
Impact of the Genotype and Phenotype of CYP3A and P-gp on the Apixaban and Rivaroxaban Exposure in a Real-World Setting

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Genotyping of CYP3A4/5 and P-Glycoprotein Encoding Genes
2.4. Phenotyping
2.5. Laboratory Markers Levels
2.6. Apixaban and Rivaroxaban Blood Concentrations
2.7. Statistical Analysis
3. Results
3.1. Demographics
3.2. Genotypes
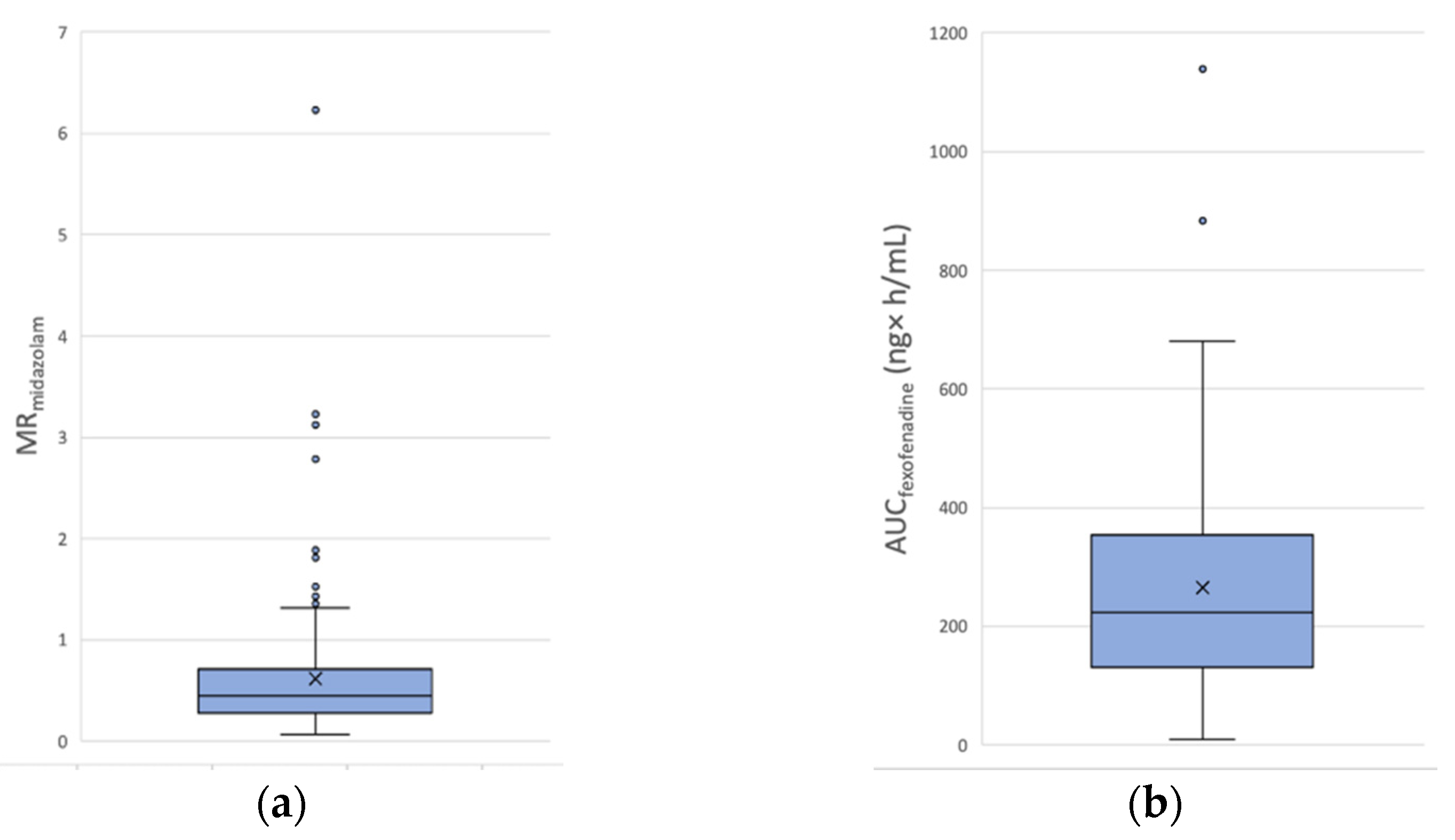
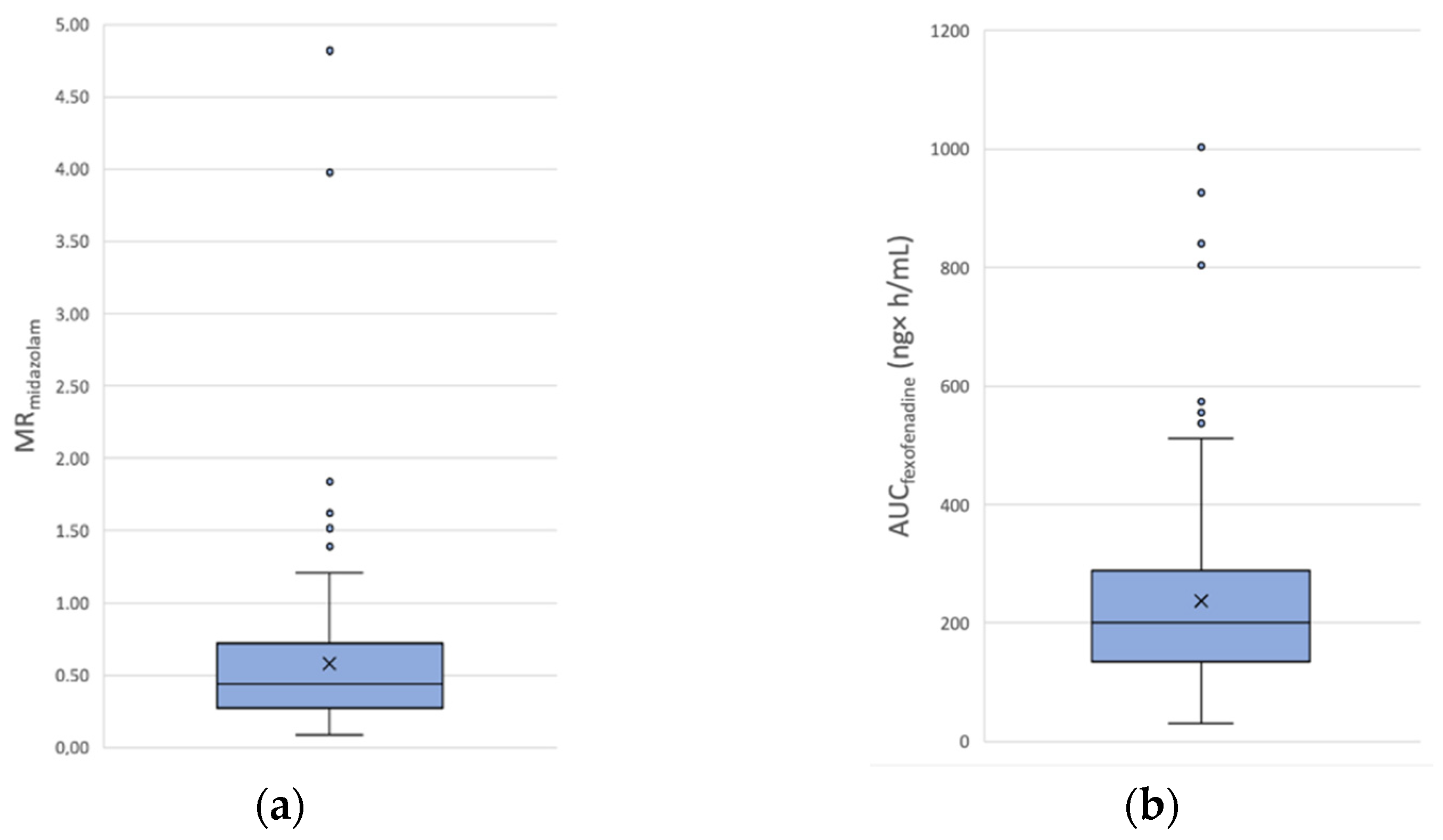
3.3. Phenotypes
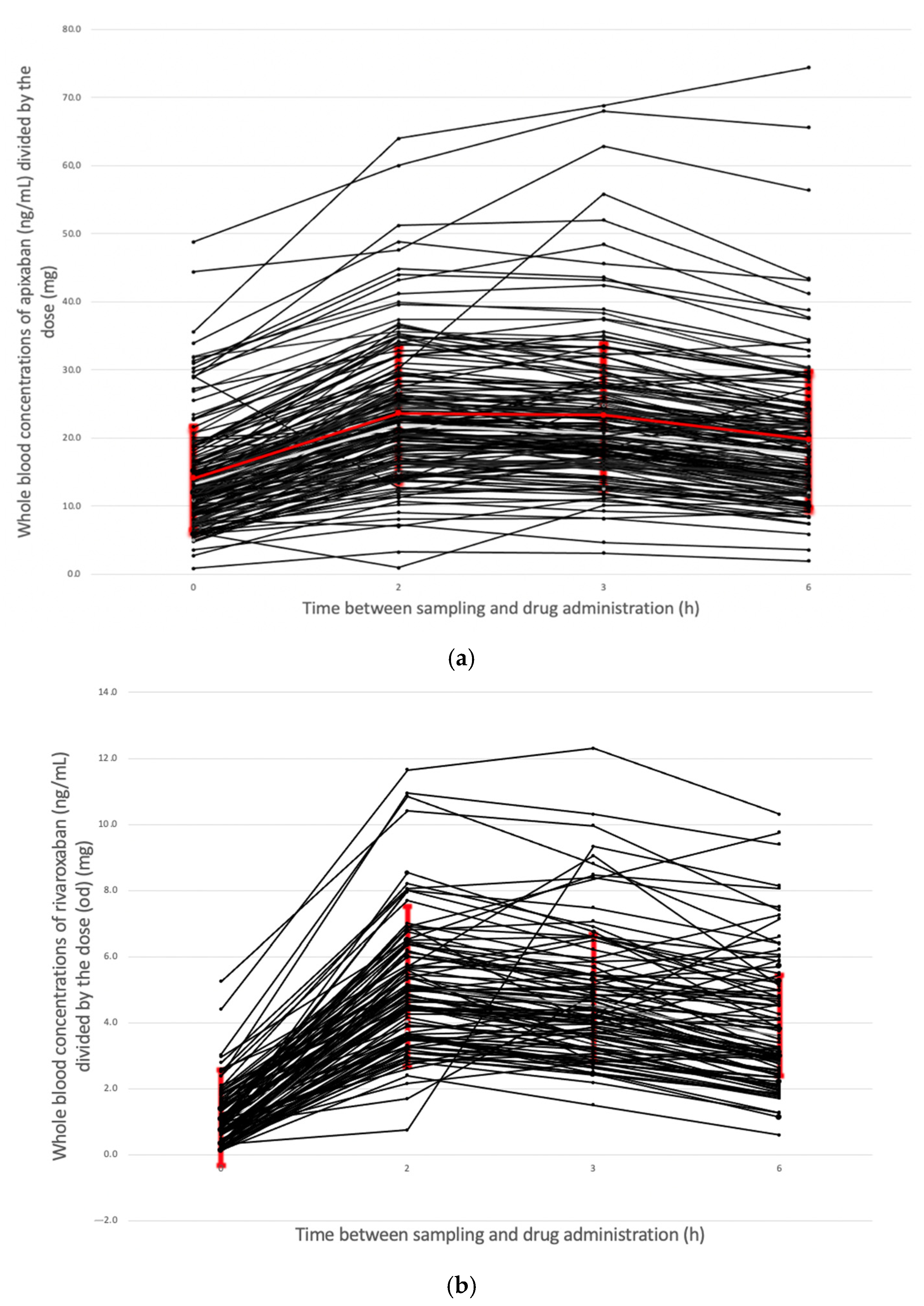
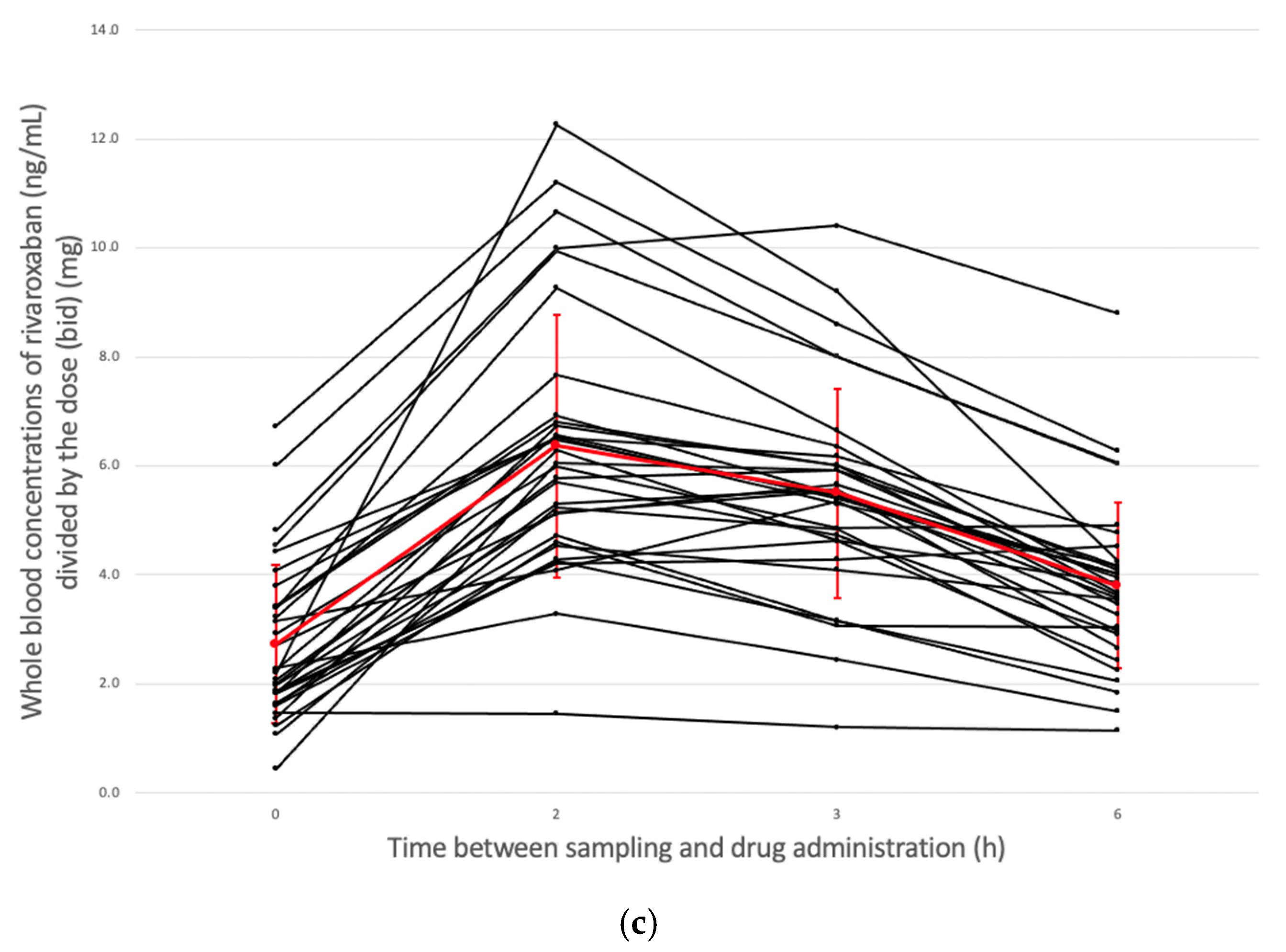
3.4. Apixaban and Rivaroxaban Blood Concentrations
3.5. Multivariable Linear Regression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, N.R.; Sandler, B.; Bergrath, E.; Milenković, D.; Ashaye, A.O.; Farooqui, U.; Cohen, A.T. A Systematic Review of Network Meta-Analyses and Real-World Evidence Comparing Apixaban and Rivaroxaban in Nonvalvular Atrial Fibrillation. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029619898764. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Stecker, E.; Warden, B.A. Direct Oral Anticoagulant Use: A Practical Guide to Common Clinical Challenges. J. Am. Heart Assoc. 2020, 9, e017559. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, R.; Sharma, T.; Garg, J.; Sukhi, A.; Bliden, K.; Tantry, U.; Turagam, M.; Lakkireddy, D.; Gurbel, P. Direct Oral Anticoagulants: A Review on the Current Role and Scope of Reversal Agents. J. Thromb. Thrombolysis 2020, 49, 271–286. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Chan, N.; Sobieraj-Teague, M.; Eikelboom, J.W. Direct Oral Anticoagulants: Evidence and Unresolved Issues. Lancet 2020, 396, 1767–1776. [Google Scholar] [CrossRef]
- Terrier, J.; Gaspar, F.; Fontana, P.; Youssef, D.; Reny, J.-L.; Csajka, C.; Samer, C.F. Drug-Drug Interactions with Direct Oral Anticoagulants: Practical Recommendations for Clinicians. Am. J. Med. 2021, 134, 939–942. [Google Scholar] [CrossRef]
- Food and Drug Administration (FDA). ELIQUIS (Apixaban) Label-Summary of Product Characteristics. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/202155s000lbl.pdf (accessed on 10 January 2022).
- Food and Drug Administration (FDA). XARELTO (Rivaroxaban)-Summary of Product Characteristics. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022406s015lbl.pdf (accessed on 10 January 2022).
