
Explainable Artificial Intelligence for Prediction of Complete Surgical Cytoreduction in Advanced-Stage Epithelial Ovarian Cancer

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
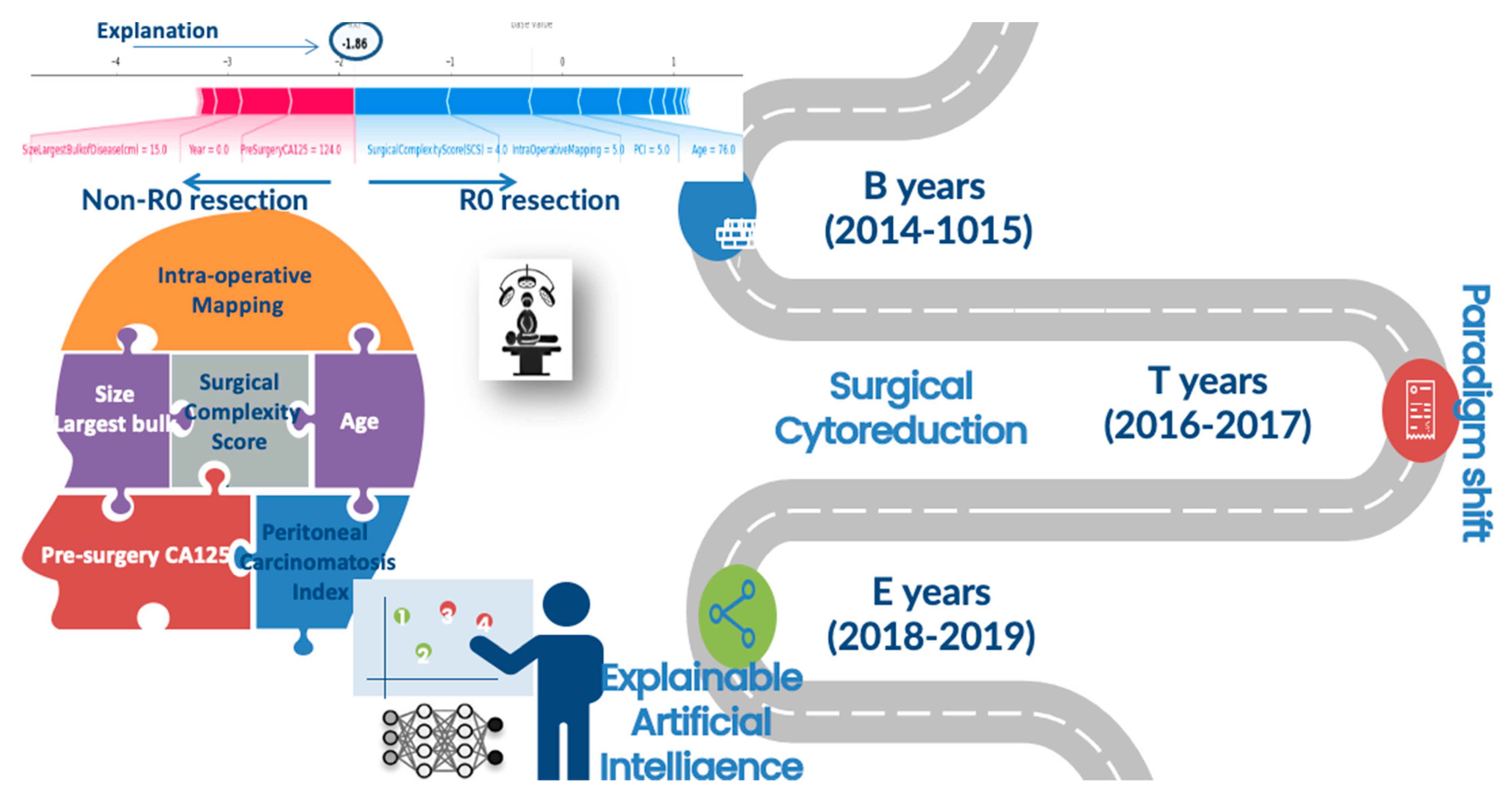
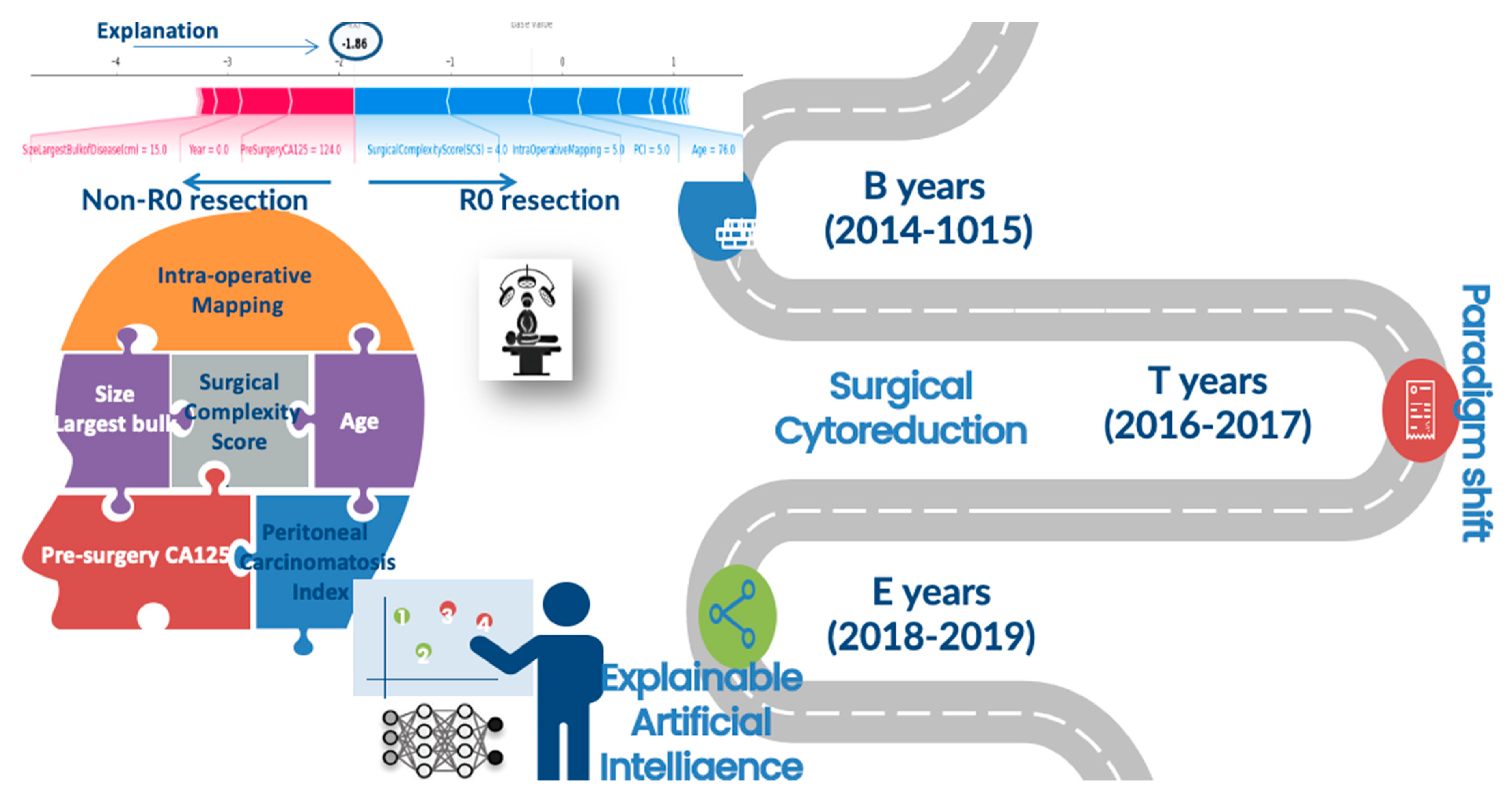
- Patient: age, year of diagnosis, year of surgery, Eastern Co-operative Oncology Group (ECOG) performance status (PS), histology type, grade (low and high), stage (FIGO 3 or 4), and pre-treatment and pre-surgery CA-125.
