
Collaborative Approach to Reach Everyone with Familial Hypercholesterolemia: CARE-FH Protocol

 , ,
, ,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
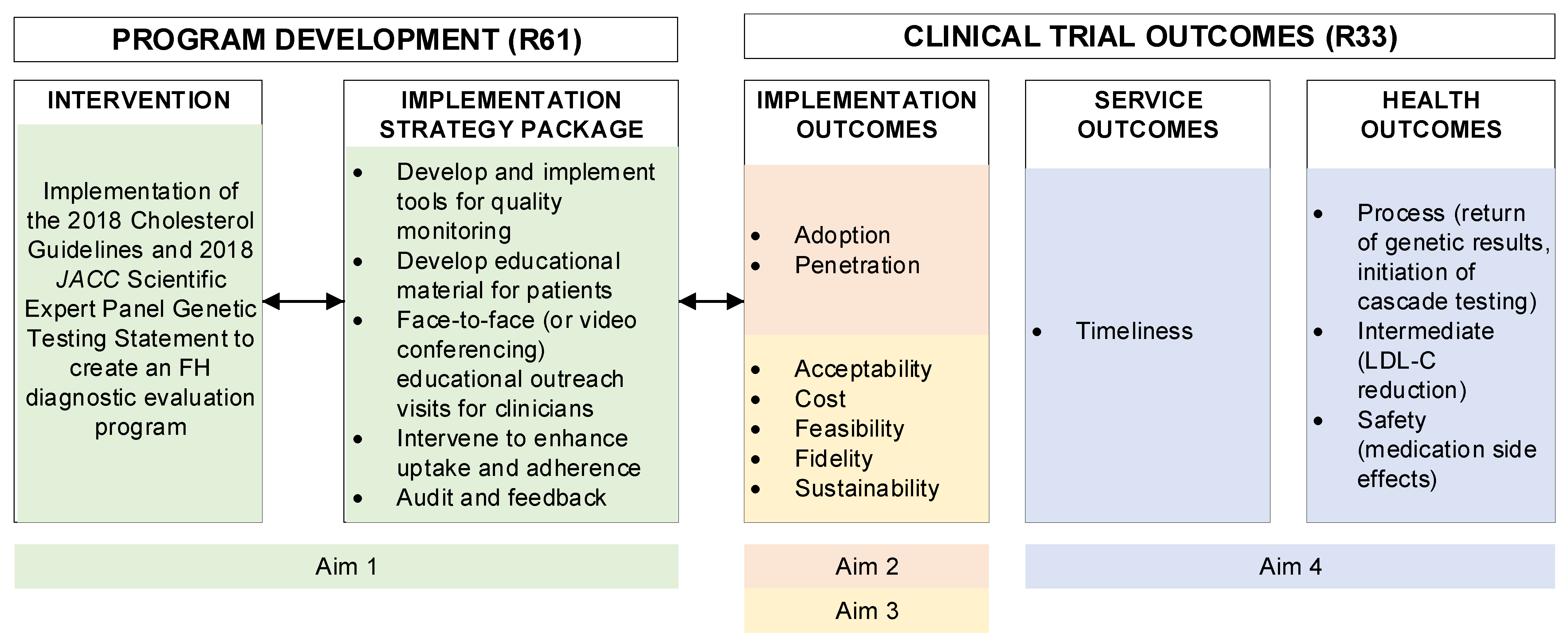
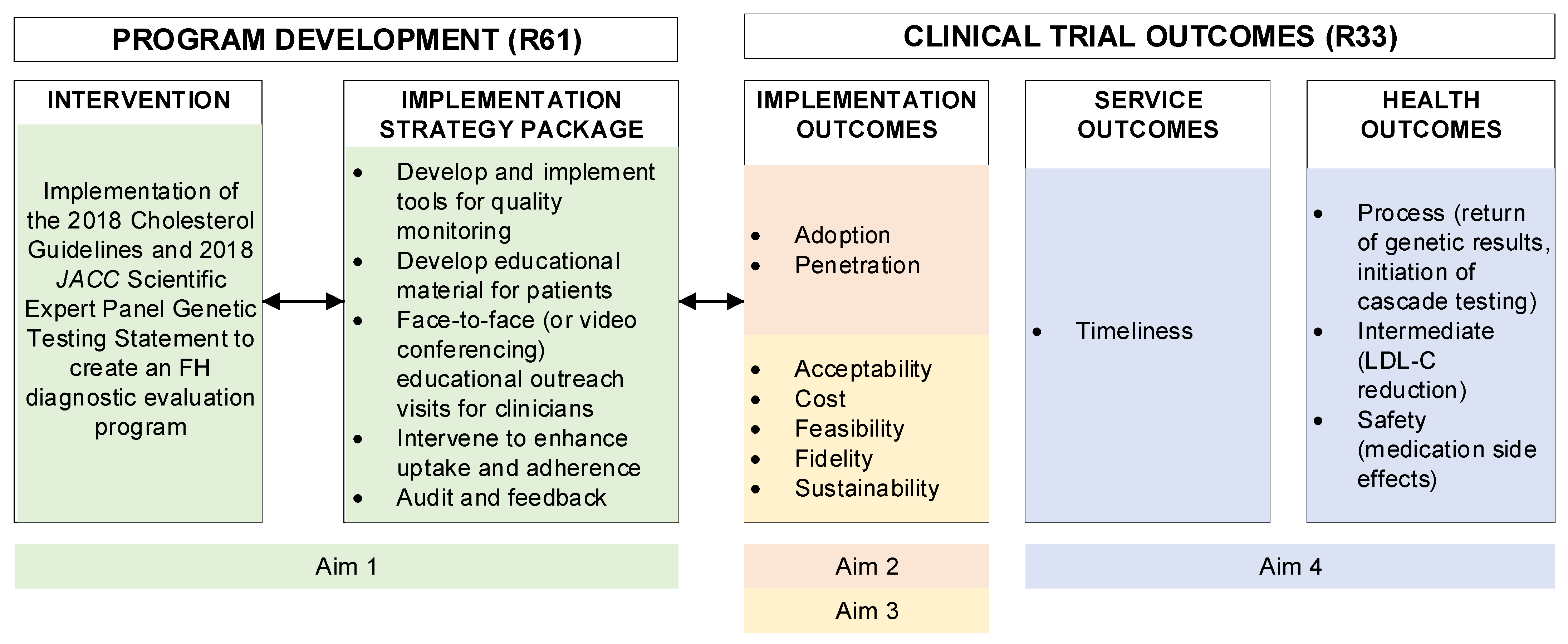
2.1. Overview
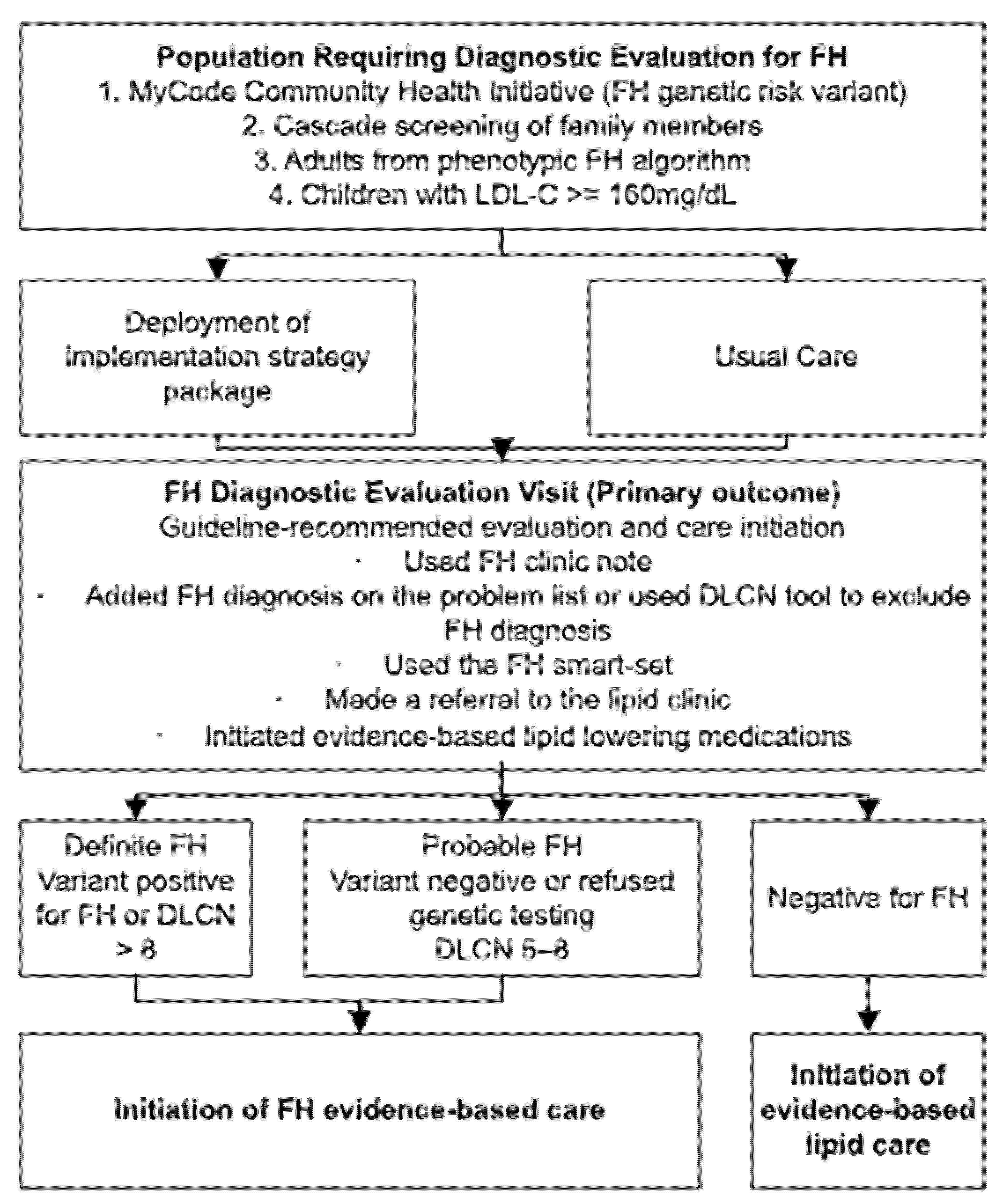
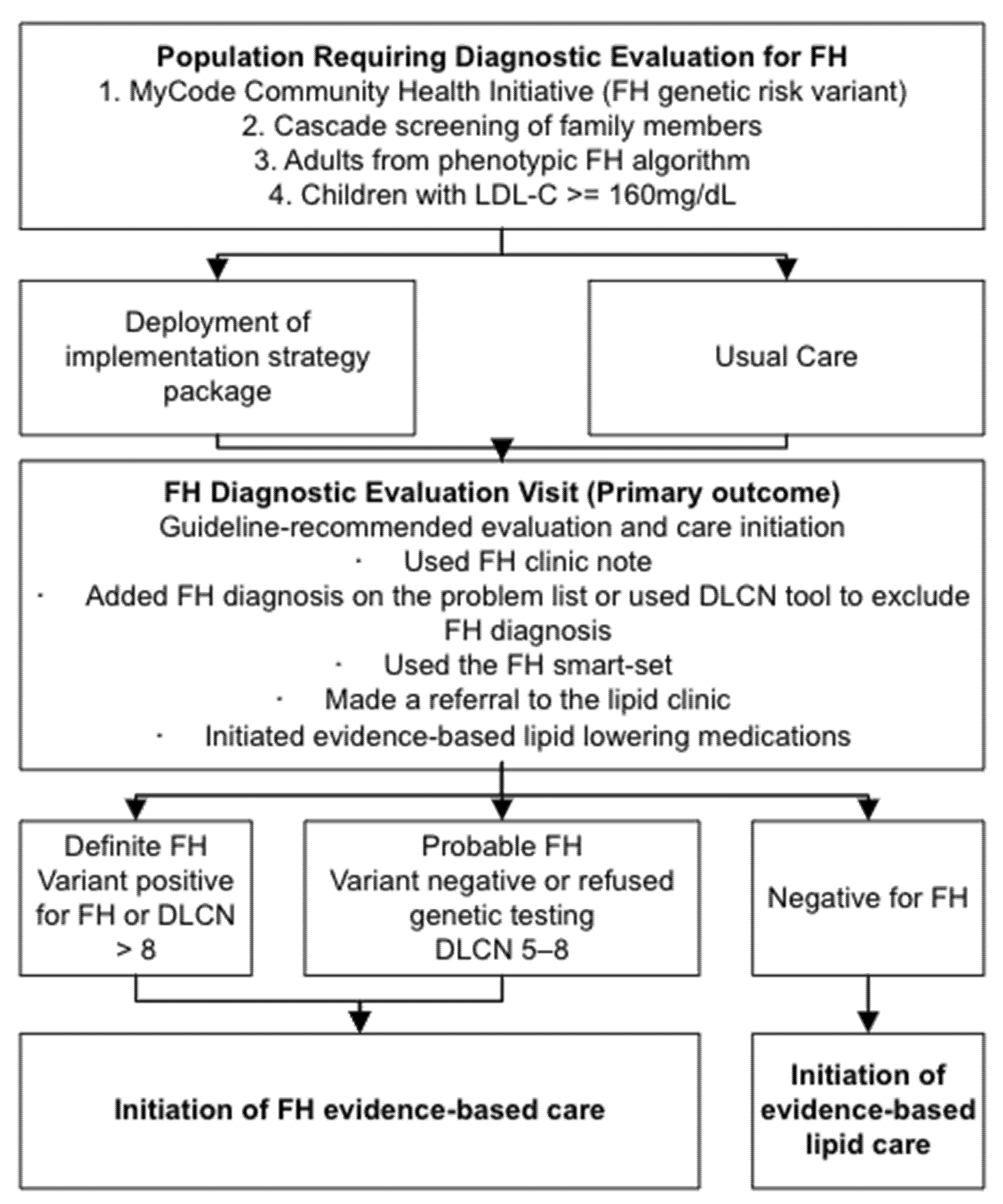
2.2. FH Diagnostic Evaluation Program
- -
- Used FH clinic note to document care
- -
- Added FH diagnosis on the problem list or used the Dutch Lipid Clinic Network score (DLCN) tool to exclude FH diagnosis
- -
- Used the FH smart-set (i.e., ordered a genetic test for FH)
- -
- Made a referral to the lipid clinic [12]
- -