- Grymonprez, M.; Steurbaut, S.; De Backer, T.L.; Petrovic, M.; Lahousse, L. Effectiveness and Safety of Oral Anticoagulants in Older Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2020, 11, 583311. [Google Scholar] [CrossRef]
- Foerster, K.I.; Hermann, S.; Mikus, G.; Haefeli, W.E. Drug-Drug Interactions with Direct Oral Anticoagulants. Clin. Pharm. 2020, 59, 967–980. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; Zhou, Z.; Zhou, J.; Chen, S.-Q. Pharmacogenomics of Drug Metabolizing Enzymes and Transporters: Relevance to Precision Medicine. Genom. Proteom. Bioinform. 2016, 14, 298–313. [Google Scholar] [CrossRef] [Green Version]
- Moner-Banet, T.; Alberio, L.; Bart, P.-A. Does One Dose Really Fit All? On the Monitoring of Direct Oral Anticoagulants: A Review of the Literature. Hamostaseologie 2020, 40, 184–200. [Google Scholar] [CrossRef] [PubMed]
- Sanborn, D.; Sugrue, A.; Amin, M.; Mehta, R.; Farwati, M.; Deshmukh, A.J.; Sridhar, H.; Ahmed, A.; Asirvatham, S.J.; Ou, N.N.; et al. Outcomes of Direct Oral Anticoagulants Co-Prescribed with Common Interacting Medications. Am. J. Cardiol. 2022, 162, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Piccini, J.P.; Hellkamp, A.S.; Washam, J.B.; Becker, R.C.; Breithardt, G.; Berkowitz, S.D.; Halperin, J.L.; Hankey, G.J.; Hacke, W.; Mahaffey, K.W.; et al. Polypharmacy and the Efficacy and Safety of Rivaroxaban Versus Warfarin in the Prevention of Stroke in Patients With Nonvalvular Atrial Fibrillation. Circulation 2016, 133, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-H.; Chou, I.-J.; Yeh, Y.-H.; Chiou, M.-J.; Wen, M.-S.; Kuo, C.-T.; See, L.-C.; Kuo, C.-F. Association Between Use of Non-Vitamin K Oral Anticoagulants With and Without Concurrent Medications and Risk of Major Bleeding in Nonvalvular Atrial Fibrillation. JAMA 2017, 318, 1250–1259. [Google Scholar] [CrossRef]
- Lee, J.Y.; Oh, I.-Y.; Lee, J.-H.; Kim, S.-Y.; Kwon, S.S.; Yang, H.-J.; Kim, Y.-K.; Bang, S.-M. The Increased Risk of Bleeding Due to Drug-Drug Interactions in Patients Administered Direct Oral Anticoagulants. Thromb. Res. 2020, 195, 243–249. [Google Scholar] [CrossRef]
- Hanigan, S.; Das, J.; Pogue, K.; Barnes, G.D.; Dorsch, M.P. The Real World Use of Combined P-Glycoprotein and Moderate CYP3A4 Inhibitors with Rivaroxaban or Apixaban Increases Bleeding. J. Thromb. Thrombolysis 2020, 49, 636–643. [Google Scholar] [CrossRef]