- Operative/tumour factors: timing of surgery (PDS or IDS), presence of ascites (yes/no), operative time, site of intra-operative bulk of the disease, size of the largest tumour deposit, Peritoneal Carcinomatosis Index (PCI), and intra-operative mapping of ovarian cancer (IMO).
- Age of consultant surgeon, as a parameter of surgical technique heuristics.
3. Results
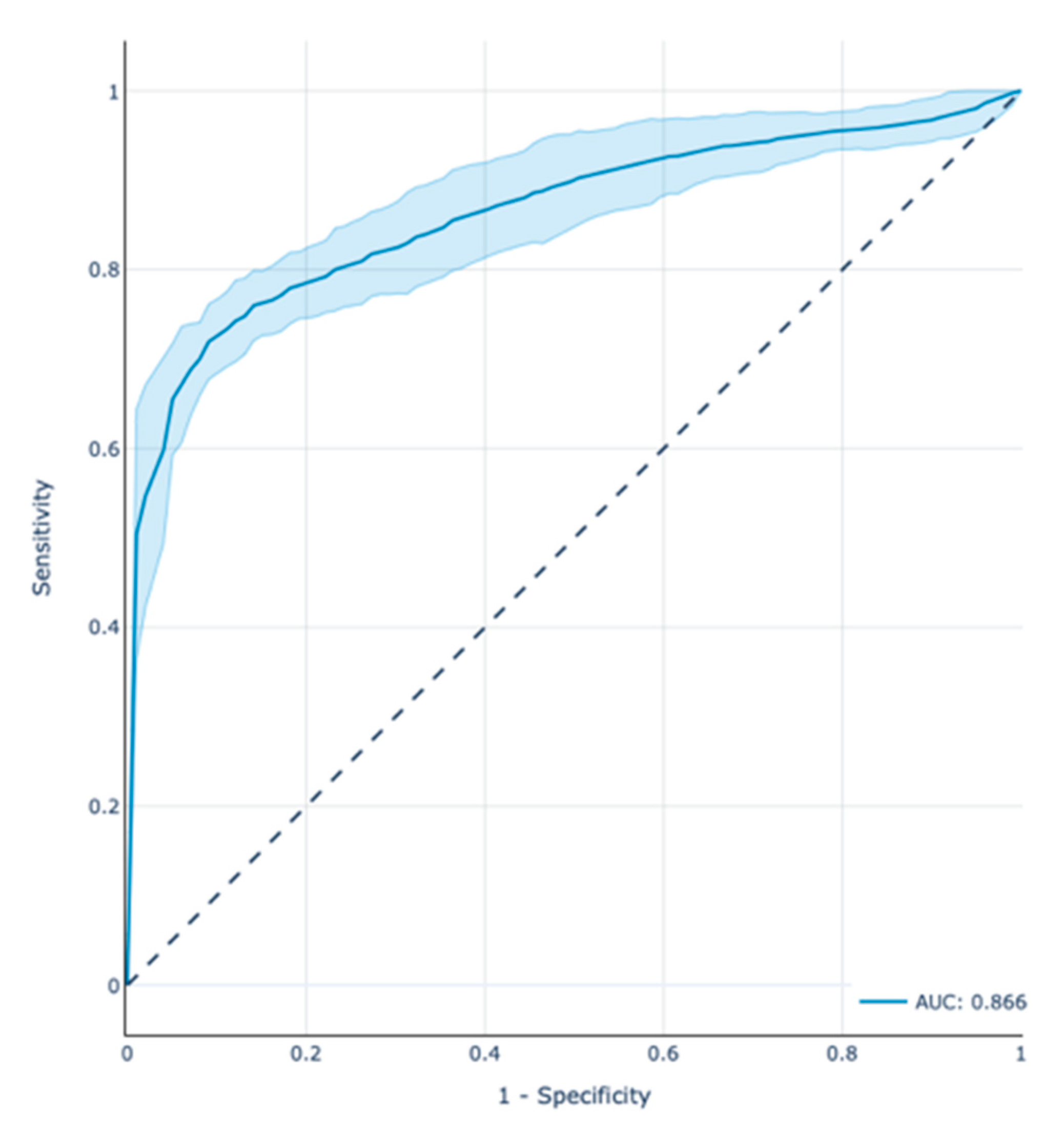
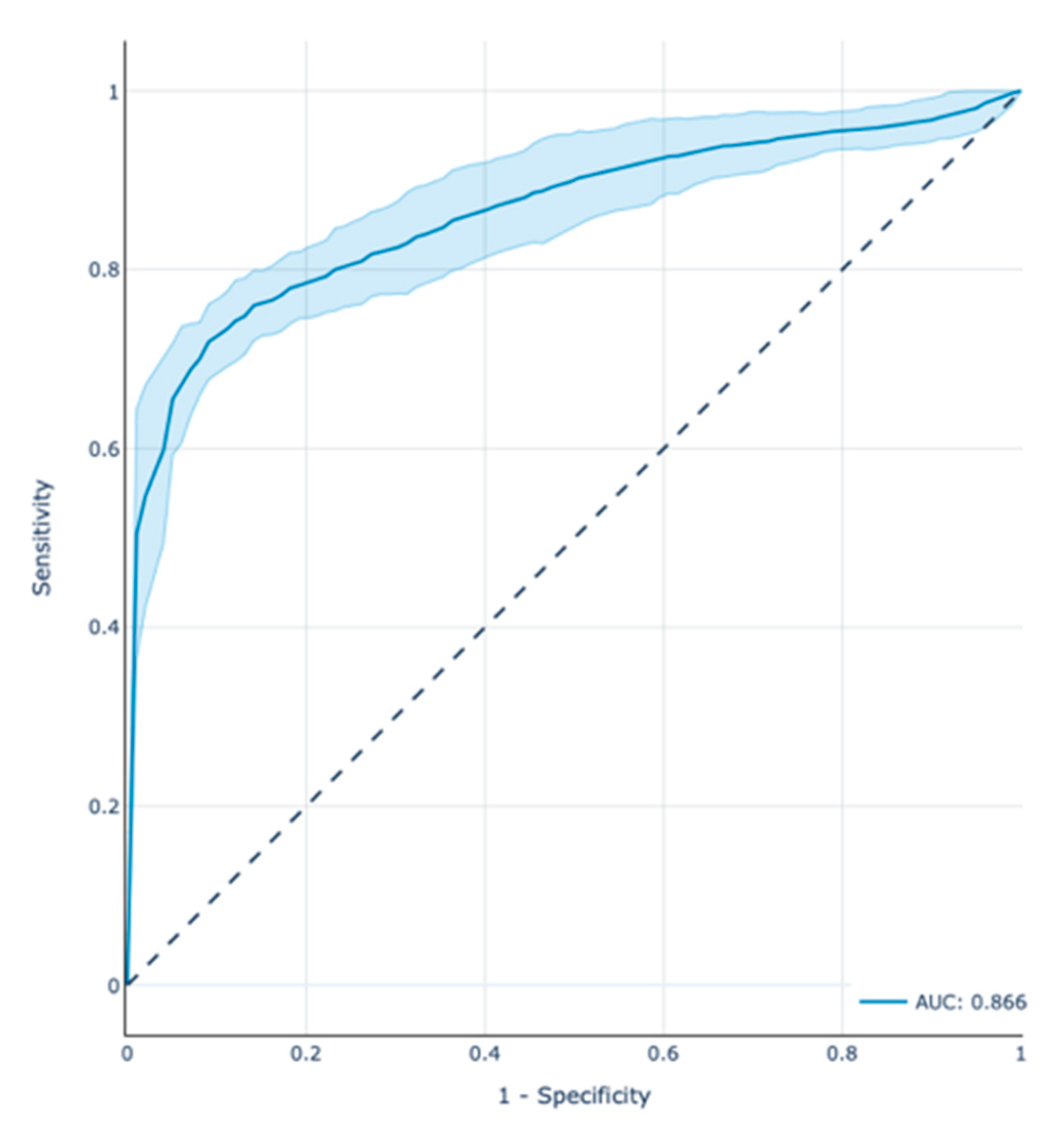
3.1. XGBoost Model Performance
3.2. Feature Analysis
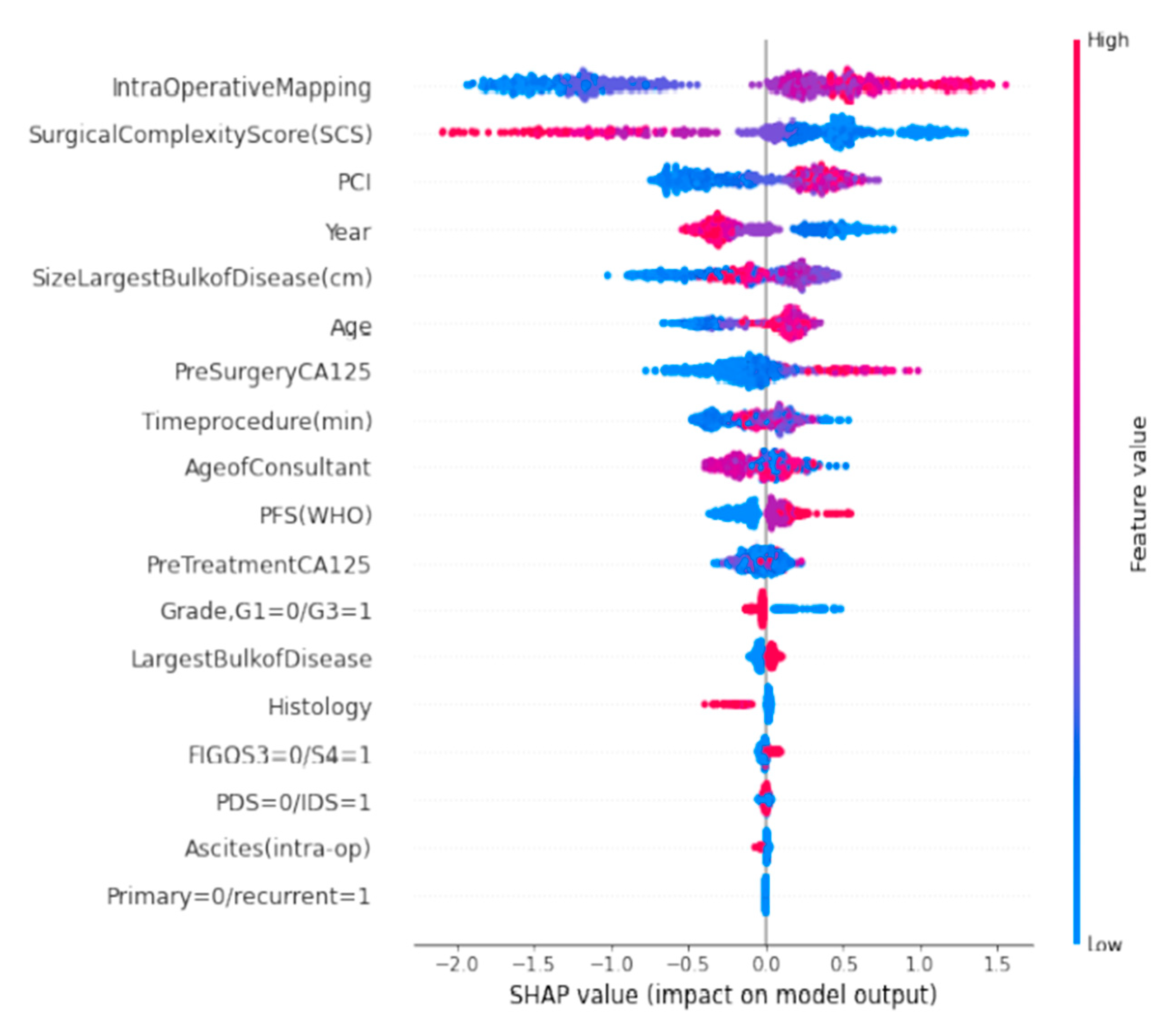
3.3. SHAP Summary Plots
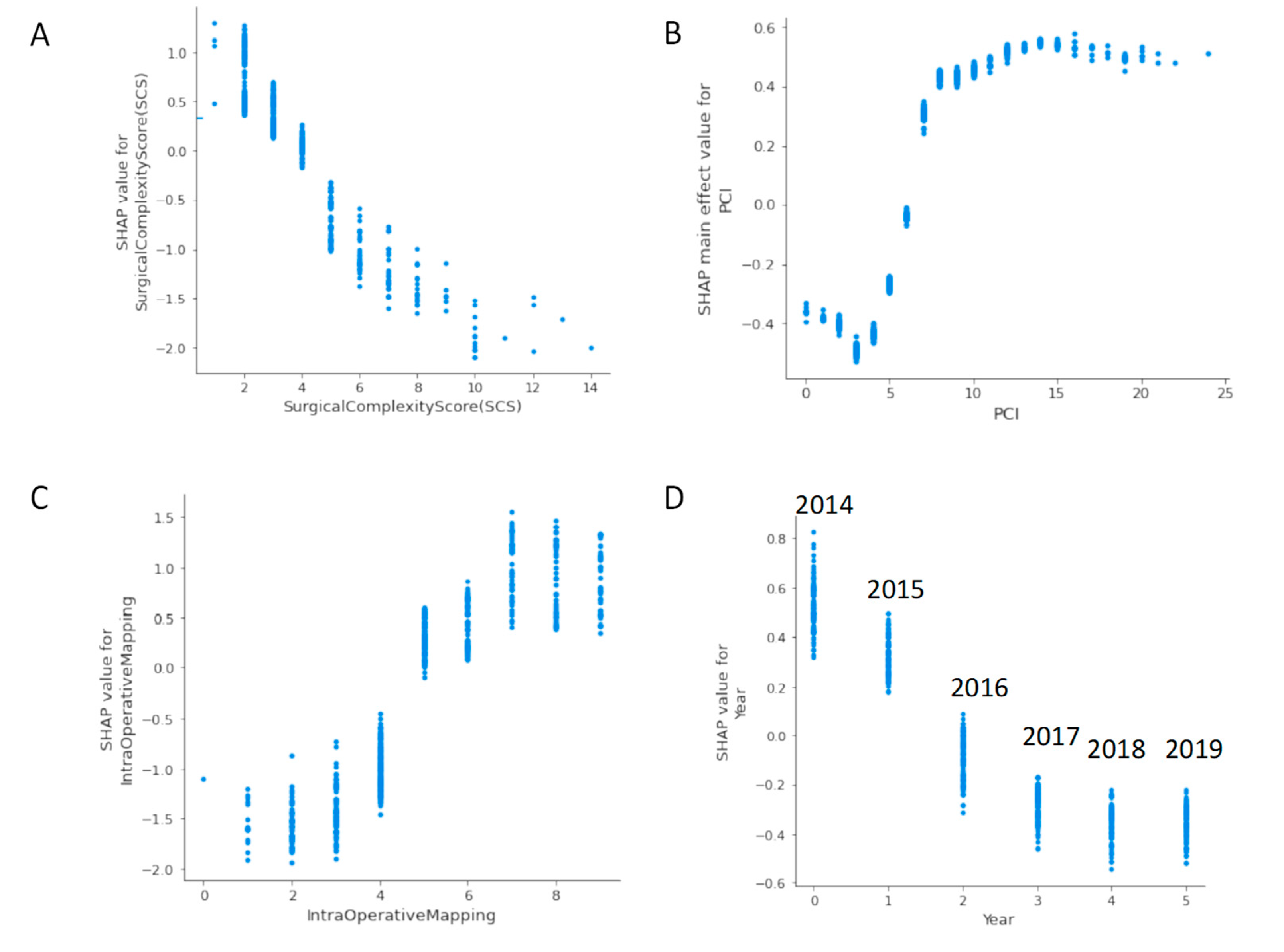
3.4. SHAP Dependence Plots
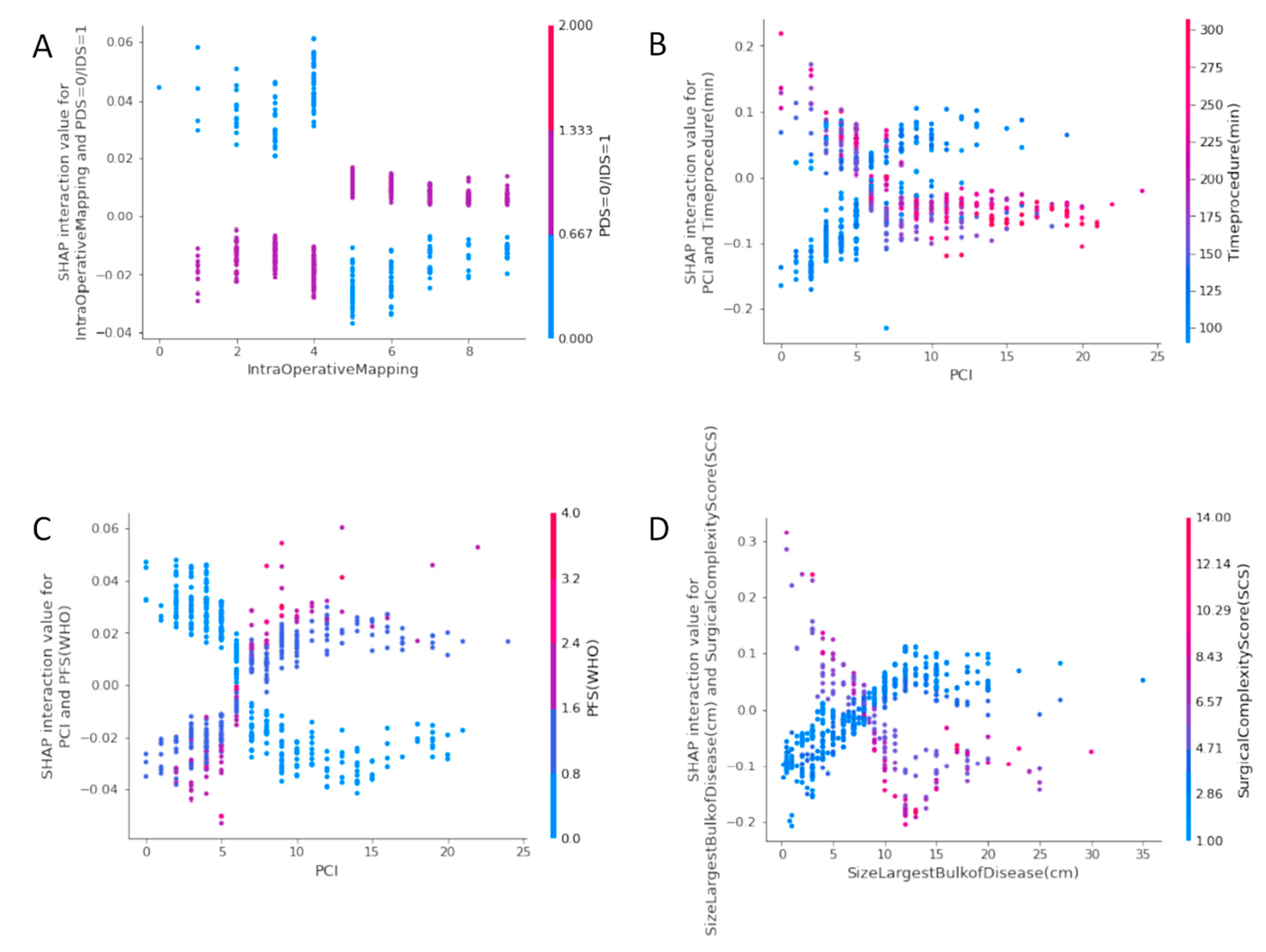
3.5. SHAP Interaction Value Dependence Plots
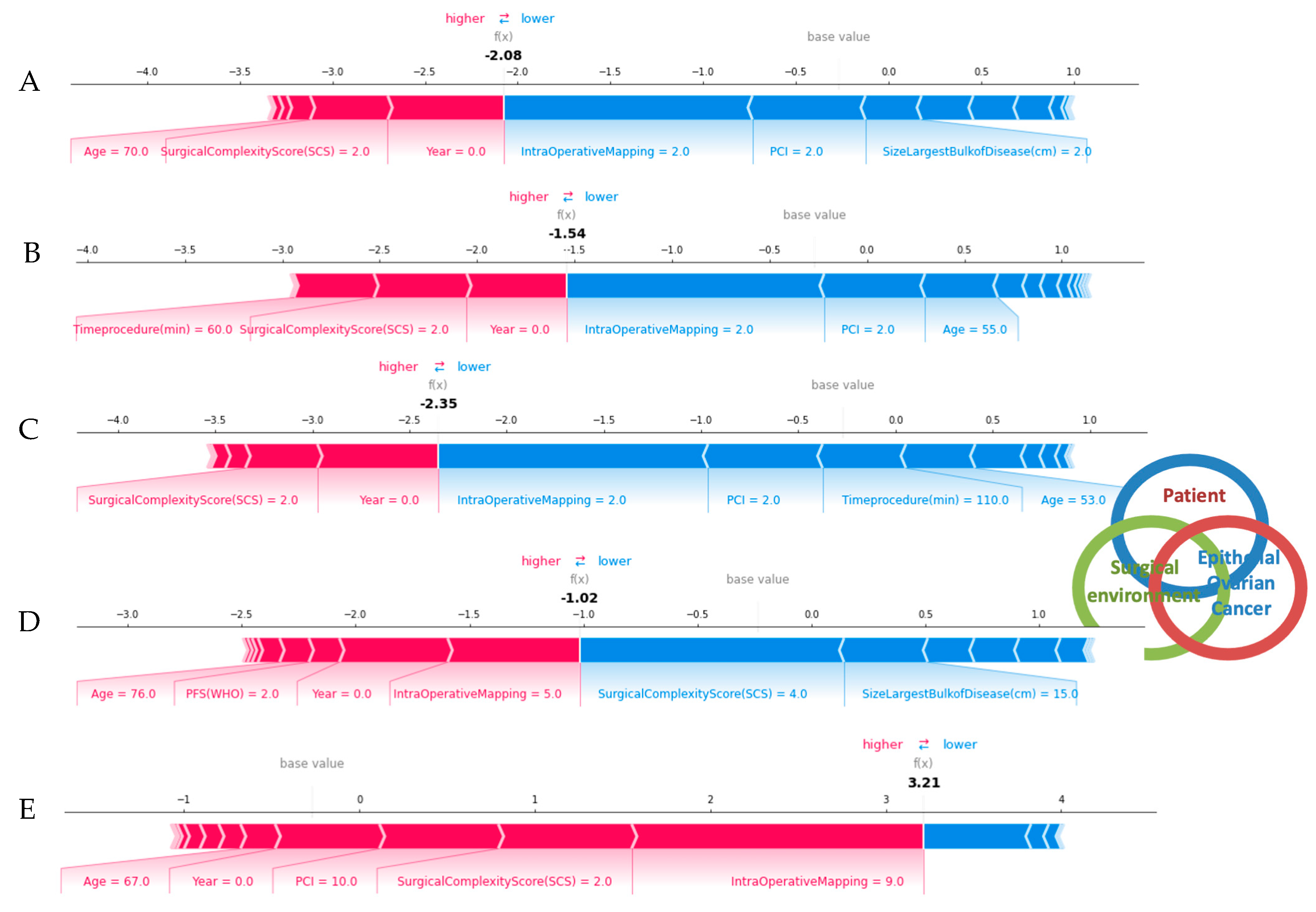
3.6. SHAP Force Plots
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hacker, N.F.; Berek, J.S.; Lagasse, L.D.; Nieberg, R.K.; Elashoff, R.M. Primary cytoreductive surgery for epithelial ovarian cancer. Obstet. Gynecol. 1983, 61, 413–420. [Google Scholar] [PubMed]
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; et al. European Society of Gynaecological Oncology (ESGO) Guidelines for Ovarian Cancer Surgery. Int. J. Gynecol. Cancer 2017, 27, 1534–1542. [Google Scholar] [CrossRef] [PubMed]
- Winter, W.E., 3rd; Maxwell, G.L.; Tian, C.; Carlson, J.W.; Ozols, R.F.; Rose, P.G.; Markman, M.; Armstrong, D.K.; Muggia, F.; McGuire, W.P.; et al. Prognostic factors for stage III epithelial ovarian cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2007, 25, 3621–3627. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.A.; Bohlke, K.; Armstrong, D.K.; Bookman, M.A.; Cliby, W.A.; Coleman, R.L.; Dizon, D.S.; Kash, J.J.; Meyer, L.A.; Moore, K.N.; et al. Neoadjuvant Chemotherapy for Newly Diagnosed, Advanced Ovarian Cancer: Society of Gynecologic Oncology and American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 3460–3473. [Google Scholar] [CrossRef] [PubMed]
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.; Kitchener, H.; Lopes, A.D.B.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- Chi, D.S.; Eisenhauer, E.L.; Lang, J.; Huh, J.; Haddad, L.; Abu-Rustum, N.R.; Sonoda, Y.; Levine, D.A.; Hensley, M.; Barakat, R.R. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol. Oncol. 2006, 103, 559–564. [Google Scholar] [CrossRef]
- Bristow, R.E.; Chi, D.S. Platinum-based neoadjuvant chemotherapy and interval surgical cytoreduction for advanced ovarian cancer: A meta-analysis. Gynecol. Oncol. 2006, 103, 1070–1076. [Google Scholar] [CrossRef]
