
Differences and Commonalities in Children with Childhood Apraxia of Speech and Comorbid Neurodevelopmental Disorders: A Multidimensional Perspective

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedures and Measures
2.2.1. Clinical Assessment
2.2.2. Speech and Language Assessment
2.2.3. Genetic Investigations
2.2.4. Neuroradiological Investigation
2.3. Statistical Analysis
3. Results
3.1. Genetic Investigation
3.2. Structural Brain MR
3.3. Speech Performances
3.4. Language Performances
3.5. Correlations between Speech and Language Measures
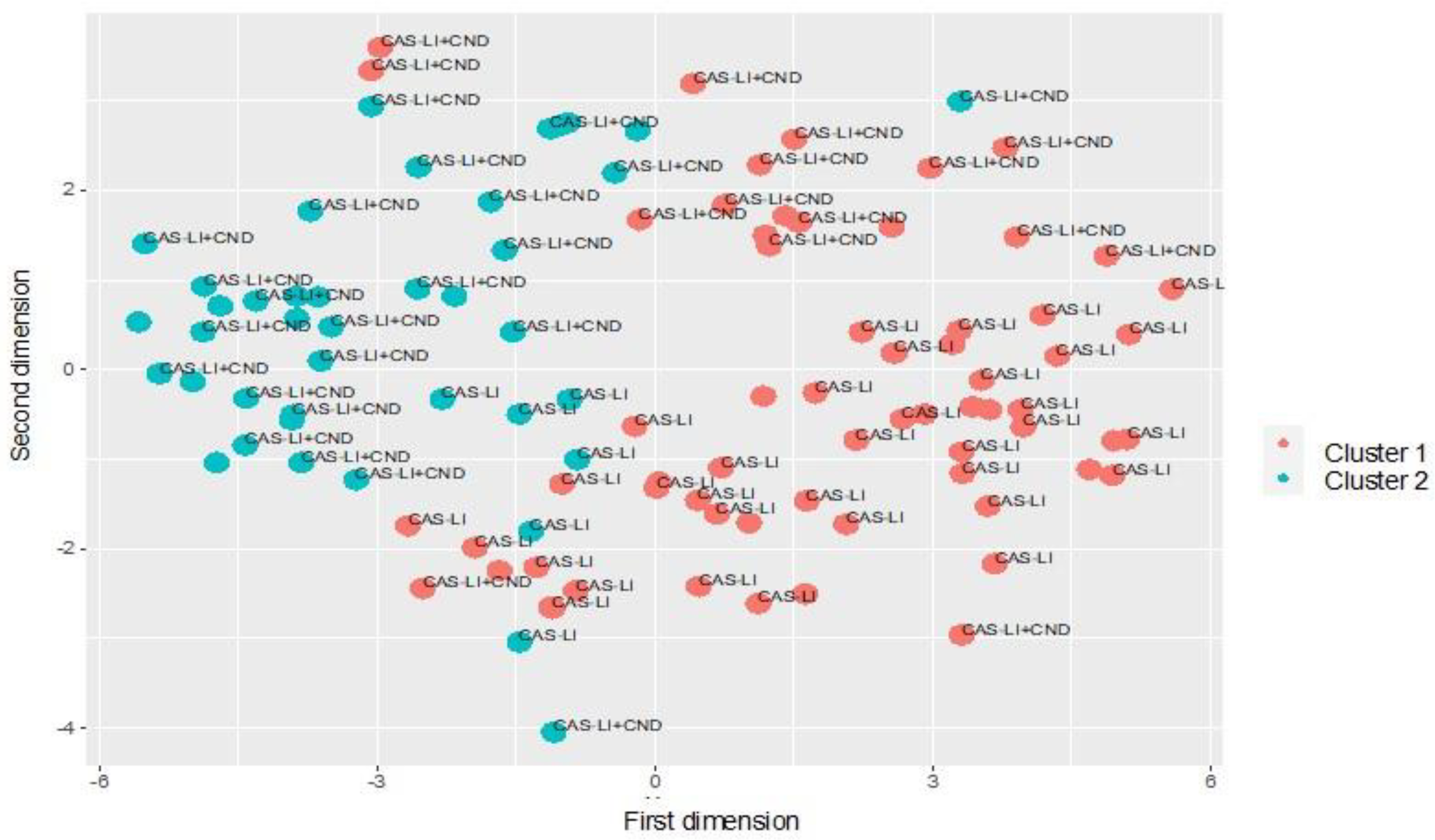
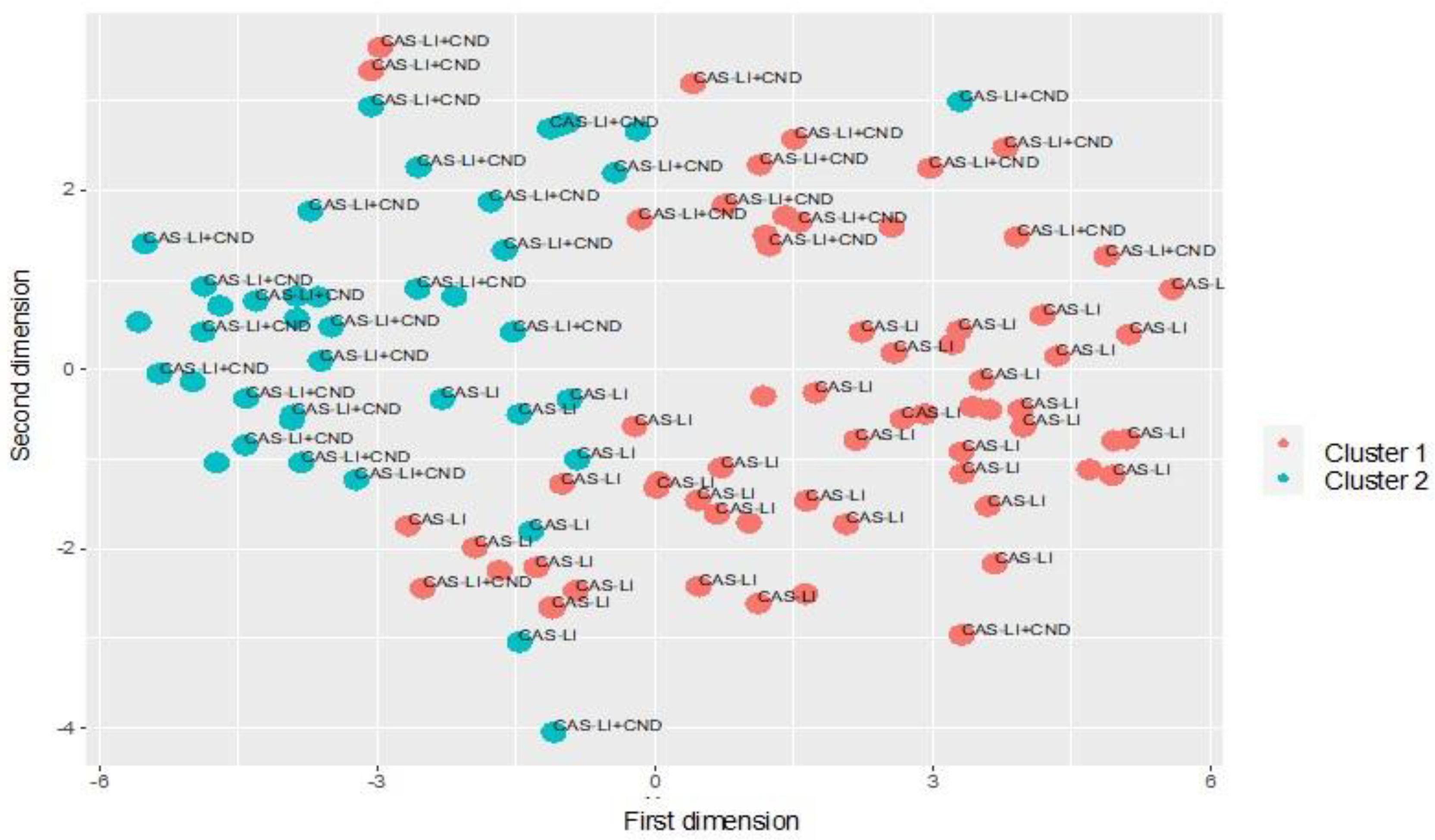
3.6. Cluster Analysis
4. Discussion
4.1. CAS Co-Occuring with Complex Neurodevelopmental Disorders
4.2. Speech and Language Profiles
4.3. Genetic and Neuroradiological Abnormalities and Their Distribution in CAS-LI and CAS-LI + CND
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Speech-Language-Hearing Association—ASHA, Childhood Apraxia of Speech. Technical Report. 2007. Available online: https://www.asha.org/policy/tr2007-00278/ (accessed on 18 February 2022).
- Shriberg, L.D.; Potter, N.L.; Strand, E.A. Prevalence and phenotype of childhood apraxia of speech in youth with galactosemia. J. Speech Lang. Hear. Res. 2011, 54, 487–519. [Google Scholar] [CrossRef] [Green Version]
- Shriberg, L.D.; Lohmeier, H.L.; Strand, E.A.; Jakielski, K.J. Encoding, memory and transcoding deficits in childhood apraxia of speech. Clin. Linguist. Phon. 2012, 26, 445–482. [Google Scholar] [CrossRef] [PubMed]
- Lewis, B.A.; Freebairn, L.A.; Hansen, A.J.; Iyengar, S.K.; Taylor, H.G. School-age follow-up of children with childhood apraxia of speech. Lang. Speech Hear. Serv Sch. 2004, 35, 122–140. [Google Scholar] [CrossRef]
- Lewis, B.A.; Allison, A.A.; Freebairn, L.A.; Hansen, A.J.; Sucheston, L.E.; Ku, I.; Taylor, G.; Iyengar, S.K.; Stein, C.M. Literacy outcome of children with early childhood speech sound disorders: Impact of endophenotypes. J. Speech Lang. Hear. 2011, 54, 1628–1643. [Google Scholar] [CrossRef] [Green Version]
- Miller, G.J.; Lewis, B.; Benchek, P.; Freebairn, L.; Tag, J.; Budge, K.; Iyengar, S.K.; Voss-Hoynes, H.; Taylor, H.G.; Stein, C. Reading outcomes for individuals with histories of suspected childhood apraxia of speech. Am. J. Speech Lang. Pathol. 2019, 28, 1432–1447. [Google Scholar] [CrossRef]
- Lai, C.S.; Fisher, S.E.; Hurst, J.A.; Vargha-Khadem, F.; Monaco, A.P. A forkhead-domain gene is mutated in a severe speech and language disorder. Nature 2001, 413, 519–523. [Google Scholar] [CrossRef]
- Graham, S.A.; Fisher, S.E. Understanding language from a genomic perspective. Annu. Rev. Genet. 2015, 49, 131–160. [Google Scholar] [CrossRef]
- Nagy, O.; Kárteszi, J.; Elmont, B.; Ujfalusi, A. Case Report: Expressive speech disorder in a family as a hallmark of 7q31 deletion involving the FOXP2 gene. Front. Pediatr. 2021, 20, 664548. [Google Scholar] [CrossRef]
- Laffin, J.J.; Raca, G.; Jackson, C.A.; Strand, E.A.; Jakielski, K.J.; Shriberg, L.D. Novel candidate genes and regions for childhood apraxia of speech identified by array comparative genomic hybridization. Genet. Med. 2012, 14, 928–936. [Google Scholar] [CrossRef] [Green Version]
- Newbury, D.F.; Mari, F.; Sadighi Akha, E.; Macdermot, K.D.; Canitano, R.; Monaco, A.P.; Taylor, J.C.; Renieri, A.; Fisher, S.E.; Knight, S.J. Dual copy number variants involving 16p11 and 6q22 in a case of childhood apraxia of speech and pervasive developmental disorder. Eur. J. Hum. Genet. 2013, 21, 361–365. [Google Scholar] [CrossRef] [Green Version]