- Fernandez, S.; Lenoir, C.; Samer, C.F.; Rollason, V. Drug-Drug Interactions Leading to Adverse Drug Reactions with Rivaroxaban: A Systematic Review of the Literature and Analysis of VigiBase. J. Pers. Med. 2021, 11, 250. [Google Scholar] [CrossRef]
- Fernandez, S.; Lenoir, C.; Samer, C.; Rollason, V. Drug Interactions with Apixaban: A Systematic Review of the Literature and an Analysis of VigiBase, the World Health Organization Database of Spontaneous Safety Reports. Pharmacol. Res. Perspect. 2020, 8, e00647. [Google Scholar] [CrossRef]
- Gronich, N.; Stein, N.; Muszkat, M. Association Between Use of Pharmacokinetic-Interacting Drugs and Effectiveness and Safety of Direct Acting Oral Anticoagulants: Nested Case-Control Study. Clin. Pharmacol. Ther. 2021, 110, 1526–1536. [Google Scholar] [CrossRef]
- Li, A.; Li, M.K.; Crowther, M.; Vazquez, S.R. Drug-Drug Interactions with Direct Oral Anticoagulants Associated with Adverse Events in the Real World: A Systematic Review. Thromb. Res. 2020, 194, 240–245. [Google Scholar] [CrossRef]
- Raymond, J.; Imbert, L.; Cousin, T.; Duflot, T.; Varin, R.; Wils, J.; Lamoureux, F. Pharmacogenetics of Direct Oral Anticoagulants: A Systematic Review. J. Pers. Med. 2021, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Shnayder, N.A.; Petrova, M.M.; Shesternya, P.A.; Savinova, A.V.; Bochanova, E.N.; Zimnitskaya, O.V.; Pozhilenkova, E.A.; Nasyrova, R.F. Using Pharmacogenetics of Direct Oral Anticoagulants to Predict Changes in Their Pharmacokinetics and the Risk of Adverse Drug Reactions. Biomedicines 2021, 9, 451. [Google Scholar] [CrossRef] [PubMed]
- Dimatteo, C.; D’Andrea, G.; Vecchione, G.; Paoletti, O.; Tiscia, G.L.; Santacroce, R.; Correale, M.; Brunetti, N.; Grandone, E.; Testa, S.; et al. ABCB1 SNP Rs4148738 Modulation of Apixaban Interindividual Variability. Thromb. Res. 2016, 145, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Ing Lorenzini, K.; Daali, Y.; Fontana, P.; Desmeules, J.; Samer, C. Rivaroxaban-Induced Hemorrhage Associated with ABCB1 Genetic Defect. Front. Pharmacol. 2016, 7, 494. [Google Scholar] [CrossRef] [Green Version]
- Gouin-Thibault, I.; Delavenne, X.; Blanchard, A.; Siguret, V.; Salem, J.E.; Narjoz, C.; Gaussem, P.; Beaune, P.; Funck-Brentano, C.; Azizi, M.; et al. Interindividual Variability in Dabigatran and Rivaroxaban Exposure: Contribution of ABCB1 Genetic Polymorphisms and Interaction with Clarithromycin. J. Thromb. Haemost. 2017, 15, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Ueshima, S.; Hira, D.; Fujii, R.; Kimura, Y.; Tomitsuka, C.; Yamane, T.; Tabuchi, Y.; Ozawa, T.; Itoh, H.; Horie, M.; et al. Impact of ABCB1, ABCG2, and CYP3A5 Polymorphisms on Plasma Trough Concentrations of Apixaban in Japanese Patients with Atrial Fibrillation. Pharm. Genom. 2017, 27, 329–336. [Google Scholar] [CrossRef]
