
CRIDECO Anticholinergic Load Scale: An Updated Anticholinergic Burden Scale. Comparison with the ACB Scale in Spanish Individuals with Subjective Memory Complaints

 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
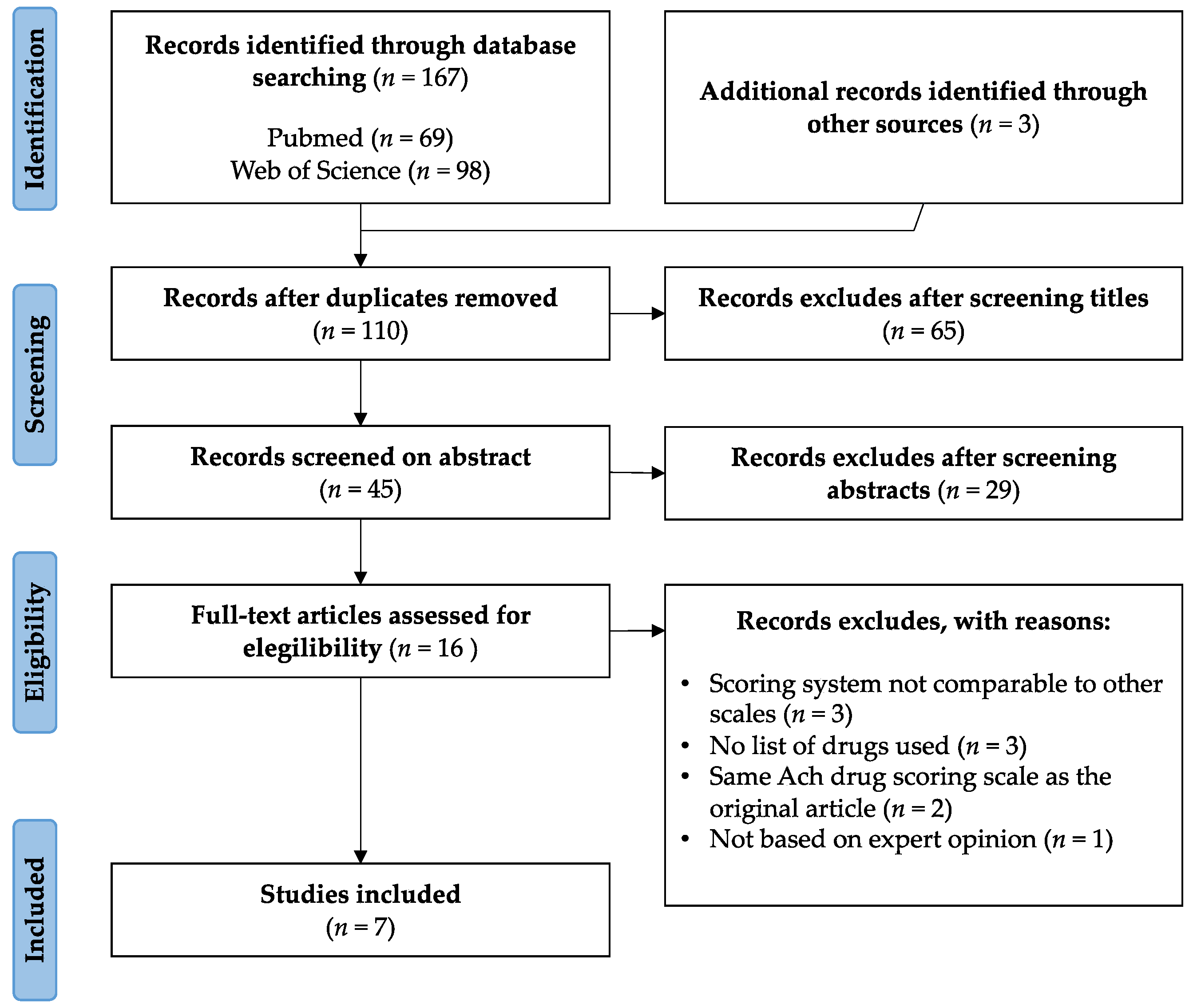
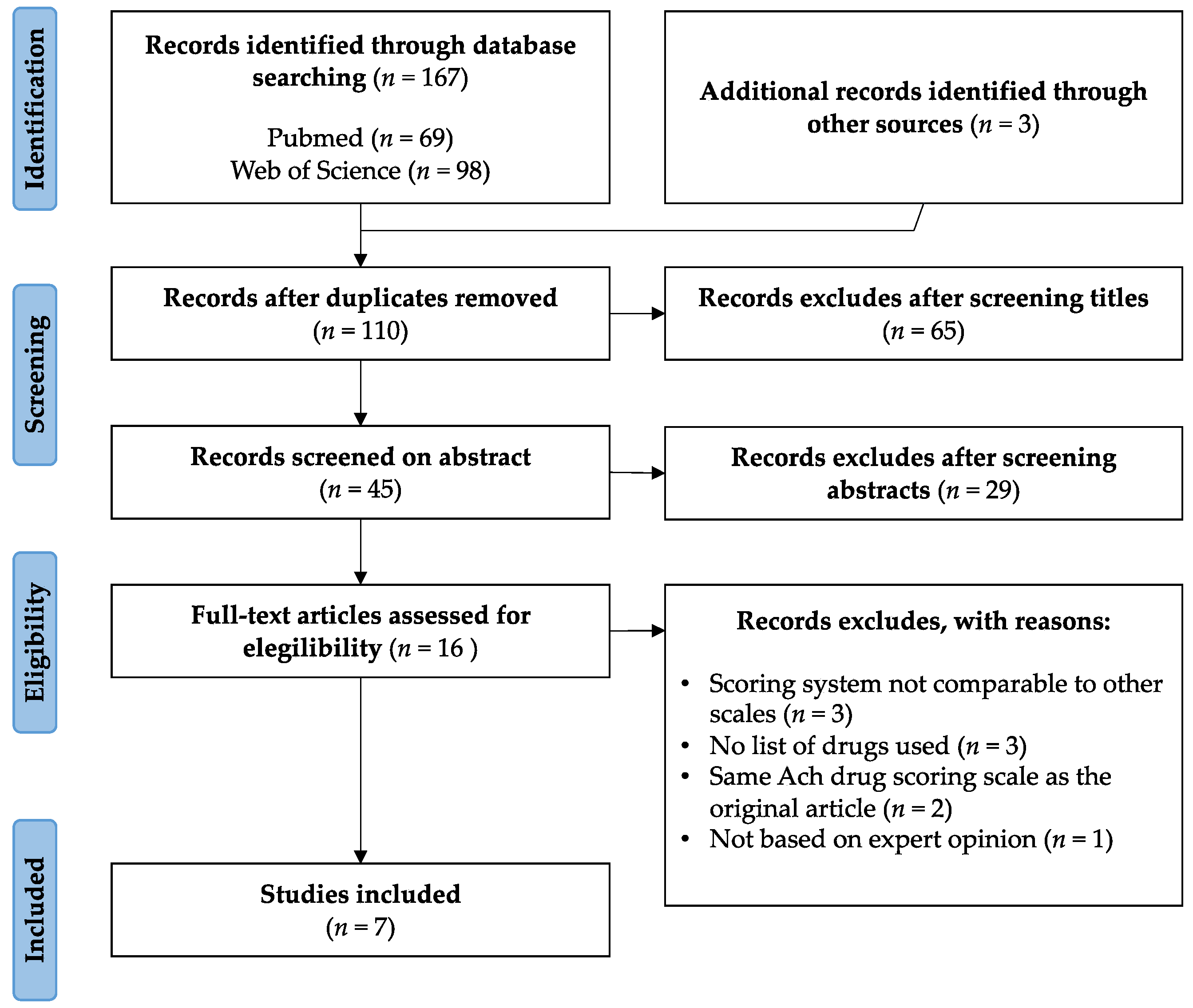
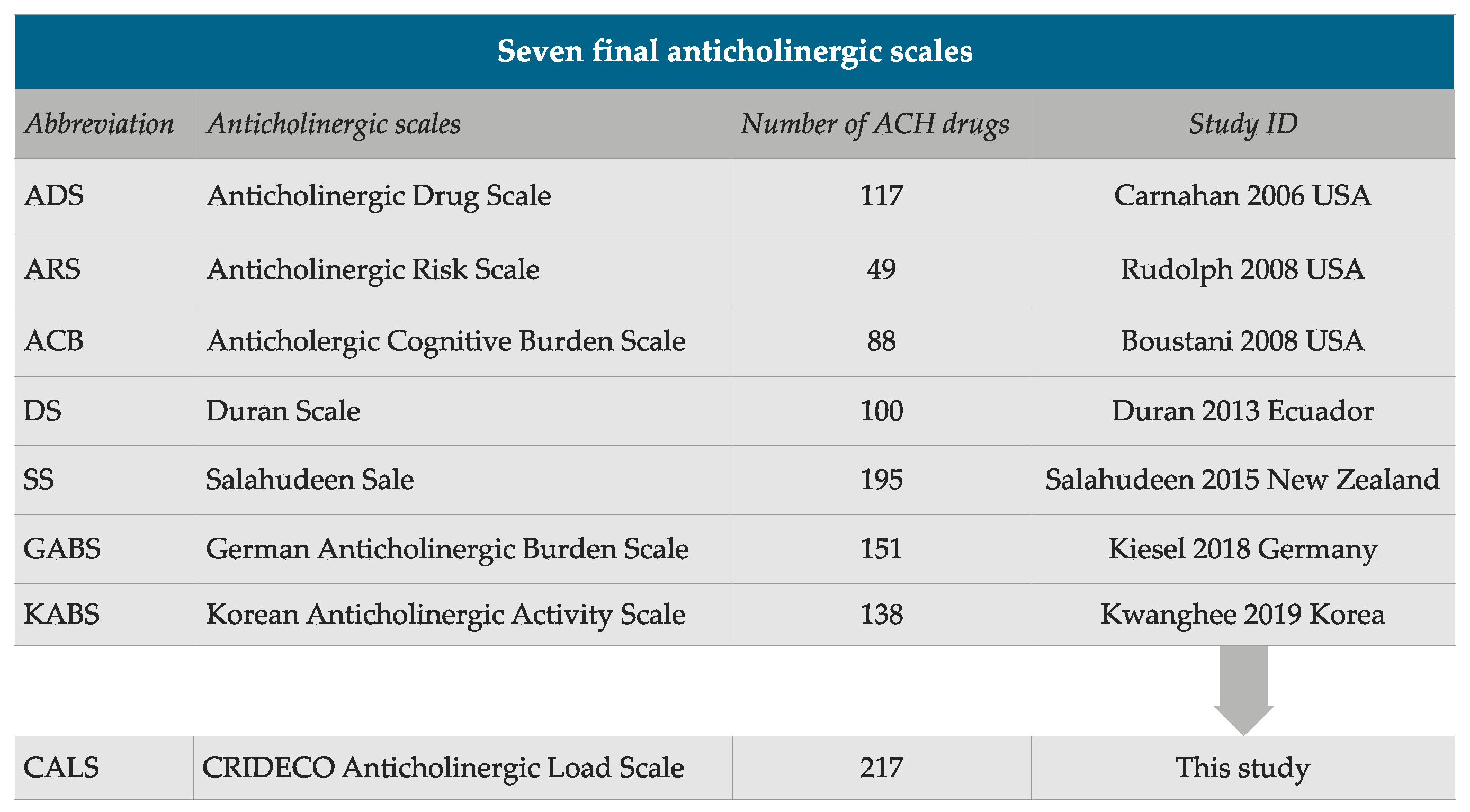
2.1. Systematic Review
2.2. Development of a New Anticholinergic Burden Scale
2.3. Subject Recruitment and Data Collection
2.4. Cognitive Impairment Assessment
2.4.1. Memory Impairment Screen
2.4.2. Short Portable Mental State Questionnaire (Spanish Version)
2.4.3. Semantic Verbal Fluency
2.5. Statistical Treatment
3. Results
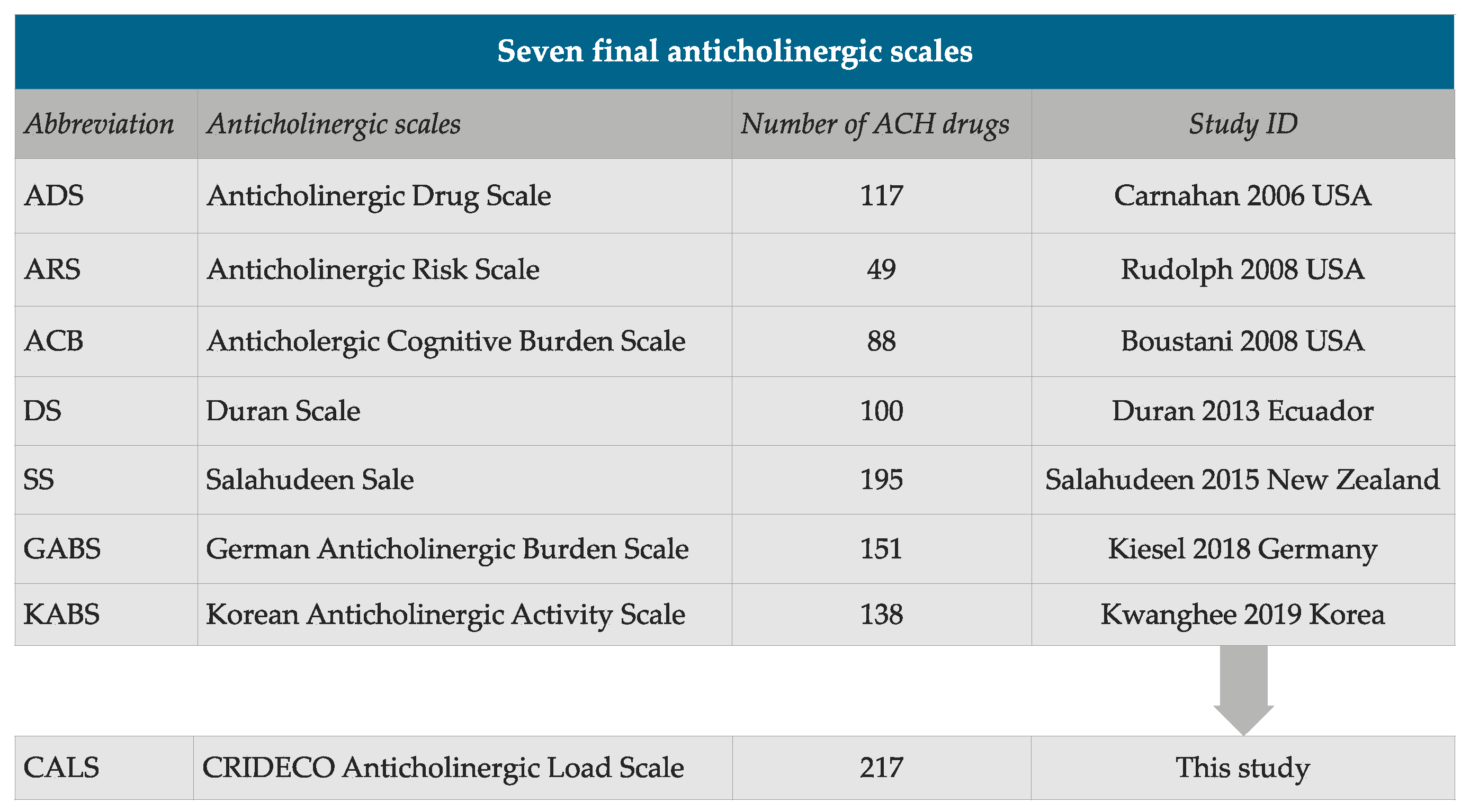
3.1. CRIDECO Anticholinergic Load Scale

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Potency (Score 1) | Medium Potency (Score 2) | High Potency (Score 3) | ||||
|---|---|---|---|---|---|---|
| Aclidinium inh | Cyclosporine | Iloperidone | Phenobarbital | Amantadine | Acepromazine | Hyoscyamine |
| Alimemazine * | Desloratadine | Ipratropium inh | Piperacillin | Baclofen | Amitriptyline | Imipramine |
| Alprazolam | Desvelanfaxine | Isosorbide mononitrate | Pramipexole | Carbamazepine | Amoxapine | Levomepromazine * |
| Alverine | Dexamethasone | Isosorbide dinitrate | Prednisolone | Cloperastine | Atropine | Meclozine * |
| Amisulpride | Dextromethorphan | Ketorolac | Prednisone | Cimetidine | Belladonna | Mequitazine |