- Thevenon, J.; Callier, P.; Andrieux, J.; Delobel, B.; David, A.; Sukno, S.; Minot, D.; Mosca Anne, L.; Marle, N.; Sanlaville, D.; et al. 12p13.33 microdeletion including ELKS/ERC1, a new locus associated with childhood apraxia of speech. Eur. J. Hum. Genet. 2013, 21, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Raca, G.; Baas, B.S.; Kirmani, S.; Laffin, J.J.; Jackson, C.A.; Strand, E.A.; Shriberg, L.D. Childhood Apraxia of Speech (CAS) in two patients with 16p11.2 microdeletion syndrome. Eur. J. Hum. Genet. 2013, 21, 455–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorenko, E.; Morgan, A.; Murray, E.; Cardinaux, A.; Mei, C.; Tager-Flusberg, H.; Fisher, S.E.; Kanwisher, N. A highly penetrant form of childhood apraxia of speech due to deletion of 16p11.2. Eur. J. Hum. Genet. 2016, 24, 310. [Google Scholar] [CrossRef] [PubMed]
- Mei, C.; Fedorenko, E.; Amor, D.J.; Boys, A.; Hoeflin, C.; Carew, P.; Burgess, T.; Fisher, S.E.; Morgan, A.T. Deep phenotyping of speech and language skills in individuals with 16p11.2 deletion. Eur. J. Hum. Genet. 2018, 26, 676–686. [Google Scholar] [CrossRef]
- Worthey, E.A.; Raca, G.; Laffin, J.J.; Wilk, B.M.; Harris, J.M.; Jakielski, K.J.; Dimmock, D.P.; Strand, E.A.; Shriberg, L.D. Whole-exome sequencing supports genetic heterogeneity in childhood apraxia of speech. J. Neurodev. Disord. 2013, 5, 29. [Google Scholar] [CrossRef] [Green Version]
- Eising, E.; Carrion-Castillo, A.; Vino, A.; Strand, E.A.; Jakielski, K.J.; Scerri, T.S.; Hildebrand, M.S.; Webster, R.; Ma, A.; Mazoyer, B.; et al. A set of regulatory genes co-expressed in embryonic human brain is implicated in disrupted speech development. Mol. Psychiatry 2019, 24, 1065–1078. [Google Scholar] [CrossRef] [Green Version]
- Hildebrand, M.S.; Jackson, V.E.; Scerri, T.S.; Van Reyk, O.; Coleman, M.; Braden, R.O.; Turner, S.; Rigbye, K.A.; Boys, A.; Barton, S.; et al. Severe childhood speech disorder: Gene discovery highlights transcriptional dysregulation. Neurology 2020, 94, e2148–e2167. [Google Scholar] [CrossRef]
- Guerra, J.; Cacabelos, R. Genomics of speech and language disorders. J. Transl. Genet. Genom. 2019, 3, 9. [Google Scholar] [CrossRef]
- Benchek, P.; Igo, R.P., Jr.; Voss-Hoynes, H.; Wren, Y.; Miller, G.; Truitt, B.; Zhang, W.; Osterman, M.; Freebairn, L.; Tag, J.; et al. Association between genes regulating neural pathways for quantitative traits of speech and language disorders. NPJ Genom. Med. 2021, 6, 64. [Google Scholar] [CrossRef]
- Liégeois, F.J.; Morgan, A.T. Neural bases of childhood speech disorders: Lateralization and plasticity for speech functions during development. Neurosci. Biobehav. Rev. 2012, 36, 439–458. [Google Scholar] [CrossRef]
- Chilosi, A.M.; Lorenzini, I.; Fiori, S.; Graziosi, V.; Rossi, G.; Pasquariello, R.; Cipriani, P.; Cioni, G. Behavioral and neurobiological correlates of childhood apraxia of speech in Italian children. Brain Lang. 2015, 150, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.T.; Webster, R. Aaetiology of childhood apraxia of speech: A clinical practice update for paediatricians. J. Paediatr. Child. Health. 2018, 54, 1090–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, E.; Thomas, D.; McKechnie, J. Comorbid morphological disorder apparent in some children aged 4–5 years with childhood apraxia of speech: Findings from 20 tandardized testing. Clin. Linguistic Phon. 2018, 33, 42–59. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.M.; Benchek, P.; Miller, G.; Hall, N.B.; Menon, D.; Freebairn, L.; Tag, J.; Vick, J.; Taylor, H.G.; Lewis, B.A.; et al. Feature-driven classification reveals potential comorbid subtypes within childhood apraxia of speech. BMC Pedriat. 2020, 20, 519. [Google Scholar] [CrossRef] [PubMed]