- Sherry, S.T.; Ward, M.H.; Kholodov, M.; Baker, J.; Phan, L.; Smigielski, E.M.; Sirotkin, K. DbSNP: The NCBI Database of Genetic Variation. Nucleic. Acids Res. 2001, 29, 308–311. [Google Scholar] [CrossRef] [Green Version]
- Kryukov, A.V.; Sychev, D.A.; Andreev, D.A.; Ryzhikova, K.A.; Grishina, E.A.; Ryabova, A.V.; Loskutnikov, M.A.; Smirnov, V.V.; Konova, O.D.; Matsneva, I.A.; et al. Influence of ABCB1 and CYP3A5 Gene Polymorphisms on Pharmacokinetics of Apixaban in Patients with Atrial Fibrillation and Acute Stroke. Pharm. Pers. Med. 2018, 11, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Sychev, D.A.; Vardanyan, A.; Rozhkov, A.; Hachatryan, E.; Badanyan, A.; Smirnov, V.; Ananichuk, A.; Denisenko, N. CYP3A Activity and Rivaroxaban Serum Concentrations in Russian Patients with Deep Vein Thrombosis. Genet. Test Mol. Biomark. 2018, 22, 51–54. [Google Scholar] [CrossRef]
- Sychev, D.; Minnigulov, R.; Bochkov, P.; Ryzhikova, K.; Yudina, I.; Lychagin, A.; Morozova, T. Effect of CYP3A4, CYP3A5, ABCB1 Gene Polymorphisms on Rivaroxaban Pharmacokinetics in Patients Undergoing Total Hip and Knee Replacement Surgery. High Blood Press Cardiovasc. Prev. 2019, 26, 413–420. [Google Scholar] [CrossRef]
- Rubboli, A.; Morici, N.; Lip, G.Y.H. Appropriate Dosing of the Individual Direct Oral Anticoagulants in Atrial Fibrillation: Differences in the Questions to Be Answered. Eur. J. Intern. Med. 2022, S0953-6205(22)00013-9. [Google Scholar] [CrossRef]
- Samer, C.F.; Lorenzini, K.I.; Rollason, V.; Daali, Y.; Desmeules, J.A. Applications of CYP450 Testing in the Clinical Setting. Mol. Diagn. Ther. 2013, 17, 165–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Interactions Médicamenteuses, Cytochromes P450 et P-Glycoprotéine (P Gp). Available online: https://www.hug.ch/sites/interhug/files/structures/pharmacologie_et_toxicologie_cliniques/a5_cytochromes_6_2.pdf (accessed on 3 September 2020).
- UpToDate Lexi-Interact Drug Interaction Checker. Available online: https://www.uptodate.com/contents/search (accessed on 17 September 2021).