| Ampicillin | Diazepam | Ketotifen | Pridinol | Cyclobenzaprine | Benzatropine* | Nortriptyline |
| Aripiprazole | Digitoxin | Levocetirizine | Pseudoephedrine | Dosulepin | Biperiden | Opipramol |
| Asenapine | Digoxin | Levodopa-carbidopa | Quinidine | Fluphenazine | Brompheniramine | Orphenadrine |
| Atenolol | Diltiazem | Lithium | Risperidone | Loxapine | Carbinoxamine | Otilonium bromide |
| Azathioprine | Dipyridamole | Loperamide | Rotigotine patch | Maprotiline | Carisoprodol | Oxybutynin |
| Benazepril | Disopyramide | Loratadine | Selegiline | Meperidine * | Chlorphenamine * | Pheniramine |
| Betaxolol | Domperidone | Lorazepam | Sertraline | Methadone | Chlorpromazine | Procyclidine |
| Bisacodyl | Entacapone | Lumiracoxib | Sumatriptan | Molindone | Chlorprothixene | Promethazine |
| Bromocriptine | Escitalopram | Mebeverine | Tapentadol | Nefopam | Cimetropium bromide | Propantheline |
| Bromperidol | Estazolam | Metformin | Temazepam | Olanzapine | Clemastine | Propiverine |
| Bupropion | Famotidine | Methocarbamol | Theophylline | Oxcarbazepine | Clomipramine | Protriptyline |
| Captopril | Fentanyl | Methotrexate | Tiotixene | Paroxetine | Clozapine | Pyrilamine * |
| Cefamandole | Fexofenadine | Methylprednisolone | Tiotropium inh | Perphenazine | Cyproheptadine | Scopolamine * |
| Cefoxitin | Flunitrazepam | Metoclopramide | Trandolapril | Pimozide | Darifenacin | Solifenacin |
| Celecoxib | Flupentixol | Metoprolol | Trazodone | Prochlorperazine | Desipramine | Thioridazine |