- McNeill, B.C.; Gillon, G.T. Expressive morphosyntactic development in three children with childhood apraxia of speech. Speech Lang. Hear. 2013, 16, 9–17. [Google Scholar] [CrossRef]
- Bombonato, C.; Casalini, C.; Pecini, C.; Angelucci, G.; Vicari, S.; Podda, I.; Cipriani, P.; Chilosia, A.M.; Menghini, D. Implicit learning in children with Childhood Apraxia of Speech. Res. Dev. Disabil. 2022, 122, 104170. [Google Scholar] [CrossRef]
- Cleaton, M.A.M.; Kirby, A. How do we find it so hard to calculate the burden of neurodevelopmental disorders? J. Child. Dev. Disord. 2018, 4, 10. [Google Scholar]
- Nijland, L.; Terband, H.; Maassen, B. Cognitive Functions in Childhood Apraxia of Speech. J. Speech Lang. Hear. Res. 2015, 58, 550–565. [Google Scholar] [CrossRef]
- Carrigg, B.; Parry, L.; Shriberg, L.D.; Ballard, K.J. Cognitive, linguistic and motor abilities in a multigenerational family with Childhood Apraxia of Speech. Arch. Clin. Neuropsych. 2016, 31, 1006–1025. [Google Scholar] [CrossRef] [Green Version]
- Henderson, S.E.; Sugden, D.A.; Barnett, A. Movement Assessment Battery for Children, 2nd ed.; Movement ABC-2; Harcourt Assessment: London, UK, 2007. [Google Scholar]
- American Psychiatric Association—APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Database of Genomic Variants (DGV). Available online: http://dgv.tcag.ca/dgv/app/home (accessed on 26 July 2020).
- Kearney, H.M.; Thorland, E.C.; Brown, K.K.; Quintero-Rivera, F.; South, S.T.; Working Group of the American College of Medical Genetics Laboratory Quality Assurance Committee. American College of Medical Genetics standards and guidelines for interpretation and reporting of postnatal constitutional copy number variants. Genet. Med. 2011, 13, 680–685. [Google Scholar] [CrossRef] [Green Version]
- Online Mendelian Inheritance in Man (OMIM) Database. Available online: https://www.omim.org (accessed on 26 July 2020).
- Simons Foundation Autism Research Initiative (SFARI) Gene Database. Available online: https://gene.sfari.org/database/human-gene (accessed on 26 July 2020).
- O’Roak, B.J.; Vives, L.; Girirajan, S.; Karakoc, E.; Krumm, N.; Coe, B.P.; Levy, R.; Ko, A.; Lee, C.; Smith, J.D.; et al. Sporadic autism exomes reveal a highly interconnected protein network of de novo mutations. Nature 2012, 485, 246–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, H.; Kahrizi, K.; Musante, L.; Fattahi, Z.; Herwig, R.; Hosseini, M.; Oppitz, C.; Abedini, S.S.; Suckow, V.; Larti, F.; et al. Genetics of intellectual disability in consanguineous families. Mol. Psychiatry 2019, 24, 1027–1039. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zou, M.; Pang, X.; Liang, S.; Sun, C.; Wang, J.; Fan, L.; Xia, W.; Wu, L. The association between NCAM1 levels and behavioral phenotypes in children with autism spectrum disorder. Behav. Brain Res. 2019, 359, 234–238. [Google Scholar] [CrossRef]
- Lewis, B.A.; Short, E.J.; Iyengar, S.K.; Taylor, H.G.; Freebairn, L.; Tag, J.; Avrich, A.A.; Stein, C.M. Speech-sound disorders and attention deficit/hyperactivity disorder symptoms. Top Lang. Disord. 2012, 32, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Zwicker, J.C.; Missiuna, C.; Harris, S.R.; Boyd, L.A. Developmental coordination disorder: A review and update. Eur. J. Paediatr. Neurol. 2012, 16, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Vissher, C.; Houwen, S.; Scherder, E.J.A.; Moolenaar, B.; Hartman, E. Motor profile of children with developmental speech and language disorders. Paediatrics 2007, 120, e158–e163. [Google Scholar] [CrossRef]