- Initiate evidence-based lipid lowering medications
2.3. Potenital Implementation Strategies
3. Specific Aim 1 (R61): Design a Clinical Trial to Assess Multi-Level Implementation Strategies for Improving FH Diagnosis in an Integrated Health System
3.1. Objectives and Work Plan by Team
3.1.1. Implementation Science Team (ImpT)
- Identification of healthcare system level barriers.
- Tailor selected implementation strategies to meet the needs of the clinical implementation sites.
- Alpha testing of implementation strategy package into two preselected clinical implementation sites.
- Define a measurement of implementation outcomes.
Survey
Contextual Inquiries
Deliberative Engagement Meetings
3.1.2. Medical Science Team (MedT)
- Partner with the InfT to revise content for EHR tools in the implementation strategy package and subsequent adaptations.
- Finalize FH care plan for adults and children.
- Finalize strategy for incorporation of genetics counselors and specialty referrals into a care plan.
- Finalize study timeline, including the schedule and sites for rolling out the implementation strategy package.
- Alpha test the implementation strategy package at one adult and one pediatric practice site.
3.1.3. Informatics and Data Science Team (InfT)
- Partner with the MedT to develop content for building EHR tools for the implementation strategy
- Provide EHR support for the alpha test.
- Finalize the data analysis plan.
- Collect baseline outcomes data, including estimates of patient flow, for the clinical trial design.
4. Specific Aim 2 (R33): Compare FH Diagnostic Evaluation Rates among Primary Care Clinicians Who Receive the Implementation Strategy Package versus Those Who Do Not
Data Collection and Analysis for Adoption and Penetration
5. Specific Aim 3 (R33): Measure Implementation Success of an Organized FH Diagnostic Evaluation Program
- What is the acceptability of an FH diagnostic evaluation program across different demographic regions of the health system?