| Cephalothin | Fluoxetine | Midazolam | Triamcinolone | Promazine | Dexbrompheniramine | Tiemonium iodide |
| Cetirizine | Flurazepam | Mirtazapine | Triamterene | Propoxyphene | Dexchlorpheniramine | Timepidium bromide |
| Cinnarizine | Fluvoxamine | Morphine | Trimebutine | Quetiapine | Dicyclomine * | Tizanidine |
| Chlordiazepoxide | Furosemide | Naratriptan | Triazolam | Ranitidine | Difemerine | Tolterodine |
| Chlortalidone | Gentamicin | Nefazodone | Umeclidinium inh | Tramadol | Diphenhydramine * | Trifluoperazine |
| Citalopram | Glycopyrronium inh | Nifedipine | Valproic acid | Triprolidine | Doxepin | Trihexyphenidyl |
| Clindamycin | Guaifenesin | Nizatidine | Vancomycin | Zotepine | Doxylamine | Trimipramine |
| Clonazepam | Haloperidol | Oxazepam | Venlafaxine | Zuclopenthixol | Emepronium | Tropatepine |
| Clorazepate | Hydralazine | Oxycodone | Warfarin | Fesoterodine | Trospium | |
| Codeine | Hydrocodone | Paliperidone | Ziprasidone | Flavoxate | Valethamate | |
| Cortisone | Hydrocortisone | Pancuronium | Zolmitriptan | Homatropine | ||
| Cycloserine | Hydromorphone | Phenelzine | Hydroxyzine | |||
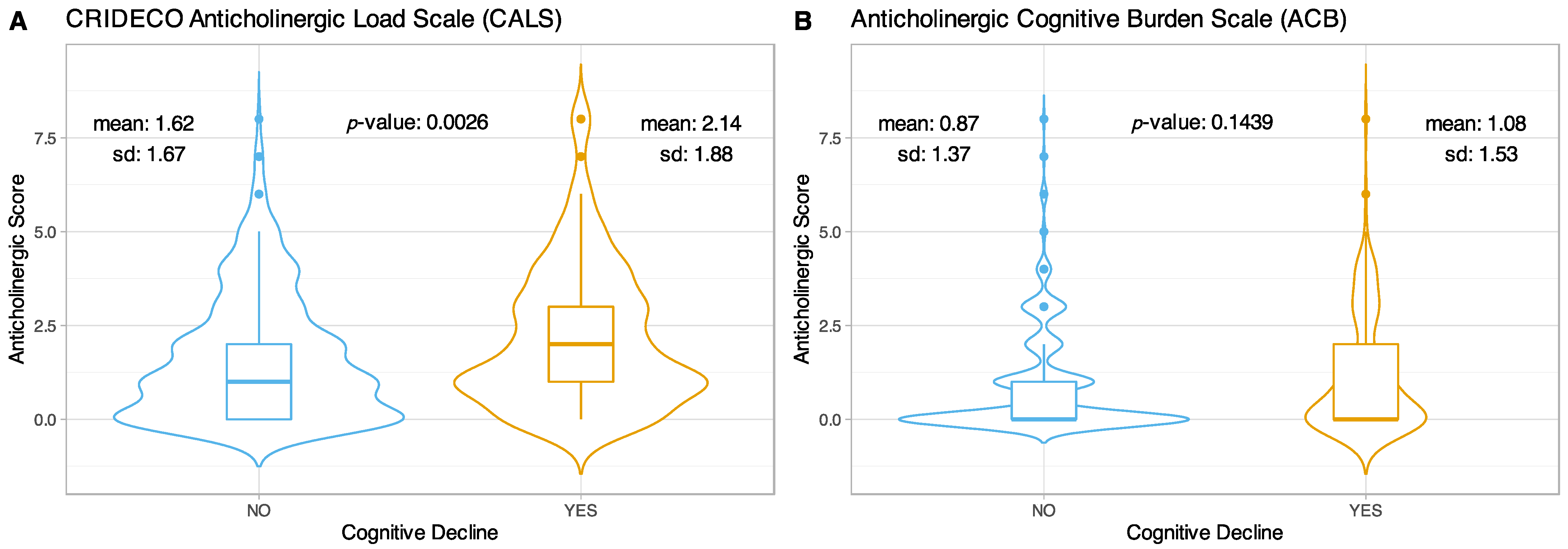
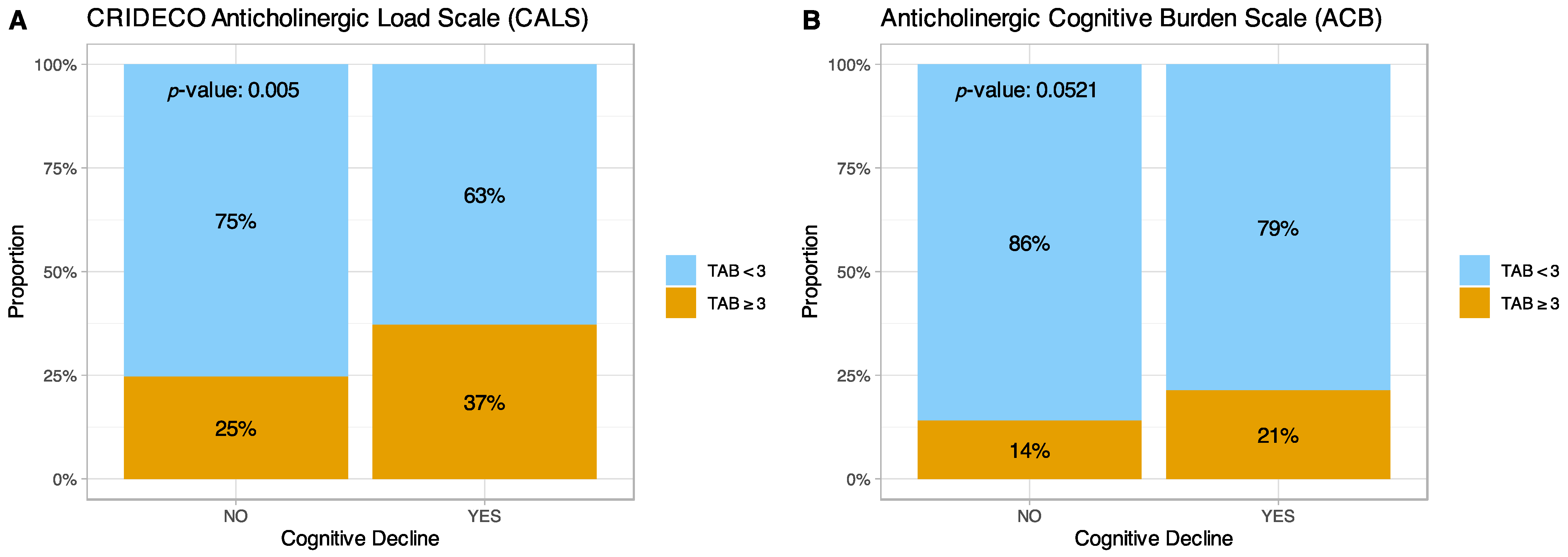
3.2. Comparison with the ACB and CALS Scale in Individuals with Subjective Memory Complaints
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Life Expectancy at Birth (Years). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/life-expectancy-at-birth-(years) (accessed on 12 November 2021).