- Tükel, Ş.; Björelius, H.; Henningsson, G.; McAllister, A.; Eliasson, A.C. Motor functions and adaptive behaviour in children with childhood apraxia of speech. Int. J. Speech Lang. Pathol. 2015, 17, 470–480. [Google Scholar] [CrossRef]
- Peter, B.; Button, L.; Stoel-Gammon, C.; Chapman, K.; Raskind, W.H. Deficits in sequential processing manifest in motor and linguistic tasks in a multigenerational family with childhood apraxia of speech. Clin. Linguistic Phon. 2013, 27, 163–191. [Google Scholar] [CrossRef] [Green Version]
- Button, L.; Peter, B.; Stoel-Gammon, C.; Raskind, W.H. Associations among measures of sequential processing in motor and linguistics tasks in adults with and without a family history of childhood apraxia of speech: A replication study. Clin. Linguist. Phon. 2013, 27, 192–212. [Google Scholar] [CrossRef] [Green Version]
- Peter, B.; Lancaster, H.; Vose, C.; Middleton, K.; Stoel-Gammon, C. Sequential processing deficit as a shared persisting biomarker in dyslexia and childhood apraxia of speech. Clin. Linguist. Phon. 2018, 32, 316–346. [Google Scholar] [CrossRef]
- Peter, B.; Raskind, W.H. A multigenerational family study of oral and hand motor sequencing ability provide evidence for a familial speech sound disorder subtype. Top. Lang. Disord. 2011, 31, 145–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iuzzini-Seigel, J. Motor performance in children with childhood apraxia of speech and speech sound disorders. J. Speech Lang. Hear. Res. 2019, 62, 3220–3233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iuzzini-Seigel, J.; Hogan, T.P.; Green, J.R. Speech inconsistency in children with childhood apraxia of speech, language impairment, and speech delay: Depends on the stimuli. J. Speech Lang. Hear. Res. 2017, 60, 1194–1210. [Google Scholar] [CrossRef] [PubMed]
- Case, J.; Grigos, M.I. Articulatory control in childhood apraxia of speech in a novel word-learning task. J. Speech Lang. Hear. Res. 2016, 59, 1253–1268. [Google Scholar] [CrossRef] [PubMed]
- Grigos, M.I.; Moss, A.; Lu, Y. Oral articulatory control in childhood apraxia of speech. J. Speech Lang. Hear. Res. 2015, 58, 1103–1118. [Google Scholar] [CrossRef] [Green Version]
- Highman, C.; Leitão, S.; Hennessey, N.; Piek, J. Prelinguistic communication development in children with childhood apraxia of speech: A retrospective analysis. Int. J. Speech Lang. Pathol. 2012, 14, 35–47. [Google Scholar] [CrossRef]
- Highman, C.; Hennessey, N.W.; Leitão, S.; Piek, J.P. Early development of children at risk for childhood apraxia of speech: A longitudinal investigation. Dev. Neuropsychol. 2013, 38, 197–210. [Google Scholar] [CrossRef]
- Overby, M.S.; Caspari, S.S.; Schreiber, J. Volubility, consonant emergence, and syllabic structure in infants and toddlers later diagnosed with childhood apraxia of speech, speech sound disorder, and typical development: A retrospective video analysis. J. Speech Lang. Hear. Res. 2019, 62, 1657–1675. [Google Scholar] [CrossRef]
- Nip, I.S.B.; Green, J.R.; Marx, D.B. The coemergence of cognition, language, and speech motor control in early development: A longitudinal correlation study. J. Commun Disord. 2011, 44, 149–160. [Google Scholar] [CrossRef] [Green Version]