- How does the implementation strategy package fit (from Aim 2) within and between different clinic settings and patient populations and what adaptations were made?
- What are the costs to the healthcare system to implement and maintain an FH diagnostic evaluation program?
5.1. Data Collection and Analysis for Each Implementation Outcome
5.1.1. Acceptability
5.1.2. Cost
5.1.3. Feasibility
5.1.4. Fidelity
5.1.5. Sustainability
6. Specific Aim 4 (R33): Measure Patient-Related Outcomes after Implementation of an FH Diagnostic Evaluation Program
6.1. Data Collection and Analysis for Service and Health Outcomes
6.1.1. Timeliness
6.1.2. Function
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- NICE’s Guideline Updates Team. Familial Hypercholesterolaemia: Identification and Management: Evidence Reviews for Case-Finding, Diagnosis and Statin Monotherapy; National Institute for Health and Care Excellence: London, UK, 2017. [Google Scholar]
- Watts, G.F.; Gidding, S.S.; Mata, P.; Pang, J.; Sullivan, D.R.; Yamashita, S.; Raal, F.J.; Santos, R.D.; Ray, K.K. Familial hypercholesterolaemia: Evolving knowledge for designing adaptive models of care. Nat. Rev. Cardiol. 2020, 17, 360–377. [Google Scholar] [CrossRef] [PubMed]
- Goodman, D.S.; Hulley, S.B.; Clark, L.T.; Davis, C.E.; Fuster, V.; LaRosa, J.C.; Oberman, A.; Schaefer, E.J.; Steinberg, D.; Brown, W.V.; et al. Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. The Expert Panel. Arch. Intern. Med. 1988, 148, 36–69. [Google Scholar] [CrossRef]
- deGoma, E.M.; Ahmad, Z.S.; O’Brien, E.C.; Kindt, I.; Shrader, P.; Newman, C.B.; Pokharel, Y.; Baum, S.J.; Hemphill, L.C.; Hudgins, L.C.; et al. Treatment Gaps in Adults With Heterozygous Familial Hypercholesterolemia in the United States: Data from the CASCADE-FH Registry. Circ. Cardiovasc. Genet. 2016, 9, 240–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duell, P.B.; Gidding, S.S.; Andersen, R.L.; Knickelbine, T.; Anderson, L.; Gianos, E.; Shrader, P.; Kindt, I.; O’Brien, E.C.; McCann, D.; et al. Longitudinal low density lipoprotein cholesterol goal achievement and cardiovascular outcomes among adult patients with familial hypercholesterolemia: The CASCADE FH registry. Atherosclerosis 2019, 289, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Luirink, I.K.; Wiegman, A.; Kusters, D.M.; Hof, M.H.; Groothoff, J.W.; de Groot, E.; Kastelein, J.J.P.; Hutten, B.A. 20-Year Follow-up of Statins in Children with Familial Hypercholesterolemia. N. Engl. J. Med. 2019, 381, 1547–1556. [Google Scholar] [CrossRef]
- Jones, L.K.; Walters, N.; Brangan, A.; Ahmed, C.D.; Salome, G.C.; Sheldon, A.; McGowan, M.; Rahm, A.K.; Sturm, A.C. Abstract 13161: Acceptability and Feasibility of Novel Screening Models and Family Communication Methods for Familial Hypercholesterolemia. Circulation 2020, 142, A13161. [Google Scholar] [CrossRef]
- Jones, L.K.; Sturm, A.C.; Seaton, T.L.; Gregor, C.; Gidding, S.S.; Williams, M.S.; Rahm, A.K. Barriers, facilitators, and solutions to familial hypercholesterolemia treatment. PLoS ONE 2020, 15, e0244193. [Google Scholar] [CrossRef]
- Banda, J.M.; Sarraju, A.; Abbasi, F.; Parizo, J.; Pariani, M.; Ison, H.; Briskin, E.; Wand, H.; Dubois, S.; Jung, K. Finding missed cases of familial hypercholesterolemia in health systems using machine learning. NPJ Digit. Med. 2019, 2, 23. [Google Scholar] [CrossRef] [Green Version]
- Safarova, M.S.; Liu, H.; Kullo, I.J. Rapid identification of familial hypercholesterolemia from electronic health records: The SEARCH study. J. Clin. Lipidol. 2016, 10, 1230–1239. [Google Scholar] [CrossRef]