- Broccanello, C.; Gerace, L.; Stevanato, P. QuantStudioTM 12K Flex OpenArray® System as a Tool for High-Throughput Genotyping and Gene Expression Analysis. Methods Mol. Biol. 2020, 2065, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Afonina, I.; Zivarts, M.; Kutyavin, I.; Lukhtanov, E.; Gamper, H.; Meyer, R.B. Efficient Priming of PCR with Short Oligonucleotides Conjugated to a Minor Groove Binder. Nucleic Acids Res. 1997, 25, 2657–2660. [Google Scholar] [CrossRef] [PubMed]
- Kutyavin, I.V.; Afonina, I.A.; Mills, A.; Gorn, V.V.; Lukhtanov, E.A.; Belousov, E.S.; Singer, M.J.; Walburger, D.K.; Lokhov, S.G.; Gall, A.A.; et al. 3′-Minor Groove Binder-DNA Probes Increase Sequence Specificity at PCR Extension Temperatures. Nucleic Acids Res. 2000, 28, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Gaedigk, A.; Ingelman-Sundberg, M.; Miller, N.A.; Leeder, J.S.; Whirl-Carrillo, M.; Klein, T.E.; PharmVar Steering Committee. The Pharmacogene Variation (PharmVar) Consortium: Incorporation of the Human Cytochrome P450 (CYP) Allele Nomenclature Database. Clin. Pharmacol. Ther. 2018, 103, 399–401. [Google Scholar] [CrossRef] [Green Version]
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics Knowledge for Personalized Medicine. Clin. Pharmacol. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef]
- Andreu, F.; Colom, H.; Elens, L.; van Gelder, T.; van Schaik, R.H.N.; Hesselink, D.A.; Bestard, O.; Torras, J.; Cruzado, J.M.; Grinyó, J.M.; et al. A New CYP3A5*3 and CYP3A4*22 Cluster Influencing Tacrolimus Target Concentrations: A Population Approach. Clin. Pharm. 2017, 56, 963–975. [Google Scholar] [CrossRef]
- Bosilkovska, M.; Samer, C.F.; Déglon, J.; Rebsamen, M.; Staub, C.; Dayer, P.; Walder, B.; Desmeules, J.A.; Daali, Y. Geneva Cocktail for Cytochrome P450 and P-Glycoprotein Activity Assessment Using Dried Blood Spots. Clin. Pharmacol. Ther. 2014, 96, 349–359. [Google Scholar] [CrossRef]
- Lloret-Linares, C.; Rollason, V.; Lorenzini, K.I.; Samer, C.; Daali, Y.; Gex-Fabry, M.; Aubry, J.-M.; Desmeules, J.; Besson, M. Screening for Genotypic and Phenotypic Variations in CYP450 Activity in Patients with Therapeutic Problems in a Psychiatric Setting, a Retrospective Study. Pharmacol. Res. 2017, 118, 104–110. [Google Scholar] [CrossRef]
- Bosilkovska, M.; Déglon, J.; Samer, C.; Walder, B.; Desmeules, J.; Staub, C.; Daali, Y. Simultaneous LC-MS/MS Quantification of P-Glycoprotein and Cytochrome P450 Probe Substrates and Their Metabolites in DBS and Plasma. Bioanalysis 2014, 6, 151–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerdi, M.C.; Daali, Y.; Oestreicher, M.K.; Cherkaoui, S.; Dayer, P. A Simplified Analytical Method for a Phenotyping Cocktail of Major CYP450 Biotransformation Routes. J. Pharm. Biomed. Anal. 2004, 35, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Ensembl Project The 1000 Genome Browser-Homo Sapiens. Available online: https://www.ensembl.org/Homo_sapiens/Info/Index (accessed on 17 February 2022).
- Sebuhyan, M.; Crichi, B.; Abdallah, N.A.; Bonnet, C.; Deville, L.; Marjanovic, Z.; Farge, D. Drug-Drug Interaction (DDI) with Direct Oral Anticoagulant (DOAC) in Patients with Cancer. J. Med. Vasc. 2020, 45, 6S31–36S38. [Google Scholar] [CrossRef] [PubMed]
- Sodhi, J.K.; Benet, L.Z. The Necessity of Using Changes in Absorption Time to Implicate Intestinal Transporter Involvement in Oral Drug-Drug Interactions. AAPS J. 2020, 22, 111. [Google Scholar] [CrossRef] [PubMed]
- Kou, W.; Sodhi, J.K.; Wu, X.; Benet, L.Z. Investigating Intestinal Transporter Involvement in Rivaroxaban Disposition through Examination of Changes in Absorption. Pharm. Res. 2021, 38, 795–801. [Google Scholar] [CrossRef]
- Saib, S.; Hodin, S.; Bin, V.; Ollier, E.; Delavenne, X. In Vitro Evaluation of P-Gp-Mediated Drug-Drug Interactions Using the RPTEC/TERT1 Human Renal Cell Model. Eur. J. Drug Metab. Pharm. 2022, 47, 223–233. [Google Scholar] [CrossRef]
- König, J.; Müller, F.; Fromm, M.F. Transporters and Drug-Drug Interactions: Important Determinants of Drug Disposition and Effects. Pharmacol. Rev. 2013, 65, 944–966. [Google Scholar] [CrossRef] [Green Version]
- Stanke-Labesque, F.; Gautier-Veyret, E.; Chhun, S.; Guilhaumou, R. French Society of Pharmacology and Therapeutics Inflammation Is a Major Regulator of Drug Metabolizing Enzymes and Transporters: Consequences for the Personalization of Drug Treatment. Pharmacol. Ther. 2020, 215, 107627. [Google Scholar] [CrossRef]
- Murakami, T.; Bodor, E.; Bodor, N. Modulation of Expression/Function of Intestinal P-Glycoprotein under Disease States. Expert Opin. Drug Metab. Toxicol. 2020, 16, 59–78. [Google Scholar] [CrossRef]
- Wolking, S.; Schaeffeler, E.; Lerche, H.; Schwab, M.; Nies, A.T. Impact of Genetic Polymorphisms of ABCB1 (MDR1, P-Glycoprotein) on Drug Disposition and Potential Clinical Implications: Update of the Literature. Clin. Pharm. 2015, 54, 709–735. [Google Scholar] [CrossRef]
- Seelig, A. P-Glycoprotein: One Mechanism, Many Tasks and the Consequences for Pharmacotherapy of Cancers. Front. Oncol. 2020, 10, 576559. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Heidbuchel, H. The Significance of Drug-Drug and Drug-Food Interactions of Oral Anticoagulation. Arrhythm. Electrophysiol. Rev. 2018, 7, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Drug Administration (FDA). SAVAYSA (Edoxaban)-Summary of Product Characteristics. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/206316lbl.pdf (accessed on 6 February 2022).