- Terband, H.; Maassen, B. Speech motor development in childhood apraxia of speech: Generating testable hypotheses by neurocomputational modeling. Folia Phoniatr. Logop. 2010, 62, 134–142. [Google Scholar] [CrossRef]
- Kuhl, P.K. Brain mechanisms in early language acquisition. Neuron 2010, 67, 713–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baylis, A.L.; Shriberg, L.D. Estimates of the prevalence of speech and motor speech disorders in youth with 22q11.2 deletion syndrome. Am. J. Speech Lang. Pathol. 2019, 28, 53–82. [Google Scholar] [CrossRef] [PubMed]
- Brazil, A.; Stanford, K.; Smolarek, T.; Hopkin, R. Delineating the phenotype of 1p36 deletion in adolescents and adults. Am. J. Med. Genet. A. 2014, 164A, 2496–2503. [Google Scholar] [CrossRef] [PubMed]
- Mefford, H.C.; Mitchell, E.; Hodge, J. 17q12 Recurrent Duplication. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Mirzaa, G., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2015; pp. 1993–2021. [Google Scholar]
- Van Bon, B.W.M.; Mefford, H.C.; de Vries, B.B.A. 15q13.3 Microdeletion. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Mirzaa, G., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2010; pp. 1993–2021, updated 2015. [Google Scholar]
- Centanni, T.M.; Sanmann, J.N.; Green, J.R.; Iuzzini-Seigel, J.; Bartlett, C.; Sanger, W.G.; Hogan, T.P. The role of candidate-gene CNTNAP2 in childhood apraxia of speech and specific language impairment. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2015, 168, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Kadis, D.S.; Goshulak, D.; Namasivayam, A.; Pukonen, M.; Kroll, R.; De Nil, L.F.; Pang, E.W.; Lerch, J.P. Cortical thickness in children receiving intensive therapy for idiopathic apraxia of speech. Brain Topogr. 2014, 27, 240–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiori, S.; Guzzetta, A.; Mitra, J.; Pannek, K.; Pasquariello, R.; Cipriani, P.; Tosetti, M.; Cioni, G.; Rose, S.E.; Chilosi, A.M. Neuroanatomical correlates of childhood apraxia of speech: A connectomic approach. Neuroimage Clin. 2016, 12, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Conti, E.; Retico, A.; Palumbo, L.; Spera, L.; Bosco, P.; Biagi, L.; Fiori, S.; Tosetti, M.; Cipriani, P.; Cioni, G.; et al. Autism Spectrum Disorder and Childhood Apraxia of Speech: Early language-related hallmarks across structural MRI study. J. Pers Med. 2020, 10, 275. [Google Scholar] [CrossRef]
- Liégeois, F.J.; Turner, S.J.; Mayes, A.; Bonthrone, A.F.; Boys, A.; Smith, L.; Parry-Fielde, B.; Mandelstam, S.; Spencer-Smith, M.; Bahlo, M.; et al. Dorsal language stream anomalies in an inherited speech disorder. Brain 2019, 142, 966–977. [Google Scholar] [CrossRef]

{kind=link}
| GENERAL CLINICAL CHARACTERISTICS | CAS-LI (n. 52) | CAS-LI + CND (n. 54) | |
|---|---|---|---|
| Males:Females ratio | 42:10 (4:1) | 45:9 (5:1) | p = 0.731 |
| Positive Familial History | 37/50 * (74%) | 28 (52%) | χ2 = 5.434 p = 0.020 |
| Nonverbal IQ | 102.10 ± 15.77 | 79.66 ± 20.97 | p < 0.001 |
| Motor delay | 12 (24%) | 26 (48.2%) | χ2 = 6.529 p = 0.011 |
| Abnormal babbling | 40 (78.4%) | 48 (90.6%) | χ2 = 2.940 p = 0.086 |
| Age at first words | 21.6 ± 9.9 | 25.9 ± 13.12 | t = −1.821 p = 0.072 |
| COMORBIDITIES (n. of children and percentage) | |||
| DCD | - | 22 (41%) | |
| ID | - | 22 (41%) | |
| ADHD | - | 7 (13%) | |
| ASD | - | 3 (6%) | |
| BRAIN MRI | |||
| Normal or minor anomalies | 48 (92%) | 51 (94%) | χ2 = 0.196 p = 0.658 |
| Structural abnormalities | 4 (8%) | 3 (6%) | |