- Chang, S.-J.; Bristow, R.E.; Ryu, H.-S. Impact of Complete Cytoreduction Leaving No Gross Residual Disease Associated with Radical Cytoreductive Surgical Procedures on Survival in Advanced Ovarian Cancer. Ann. Surg. Oncol. 2012, 19, 4059–4067. [Google Scholar] [CrossRef]
- Aletti, G.; Dowdy, S.C.; Podratz, K.C.; Cliby, W.A. Relationship among surgical complexity, short-term morbidity, and overall survival in primary surgery for advanced ovarian cancer. Am. J. Obstet. Gynecol. 2007, 197, 676.e1–676.e7. [Google Scholar] [CrossRef]
- Zhou, J.; Zeng, Z.Y.; Li, L. Progress of Artificial Intelligence in Gynecological Malignant Tumors. Cancer Manag. Res. 2020, 12, 12823–12840. [Google Scholar] [CrossRef]
- Lu, M.; Fan, Z.; Xu, B.; Chen, L.; Zheng, X.; Li, J.; Znati, T.; Mi, Q.; Jiang, J. Using machine learning to predict ovarian cancer. Int. J. Med. Inform. 2020, 141, 104195. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, E.; Tabata, J.; Yanaihara, N.; Ishikawa, T.; Koseki, K.; Iida, Y.; Saito, M.; Komazaki, H.; Shapiro, J.S.; Goto, C.; et al. Application of Artificial Intelligence for Preoperative Diagnostic and Prognostic Prediction in Epithelial Ovarian Cancer Based on Blood Biomarkers. Clin. Cancer Res. 2019, 25, 3006–3015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laios, A.; Gryparis, A.; DeJong, D.; Hutson, R.; Theophilou, G.; Leach, C. Predicting complete cytoreduction for advanced ovarian cancer patients using nearest-neighbor models. J. Ovarian Res. 2020, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Laios, A.; Katsenou, A.; Tan, Y.S.; Johnson, R.; Otify, M.; Kaufmann, A.; Munot, S.; Thangavelu, A.; Hutson, R.; Broadhead, T.; et al. Feature Selection is Critical for 2-Year Prognosis in Advanced Stage High Grade Serous Ovarian Cancer by Using Machine Learning. Cancer Control 2021, 28, 10732748211044678. [Google Scholar] [CrossRef] [PubMed]
- Lamy, J.-B.; Sekar, B.; Guezennec, G.; Bouaud, J.; Séroussi, B. Explainable artificial intelligence for breast cancer: A visual case-based reasoning approach. Artif. Intell. Med. 2019, 94, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, A.B.; Díaz-Rodríguez, N.; Del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; Herrera, F. Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and challenges toward responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, S.M.; Nair, B.; Vavilala, M.S.; Horibe, M.; Eisses, M.J.; Adams, T.; Liston, D.E.; Low, D.K.-W.; Newman, S.-F.; Kim, J.; et al. Explainable machine learning predictions to help anesthesiologists prevent hypoxemia during surgery. Nat. Biomed. Eng. 2018, 2, 749–760. [Google Scholar] [CrossRef]