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsh Raccah, B.; Rottenstreich, A.; Zacks, N.; Muszkat, M.; Matok, I.; Perlman, A.; Kalish, Y. Drug Interaction as a Predictor of Direct Oral Anticoagulant Drug Levels in Atrial Fibrillation Patients. J. Thromb. Thrombolysis 2018, 46, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Poggesi, I.; Benedetti, M.S.; Whomsley, R.; Le Lamer, S.; Molimard, M.; Watelet, J.-B. Pharmacokinetics in Special Populations. Drug Metab. Rev. 2009, 41, 422–454. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.-C.; Lin, C.-J. The Regulation of Drug-Metabolizing Enzymes and Membrane Transporters by Inflammation: Evidences in Inflammatory Diseases and Age-Related Disorders. J. Food Drug Anal. 2019, 27, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Aitken, A.E.; Richardson, T.A.; Morgan, E.T. Regulation of Drug-Metabolizing Enzymes and Transporters in Inflammation. Annu. Rev. Pharmacol. Toxicol. 2006, 46, 123–149. [Google Scholar] [CrossRef] [PubMed]
- Aitken, A.E.; Morgan, E.T. Gene-Specific Effects of Inflammatory Cytokines on Cytochrome P450 2C, 2B6 and 3A4 MRNA Levels in Human Hepatocytes. Drug Metab. Dispos. 2007, 35, 1687–1693. [Google Scholar] [CrossRef] [PubMed]
- Lenoir, C.; Rollason, V.; Desmeules, J.A.; Samer, C.F. Influence of Inflammation on Cytochromes P450 Activity in Adults: A Systematic Review of the Literature. Front. Pharmacol. 2021, 12, 733935. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, C.; Buyse, M.; German-Fattal, M.; Gimenez, F. Influence of the Pro-Inflammatory Cytokines on P-Glycoprotein Expression and Functionality. J. Pharm. Pharm. Sci. 2004, 7, 359–371. [Google Scholar] [PubMed]
- Drozdzik, M.; Czekawy, I.; Oswald, S.; Drozdzik, A. Intestinal Drug Transporters in Pathological States: An Overview. Pharmacol. Rep. 2020, 72, 1173–1194. [Google Scholar] [CrossRef] [PubMed]
- McRae, M.P.; Brouwer, K.L.R.; Kashuba, A.D.M. Cytokine Regulation of P-Glycoprotein. Drug Metab. Rev. 2003, 35, 19–33. [Google Scholar] [CrossRef]
- Elmeliegy, M.; Vourvahis, M.; Guo, C.; Wang, D.D. Effect of P-Glycoprotein (P-Gp) Inducers on Exposure of P-Gp Substrates: Review of Clinical Drug-Drug Interaction Studies. Clin. Pharm. 2020, 59, 699–714. [Google Scholar] [CrossRef] [Green Version]
- Harskamp, R.E.; Teichert, M.; Lucassen, W.A.M.; van Weert, H.C.P.M.; Lopes, R.D. Impact of Polypharmacy and P-Glycoprotein- and CYP3A4-Modulating Drugs on Safety and Efficacy of Oral Anticoagulation Therapy in Patients with Atrial Fibrillation. Cardiovasc. Drugs Ther. 2019, 33, 615–623. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, G.R. Drug Metabolism and Variability among Patients in Drug Response. N. Engl. J. Med. 2005, 352, 2211–2221. [Google Scholar] [CrossRef] [Green Version]
- Wright, W.C.; Chenge, J.; Chen, T. Structural Perspectives of the CYP3A Family and Their Small Molecule Modulators in Drug Metabolism. Liver Res. 2019, 3, 132–142. [Google Scholar] [CrossRef]
- Huppertz, A.; Grond-Ginsbach, C.; Dumschat, C.; Foerster, K.I.; Burhenne, J.; Weiss, J.; Czock, D.; Purrucker, J.C.; Rizos, T.; Haefeli, W.E. Unexpected Excessive Apixaban Exposure: Case Report of a Patient with Polymorphisms of Multiple Apixaban Elimination Pathways. BMC Pharmacol. Toxicol. 2019, 20, 53. [Google Scholar] [CrossRef] [Green Version]
- Gulilat, M.; Keller, D.; Linton, B.; Pananos, A.D.; Lizotte, D.; Dresser, G.K.; Alfonsi, J.; Tirona, R.G.; Kim, R.B.; Schwarz, U.I. Drug Interactions and Pharmacogenetic Factors Contribute to Variation in Apixaban Concentration in Atrial Fibrillation Patients in Routine Care. J. Thromb. Thrombolysis 2020, 49, 294–303. [Google Scholar] [CrossRef]
- Sodhi, J.K.; Liu, S.; Benet, L.Z. Intestinal Efflux Transporters P-Gp and BCRP Are Not Clinically Relevant in Apixaban Disposition. Pharm. Res. 2020, 37, 208. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, J.; Kinjo, T.; Iizuka, M.; Ueno, K.; Tomita, H.; Niioka, T. Impact of Gene Polymorphisms in Drug-Metabolizing Enzymes and Transporters on Trough Concentrations of Rivaroxaban in Patients with Atrial Fibrillation. Basic Clin. Pharmacol. Toxicol. 2021, 128, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Mueck, W.; Kubitza, D.; Becka, M. Co-Administration of Rivaroxaban with Drugs that Share Its Elimination Pathways: Pharmacokinetic Effects in Healthy Subjects. Br. J. Clin. Pharmacol. 2013, 76, 455–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, T.; Chen, Y.; Wang, D.; Wang, L.; Dong, P.; Zhao, S.; Wang, C.; Meng, Q.; Sun, H.; Liu, K.; et al. Identifying the Dominant Contribution of Human Cytochrome P450 2J2 to the Metabolism of Rivaroxaban, an Oral Anticoagulant. Cardiovasc. Drugs Ther. 2022, 36, 121–129. [Google Scholar] [CrossRef]
- Zanger, U.M.; Schwab, M. Cytochrome P450 Enzymes in Drug Metabolism: Regulation of Gene Expression, Enzyme Activities, and Impact of Genetic Variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef] [PubMed]
- Vio, R.; Proietti, R.; Rigato, M.; Calò, L.A. Clinical Evidence for the Choice of the Direct Oral Anticoagulant in Patients with Atrial Fibrillation According to Creatinine Clearance. Pharmaceuticals 2021, 14, 279. [Google Scholar] [CrossRef]
- DeWald, T.A.; Washam, J.B.; Becker, R.C. Anticoagulants: Pharmacokinetics, Mechanisms of Action, and Indications. Neurosurg. Clin. N. Am. 2018, 29, 503–515. [Google Scholar] [CrossRef]
- Fava, J.P.; Starr, K.M.; Ratz, D.; Clemente, J.L. Dosing Challenges with Direct Oral Anticoagulants in the Elderly: A Retrospective Analysis. Ther. Adv. Drug Saf. 2018, 9, 405–414. [Google Scholar] [CrossRef] [Green Version]
- Sugrue, A.; Sanborn, D.; Amin, M.; Farwati, M.; Sridhar, H.; Ahmed, A.; Mehta, R.; Siontis, K.C.; Mulpuru, S.K.; Deshmukh, A.J.; et al. Inappropriate Dosing of Direct Oral Anticoagulants in Patients with Atrial Fibrillation. Am. J. Cardiol. 2021, 144, 52–59. [Google Scholar] [CrossRef]