- Gutiérrez-Valencia, M.; Herce, P.A.; Lacalle-Fabo, E.; Escámez, B.C.; Cedeno-Veloz, B.; Martínez-Velilla, N. Prevalence of polypharmacy and associated factors in older adults in Spain: Data from the National Health Survey 2017. Med. Clin. 2019, 153, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Nanji, K.; Mujeeb, R.; Patel, M.J. Effects of polypharmacy on adverse drug reactions among geriatric outpatients at a tertiary care Hospital in Karachi: A prospective cohort study. PLoS ONE 2014, 9, e112133. [Google Scholar] [CrossRef]
- González-Bueno, J.; Sevilla-Sánchez, D.; Puigoriol-Juvanteny, E.; Molist-Brunet, N.; Codina-Jané, C.; Espaulella-Panicot, J. Factors associated with medication non-adherence among patients with multimorbidity and polypharmacy admitted to an intermediate care center. Int. J. Environ. Res. Public Health 2021, 18, 9606. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Pilotto, A.; Vaona, A.; Demurtas, J.; Mueller, C.; Huntley, J.; Crepaldi, G.; et al. Polypharmacy Is Associated With Higher Frailty Risk in Older People: An 8-Year Longitudinal Cohort Study. J. Am. Med. Dir. Assoc. 2017, 18, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Kim, S.; Sohn, H.S.; Kwon, J.W. The Association between Polypharmacy and Hip Fracture in Osteoporotic Women: A Nested Case–Control Study in South Korea. Clin. Drug Investig. 2019, 39, 63–71. [Google Scholar] [CrossRef]
- Zaninotto, P.; Huang, Y.T.; Di Gessa, G.; Abell, J.; Lassale, C.; Steptoe, A. Polypharmacy is a risk factor for hospital admission due to a fall: Evidence from the English Longitudinal Study of Ageing. BMC Public Health 2020, 20, 1804. [Google Scholar] [CrossRef]
- Grossi, C.M.; Richardson, K.; Savva, G.M.; Fox, C.; Arthur, A.; Loke, Y.K.; Steel, N.; Brayne, C.; Matthews, F.E.; Robinson, L.; et al. Increasing prevalence of anticholinergic medication use in older people in England over 20 years: Cognitive function and ageing study i and II. BMC Geriatr. 2020, 20, 267. [Google Scholar] [CrossRef]
- Nishtala, P.S.; Salahudeen, M.S.; Hilmer, S.N. Anticholinergics: Theoretical and clinical overview. Expert Opin. Drug Saf. 2016, 15, 753–768. [Google Scholar] [CrossRef]
- Tune, L.E. Anticholinergic effects of medication in elderly patients. J. Clin. Psychiatry 2001, 62, 11–14. [Google Scholar]
- Chancellor, M.B.; Staskin, D.R.; Kay, G.G.; Sandage, B.W.; Oefelein, M.G.; Tsao, J.W. Blood-brain barrier permeation and efflux exclusion of anticholinergics used in the treatment of overactive bladder. Drugs Aging 2012, 29, 259–273. [Google Scholar] [CrossRef]
- Gorup, E.; Rifel, J.; Petek Šter, M. Anticholinergic burden and most common anticholinergic-acting medicines in older general practice patients. Zdr. Varst. 2018, 57, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, O.; Gnjidic, D.; Hilmer, S.N.; Naganathan, V.; McLachlan, A.J. Investigating polypharmacy and drug burden index in hospitalised older people. Intern. Med. J. 2013, 43, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Sathienluckana, T.; Unaharassamee, W.; Suthisisang, C.; Suanchang, O.; Suansanae, T. Anticholinergic discontinuation and cognitive functions in patients with schizophrenia: A pharmacist-physician collaboration in the outpatient department. Integr. Pharm. Res. Pract. 2018, 7, 161–171. [Google Scholar] [CrossRef] [Green Version]
- Bishara, D.; Harwood, D.; Sauer, J.; Taylor, D.M. Anticholinergic effect on cognition (AEC) of drugs commonly used in older people. Int. J. Geriatr. Psychiatry 2017, 32, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Pasina, L.; Lucca, U.; Tettamanti, M. Relation between anticholinergic burden and cognitive impairment: Results from the Monzino 80-plus population-based study. Pharmacoepidemiol. Drug Saf. 2020, 29, 1696–1702. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Bali, V.; Carnahan, R.M.; Chen, H.; Johnson, M.L.; Aparasu, R.R. Anticholinergic burden and risk of cognitive impairment in elderly nursing home residents with depression. Res. Soc. Adm. Pharm. 2020, 16, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Sargent, L.; Nalls, M.; Amella, E.J.; Mueller, M.; Lageman, S.K.; Bandinelli, S.; Colpo, M.; Slattum, P.W.; Singleton, A.; Ferrucci, L. Anticholinergic Drug Induced Cognitive and Physical Impairment: Results from the InCHIANTI Study. J. Gerontol. A Biol. Sci. Med. Sci 2020, 75, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Weigand, A.J.; Bondi, M.W.; Thomas, K.R.; Campbell, N.L.; Galasko, D.R.; Salmon, D.P.; Sewell, D.; Brewer, J.B.; Feldman, H.H.; Delano-Wood, L. Association of anticholinergic medications and AD biomarkers with incidence of MCI among cognitively normal older adults. Neurology 2020, 95, e2295–e2304. [Google Scholar] [CrossRef]
- Gray, S.L.; Anderson, M.L.; Dublin, S.; Hanlon, J.T.; Hubbard, R.; Walker, R.; Yu, O.; Crane, P.K.; Larson, E.B. Cumulative use of strong anticholinergics and incident dementia: A prospective cohort study. JAMA Intern. Med. 2015, 175, 401–407. [Google Scholar] [CrossRef]
- Richardson, K.; Fox, C.; Maidment, I.; Steel, N.; Loke, Y.K.; Arthur, A.; Myint, P.K.; Grossi, C.M.; Mattishent, K.; Bennett, K.; et al. Anticholinergic drugs and risk of dementia: Case-control study. BMJ 2018, 361, k1315. [Google Scholar] [CrossRef] [Green Version]
- Grossi, C.M.; Richardson, K.; Fox, C.; Maidment, I.; Steel, N.; Loke, Y.K.; Arthur, A.; Myint, P.K.; Campbell, N.; Boustani, M.; et al. Anticholinergic and benzodiazepine medication use and risk of incident dementia: A UK cohort study. BMC Geriatr. 2019, 19, 276. [Google Scholar] [CrossRef] [Green Version]
- Coupland, C.A.C.; Hill, T.; Dening, T.; Morriss, R.; Moore, M.; Hippisley-Cox, J. Anticholinergic Drug Exposure and the Risk of Dementia: A Nested Case-Control Study. JAMA Intern. Med. 2019, 179, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Graves-Morris, K.; Stewart, C.; Soiza, R.L.; Taylor-Rowan, M.; Quinn, T.J.; Loke, Y.K.; Myint, P.K. The prognostic value of anticholinergic burden measures in relation to mortality in older individuals: A systematic review and meta-analysis. Front. Pharmacol. 2020, 11, 570. [Google Scholar] [CrossRef] [PubMed]
- McMichael, A.J.; Zafeiridi, E.; Ryan, M.; Cunningham, E.L.; Passmore, A.P.; McGuinness, B. Anticholinergic drug use and risk of mortality for people with dementia in Northern Ireland. Aging Ment. Health 2021, 25, 1475–1482. [Google Scholar] [CrossRef]
- Kalisch Ellett, L.M.; Pratt, N.L.; Ramsay, E.N.; Barratt, J.D.; Roughead, E.E. Multiple anticholinergic medication use and risk of hospital admission for confusion or dementia. J. Am. Geriatr. Soc. 2014, 62, 1916–1922. [Google Scholar] [CrossRef] [PubMed]
- Lisibach, A.; Benelli, V.; Ceppi, M.G.; Waldner-Knogler, K.; Csajka, C.; Lutters, M. Quality of anticholinergic burden scales and their impact on clinical outcomes: A systematic review. Eur. J. Clin. Pharmacol. 2021, 77, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Jessen, F.; Amariglio, R.E.; Buckley, R.F.; van der Flier, W.M.; Han, Y.; Molinuevo, J.L.; Rabin, L.; Rentz, D.M.; Rodriguez-Gomez, O.; Saykin, A.J.; et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020, 19, 271–278. [Google Scholar] [CrossRef]