- Azaïs, H.; Vignion-Dewalle, A.-S.; Carrier, M.; Augustin, J.; Da Maïa, E.; Penel, A.; Belghiti, J.; Nikpayam, M.; Gonthier, C.; Ziane, L.; et al. Microscopic Peritoneal Residual Disease after Complete Macroscopic Cytoreductive Surgery for Advanced High Grade Serous Ovarian Cancer. J. Clin. Med. 2020, 10, 41. [Google Scholar] [CrossRef]
- Newsham, A.C.; Johnston, C.; Hall, G.; Leahy, M.G.; Smith, A.B.; Vikram, A.; Donnelly, A.M.; Velikova, G.; Selby, P.J.; Fisher, S.E. Development of an advanced database for clinical trials integrated with an electronic patient record system. Comput. Biol. Med. 2011, 41, 575–586. [Google Scholar] [CrossRef]
- Mutch, D.G.; Prat, J. 2014 FIGO staging for ovarian, fallopian tube and peritoneal cancer. Gynecol. Oncol. 2014, 133, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Fotopoulou, C.; Hall, M.; Cruickshank, D.; Gabra, H.; Ganesan, R.; Hughes, C.; Kehoe, S.; Ledermann, J.; Morrison, J.; Naik, R.; et al. British Gynaecological Cancer Society (BGCS) epithelial ovarian/fallopian tube/primary peritoneal cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Nelson, G.; Bakkum-Gamez, J.; Kalogera, E.; Glaser, G.; Altman, A.; Meyer, L.A.; Taylor, J.S.; Iniesta, M.; LaSala, J.; Mena, G.; et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations—2019 update. Int. J. Gynecol. Cancer 2019, 29, 651–668. [Google Scholar] [CrossRef]
- Laios, A.; Silva, R.V.D.O.; De Freitas, D.L.D.; Tan, Y.S.; Saalmink, G.; Zubayraeva, A.; Johnson, R.; Kaufmann, A.; Otify, M.; Hutson, R.; et al. Machine Learning-Based Risk Prediction of Critical Care Unit Admission for Advanced Stage High Grade Serous Ovarian Cancer Patients Undergoing Cytoreductive Surgery: The Leeds-Natal Score. J. Clin. Med. 2021, 11, 87. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. In Peritoneal Carcinomatosis: Principles of Management; Sugarbaker, P.H., Ed.; Springer: Boston, MA, USA, 1996; pp. 359–374. [Google Scholar]
- Sehouli, J.; Könsgen, D.; Mustea, A.; Oskay-Ozcelik, G.; Katsares, I.; Weidemann, H.; Lichtenegger, W. ”IMO"—Intraoperatives Mapping des Ovarialkarzinoms [“IMO”—Intraoperative mapping of ovarian cancer]. Zentralblatt fur Gynakologie 2003, 125, 129–135. [Google Scholar] [PubMed]
- Friedman, J.H. Greedy function approximation: A gradient boosting machine. Ann. Stat. 2001, 29, 1189–1232. [Google Scholar] [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable AI: A Review of Machine Learning Interpretability Methods. Entropy 2020, 23, 18. [Google Scholar] [CrossRef]