| CMA | |||
| w-CNVs | 38 (73%) | 27 (50%) | χ2 = 6.272 p = 0.043 |
| N-CNVs | 6 (11.5%) | 9 (16.7%) | |
| C-CNVs | 8 (15.5 %) | 18 (33.35%) | |
| SPEECH | |||
| Phonetic inventory (n. of consonants) | 12.2 ± 5.1 | 11.2 ± 4.6 | t = 1.021 p = 0.310 |
| Inaccuracy (% on productions) | 65.02 ± 30.70 | 73.65 ± 25.69 | t = −1.577 p = 0.119 |
| Inconsistency (% on productions) | 38.62 ± 28.91 | 46.35 ± 27.07 | t = −1.367 p = 0.175 |
| DDK3 (n. of trisyllabic sequences repetitions) | 10 [0–14] | 9 [0–13] | Z = 1.047 p = 0.295 |
| Intelligibility score (range 0–5) | 2.52 ± 0.96 | 2.56 ± 0.86 | p = 0.619 |
| Syllable omissions in words (%) | 28.10 ± 33.58 Median 17 | 45.25 ± 42.11 Median 32 | p = 0.062 |
| Speech Composite Severity Score (range: 0–6) | 5.01 ± 1.14 | 5.29 ± 0.90 | t = −1.385 p = 0.273 |
| LANGUAGE | |||
| Receptive vocabulary (% of subjects with deficient performance) | 12/51 (23.5%) ** | 24 (44.4%) | χ2 = 5.092 p = 0.024 |
| Expressive vocabulary (% of subjects with deficient performance) | 24 (46.1%) | 38 (70.4%) | χ2 = 6.399 p = 0.011 |
| Receptive grammar (% of subjects with deficient performance) | 11 (21.1%) | 29/53 (54.7%) ** | p < 0.001 |
| Complexity of expressive grammar (% of subjects with deficient performance) | 48 (92.3%) | 51 (94.4%) | p = 0.658 |
| Language Composite Severity score (range: 0–4) | 2.60 ± 0.93 | 3.27 ± 0.95 | t = 3.567 p < 0.001 |
| Patient n. | Chromosome | CMA Findings (hg19) | Size (bp) | Inheritance | Candidate Genes/Loci (Reference) | Disorder |
|---|---|---|---|---|---|---|
| 1 | 11 | 11p13 deletion | 643,641 | de novo | CAPRIN1 [36] | CAS-LI |
| 2 | 4 | 4q31.1duplication | 331,420 | maternal | LRBA [36] | CAS-LI + CND (ID) |
| 3 | 16 | 16p13.2 duplication | 220,893 | paternal | ABAT [36] | CAS-LI + CND (ID) |
| 16 | 16q23.1 deletion | 72,365 | maternal | WWOX [36] | ||
| 4 | 8 | 8p23.1 duplication | 366,866 | paternal | TNKS [37] | CAS-LI + CND (ID) |
| 5 | 1 | 1p34.1 duplication | 393,673 | paternal | IPP [38] | CAS-LI + CND(ASD) |
| 6 | 11 | 11q23.2 duplication | 273,131 | maternal | NCAM1 [39] | CAS-LI + CND (ADHD) |
| 7 | X | Xp11.4 duplication | 106,971 | maternal | ATP6AP2 [MIM 300423] | CAS-LI + CND (ASD) |
| 8 | 17 | 17q12 duplication | 1,261,947 | paternal | Chromosome 17q12 duplication syndrome [MIM 614526] | CAS-LI |
| 9 | 15 | 15q13.2q13.3 deletion | 1,496,355 | unknown | Chromosome 15q13 deletion syndrome [MIM 612001] | CAS-LI |
| 10 | 7 | 7q35 duplication | 1350 | maternal | CNTNAP2 [36] | CAS-LI + CND (ADHD) |
| 11 | 16 | 16p11.2 deletion | 524,646 | de novo | Chromosome 16p11.2 deletion syndrome [MIM* 611913] | CAS-LI + CND(DCD) |
| 12 | 16 | 16p11.2 deletion | 446,165 | paternal | Chromosome 16p11.2 deletion syndrome [MIM * 611913] | CAS-LI + CND (ADHD) |
| 13 | 6 | 6q21 deletion | 1,432,328 | unknown | 6q21 deletion | CAS-LI |
| 14 | X | Xq13.3 duplication | 18,2919 | maternal | ZDHHC15 [MIM * 300577] | CAS-LI + CND (ADHD) |
| 15 | 16 | 16p11.2 deletion | 545,601 | de novo | Chromosome 16p11.2 deletion syndrome [MIM * 611913] | CAS-LI |
| 16 | 16 | 16p11.2 deletion | 524,999 | unknown | Chromosome 16p11.2 deletion syndrome [MIM * 611913] | CAS-LI |
| 17 | 7 | 7q11.23 duplication | 1,400,000 | de novo | Chromosome 7q11 duplication syndrome [MIM * 609757] | CAS-LI |
| 18 | 4 | 4q25q26 deletion | 5,343,965 | de novo | 5.3 Mbp deletion | CAS-LI |
| 19 | 3 | 3p25.3p26.3 duplication | 10,184,886 | de novo | 10 Mbp duplication, resulting from an unbalanced translocation | CAS-LI + CND(ID) |