- Rabin, L.A.; Smart, C.M.; Amariglio, R.E. Subjective Cognitive Decline in Preclinical Alzheimer’s Disease. Annu. Rev. Clin. Psychol. 2017, 13, 369–396. [Google Scholar] [CrossRef]
- Jessen, F. Subjective and objective cognitive decline at the pre-dementia stage of Alzheimer’s disease. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, S3–S7. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Beaumont, H.; Ferguson, D.; Yadegarfar, M.; Stubbs, B. Risk of dementia and mild cognitive impairment in older people with subjective memory complaints: Meta-analysis. Acta Psychiatr. Scand. 2014, 130, 439–451. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Klamer, T.T.; Wauters, M.; Azermai, M.; Durán, C.; Christiaens, T.; Elseviers, M.; Vander Stichele, R. A Novel Scale Linking Potency and Dosage to Estimate Anticholinergic Exposure in Older Adults: The Muscarinic Acetylcholinergic Receptor ANTagonist Exposure Scale. Basic Clin. Pharmacol. Toxicol. 2017, 120, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Weichert, I.; Romero-Ortuno, R.; Tolonen, J.; Soe, T.; Lebus, C.; Choudhury, S.; Nadarajah, C.V.; Nanayakkara, P.; Orrù, M.; Di Somma, S. Anticholinergic medications in patients admitted with cognitive impairment or falls (AMiCI). The impact of hospital admission on anticholinergic cognitive medication burden. Results of a multicentre observational study. J. Clin. Pharm. Ther. 2018, 43, 682–694. [Google Scholar] [CrossRef]
- López-Álvarez, J.; Sevilla-Llewellyn-Jones, J.; Agüera-Ortiz, L. Anticholinergic Drugs in Geriatric Psychopharmacology. Front. Neurosci. 2019, 13, 1309. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Kisely, S.; Zolotarev, B.; Warren, A.; Henderson, J.; George, M. Anticholinergic burden in older inpatients on psychotropic medication: Do we care? Australas. Psychiatry 2017, 25, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Sera, L.; McPherson, M.L. Anticholinergic Burden in Hospice Patients With Dementia. Am. J. Hosp. Palliat. Med. 2019, 36, 222–227. [Google Scholar] [CrossRef]
- Salahudeen, M.S.; Chyou, T.Y.; Nishtala, P.S. Serum anticholinergic activity and cognitive and functional adverse outcomes in older people: A systematic review and meta-analysis of the literature. PLoS ONE 2016, 11, e0151084. [Google Scholar] [CrossRef]
- Lozano-Ortega, G.; Johnston, K.M.; Cheung, A.; Wagg, A.; Campbell, N.L.; Dmochowski, R.R.; Ng, D.B. A review of published anticholinergic scales and measures and their applicability in database analyses. Arch. Gerontol. Geriatr. 2020, 87, 103885. [Google Scholar] [CrossRef] [PubMed]
- Nery, R.T.; Reis, A.M.M. Development of a Brazilian anticholinergic activity drug scale. Einstein 2019, 17, eAO4435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnahan, R.M.; Lund, B.C.; Perry, P.J.; Pollock, B.G.; Gulp, K.R. The anticholinergic drug scale as a measure of drug-related anticholinergic burden: Associations with serum anticholinergic activity. J. Clin. Pharmacol. 2006, 46, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, J.L.; Salow, M.J.; Angelini, M.C.; McGlinchey, R.E. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch. Intern. Med. 2008, 168, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boustani, M.; Campbell, N.; Munger, S.; Maidment, I.; Fox, C. Impact of anticholinergics on the ageing brain: A review and practical application. Aging Health 2008, 4, 311–320. [Google Scholar] [CrossRef]
- Durán, C.E.; Azermai, M.; Vander Stichele, R.H. Systematic review of anticholinergic risk scales in older adults. Eur. J. Clin. Pharmacol. 2013, 69, 1485–1496. [Google Scholar] [CrossRef]
- Salahudeen, M.S.; Duffull, S.B.; Nishtala, P.S. Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: A systematic review. BMC Geriatr. 2015, 15, 31. [Google Scholar] [CrossRef] [Green Version]
- Kiesel, E.K.; Hopf, Y.M.; Drey, M. An anticholinergic burden score for German prescribers: Score development. BMC Geriatr. 2018, 18, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jun, K.; Hwang, S.; Ah, Y.M.; Suh, Y.; Lee, J.Y. Development of an Anticholinergic Burden Scale specific for Korean older adults. Geriatr. Gerontol. Int. 2019, 19, 628–634. [Google Scholar] [CrossRef]
- Base de Datos de medicamentos del Consejo General de Farmacéuticos (BotPlus 2.0). Available online: https://botplusweb.portalfarma.com (accessed on 20 November 2021).
- Ramos, H.; Pardo, J.; Sánchez, R.; Puchades, E.; Pérez-Tur, J.; Navarro, A.; Moreno, L. Pharmacist-Physician Interprofessional Collaboration to Promote Early Detection of Cognitive Impairment: Increasing Diagnosis Rate. Front. Pharmacol. 2021, 12, 579489. [Google Scholar] [CrossRef]
- Ramos, H.; Alacreu, M.; Guerrero, M.D.; Sánchez, R.; Moreno, L. Lifestyle Variables Such as Daily Internet Use as Promising Protective Factors against Cognitive Impairment in Patients with Subjective Memory Complaints. Preliminary Results. J. Pers. Med. 2021, 11, 1366. [Google Scholar] [CrossRef]
- 52. WHO Collaborating Centre for Drug Statistics Methodology, ATC Classification Index with DDDs, 2022. Oslo, Norway 2021. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 16 November 2021).
- Buschke, H.; Kuslansky, G.; Katz, M.; Stewart, W.F.; Sliwinski, M.J.; Eckholdt, H.M.; Lipton, R.B. Screening for dementia with the Memory Impairment Screen. Neurology 1999, 52, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Böhm, P.; Peña-Casanova, J.; Gramunt, N.; Manero, R.M.; Terrón, C.; Quiñones Úbeda, S. Spanish version of the Memory Impairment Screen (MIS): Normative data and discriminant validity. Neurologia 2005, 20, 402–411. [Google Scholar]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Martínez de la Iglesia, J.; Dueñas, R.; Onís, M.C.; Aguado, C.; Albert, C.; Luque, R. Spanish language adaptation and validation of the Pfeiffer’s questionnaire (SPMSQ) to detect cognitive deterioration in people over 65 years of age. Med. Clin. 2001, 117, 129–134. [Google Scholar] [CrossRef]
- Lopes, M.; Brucki, S.M.D.; Giampaoli, V.; Mansur, L.L. Semantic Verbal Fluency test in dementia: Preliminary retrospective analysis. Dement. Neuropsychol. 2009, 3, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Canning, S.J.; Leach, L.; Stuss, D.; Ngo, L.; Black, S.E. Diagnostic utility of abbreviated fluency measures in Alzheimer disease and vascular dementia. Neurology 2004, 62, 556–562. [Google Scholar] [CrossRef]
- Pardo, C.C.; González, A.L. The utility of the semantic verbal fluency test in diagnosis of dementia. Rev. Neurol. 1999, 29, 709–714. [Google Scholar] [CrossRef]
- Muñoz-Almaraz, F.J.; Climent, M.T.; Guerrero, M.D.; Moreno, L.; Pardo, J. A machine learning approach to design an efficient selective screening of mild cognitive impairment. J. Vis. Exp. 2020, 155, e59649. [Google Scholar] [CrossRef] [PubMed]
- RStudio Team. RStudio: Integrated Development for R. RStudio, PBC, Boston, MA. 2020. Available online: https://www.rstudio.com (accessed on 28 November 2021).
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- FDA U.S. Food and Drug Administration. Drug Safety Communications. Available online: https://www.fda.gov/media/99761/download#:~:text=%5B8%2D31%2D2016%5D,or%20difficult%20breathing%20and%20deaths (accessed on 30 November 2021).