- Jones, L.K.; McMinn, M.; Kann, D.; Lesko, M.; Sturm, A.C.; Walters, N.; Chen, N.; Fry, K.; Brownson, R.C.; Gidding, S.S.; et al. Evaluation of a multidisciplinary lipid clinic to improve the care of individuals with severe lipid conditions: A RE-AIM Framework Analysis. Implement. Sci. Commun. 2021, 2, 32. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.S.; Buchanan, A.H.; Davis, F.D.; Faucett, W.A.; Hallquist, M.L.G.; Leader, J.B.; Martin, C.L.; McCormick, C.Z.; Meyer, M.N.; Murray, M.F.; et al. Patient-Centered Precision Health In A Learning Health Care System: Geisinger’s Genomic Medicine Experience. Health Aff. (Proj. Hope) 2018, 37, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Tilberry, S.; Gregor, C.; Yaeger, L.; Hu, Y.; Sturm, A.C.; Seaton, T.L.; Waltz, T.J.; Rahm, A.K.; Goldberg, A.; et al. Implementation strategies to improve statin utilization in individuals with hypercholesterolemia: A systematic review and meta-analysis. Implement. Sci. 2021, 16, 40. [Google Scholar] [CrossRef] [PubMed]
- Tabak, R.G.; Khoong, E.C.; Chambers, D.A.; Brownson, R.C. Bridging research and practice: Models for dissemination and implementation research. Am. J. Prev. Med. 2012, 43, 337–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsen, P. Making sense of implementation theories, models and frameworks. Implement. Sci. 2015, 10, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, M.S.; Kirchner, J. Implementation science: What is it and why should I care? Psychiatry Res. 2020, 283, 112376. [Google Scholar] [CrossRef]
- Sturm, A.C.; Knowles, J.W.; Gidding, S.S.; Ahmad, Z.S.; Ahmed, C.D.; Ballantyne, C.M.; Baum, S.J.; Bourbon, M.; Carrie, A.; Cuchel, M.; et al. Clinical Genetic Testing for Familial Hypercholesterolemia: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2018, 72, 662–680. [Google Scholar] [CrossRef]
- Powell, B.J.; Waltz, T.J.; Chinman, M.J.; Damschroder, L.J.; Smith, J.L.; Matthieu, M.M.; Proctor, E.K.; Kirchner, J.E. A refined compilation of implementation strategies: Results from the Expert Recommendations for Implementing Change (ERIC) project. Implement. Sci. 2015, 10, 21. [Google Scholar] [CrossRef] [Green Version]
- Carey, D.J.; Fetterolf, S.N.; Davis, F.D.; Faucett, W.A.; Kirchner, H.L.; Mirshahi, U.; Murray, M.F.; Smelser, D.T.; Gerhard, G.S.; Ledbetter, D.H. The Geisinger MyCode community health initiative: An electronic health record-linked biobank for precision medicine research. Genet. Med. 2016, 18, 906–913. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, M.L.B.; McCormick, C.Z.; Lazzeri, A.L.; Lindbuchler, D.M.; Hallquist, M.L.G.; Manickam, K.; Buchanan, A.H.; Rahm, A.K.; Giovanni, M.A.; Frisbie, L.; et al. A Model for Genome-First Care: Returning Secondary Genomic Findings to Participants and Their Healthcare Providers in a Large Research Cohort. Am. J. Hum. Genet. 2018, 103, 328–337. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.S. Early Lessons from the Implementation of Genomic Medicine Programs. Annu. Rev. Genom. Hum. Genet. 2019, 20, 389–411. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.A.; Leader, J.B.; Wain, K.E.; Bodian, D.; Oetjens, M.T.; Ledbetter, D.H.; Martin, C.L.; Strande, N.T. Leveraging population-based exome screening to impact clinical care: The evolution of variant assessment in the Geisinger MyCode research project. Am. J. Med. Genet. C Semin. Med. Genet. 2021, 187, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Dewey, F.E.; Murray, M.F.; Overton, J.D.; Habegger, L.; Leader, J.B.; Fetterolf, S.N.; O’Dushlaine, C.; Van Hout, C.V.; Staples, J.; Gonzaga-Jauregui, C.; et al. Distribution and clinical impact of functional variants in 50,726 whole-exome sequences from the DiscovEHR study. Science 2016, 354, aaf6814. [Google Scholar] [CrossRef] [PubMed]
- MyCode Scorecard. Available online: https://www.geisinger.org/-/media/OneGeisinger/pdfs/ghs/research/mycode/mycode-scorecard.pdf?la=en (accessed on 15 January 2022).
