho, V.; Jamal, S.; et al. Vaccination Guidelines for Patients with Immune-Mediated Disorders on Immunosuppressive Therapies. J. Cutan. Med. Surg. 2019, 23, 50–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scribano, M.L. Vedolizumab for inflammatory bowel disease: From randomized controlled trials to real-life evidence. World J. Gastroenterol. 2018, 24, 2457–2467. [Google Scholar] [CrossRef]
- Li, D.; Xu, A.; Mengesha, E.; Elyanow, R.; Gittelman, R.M.; Chapman, H.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Pozdnyakova, V.; et al. The T-cell clonal response to SARS-CoV-2 vaccination in inflammatory bowel disease patients is augmented by anti-TNF therapy and often deficient in antibody-responders. medRxiv 2021. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e0024721. [Google Scholar] [CrossRef]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.-C.; Tiu, C.; Hu, Z.; Chen, V.C.-W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Naschitz, J.E.; Kertes, J.; Pinto, G.; Zaigraykin, N.; Oz, D.; Goland, E.; Nasser, S.; Supino-Rosin, L.; Lazar, R.; Ekka-Zohar, A. Comparison of Covid-19 antibody status after vaccination between residents in long-term geriatric care and residents assisted-living facilities. Infect. Dis. 2022, 54, 292–296. [Google Scholar] [CrossRef]
- Sourij, C.; Tripolt, N.J.; Aziz, F.; Aberer, F.; Forstner, P.; Obermayer, A.M.; Kojzar, H.; Kleinhappl, B.; Pferschy, P.N.; Mader, J.K.; et al. Humoral immune response to COVID-19 vaccination in diabetes is age-dependent but independent of type of diabetes and glycaemic control: The prospective COVAC-DM cohort study. Diabetes Obes. Metab. 2022, 24, 849–858. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Controls (n = 9) | IBD (n = 20) | p-Value 1 | Vedolizumab (n = 4) | Anti-TNF (n = 14) | Anti-TNF + Azathioprine (n = 2) | p-Value 2 | |
|---|---|---|---|---|---|---|---|---|
| Patient characteristics | Age, years median (IQR) | 42 (37–57) | 39 (26–47) | 0.216 | 40 (35–55) | 36 (24–49) | 39 | 0.709 |
| Sex, male (%) | 5 (55) | 12 (60) | 0.822 | 4 (100) | 8 (57) | 2 (100) | 0.057 | |
| BMI (kg/m2) | 23 (22–24) | 25 (23–28) | 0.198 | 23 (21–31) | 25 (23–28) | 27 | 0.613 | |
| IBD | Crohn’s disease (%) | 0 (0) | 9 (45) | 2 (50) | 4 (29) | 2 (100) | 0.634 | |
| CDAI score, median (IQR) | 0 (0) | 0 (0–0) | 120 (0–120) | 0 (0–0) | 0 (0–0) | 0.104 | ||
| Ulcerative colitis (%) | 0 (0) | 11 (55) | 2 (50) | 10 (71) | 0 (0) | 0.634 | ||
| Mayo score, median (IQR) | 0 (0) | 2 (0–3.5) | 2.5 (2–2.5) | 0 (0–0) | 0 (0–0) | 0.554 | ||
| Medication | Prednisolone p.o. (%) | 0 (0) | 2 (10) | 2 (50) | 0 (0) | 0 (0) | 0.012 | |
| Budesonide p.o. (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1.000 | ||
| Budesonide supp. (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1.000 | ||
| Mesalazine p.o. (%) | 0 (0) | 4 (20) | 0 (0) | 4 (29) | 0 (0) | 0.159 | ||
| Mesalazine supp. (%) | 0 (0) | 2 (10) | 0 (0) | 2 (14) | 0 (0) | 0.360 | ||
| Pre-existing conditions | Cardiovascular disease | 0 (0) | 1 (5) | 1 (25) | 0 (0) | 0 (0) | 0.086 | |
| Respiratory disease (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1.000 | ||
| Kidney insufficiency (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1.000 | ||
| Metastatic neoplasm (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1.000 | ||
| Diabetes (%) | 0 (0) | 1 (5) | 1 (25) | 0 (0) | 0 (0) | 0.086 | ||
| Hematologic malignancy (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| T-Cell-Reactivity | IBD Patients (n = 15) | Controls (n = 8) | p-Value 1 | Vedolizumab (n = 4) | Anti-TNF (n = 11) | Anti-TNF + Azathioprine (n = 0) | p-Value 2 |
|---|---|---|---|---|---|---|---|
| Positive T-Cell reactivity (%) | 11 (73) | 6 (67) | 0.189 | 3 (75) | 8 (73) | 0 (0) | 1.000 |
| Marginal T-Cell reactivity (%) | 4 (27) | 1 (13) | 0.189 | 1 (25) | 3 (27) | 0 (0) | 1.000 |
| Negative T-Cell reactivity (%) | 0 (0) | 1 (13) | 0.189 | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Humoral Reactivity | IBD Patients (n = 20) | Controls (n = 8) | p-Value 1 | Vedolizumab (n = 4) | Anti-TNF (n = 14) | Anti-TNF + Azathioprine (n = 2) | p-Value 2 |
| SARS-CoV-2 S-IgG (AU/mL), median (IQR) | 189 (22–514) | 1018 (618–1583) | 0.001 | 694 (370–3633) | 141 (0–340) | 98 | 0.057 |
| Seroconversion rate S-IgG (%) | 75 | 100 | 0.153 | 100 | 64 | 100 | 0.640 |
| sVNT (%), median (IQR) | 14 (0–52) | 79 (57–85) | 0.002 | 55 (31–87) | 2 (0–42) | 0 | 0.042 |
| Seroconversion rate sVNT (%) | 45 | 100 | 0.005 | 75 | 43 | 0 | 0.088 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vollenberg, R.; Tepasse, P.-R.; Lorentzen, E.; Nowacki, T.M. Impaired Humoral Immunity with Concomitant Preserved T Cell Reactivity in IBD Patients on Treatment with Infliximab 6 Month after Vaccination with the SARS-CoV-2 mRNA Vaccine BNT162b2: A Pilot Study. J. Pers. Med. 2022, 12, 694. https://doi.org/10.3390/jpm12050694
Vollenberg R, Tepasse P-R, Lorentzen E, Nowacki TM. Impaired Humoral Immunity with Concomitant Preserved T Cell Reactivity in IBD Patients on Treatment with Infliximab 6 Month after Vaccination with the SARS-CoV-2 mRNA Vaccine BNT162b2: A Pilot Study. Journal of Personalized Medicine. 2022; 12(5):694. https://doi.org/10.3390/jpm12050694
Chicago/Turabian StyleVollenberg, Richard, Phil-Robin Tepasse, Eva Lorentzen, and Tobias Max Nowacki. 2022. "Impaired Humoral Immunity with Concomitant Preserved T Cell Reactivity in IBD Patients on Treatment with Infliximab 6 Month after Vaccination with the SARS-CoV-2 mRNA Vaccine BNT162b2: A Pilot Study" Journal of Personalized Medicine 12, no. 5: 694. https://doi.org/10.3390/jpm12050694
APA StyleVollenberg, R., Tepasse, P.-R., Lorentzen, E., & Nowacki, T. M. (2022). Impaired Humoral Immunity with Concomitant Preserved T Cell Reactivity in IBD Patients on Treatment with Infliximab 6 Month after Vaccination with the SARS-CoV-2 mRNA Vaccine BNT162b2: A Pilot Study. Journal of Personalized Medicine, 12(5), 694. https://doi.org/10.3390/jpm12050694