- Risacher, S.L.; McDonald, B.C.; Tallman, E.F.; West, J.D.; Farlow, M.R.; Unverzagt, F.W.; Gao, S.; Boustani, M.; Crane, P.K.; Petersen, R.C.; et al. Association Between Anticholinergic Medication Use and Cognition, Brain Metabolism, and Brain Atrophy in Cognitively Normal Older Adults. JAMA Neurol. 2016, 73, 721–732. [Google Scholar] [CrossRef] [Green Version]
- Ramos, H.; Moreno, L.; Gil, M.; García-Lluch, G.; Sendra-Lillo, J.; Alacreu, M. Pharmacists’ Knowledge of Factors Associated with Dementia: The A-to-Z Dementia Knowledge List. Int. J. Environ. Res. Public Health 2021, 18, 9934. [Google Scholar] [CrossRef]
- Soundararajan, K.; Balchandra, P. Staff Awareness of Anti-Cholinergic Burden (ACB)—A Qualitative Cross-Sectional Study in a Tertiary Care Hospital. Cureus 2021, 13, e14141. [Google Scholar] [CrossRef] [PubMed]
- Lampela, P.; Lavikainen, P.; Garcia-Horsman, J.A.; Bell, J.S.; Huupponen, R.; Hartikainen, S. Anticholinergic drug use, serum anticholinergic activity, and adverse drug events among older people: A population-based study. Drugs Aging 2013, 30, 321–330. [Google Scholar] [CrossRef]
- Martorana, A.; Assogna, M.; De Lucia, V.; Motta, C.; Bonomi, C.G.; Bernocchi, F.; Di Donna, M.G.; Koch, G. Cognitive reserve and Alzheimer’s biological continuum: Clues for prediction and prevention of dementia. Minerva Med. 2021, 112, 441–447. [Google Scholar] [CrossRef]
- Breijyeh, Z.; Karaman, R. Comprehensive Review on Alzheimer’s Disease: Causes and Treatment. Molecules 2020, 25, 5789. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K. Cholinesterase inhibitors as Alzheimer’s therapeutics (Review). Mol. Med. Rep. 2019, 20, 1479–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montastruc, F.; Benevent, J.; Touafchia, A.; Chebane, L.; Araujo, M.; Guitton-Bondon, E.; Durrieu, G.; Arbus, C.; Schmitt, L.; Begaud, B.; et al. Atropinic (anticholinergic) burden in antipsychotic-treated patients. Fundam. Clin. Pharmacol. 2018, 32, 114–119. [Google Scholar] [CrossRef]
- Niikawa, H.; Okamura, T.; Ito, K.; Ura, C.; Miyamae, F.; Sakuma, N.; Ijuin, M.; Inagaki, H.; Sugiyama, M.; Awata, S. Association between polypharmacy and cognitive impairment in an elderly Japanese population residing in an urban community. Geriatr. Gerontol. Int. 2017, 17, 1286–1293. [Google Scholar] [CrossRef]
- Baek, Y.H.; Kim, H.J.; Bae, J.H.; Lee, H.; Oh, I.S.; Kim, W.J.; Shin, J.Y. Benzodiazepine-Related Cognitive Impairment or Dementia: A Signal Detection Study Using a Case/Non-Case Approach. Psychiatry Investig. 2020, 17, 587–595. [Google Scholar] [CrossRef]
- Tapiainen, V.; Taipale, H.; Tanskanen, A.; Tiihonen, J.; Hartikainen, S.; Tolppanen, A.M. The risk of Alzheimer’s disease associated with benzodiazepines and related drugs: Aa nested case–control study. Acta Psychiatr. Scand. 2018, 138, 91–100. [Google Scholar] [CrossRef] [Green Version]


| Drug Name | ATC Code | Carnahan 2006 | Rudolph 2008 | Boustani 2008 | Durán 2013 | Salahudeen 2015 | Kiesel 2018 | Jun 2019 |
|---|---|---|---|---|---|---|---|---|
| Aclidinium inh | R03BB05 | 1 | ||||||
| Alimemazine * | R06AD01 | 1 | 2 | 1 or 2 | 1 | |||
| Alprazolam | N05BA12 | 1 | 1 | Disc | 1 or 3 | 1 | 1 | |
| Alverine | A03AX08 | 1 | Disc | 1 or 2 | 0 | |||
| Amisulpride | N05AL05 | 1 | ||||||
| Ampicillin | J01CA01 | 1 | Disc | 1 | 1 | 0 | ||
| Aripiprazole | N05AX12 | 1 | 1 | 1 | ||||
| Asenapine | N05AH05 | 1 | 1 | |||||
| Atenolol | C07AB03 | 0 | 1 | 1 | 1 | 0 | ||
| Azathioprine | L04AX01 | 1 | Disc | 1 | 1 | 0 | ||
| Benazepril | C09AA07 | 0 | Disc | 1 | 1 | 0 | ||
| Betaxolol | C07AB05 | 0 | Disc | 1 | 1 | 0 | ||
| Bisacodyl | A06AB02 | 0 | Disc | 1 | 1 | 0 | ||
| Bromocriptine | N04BC01 | 1 | 1 or 2 | 1 | 1 | 0 | ||
| Bromperidol | N05AD06 | 1 | ||||||
| Bupropion | N06AX12 | 0 | 1 | Disc | 1 | 1 | 1 | |
| Captopril | C09AA01 | 1 | 1 | Disc | 1 | 1 | 0 | |
| Cefamandole | J01DC03 | 1 | Disc | 1 | 0 | |||
| Cefoxitin | J01DC01 | 1 | Disc | 1 | 0 | |||
| Celecoxib | M01AH01 | 0 | Disc | 1 | 1 | 0 | ||
| Cephalothin | J01DB03 | 1 | Disc | 1 | 0 | |||
| Cetirizine | R06AE07 | 0 | 2 | 2 | 1 or 2 | 1 | 1 | |
| Cinnarizine | N07CA02 | 1 | ||||||
| Chlordiazepoxide | N05BA02 | 1 | 1 | 1 | 1 | 1 | ||
| Chlorthalidone | C03BA04 | 1 | 1 | Disc | 1 | 1 | 0 | |
| Citalopram | N06AB04 | 0 | 1 | 1 | 1 | 1 | ||
| Clindamycin | J01FF01 | 1 | Disc | 1 | 1 | 0 | ||
| Clonazepam | N03AE01 | 1 | 1 | 1 | 1 | 1 | ||
| Clorazepate | N05BA05 | 1 | 1 | Disc | 1 or 3 | 1 | 1 | |
| Codeine | R05DA04 | 1 | 1 | 1 or 2 | 1 or 2 | 1 | 1 | |
| Colchicine | M04AC01 | 0 | Disc | 1 or 3 | 0 | |||
| Cortisone | H02AB10 | 1 | Disc | 1 | ||||
| Cycloserine | J04AB01 | 1 | Disc | 1 | 0 | |||
| Cyclosporine | L04AD01 | 1 | Disc | 1 | 0 | |||
| Desloratadine | R06AX27 | 1 | 1 | 1 | ||||
| Desvenlafaxine | N06AX23 | 1 | ||||||
| Dexamethasone | H02AB02 | 1 | Disc | 1 | 1 | 0 | ||
| Dextromethorphan | R05DA09 | 0 | Disc | 1 | 1 | 1 | ||
| Diazepam | N05BA01 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Digitoxin | C01AA04 | 1 | 1 | 1 | 1 | |||
| Digoxin | C01AA05 | 1 | 1 | Disc | 1 or 3 | 1 | 1 | |
| Diltiazem | C08DB01 | 1 | Disc | 1 | 1 | 0 | ||
| Dipyridamole | B01AC07 | 1 | 1 | Disc | 1 | 1 | 0 | |
| Disopyramide | C01BA03 | 2 | 1 | 2 | 1 or 2 | |||
| Domperidone | A03FA03 | 1 | 1 | 1 | 0 | |||
| Entacapone | N04BX02 | 0 | 1 | 1 | 1 | 1 | 0 | |
| Escitalopram | N06AB10 | 0 | Disc | 1 | 1 | 1 | ||
| Estazolam | N05CD04 | 1 | Disc | 1 | 1 | |||
| Famotidine | A02BA03 | 1 | Disc | 1 | 1 | 0 | ||
| Fentanyl | N01AH01 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Fexofenadine | R06AX26 | 0 | 2 | 2 | 1 | 0 | ||
| Flunitrazepam | N05CD03 | Disc | 1 | 1 | ||||