- Jones, L.K.; Gidding, S.S.; Seaton, T.L.; Goldberg, A.; Gregor, C.; Sturm, A.C.; Brownson, R.C.; Rahm, A.K.; Williams, M.S. Developing implementation strategies to improve uptake of guideline-recommended treatments for individuals with familial hypercholesterolemia: A protocol. Res. Soc. Adm. Pharm. 2020, 16, 390–395. [Google Scholar] [CrossRef]
- Proctor, E.K.; Powell, B.J.; McMillen, J.C. Implementation strategies: Recommendations for specifying and reporting. Implement. Sci. 2013, 8, 139. [Google Scholar] [CrossRef] [Green Version]
- Weiner, B.J.; Lewis, C.C.; Stanick, C.; Powell, B.J.; Dorsey, C.N.; Clary, A.S.; Boynton, M.H.; Halko, H. Psychometric assessment of three newly developed implementation outcome measures. Implement. Sci. 2017, 12, 108. [Google Scholar] [CrossRef]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef] [Green Version]
- Hemming, K.; Taljaard, M.; McKenzie, J.E.; Hooper, R.; Copas, A.; Thompson, J.A.; Dixon-Woods, M.; Aldcroft, A.; Doussau, A.; Grayling, M.; et al. Reporting of stepped wedge cluster randomised trials: Extension of the CONSORT 2010 statement with explanation and elaboration. BMJ (Clin. Res. Ed.) 2018, 363, k1614. [Google Scholar] [CrossRef] [Green Version]
- Hussey, M.A.; Hughes, J.P. Design and analysis of stepped wedge cluster randomized trials. Contemp. Clin. Trials 2007, 28, 182–191. [Google Scholar] [CrossRef]
- Hu, Y.; Hoover, D.R. Non-randomized and randomized stepped-wedge designs using an orthogonalized least squares framework. Stat. Methods Med. Res. 2018, 27, 1202–1218. [Google Scholar] [CrossRef] [Green Version]
- RStudio Team. RStudio: Integrated Development for R. Available online: http://www.rstudio.com/ (accessed on 15 January 2022).
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proctor, E.K.; Landsverk, J.; Aarons, G.; Chambers, D.; Glisson, C.; Mittman, B. Implementation research in mental health services: An emerging science with conceptual, methodological, and training challenges. Adm. Policy Ment. Health 2009, 36, 24–34. [Google Scholar] [CrossRef]
- Pope, C.; Ziebland, S.; Mays, N. Analysing qualitative data. BMJ Br. Med. J. 2000, 320, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programme; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Int J. Technol. Assess. Health Care 2013, 29, 117–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiltsey Stirman, S.; Baumann, A.A.; Miller, C.J. The FRAME: An expanded framework for reporting adaptations and modifications to evidence-based interventions. Implement. Sci 2019, 14, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Name of Strategy * | Study Specific Definition | Actor | Action | Action Target |
|---|---|---|---|---|
| Develop and implement tools for quality monitoring | EHR tools to order labs, record results, and document FH care | ImpT, MedT, and InfT | Use EHR to record, order, and prescribe FH Care | Service and health outcomes |
| Develop educational materials | Education regarding guidelines for identification and treatment of FH | MedT and InfT | Create a CME course for clinicians about FH. Explore clinician workflow and educational needs to design novel focused educational interventions integrated within clinical workflows to support evidence-based care | MedT ready to train clinicians on FH |
| Conduct educational outreach visits | CME educational material for FH that is presented to each clinic | MedT and clinicians | Attend CME course on FH | Improve knowledge about FH |
| Intervene with patients to enhance uptake and adherence | Reach out directly to patients to recommend screening for FH | Clinicians and ImpT | Letter sent to the patient. Clinician schedules patient for appointment. | Patients diagnosed with FH from those at-risk |