- Trujillo-Santos, J.; Beroiz, P.; Moustafa, F.; Alonso, A.; Morejon, E.; López-Reyes, R.; Casado, I.; Porras, J.A.; Flores, K.; López-Núñez, J.J.; et al. Rivaroxaban or Apixaban in Fragile Patients with Acute Venous Thromboembolism. Thromb. Res. 2020, 193, 160–165. [Google Scholar] [CrossRef]
- Gulilat, M.; Jandoc, R.; Jeyakumar, N.; McArthur, E.; Garg, A.X.; Kim, R.B.; Tirona, R.G.; Schwarz, U.I. Association of Sex With Stroke and Bleeding Risk of Apixaban and Rivaroxaban in Elderly Atrial Fibrillation Patients Using Propensity Score Weights. CJC Open 2022, 4, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Toorop, M.M.A.; van Rein, N.; Nierman, M.C.; Vermaas, H.W.; Huisman, M.V.; van der Meer, F.J.M.; Cannegieter, S.C.; Lijfering, W.M. Inter- and Intra-Individual Concentrations of Direct Oral Anticoagulants: The KIDOAC Study. J. Thromb. Haemost. 2022, 20, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.R.; Li, N.; Vanassche, T.; Coppens, M.; Spyropoulos, A.C.; Syed, S.; Radwi, M.; Duncan, J.; Schulman, S.; Douketis, J.D. Predictors of Preprocedural Direct Oral Anticoagulant Levels in Patients Having an Elective Surgery or Procedure. Blood Adv. 2020, 4, 3520–3527. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.H.; Andersson, U.; Lopes, R.D.; Hijazi, Z.; Hohnloser, S.H.; Ezekowitz, J.A.; Halvorsen, S.; Hanna, M.; Commerford, P.; Ruzyllo, W.; et al. Apixaban 5 Mg Twice Daily and Clinical Outcomes in Patients With Atrial Fibrillation and Advanced Age, Low Body Weight, or High Creatinine: A Secondary Analysis of a Randomized Clinical Trial. JAMA Cardiol. 2016, 1, 673–681. [Google Scholar] [CrossRef] [Green Version]
- Frost, C.E.; Song, Y.; Shenker, A.; Wang, J.; Barrett, Y.C.; Schuster, A.; Harris, S.I.; LaCreta, F. Effects of Age and Sex on the Single-Dose Pharmacokinetics and Pharmacodynamics of Apixaban. Clin. Pharm. 2015, 54, 651–662. [Google Scholar] [CrossRef] [Green Version]
- Upreti, V.V.; Wang, J.; Barrett, Y.C.; Byon, W.; Boyd, R.A.; Pursley, J.; LaCreta, F.P.; Frost, C.E. Effect of Extremes of Body Weight on the Pharmacokinetics, Pharmacodynamics, Safety and Tolerability of Apixaban in Healthy Subjects. Br. J. Clin. Pharmacol. 2013, 76, 908–916. [Google Scholar] [CrossRef]
- Manikandan, P.; Nagini, S. Cytochrome P450 Structure, Function and Clinical Significance: A Review. Curr. Drug Targets 2018, 19, 38–54. [Google Scholar] [CrossRef]
- Keller, G.A.; Gago, M.L.F.; Diez, R.A.; Di Girolamo, G. In Vivo Phenotyping Methods: Cytochrome P450 Probes with Emphasis on the Cocktail Approach. Curr. Pharm. Des. 2017, 23, 2035–2049. [Google Scholar] [CrossRef]
- Song, Y.; Li, C.; Liu, G.; Liu, R.; Chen, Y.; Li, W.; Cao, Z.; Zhao, B.; Lu, C.; Liu, Y. Drug-Metabolizing Cytochrome P450 Enzymes Have Multifarious Influences on Treatment Outcomes. Clin. Pharm. 2021, 60, 585–601. [Google Scholar] [CrossRef]
- Ing Lorenzini, K.; Desmeules, J.; Rollason, V.; Bertin, S.; Besson, M.; Daali, Y.; Samer, C.F. CYP450 Genotype-Phenotype Concordance Using the Geneva Micrococktail in a Clinical Setting. Front. Pharmacol. 2021, 12, 730637. [Google Scholar] [CrossRef]
- Bachmann, K.A. Genotyping and Phenotyping the Cytochrome P-450 Enzymes. Am. J. Ther. 2002, 9, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.R.; Smith, R.L. Addressing Phenoconversion: The Achilles’ Heel of Personalized Medicine. Br. J. Clin. Pharmacol. 2015, 79, 222–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.H.; Yamazaki, M. Role of P-Glycoprotein in Pharmacokinetics: Clinical Implications. Clin. Pharm. 2003, 42, 59–98. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Apixaban | Rivaroxaban |
|---|---|---|
| Gender, n (%) | ||
| Male | 101 (61.6%) | 89 (65.9%) |
| Female | 63 (38.4%) | 46 (34.1%) |
| Age, mean (SD) | ||
| Age (years) | 77.4 (9.8) | 71.1 (12.1) |
| Weight, mean (SD) | ||
| Weight (kg) | 77.4 (9.8) | 82.1 (18.0) |
| BMI (kg/m2) | 26.8 (5.6) | 27.7 (5.7) |
| Indication, n (%) | ||
| AF | 145 (88.4%) | 92 (67.6%) |
| DVT and PE treatment | 13 (7.9%) | 35 (25.7%) |
| DVT and PE prophylaxis | 6 (3.7%) | 9 (6.6%) |
| Doses, n (%) | ||
| 2.5 mg bid | 70 (42.7%) | NA |
| 5 mg bid | 87 (53%) | NA |
| 10 mg bid | 7 (4.3%) | NA |
| 10 mg od | NA | 6 (4.4%) |
| 15 mg od | NA | 17 (12.6%) |
| 20 mg od | NA | 80 (59.3%) |
| 15 mg bid | NA | 32 (23.7%) |
| Dosage adequacy, n (%) | ||
| Adequate dosage | 166 (70.7%) | 108 (80%) |
| Inadequate dosage | 47 (28.7%) | 27 (20%) |
| Unknown | 1 | 0 |
| Inadequate dosage, n (%) | ||
| 2.5 mg bid | 45 (95.7%) | NA |
| 10 mg od | NA | 3 (11.1%) |
| 15 mg od | NA | 9 (33.3%) |
| 20 mg od | NA | 9 (33.3%) |
| 15 mg bid | NA | 6 (22.2%) |
| AF | 43 (91.5%) | 22 (81.5%) |
| Liver injury, n (%) or mean (SD) | ||
| ALAT | 34.5 (46.7) | 38.9 (41.6) |
| No | 149 (92.5%) | 122 (90.4%) |
| Yes | 12 (7.5%) | 13 (9.6%) |
| Missing data | 3 | 0 |
| Renal function, n (%) or mean (SD) | ||
| Creatinine (μ/moL) | 110.8 (111.4) | 95.8 (88.3) |
| CrCl (mL/min/1.73 m2) according to Cockcroft | 63.8 (27.5) | 77.7 (28.0) |
| Normal | 75 (46.0%) | 91 (67.4%) |
| Moderate | 79 (48.5%) | 43 (31.9%) |
| Severe | 9 (5.5%) | 1 (0.7%) |
| Missing data | 1 | 0 |
| Characteristics | Apixaban | Rivaroxaban |
|---|---|---|
| Predicted phenotype from genotype CYP3A, n (%) | ||
| PM | 18 (11.3%) | 13 (10.1%) |
| IM | 127 (79.9%) | 99 (76.7%) |
| NM | 14 (8.8%) | 17 (13.2%) |
| Missing data | 5 | 6 |
| Genotype ABCB1 1236C>T, n (%) | ||
| No T | 52 (32.1%) | 44 (33.6%) |
| One T | 74 (45.7%) | 62 (47.3%) |
| Two T | 36 (22.2%) | 25 (19.1%) |
| Missing data | 2 | 4 |
| Genotype ABCB1 2677G>T, n (%) | ||
| No T | 49 (30.4%) | 43 (33.1%) |
| One T | 75 (46.6%) | 56 (43.1%) |
| Two T | 37 (23.0%) | 31 (23.8%) |
| Missing data | 3 | 5 |
| Genotype ABCB1 3435C>T, n (%) | ||
| No T | 41 (25.5%) | 36 (27.5%) |
| One T | 74 (46.0%) | 58 (44.3%) |
| Two T | 46 (28.6%) | 37 (28.2%) |
| Missing data | 3 | 4 |