| Flupentixol | N05AF01 | 1 | ||||||
| Fluoxetine | N06AB03 | 1 | 1 | 1 | 1 | 1 | ||
| Flurazepam | N05CD01 | 1 | Disc | 1 | 1 | 1 | ||
| Fluvoxamine | N06AB08 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Furosemide | C03CA01 | 1 | 1 | Disc | 1 or 3 | 1 | 1 | |
| Gentamicin | J01GB03 | 1 | Disc | 1 | 1 | 0 | ||
| Glycopyrronium inh | R03BB06 | 1 | 2 | |||||
| Guaifenesin | R05CA03 | 0 | Disc | 1 | 1 | 1 | ||
| Haloperidol | N05AD01 | 0 | 1 | 1 | 1 or 2 | 1 or 2 | 2 | 1 |
| Hydralazine | C02DB02 | 1 | 1 | Disc | 1 | 1 | 1 | |
| Hydrocodone | R05DA03 | 0 | 1 or 2 | 2 | 1 | |||
| Hydrocortisone | H02AB09 | 1 | 1 | Disc | 1 | 1 | 1 | |
| Iloperidone | N05AX14 | 1 | ||||||
| Ipratropium inh | R03BB01 | 0 | 3 | 3 | 1 | |||
| Isosorbide mononitrate | C01DA08 | 1 | 1 | Disc | 1 | 1 | 0 | |
| Isosorbide dinitrate | C01DA14 | 1 | 1 | Disc | 1 | 1 | 0 | |
| Ketorolac | M01AB15 | 1 | 1 | 1 | 0 | |||
| Ketotifen | R06AX17 | 1 | Disc | 1 | 1 | |||
| Levocetirizine | R06AE09 | 1 | 1 | 1 | ||||
| Levodopa—carbidopa | N04BA02 | 0 | 1 | Disc | 1 | 1 | 0 | |
| Lithium | N05AN01 | 0 | 1 | 1 | 1 | 0 | ||
| Loperamide | A07DA03 | 1 | 2 | 1 | 1 or 2 | 1 or 2 | 2 | 1 |
| Loratadine | R06AX13 | 0 | 2 | 1 or 2 | 1 or 2 | 1 | 1 | |
| Lorazepam | N05BA06 | 1 | Disc | 1 | 1 | 1 | ||
| Lumiracoxib | M01AH06 | Disc | 1 | |||||
| Mebeverine | A03AA04 | 1 | ||||||
| Metformin | A10BA02 | 0 | Disc | 1 | 1 | 0 | ||
| Methocarbamol | M03BA03 | 1 | 1 | 1 | 1 | 1 | ||
| Methotrexate | L04AX03 | 0 | Disc | 1 | 1 | 0 | ||
| Methylprednisolone | H02AB04 | 1 | Disc | 1 | 1 | 0 | ||
| Metoclopramide | A03FA01 | 0 | 1 | Disc | 1 | 1 | 0 | |
| Metoprolol | C07AB02 | 0 | 1 | 0 | 1 | 1 | 0 | |
| Midazolam | N05CD08 | 1 | Disc | 1 | 1 | 1 | ||
| Mirtazapine | N06AX11 | 0 | 1 | 1 | 1 | 1 | 1 | |
| Morphine | N02AA01 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Naratriptan | N02CC02 | Disc | 1 | 1 | 0 | |||
| Nefazodone | N06AX06 | 0 | 1 | 1 | ||||
| Nifedipine | C08CA05 | 1 | 1 | 0 | 1 | 1 | 0 | |
| Nizatidine | A02BA04 | 1 | Disc | 1 | ||||
| Oxazepam | N05BA04 | 1 | Disc | 1 | 1 | |||
| Oxycodone | N02AA05 | 1 | 1 | 1 | 1 | 1 | ||
| Paliperidone | N05AX13 | 1 | 1 | 1 | ||||
| Pancuronium | M03AC01 | 1 | Disc | 1 | 1 | |||
| Phenelzine | N06AF03 | 1 | 1 | 1 | ||||
| Phenobarbital | N03AA02 | 0 | Disc | 1 | 1 | 0 | ||
| Piperacillin | J01CA12 | 1 | Disc | 1 | 1 | 0 | ||
| Pramipexole | N04BC05 | 0 | 1 | Disc | 1 | 1 | ||
| Prednisolone | H02AB06 | 1 | Disc | 1 | 1 | 1 | ||
| Prednisone | H02AB07 | 1 | 1 | 1 | 1 | |||
| Pridinol | M03BX03 | 1 | ||||||
| Pseudoephedrine | R01BA02 | 0 | 2 | Disc | 2 | 1 | 0 | |
| Quinidine | C01BA01 | 0 | 1 | 1 | 1 | |||
| Risperidone | N05AX08 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Rotigotine patch | N04BC09 | 1 | ||||||
| Selegiline | N04BD01 | 0 | 1 | Disc | 1 | 1 | 0 | |
| Sertraline | N06AB06 | 1 | 0 | 1 | 1 | 0 | ||
| Sumatriptan | N02CC01 | Disc | 1 | 1 | 0 | |||
| Temazepam | N05CD07 | 1 | 1 | 1 | 1 | 1 | ||
| Theophylline | R03DA04 | 1 | 1 | 1 or 2 | 1 or 2 | 2 | 1 | |
| Tiotixene | N05AF04 | 1 | 3 | 3 | 1 or 3 | 1 | ||
| Tiotropium inh | R03BB04 | 1 | ||||||
| Trandolapril | C09AA10 | 0 | Disc | 1 | 1 | |||
| Trazodone | N06AX05 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Triamcinolone | H02AB08 | 1 | Disc | 1 | 1 | 0 | ||
| Triamterene | C03DB02 | 1 | 1 | Disc | 1 | 1 | 0 | |
| Trimebutine | A03AA05 | 1 | ||||||
| Triazolam | N05CD05 | 1 | 1 | 1 | 1 | 1 | ||
| Valproic acid | N03AG01 | 1 | Disc | 1 | 1 | 0 | ||
| Vancomycin | J01XA01 | 1 | Disc | 1 | 1 | 0 | ||
| Venlafaxine | N06AX16 | 0 | 0 | 1 | 1 | 1 | ||
| Warfarin | B01AA03 | 1 | 0 | 1 | 1 | 0 | ||
| Ziprasidone | N05AE04 | 1 | Disc | 1 | 1 | 1 | ||
| Zolmitriptan | N02CC03 | Disc | 1 | 1 | 0 |
| Drug Name | ATC Code | Carnahan 2006 | Rudolph 2008 | Boustani 2008 | Durán 2013 | Salahudeen 2015 | Kiesel 2018 | Jun 2019 |
|---|---|---|---|---|---|---|---|---|
| Amantadine | N04BB01 | 1 | 2 | 2 | 1 or 2 | 1 or 2 | 2 | 2 |
| Baclofen | M03BX01 | 0 | 2 | 2 | 2 | 1 | 1 | |
| Carbamazepine | N03AF01 | 2 | 2 | 1 or 2 | 1 or 2 | 2 | 1 | |
| Cloperastine | R05DB21 | 2 | ||||||
| Cimetidine | A02BA01 | 2 | 2 | 1 | 2 | 1 or 2 | 2 | 2 |
| Cyclobenzaprine | M03BX08 | 2 | 2 | 2 | 1 or 2 | 1 or 2 | 2 | |
| Dosulepin | N06AA16 | 2 | 2 | |||||
| Fluphenazine | N05AB02 | 1 | 3 | 3 | 1 or 3 | 1 | ||
| Loxapine | N05AH01 | 2 | 2 | 2 | 2 | 2 | 2 | |
| Maprotiline | N06AA21 | Disc | 3 | 2 | ||||
| Meperidine * | N02AB02 | 2 | 2 | 2 | 2 | 2 | ||
| Methadone | N07BC02 | 2 | 2 | 2 | ||||
| Molindone | N05AE02 | 2 | 2 | 2 | 2 | 2 | ||
| Nefopam | N02BG06 | 2 | 2 | |||||
| Olanzapine | N05AH03 | 1 | 2 | 3 | 1 or 2 | 1, 2 or 3 | 2 | 3 |
| Oxcarbazepine | N03AF02 | 2 | 2 | 2 | 2 | 2 | 2 | |
| Paroxetine | N06AB05 | 1 | 1 | 3 | 1 or 2 | 1, 2 or 3 | 2 | 2 |
| Perphenazine | N05AB03 | 1 | 3 | 3 | Disc | 1, 2 or 3 | 1 | 2 |
| Pimozide | N05AG02 | 2 | 2 | 2 | 2 | 2 | 2 | |
| Prochlorperazine | N05AB04 | 1 | 2 | 1 or 2 | 1 or 2 | |||
| Promazine | N05AA03 | 3 | 2 | 2 | ||||
| Propoxyphene | N02AC04 | 0 | 1 or 2 | 2 | ||||
| Quetiapine | N05AH04 | 0 | 1 | 3 | 1 or 2 | 1, 2 or 3 | 2 | 2 |
| Ranitidine | A02BA02 | 2 | 1 | 1 or 2 | 1 or 2 | 2 | 1 | |
| Tramadol | N02AX02 | 1 | 1 or 2 | 1 or 2 | 2 | 2 | ||
| Triprolidine | R06AX07 | 2 | ||||||
| Zotepine | N05AX11 | 2 | ||||||
| Zuclopenthixol | N05AF05 | 2 |
| Drug Name | ATC Code | Carnahan 2006 | Rudolph 2008 | Boustani 2008 | Durán 2013 | Salahudeen 2015 | Kiesel 2018 | Jun 2019 |
|---|---|---|---|---|---|---|---|---|
| Acepromazine | N05AA04 | 3 | 3 | |||||
| Amitriptyline | N06AA09 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Amoxapine | N06AA17 | 3 | Disc | 3 | 3 | |||