- Parsa, A.B.; Movahedi, A.; Taghipour, H.; Derrible, S.; Mohammadian, A. (Kouros) Toward safer highways, application of XGBoost and SHAP for real-time accident detection and feature analysis. Accid. Anal. Prev. 2020, 136, 105405. [Google Scholar] [CrossRef]
- Ramon, Y.; Martens, D.; Provost, F.; Evgeniou, T. A comparison of instance-level counterfactual explanation algorithms for behavioral and textual data: SEDC, LIME-C and SHAP-C. Adv. Data Anal. Classif. 2020, 14, 801–819. [Google Scholar] [CrossRef]
- Slack, D.; Hilgard, S.; Jia, E.; Singh, S.; Lakkaraju, H. Fooling lime and shap: Adversarial attacks on post hoc explanation methods. In Proceedings of the AAAI/ACM Conference on AI, Ethics, and Society, New York, NY, USA, 7–8 February 2020; pp. 180–186. [Google Scholar]
- Hall, M.; Savvatis, K.; Nixon, K.; Kyrgiou, M.; Hariharan, K.; Padwick, M.; Owens, O.; Cunnea, P.; Campbell, J.; Farthing, A.; et al. Maximal-Effort Cytoreductive Surgery for Ovarian Cancer Patients with a High Tumor Burden: Variations in Practice and Impact on Outcome. Ann. Surg. Oncol. 2019, 26, 2943–2951. [Google Scholar] [CrossRef] [Green Version]
- Jónsdóttir, B.; Lomnytska, M.; Poromaa, I.S.; Silins, I.; Stålberg, K. The Peritoneal Cancer Index is a Strong Predictor of Incomplete Cytoreductive Surgery in Ovarian Cancer. Ann. Surg. Oncol. 2020, 28, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Cliby, W.A. Advanced Ovarian Cancer: Weighing the Risks and Benefits of Surgery. Clin. Obstet. Gynecol. 2020, 63, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Eisenkop, S.M.; Friedman, R.L.; Wang, H.-J. Complete Cytoreductive Surgery Is Feasible and Maximizes Survival in Patients with Advanced Epithelial Ovarian Cancer: A Prospective Study. Gynecol. Oncol. 1998, 69, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Hlatky, M.A.; Cotugno, H.; O’Connor, C.; Mark, D.B.; Pryor, D.B.; Califf, R.M. Adoption of thrombolytic therapy in the management of acute myocardial infarction. Am. J. Cardiol. 1988, 61, 510–514. [Google Scholar] [CrossRef]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017, 2017, CD001431. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.L.; Laios, A.; Jackson, D.; Nugent, D.; Orsi, N.M.; Theophilou, G.; Thangavelu, A.; de Jong, D. The Uncertain Benefit of Adjuvant Chemotherapy in Advanced Low-Grade Serous Ovarian Cancer and the Pivotal Role of Surgical Cytoreduction. J. Clin. Med. 2021, 10, 5927. [Google Scholar] [CrossRef]
- Chi, D.S.; Eisenhauer, E.L.; Zivanovic, O.; Sonoda, Y.; Abu-Rustum, N.R.; Levine, D.A.; Guile, M.W.; Bristow, R.E.; Aghajanian, C.; Barakat, R.R. Improved progression-free and overall survival in advanced ovarian cancer as a result of a change in surgical paradigm. Gynecol. Oncol. 2009, 114, 26–31. [Google Scholar] [CrossRef]