| 21 | 21q22.3 deletion | 3,006,682 | de novo | 3 Mbp deletion, resulting from an unbalanced translocation | ||
| 20 | 1 | 1p36 deletion | NA | de novo | Chromosome 1p36 deletion syndrome [MIM * 607872] | CAS-LI + CND(ID) |
| 21 | 4 | 4q35.1q35.2 deletion | 5,745,530 | de novo | 5.7 Mbp deletion, resulting from an unbalanced translocation | CAS-LI + CND (ID) |
| 9 | 9p24.3p22.1 duplication | 18,355 | de novo | 18 Mbp duplication, resulting from an unbalanced translocation | ||
| 22 | 2 | 2p16.3 deletion | 373,326 | de novo | FBXO11 [MIM * 618089] | CAS-LI + CND(ID) |
| 23 | 22 | 22q11.21 deletion | 1,936,872 | unknown | Chromosome 22q11.2 deletion syndrome [MIM * 188400] | CAS-LI + CND(DCD) |
| 24 | 16 | 16p13.11 duplication | 1144392 | unknown | NDE1 [MIM * 614019] | CAS-LI + CND (ID) |
| 25 | 3 | 3q29 deletion | 1,532,486 | paternal | Chromosome 3q29 microdeletion syndrome [MIM * 609425] | CAS-LI + CND (DCD) |
| 26 | 16 | 16p11.2 deletion | 445,805 | de novo | Chromosome 16p11.2 deletion syndrome [MIM * 611913] | CAS-LI + CND(DCD) |
| CAS-LI | Nonverbal IQ | Age | Age at First Words | Expressive Grammar | Language Composite Severity Score | Phonetic Inventory | Inconsistency | Inaccuracy | Syllable Omissions | DDK3 | Intelligibility |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Nonverbal IQ | — | ||||||||||
| Age | 0.157 | — | |||||||||
| Age at first words | −0.054 | 0.073 | — | ||||||||
| Expressive Grammar | 0.235 | 0.427 ** | −0.223 | — | |||||||
| Language Composite Severity Score | −0.363 * | −0.003 | 0.124 | −0.477 *** | — | ||||||
| Phonetic Inventory | 0.197 | 0.462 *** | −0.292 * | 0.714 *** | −0.301 * | — | |||||
| Inconsistency | −0.235 | −0.247 | 0.117 | −0.306 * | 0.167 | −0.418 ** | — | ||||
| Inaccuracy | −0.384 ** | −0.503 *** | 0.164 | −0.525 *** | 0.322 * | −0.618 *** | 0.611 *** | — | |||
| Syllable Omissions | −0.297 * | −0.333 * | 0.302 * | −0.718 *** | 0.459 ** | −0.720 *** | 0.634 *** | 0.675 *** | — | ||
| DDK3 | 0.360 * | 0.475 *** | −0.146 | 0.510 *** | −0.329 * | 0.525 *** | −0.435 ** | −0.596 *** | −0.634 *** | — | |
| Intelligibility | 0.201 | 0.268 | −0.015 | 0.433 ** | −0.114 | 0.461 *** | −0.234 | −0.287 * | −0.386 ** | 0.439 ** | — |
| Speech Composite Severity Score | −0.103 | −0.349 * | 0.22 | −0.619 *** | 0.364 ** | −0.714 *** | 0.431 ** | 0.591 *** | 0.730 *** | −0.634 *** | −0.380 ** |
| Nonverbal IQ | — | ||||||||||
| Age | −0.309 * | — | |||||||||
| Age at first words | 0.004 | 0.211 | — | ||||||||
| Expressive Grammar | 0.317 * | 0.19 | 0.219 | — | |||||||
| Language Composite Severity Score | −0.462 *** | 0.024 | −0.07 | −0.499 *** | — | ||||||
| Phonetic Inventory | 0.237 | 0.242 | 0.096 | 0.536 *** | −0.227 | — | |||||
| Inconsistency | −0.168 | −0.082 | 0.064 | −0.410 ** | 0.357 * | −0.400 ** | — | ||||
| Inaccuracy | −0.245 | −0.185 | −0.012 | −0.578 *** | 0.409 ** | −0.649 *** | 0.590 *** | — | |||
| Syllable Omissions | −0.226 | −0.135 | −0.051 | −0.560 *** | 0.469 ** | −0.472 ** | 0.720 *** | 0.830 *** | — | ||
| DDK3 | 0.410 ** | 0.261 | 0.008 | 0.630 *** | −0.476 *** | 0.468 *** | −0.495 *** | −0.649 *** | −0.764 *** | — | |
| Intelligibility | −0.027 | 0.145 | −0.029 | 0.226 | 0.064 | 0.436 ** | −0.171 | −0.361 ** | −0.190 | 0.232 | — |
| Speech Composite Severity Score | −0.106 | −0.089 | 0.236 | −0.401 ** | 0.081 | −0.509 *** | 0.632 *** | 0.653 *** | 0.747 *** | −0.498 *** | −0.500 *** |
| Cluster 1 (n = 65) | Cluster 2 (n = 41) | p-Value | |
|---|---|---|---|
| CLINICAL SUBGROUPS | |||
| CAS-LI | 46 (88.5%) | 6 (11.5%) | <0.001 |