| Atropine | A03BA01 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Belladonna | A03BA04 | 2 | 3 | 2 or 3 | 3 | |||
| Benzatropine * | N04AC01 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Biperiden | N04AA02 | 3 | ||||||
| Brompheniramine | R06AB01 | 3 | 3 | 3 | 3 | 3 | ||
| Carbinoxamine | R06AA08 | 3 | 3 | 3 | 3 | 3 | ||
| Carisoprodol | M03BA02 | 0 | 3 | Disc | 3 | |||
| Chlorphenamine * | R06AB04 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Chlorpromazine | N05AA01 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Chlorprothixene | N05AF03 | 3 | ||||||
| Cimetropium bromide | A03BB05 | 3 | ||||||
| Clemastine | R06AA04 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Clomipramine | N06AA04 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Clozapine | N05AH02 | 3 | 2 | 3 | 3 | 2 or 3 | 3 | 3 |
| Cyproheptadine | R06AX02 | 2 | 3 | 2 | 3 | 2 or 3 | 3 | 2 |
| Darifenacin | G04BD10 | 3 | 3 | 3 | 3 | 3 | ||
| Desipramine | N06AA01 | 3 | 2 | 3 | 3 | 2 or 3 | ||
| Dexbrompheniramine | R06AB06 | 3 | ||||||
| Dexchlorpheniramine | R06AB02 | 3 | 3 | 3 | ||||
| Dicyclomine * | A03AA07 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Difemerine | A03AA09 | 3 | ||||||
| Diphenhydramine * | R06AA02 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Doxepin | N06AA12 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Doxylamine | R06AA09 | 3 | 1 | 3 | ||||
| Emepronium | G04BD01 | 3 | 3 | |||||
| Fesoterodine | G04BD11 | 3 | 3 | |||||
| Flavoxate | G04BD02 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Homatropine | S01FA05 | 3 | 3 | |||||
| Hydroxyzine | N05BB01 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Hyoscyamine | A03BA03 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Imipramine | N06AA02 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Levomepromazine * | N05AA02 | 2 | 2 | 3 | 3 | 3 | 2 | |
| Meclozine * | R06AE05 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Mequitazine | R06AD07 | 3 | ||||||
| Nortriptyline | N06AA10 | 3 | 2 | 3 | 3 | 2 or 3 | 3 | 3 |
| Opipramol | N06AA05 | Disc | 3 | 2 | ||||
| Orphenadrine | N04AB02 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Otilonium bromide | A03AB06 | 3 | ||||||
| Oxybutynin | G04BD04 | 3 | 3 | 3 | 3 | 2 or 3 | 3 | 3 |
| Pheniramine | R06AB05 | 3 | ||||||
| Procyclidine | N04AA04 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Promethazine | R06AD02 | 3 | 3 | 3 | 3 | 3 | 1 | |
| Propantheline | A03AB05 | 3 | 3 | 3 | 2 or 3 | |||
| Propiverine | G04BD06 | 3 | 3 | 3 | ||||
| Protriptyline | N06AA11 | 3 | 3 | 3 | ||||
| Pyrilamine * | R03DA12 | 3 | 3 | 3 | 3 | 3 | ||
| Scopolamine * | A04AD01 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Solifenacin | G04BD08 | 3 | 3 | 3 | ||||
| Thioridazine | N05AC02 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Tiemonium iodide | A03AB17 | 3 | ||||||
| Timepidium bromide | A03AB19 | 3 | ||||||
| Tizanidine | M03BX02 | 3 | 3 | 3 | 3 | 2 | ||
| Tolterodine | G04BD07 | 3 | 2 | 3 | 3 | 2 or 3 | 3 | 3 |
| Trifluoperazine | N05AB06 | 1 | 3 | 3 | Disc | 1 or 3 | ||
| Trihexyphenidyl | N04AA01 | 3 | 3 | 3 | 3 | 3 | 3 | |
| Trimipramine | N06AA06 | 3 | 3 | 3 | 3 | 3 | ||
| Tropatepine | N04AA12 | 3 | 3 | |||||
| Trospium | G04BD09 | 3 | 3 | 3 | ||||
| Valethamate | A03AX14 | 3 |
| Characteristics of Study Participants (n = 512) | Cognitive Decline (n = 164) | No Cognitive Decline (n = 348) |
|---|---|---|
| Age, years (mean (SD)) | 74.67 (7.91) | 68.09 (9.08) |
| Female (n (%)) | 123 (75%) | 255 (73.27%) |
| BMI (mean (SD)) | 27.15 (3.85) | 27.15 (3.90) |
| Drugs (mean (SD)) | 6.52 (3.31) | 5.74 (3.28) |
| Mean TAB ACB score (mean (SD)) | 1.08 (1.53) | 0.87 (1.37) |
| Mean TAB CALS score (mean (SD)) | 2.14 (1.88) | 1.62 (1.67) |
| TAB CALS score ≥ 3 (n (%)) | 61 (37.20%) | 86 (24.71%) |
| TAB ACB score ≥ 3 (n (%)) | 35 (21.34%) | 49 (14.10%) |
| MIS test (mean (SD)) | 4.44 (2.31) | 7.09 (0.99) |
| SPMSQ test (mean (SD)) | 2.99 (1.96) | 0.73 (0.78) |
| SVF test (mean (SD)) | 10.05 (3.82) | 16.10 (4.38) |
| Diabetes (n (%)) | 40 (24.39%) | 77 (22.13%) |
| Hypertension (n (%)) | 100 (60.98%) | 189 (54.31%) |
| Hypercholesterolemia (n (%)) | 82 (50%) | 159 (45.69%) |
| Depression (n (%)) | 62 (37.80%) | 100 (28.74%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos, H.; Moreno, L.; Pérez-Tur, J.; Cháfer-Pericás, C.; García-Lluch, G.; Pardo, J. CRIDECO Anticholinergic Load Scale: An Updated Anticholinergic Burden Scale. Comparison with the ACB Scale in Spanish Individuals with Subjective Memory Complaints. J. Pers. Med. 2022, 12, 207. https://doi.org/10.3390/jpm12020207
Ramos H, Moreno L, Pérez-Tur J, Cháfer-Pericás C, García-Lluch G, Pardo J. CRIDECO Anticholinergic Load Scale: An Updated Anticholinergic Burden Scale. Comparison with the ACB Scale in Spanish Individuals with Subjective Memory Complaints. Journal of Personalized Medicine. 2022; 12(2):207. https://doi.org/10.3390/jpm12020207
Chicago/Turabian StyleRamos, Hernán, Lucrecia Moreno, Jordi Pérez-Tur, Consuelo Cháfer-Pericás, Gemma García-Lluch, and Juan Pardo. 2022. "CRIDECO Anticholinergic Load Scale: An Updated Anticholinergic Burden Scale. Comparison with the ACB Scale in Spanish Individuals with Subjective Memory Complaints" Journal of Personalized Medicine 12, no. 2: 207. https://doi.org/10.3390/jpm12020207
APA StyleRamos, H., Moreno, L., Pérez-Tur, J., Cháfer-Pericás, C., García-Lluch, G., & Pardo, J. (2022). CRIDECO Anticholinergic Load Scale: An Updated Anticholinergic Burden Scale. Comparison with the ACB Scale in Spanish Individuals with Subjective Memory Complaints. Journal of Personalized Medicine, 12(2), 207. https://doi.org/10.3390/jpm12020207