- Fotopoulou, C.; Concin, N.; Planchamp, F.; Morice, P.; Vergote, I.; Du Bois, A.; Querleu, D. Quality indicators for advanced ovarian cancer surgery from the European Society of Gynaecological Oncology (ESGO): 2020 update. Int. J. Gynecol. Cancer 2020, 30, 436–440. [Google Scholar] [CrossRef]
- Bristow, R.E.; Palis, B.E.; Chi, D.S.; Cliby, W.A. The National Cancer Database report on advanced-stage epithelial ovarian cancer: Impact of hospital surgical case volume on overall survival and surgical treatment paradigm. Gynecol. Oncol. 2010, 118, 262–267. [Google Scholar] [CrossRef]
- Fagotti, A.; Ferrandina, M.G.; Vizzielli, G.; Pasciuto, T.; Fanfani, F.; Gallotta, V.; Margariti, P.A.; Chiantera, V.; Costantini, B.; Alletti, S.G.; et al. Randomized trial of primary debulking surgery versus neoadjuvant chemotherapy for advanced epithelial ovarian cancer (SCORPION-NCT01461850). Int. J. Gynecol. Cancer 2020, 30, 1657–1664. [Google Scholar] [CrossRef]
- Suidan, R.S.; Ramirez, P.T.; Sarasohn, D.; Teitcher, J.B.; Mironov, S.; Iyer, R.B.; Zhou, Q.; Iasonos, A.; Paul, H.; Hosaka, M.; et al. A multicenter prospective trial evaluating the ability of preoperative computed tomography scan and serum CA-125 to predict suboptimal cytoreduction at primary debulking surgery for advanced ovarian, fallopian tube, and peritoneal cancer. Gynecol. Oncol. 2014, 134, 455–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llueca, A.; Serra, A.; Delgado, K.; Maiocchi, K.; Jativa, R.; Gomez, L.; Escrig, J. A radiologic-laparoscopic model to predict suboptimal (or complete and optimal) debulking surgery in advanced ovarian cancer: A pilot study. Int. J. Womens Health 2019, 11, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenkop, S.M.; Spirtos, N.M.; Friedman, R.L.; Lin, W.C.; Pisani, A.L.; Perticucci, S. Relative influences of tumor volume before surgery and the cytoreductive outcome on survival for patients with advanced ovarian cancer: A prospective study. Gynecol. Oncol. 2003, 90, 390–396. [Google Scholar] [CrossRef]
- Wise, J. Survey of UK doctors highlights blame culture within the NHS. BMJ 2018, 362, k4001. [Google Scholar] [CrossRef] [PubMed]
- Barton, D.P.J.; Adib, T.; Butler, J. Surgical practice of UK gynaecological oncologists in the treatment of primary advanced epithelial ovarian cancer (PAEOC): A questionnaire survey. Gynecol. Oncol. 2013, 131, 347–351. [Google Scholar] [CrossRef]