| CAS-LI + CND | 19 (34.2%) | 35 (64.8%) | |
| COMORBID DISORDERS LI-only | 46 (70.8%) | 6 (14.6%) | <0.001 |
| ADHD | 5 (7.7%) | 2 (4.9%) | 0.704 |
| ASD | 1 (1.5%) | 2 (4.7%) | 0.558 |
| ID | 2 (3.1%) | 20 (48.8%) | <0.001 |
| DCD | 11 (16.9%) | 11 (26.8%) | 0.328 |
| BRAIN MRI | |||
| Normal | 61 (93.8%) | 38 (92.7%) | 1 |
| Abnormal | 4 (6.2%) | 3 (7.3%) | |
| CMA | |||
| w-CNVs and N-CNVs | 51 (78.5%) | 30 (73.2%) | 0.687 |
| C-CNVs | 14 (21.5%) | 11 (26.8%) | |
| AGE | 75.9 ± 25.7 | 81.1±28.6 | 0.352 |
| GENDER | |||
| Male | 55 (84.6%) | 32 (78%) | 0.55 |
| Female | 10 (15.4%) | 9 (22%) | |
| FAMILY HISTORY | |||
| No | 19 (29.7%) | 20 (50%) | 0.061 |
| Yes | 45 (70.3%) | 20 (50%) | |
| GROSS MOTOR DELAY | |||
| No | 51 (81%) | 15 (36.6%) | <0.001 |
| Yes | 12 (19%) | 26 (63.4%) | |
| BABBLING | |||
| Normal | 13 (20.7%) | 3 (7.5%) | 0.159 |
| Atypical | 51 (79.7%) | 37 (92.5%) | |
| FIRST WORDS (age in months) | 21.7 ± 10 | 27.1 ± 13.7 | 0.046 |
| LANGUAGE | |||
| Receptive Vocabulary | |||
| Normal | 56 (87.5%) | 13 (31.7%) | <0.001 |
| Deficient | 8 (12.5%) | 28 (68.3%) | |
| Expressive Vocabulary | |||
| Normal | 41 (63.1%) | 3 (7.3%) | <0.001 |
| Deficient | 24 (36.9%) | 38 (92.7%) | |
| Receptive Grammar | |||
| Normal | 56 (86.1%) | 9 (22.5%) | <0.001 |
| Deficient | 9 (13.9%) | 31 (77.5%) | |
| Expressive grammar | |||
| Normal | 7 (10.8%) | 0 (0%) | 0.041 |
| Deficient | 58 (89.2%) | 41 (100%) | |
| LANGUAGE COMPOSITE SEVERITY SCORE | 2.5 ± 0.9 | 3.7 ± 0.4 | <0.001 |
| SPEECH | |||
| Phonetic Inventory | 12.7 ± 4.9 | 10±4.5 | 0.005 |
| Inconsistency | 32.5 (15–46) | 44.5 (34.5–67.5) | 0.008 |
| Inaccuracy | 62.9 ± 29.9 | 79.8 ± 22.8 | 0.001 |
| Syllable Omissions | 13 (0–32) | 43 (14.3–97.5) | <0.001 |
| DDK3 | 11.5 (0–15) | 0 (0–10.25) | 0.002 |
| Intelligibility | 2.6 ± 0.9 | 2.5 ± 0.8 | 0.859 |
| SPEECH COMPOSITE SEVERITY SCORE | 5.0 ± 1.2 | 5.4 ± 0.7 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chilosi, A.M.; Podda, I.; Ricca, I.; Comparini, A.; Franchi, B.; Fiori, S.; Pasquariello, R.; Casalini, C.; Cipriani, P.; Santorelli, F.M. Differences and Commonalities in Children with Childhood Apraxia of Speech and Comorbid Neurodevelopmental Disorders: A Multidimensional Perspective. J. Pers. Med. 2022, 12, 313. https://doi.org/10.3390/jpm12020313
Chilosi AM, Podda I, Ricca I, Comparini A, Franchi B, Fiori S, Pasquariello R, Casalini C, Cipriani P, Santorelli FM. Differences and Commonalities in Children with Childhood Apraxia of Speech and Comorbid Neurodevelopmental Disorders: A Multidimensional Perspective. Journal of Personalized Medicine. 2022; 12(2):313. https://doi.org/10.3390/jpm12020313
Chicago/Turabian StyleChilosi, Anna Maria, Irina Podda, Ivana Ricca, Alessandro Comparini, Beatrice Franchi, Simona Fiori, Rosa Pasquariello, Claudia Casalini, Paola Cipriani, and Filippo Maria Santorelli. 2022. "Differences and Commonalities in Children with Childhood Apraxia of Speech and Comorbid Neurodevelopmental Disorders: A Multidimensional Perspective" Journal of Personalized Medicine 12, no. 2: 313. https://doi.org/10.3390/jpm12020313
APA StyleChilosi, A. M., Podda, I., Ricca, I., Comparini, A., Franchi, B., Fiori, S., Pasquariello, R., Casalini, C., Cipriani, P., & Santorelli, F. M. (2022). Differences and Commonalities in Children with Childhood Apraxia of Speech and Comorbid Neurodevelopmental Disorders: A Multidimensional Perspective. Journal of Personalized Medicine, 12(2), 313. https://doi.org/10.3390/jpm12020313