| AUC0–6h of Apixaban | AUC0–6h of Rivaroxaban | |
|---|---|---|
| Intercept | −46.30 (−339.86 to 247.26); p = 0.7557 | −418.12 (−776.92 to −59.32); p = 0.0228 |
| Variables | ||
| MRmidazolam, per log10 | 10.03 (−64.67 to 84.72); p = 0.7912 | −90.27 (−209.99 to 29.45); p = 0.1381 |
| AUCfexofenadine, per log10 | 173.96 (77.33 to 270.58); p = 0.0005 | 232.51 (105.69 to 359.33); p = 0.0004 |
| Weight, per kg | −0.25 (−2.12 to 1.61); p = 0.7881 | 1.19 (−0.63 to 3.01); p = 0.1973 |
| CrCl, per unit | −2.13 (−3.72 to −0.54); p = 0.0091 | −0.44 (−2.53 to 1.65); p = 0.6675 |
| ALAT, per unit | 0.44 (−0.91 to 1.79); p = 0.5217 | 0.08 (−0.65 to 0.81); p = 0.8314 |
| Gender | ||
| Male | Reference category | Reference category |
| Female | 43.31 (−15.31 to 101.92); p = 0.1464 | 44.63 (−27.63 to 116.89); p = 0.2238 |
| Dose | ||
| 2.5 mg bid | Reference category; p < 0.0001 * | NA |
| 5 mg bid | 279.44 (221.14 to 337.75); p < 0.0001 | NA |
| 10 mg bid | 688.81 (478.01 to 889.60); p < 0.0001 | NA |
| 10 mg od | NA | Reference category; p = 0.0045 * |
| 15 mg od | NA | 90.97 (−32.04 to 213.99); p = 0.1457 |
| 20 mg od | NA | 165.18 (37.54 to 292.83); p = 0.0116 |
| 15 mg bid | NA | 180.44 (64.84 to 296.02); p = 0.0025 |
| Age | ||
| <65 years | Reference category; p = 0.2064 * | Reference category; p = 0.1191 * |
| 65–74 years | 95.82 (−10.13 to 201.76); p = 0.0759 | 81.34 (15.35 to 147.32); p = 0.0161 |
| 75–84 years | 82.33 (−22.35 to 187.01); p = 0.1222 | 59.56 (−53.36 to 172.48); p = 0.2984 |
| >85 years | 113.34 (−1.13 to 227.82); p = 0.0523 | 56.06 (−54.25 to 166.38); p = 0.3163 |
| AUC0–6h of Apixaban | AUC0–6h of Rivaroxaban | |
|---|---|---|
| Intercept | 398.75 (196.35 to 601.15); p = 0.0002 | −39.45 (−424.81 to 345.91); p = 0.8396 |
| Variables | ||
| Weight, per kg | −0.11 (−2.08 to 1.86); p = 0.9142 | 1.89 (0.05 to 3.72); p = 0.0442 |
| CrCl, per unit | 2.38 (−3.97 to −0.79); p = 0.0036 | −0.43 (−2.90 to 2.05); p = 0.7333 |
| ALAT, per unit | 0.45 (−1.20 to 2.11); p = 0.5893 | 0.34 (−0.35 to 1.04); p = 0.3280 |
| Predicted phenotype from genotype CYP3A | ||
| IM | Reference category; p = 0.2154 * | Reference category; p = 0.0021 * |
| NM | −15.50 (−139.46 to 108.47); p = 0.8051 | 142.49 (56.08 to 228.90); p = 0.0014 |
| PM | −77.10 (-164.78 to 10.58); p = 0.0843 | 134.23 (−24.82 to 293.28); p = 0.0973 |
| Genotype ABCB1 1236C>T | ||
| No mutation | Reference category; p = 0.9723 * | Reference category; p = 0.4955 * |
| Heterozygous for mutation | −12.33 (−138.96 to 114.30); p = 0.8476 | −46.50 (−163.59 to 70.59); p = 0.4329 |
| Homozygous for mutation | −20.09 (−190.52 to 150.34); p = 0.8160 | 21.46 (−125.94 to 168.86); p = 0.7735 |
| Genotype ABCB1 3435C>T | ||
| No mutation | Reference category; p = 0.5600 * | Reference category; p = 0.2663 * |
| Heterozygous for mutation | −51.58 (−149.70 to 46.54); p = 0.3004 | −51.69 (−170.92 to 67.54); p = 0.3921 |
| Homozygous for mutation | −18.22 (−112.45 to 76.01); p = 0.7028 | −71.90 (−161.27 to 17.46); p = 0.1137 |
| Genotype ABCB1 2677G>T | ||
| No mutation | Reference category; p = 0.9069 * | Reference category; p = 0.6892 * |
| Heterozygous for mutation | 29.83 (−106.91 to 166.57); p = 0.6669 | 56.52 (−75.24 to 188.29); p = 0.3971 |
| Homozygous for mutation | 32.15 (−138.11 to 202.40); p = 0.7095 | 54.86 (−96.09 to 205.81); p = 0.4728 |
| Gender | ||
| Male | Reference category | Reference category |
| Female | 50.24 (−19.91 to 120.38); p = 0.3004 | 46.71 (−29.08 to 122.49); p = 0.2246 |
| Dose | ||
| 2.5 mg bid | Reference category; p < 0.0001 * | NA |
| 5 mg bid | 275.77 (201.67 to 349.87); p < 0.0001 | NA |
| 10 mg bid | 689.14 (470.72 to 907.55); p < 0.0001 | NA |
| 10 mg od | NA | Reference category; p = 0.0012 * |
| 15 mg od | NA | 128.66 (−17.23 to 274.55); p = 0.0833 |
| 20 mg od | NA | 250.76 (117.30 to 384.22); p = 0.0003 |
| 15 mg bid | NA | 221.57 (75.08 to 368.07); p = 0.0034 |
| Age | ||
| <65 years | Reference category; p = 0.3989 * | Reference category; p = 0.0062 * |
| 65–74 years | 81.29 (−37.74 to 200.33); p = 0.1719 | 138.27 (61.87 to 214.67); p = 0.0005 |
| 75–84 years | 57.29 (−50.00 to 164.58); p = 0.2929 | 127.49 (−17.50 to 272.48); p = 0.0842 |
| >85 years | 104.66 (−32.37 to 241.70); p = 0.1333 | 124.29 (−14.68 to 263.25); p = 0.0791 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenoir, C.; Terrier, J.; Gloor, Y.; Gosselin, P.; Daali, Y.; Combescure, C.; Desmeules, J.A.; Samer, C.F.; Reny, J.-L.; Rollason, V. Impact of the Genotype and Phenotype of CYP3A and P-gp on the Apixaban and Rivaroxaban Exposure in a Real-World Setting. J. Pers. Med. 2022, 12, 526. https://doi.org/10.3390/jpm12040526
Lenoir C, Terrier J, Gloor Y, Gosselin P, Daali Y, Combescure C, Desmeules JA, Samer CF, Reny J-L, Rollason V. Impact of the Genotype and Phenotype of CYP3A and P-gp on the Apixaban and Rivaroxaban Exposure in a Real-World Setting. Journal of Personalized Medicine. 2022; 12(4):526. https://doi.org/10.3390/jpm12040526
Chicago/Turabian StyleLenoir, Camille, Jean Terrier, Yvonne Gloor, Pauline Gosselin, Youssef Daali, Christophe Combescure, Jules Alexandre Desmeules, Caroline Flora Samer, Jean-Luc Reny, and Victoria Rollason. 2022. "Impact of the Genotype and Phenotype of CYP3A and P-gp on the Apixaban and Rivaroxaban Exposure in a Real-World Setting" Journal of Personalized Medicine 12, no. 4: 526. https://doi.org/10.3390/jpm12040526
APA StyleLenoir, C., Terrier, J., Gloor, Y., Gosselin, P., Daali, Y., Combescure, C., Desmeules, J. A., Samer, C. F., Reny, J.-L., & Rollason, V. (2022). Impact of the Genotype and Phenotype of CYP3A and P-gp on the Apixaban and Rivaroxaban Exposure in a Real-World Setting. Journal of Personalized Medicine, 12(4), 526. https://doi.org/10.3390/jpm12040526