- Kausch, S.L.; Sullivan, B.; Spaeder, M.C.; Keim-Malpass, J. Individual illness dynamics: An analysis of children with sepsis admitted to the pediatric intensive care unit. PLoS Digit. Health 2022, 1, e0000019. [Google Scholar] [CrossRef]
- Batista, G.E.A.P.A.; Prati, R.C.; Monard, M.C. A study of the behavior of several methods for balancing machine learning training data. ACM SIGKDD Explor. Newsl. 2004, 6, 20–29. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Overall (n = 571) | Train Set (n = 399) | Test Set (n = 172) | p Value | Non R0 (n = 196) | R0 (n = 375) | p Value |
|---|---|---|---|---|---|---|---|
| Age (y) | 63.5 ± 11.2 | 63.6 ± 11 | 63.2 ± 11.7 | 0.71 | 65.6 ± 10.1 | 62.4 ± 11.6 | <0.001 |
| Histology | 0.217 | 0.008 | |||||
| Serous | 504 (0.88) | 350 (0.88) | 153 (0.89) | 186 (0.94) | 318 (0.85) | ||
| Mucinous | 13 (0.02) | 7 (0.017) | 6 (0.035) | 1 (0.005) | 12 (0.03) | ||
| Clear cell/endometrioid | 33 (0.06) | 23 (0.057) | 10 (0.058) | 6 (0.03) | 27 (0.07) | ||
| Miscellaneous | 22 (0.04) | 19 (0.047) | 3 (0.017) | 4 (0.02) | 18 (0.05) | ||
| Primary = 0/recurrent = 1 | 0.37 | ||||||
| Primary | 561 (0.98) | 370 (0.66) | 191 (0.32) | 0.7 | 192 (0.98) | 369 (0.98) | |
| Recurrent | 10 (0.02) | 7 (0.02) | 3 (0.02) | ||||
| Grade (G1 = 0/G3 = 1) | 516 (0.9) | 354 (0.89) | 162 (0.94) | 174 (0.89) | 342 (0.91) | 0.43 | |
| FIGO stage (S3 = 0/S4 = 1) | 157 (0.27) | 106 (0.27) | 51 (0.3) | 59 (0.3) | 98 (0.26) | 0.36 | |
| Performance status (WHO) | 0.74 | 0.001 | |||||
| 0 | 273 (0.48) | 192 (0.48) | 80 (0.46) | 70 (0.35) | 203 (0.54) | ||
| 1 | 212 (0.37) | 144 (0.36) | 68 (0.39) | 90 (0.46) | 122 (0.32) | ||
| 2 | 68 (0.12) | 50 (0.125) | 18 (0.1) | 28 (0.14) | 40 (0.1) | ||
| 3 | 19 (0.03) | 13 (0.276) | 6 (0.35) | 9 (0.04) | 10 (0.02) | ||
| Age of consultant (y) | 49.2 ± 6 | 49.3 ± 6 | 48.9 ± 6 | 0.46 | 49.2 ± 6.3 | 49.2 ± 5.9 | 0.99 |
| Timing of surgery | 0.6 | 0.38 | |||||
| Interval debulking surgery | 396 (0.69) | 278 (0.7) | 118 (0.69) | 141 (0.72) | 255 (0.68) | ||
| Primary debulking surgery | 175 (0.31) | 113 (0.64) | 62 (0.36) | 122 (0.7) | 53 (0.3) | ||
| Year | 0.7 | 0.012 | |||||
| 2014 | 91 (0.158) | 63 (0.158) | 27 (0.156) | 44 (0.22) | 47 (0.12) | ||
| 2015 | 93 (0.162) | 65 (0.163) | 28 (0.16) | 36 (0.18) | 57 (0.15) | ||
| 2016 | 108 (0.19) | 74 (0.185) | 34 (0.198) | 38 (0.19) | 70 (0.19) | ||
| 2017 | 96 (0.17) | 64 (0.16) | 32 (0.186) | 31 (0.16) | 65 (0.17) | ||
| 2018 | 82 (0.14) | 55 (0.138) | 27 (0.157) | 23 (0.12) | 59 (0.16) | ||
| 2019 | 102 (0.18) | 78 (0.195) | 24 (0.14) | 25 (0.13) | 77 (0.21) | ||
| Pre-treatment CA125 | 1572.7 ± 2993.2 | 1542.9 ± 3070.7 | 1641.8 ± 2812.9 | 0.7 | 1790.9 ± 3207 | 1458.7 ± 2873.1 | 0.22 |