| Identify and prepare champions | Clinical lipid champions | MedT | Identify and train lipid champions | Improved performance of study metrics, reduced costs |
| Stage FH care delivery model scale up | Develop the timeline for the stepped-wedge rollout to primary care | Leadership team | Notify practices of roll out and schedule education | Begin the trial |
| Audit and provide feedback | Provide aggregate level feedback to clinics on diagnosing FH | MedT, InfT, and clinical leadership | Report back to clinicians’ aggregate level data | Improve effectiveness of the FH Diagnosis Program |
| Advisory board review | Clinical trial protocol | Advisory Board | Provide feedback on the clinical trial regarding protocol, generalizability and ethical issues | Protocol revision based on feedback |
| Domain | Aim | Outcome | Construct Measured | Data Source |
|---|---|---|---|---|
| Implementation | 2 | Adoption | FH diagnostic evaluation defined as completed of one of the following:
| EHR, administrative data |
| Penetration | Proportion of the primary care clinicians that completed the five components of the FH diagnostic evaluation compared to those that did not use it. | |||
| 3 | Acceptability | Clinician and patient satisfaction and self-efficacy with the implementation strategy package | Semi-structured interviews | |
| Cost | Cost to implement the implementation strategy package | Micro-costing | ||
| Feasibility | Clinician adoption and penetration for completion of the FH diagnostic evaluation and measured utility of implementation strategy package | Semi-structured interviews and EHR data | ||
| Fidelity | Documentation of adaptations to the FH diagnostic evaluation program | Checklist, direct observation | ||
| Sustainability | Potential for institutionalization | Surveys, Advisory board consultation | ||
| Service | 4 | Timeliness | Time to: FH screen, completion of diagnostic evaluation, medication initiation | EHR, administrative data |
| Health | Safety | Medication-related side effects | ||
| Intermediate | LDL-C reduction | |||
| Process | Return of genetic result | |||
| Initiation of cascade screening |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, L.K.; Williams, M.S.; Ladd, I.G.; Cawley, D.; Ge, S.; Hao, J.; Hassen, D.; Hu, Y.; Kirchner, H.L.; Kobylinski, M.; et al. Collaborative Approach to Reach Everyone with Familial Hypercholesterolemia: CARE-FH Protocol. J. Pers. Med. 2022, 12, 606. https://doi.org/10.3390/jpm12040606
Jones LK, Williams MS, Ladd IG, Cawley D, Ge S, Hao J, Hassen D, Hu Y, Kirchner HL, Kobylinski M, et al. Collaborative Approach to Reach Everyone with Familial Hypercholesterolemia: CARE-FH Protocol. Journal of Personalized Medicine. 2022; 12(4):606. https://doi.org/10.3390/jpm12040606
Chicago/Turabian StyleJones, Laney K., Marc S. Williams, Ilene G. Ladd, Dylan Cawley, Shuping Ge, Jing Hao, Dina Hassen, Yirui Hu, H. Lester Kirchner, Maria Kobylinski, and et al. 2022. "Collaborative Approach to Reach Everyone with Familial Hypercholesterolemia: CARE-FH Protocol" Journal of Personalized Medicine 12, no. 4: 606. https://doi.org/10.3390/jpm12040606
APA StyleJones, L. K., Williams, M. S., Ladd, I. G., Cawley, D., Ge, S., Hao, J., Hassen, D., Hu, Y., Kirchner, H. L., Kobylinski, M., Lesko, M. G., Nelson, M. C., Rahm, A. K., Rolston, D. D., Romagnoli, K. M., Schubert, T. J., Shuey, T. C., Sturm, A. C., & Gidding, S. S. (2022). Collaborative Approach to Reach Everyone with Familial Hypercholesterolemia: CARE-FH Protocol. Journal of Personalized Medicine, 12(4), 606. https://doi.org/10.3390/jpm12040606