| Pre-surgery CA125 | 411.79 ± 1170 | 387.3 ± 943.7 | 468.6 ± 1576.7 | 0.52 | 451 ± 931.7 | 391.3 ± 1277.7 | 0.52 |
| Size of largest disease bulk (cm) | 8.9 ± 5.58 | 9.0 ± 5.79 | 8.63 ± 5.09 | 0.43 | 9.79 ± 5.24 | 8.41 ± 5.7 | 0.004 |
| Peritoneal Carcinomatosis Index (PCI) | 7.39 ± 4.53 | 7.39 ± 4.52 | 7.4 ± 4.56 | 0.99 | 8.91 ± 4.31 | 6.6 ± 4.44 | <0.001 |
| Surgical Complexity Score (SCS) | 3.8 ± 2.12 | 3.79 ± 2.14 | 3.82 ± 2.09 | 0.89 | 3.1 ± 1.44 | 4.17 ± 2.32 | <0.001 |
| Time procedure (min) | 170.36 ± 77.48 | 170.1 ± 79.48 | 170.96 ± 72.85 | 0.9 | 161.84 ± 63.81 | 174.81 ± 83.47 | 0.039 |
| Site of largest tumour deposit | 0.28 | <0.001 | |||||
| Ovary | 298 (0.52) | 216 (0.54) | 82 (0.477) | 83 (0.42) | 215 (0.57) | ||
| Omentum | 258 (0.45) | 171 (0.43) | 86 (0.5) | 110 (0.56) | 148 (0.39) | ||
| Miscellaneous | 16 (0.03) | 12 (0.03) | 4 (0.023) | 4 (0.02) | 12 (0.03) | ||
| Intra Operative Mapping Score | 4.92 ± 1.99 | 4.95 ± 1.99 | 4.85 ± 2.01 | 0.58 | 5.96 ± 1.69 | 4.38 ± 1.93 | <0.001 |
| Ascites (intra-op) | 131 (0.23) | 93 (0.23) | 38 (0.22) | 49 (0.25) | 82 (0.22) | 0.458 |
| Precision | Recall | f1-Score | |
|---|---|---|---|
| CC0 | 0.91 | 0.87 | 0.89 |
| Non-CC0 | 0.71 | 0.78 | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laios, A.; Kalampokis, E.; Johnson, R.; Thangavelu, A.; Tarabanis, C.; Nugent, D.; De Jong, D. Explainable Artificial Intelligence for Prediction of Complete Surgical Cytoreduction in Advanced-Stage Epithelial Ovarian Cancer. J. Pers. Med. 2022, 12, 607. https://doi.org/10.3390/jpm12040607
Laios A, Kalampokis E, Johnson R, Thangavelu A, Tarabanis C, Nugent D, De Jong D. Explainable Artificial Intelligence for Prediction of Complete Surgical Cytoreduction in Advanced-Stage Epithelial Ovarian Cancer. Journal of Personalized Medicine. 2022; 12(4):607. https://doi.org/10.3390/jpm12040607
Chicago/Turabian StyleLaios, Alexandros, Evangelos Kalampokis, Racheal Johnson, Amudha Thangavelu, Constantine Tarabanis, David Nugent, and Diederick De Jong. 2022. "Explainable Artificial Intelligence for Prediction of Complete Surgical Cytoreduction in Advanced-Stage Epithelial Ovarian Cancer" Journal of Personalized Medicine 12, no. 4: 607. https://doi.org/10.3390/jpm12040607
APA StyleLaios, A., Kalampokis, E., Johnson, R., Thangavelu, A., Tarabanis, C., Nugent, D., & De Jong, D. (2022). Explainable Artificial Intelligence for Prediction of Complete Surgical Cytoreduction in Advanced-Stage Epithelial Ovarian Cancer. Journal of Personalized Medicine, 12(4), 607. https://doi.org/10.3390/jpm12040607