
Quality of Life in Patients with Acute Severe Ulcerative Colitis: Long-Term Follow-Up Results from the CONSTRUCT Trial

 , , ,
, , ,
Abstract
1. Introduction
Key messages
- Acute severe Ulcerative colitis (ASUC) can have a negative effect on patient quality of life;
- Drug treatment of ASUC can improve patient-reported quality of life;
- QoL should be assessed alongside clinical parameters.
- Generic and disease-specific QoL improvements following drug treatment for ASUC are maintained long term (up to 84 months) after treatment;
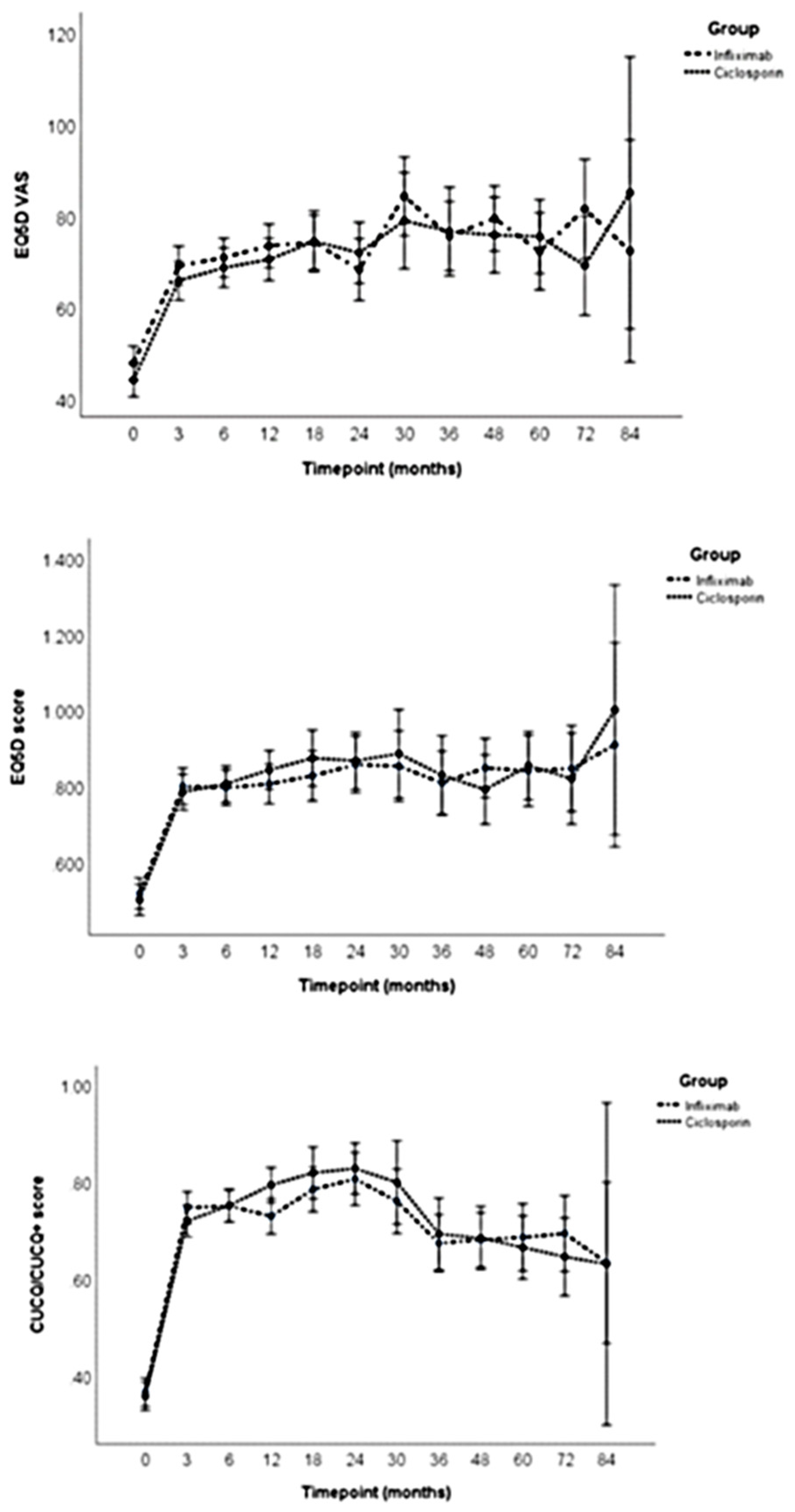
- There are no differences in long-term QoL in patients receiving infliximab or ciclosporin as a rescue therapy for ASUC.
- A colectomy did not appear to adversely affect QoL in patients postsurgery;
- It would be interesting to explore differences in QoL between patients with and without a stoma at the various time points and other factors that can affect QoL.
2. Materials and Methods
2.1. QoL Questionnaires
2.1.1. Crohn’s and Ulcerative Colitis Questionnaire (CUCQ) and CUCQ+
2.1.2. EQ-5D-3 Level (EQ5D-3L)
2.2. Analysis
2.3. Ethical Considerations
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Ordas, I.; Eckmann, L.; Talamini, M.; Baumgart, D.C.; Sandborn, W.J. Ulcerative colitis. Lancet 2012, 380, 1606–1619. [Google Scholar] [CrossRef] [PubMed]
- Loftus, E.V.; Sandborn, W.J. Epidemiology of inflammatory bowel disease. Gastroenterol. Clin. N. Am. 2002, 31, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Irvine, E.J. Quality of life of patients with ulcerative colitis: Past, present, and future. Inflamm. Bowel Dis. 2008, 14, 554–565. [Google Scholar] [CrossRef]
- Moradkhani, A.; Beckman, L.J.; Tabibian, J.H. Health-related quality of life in inflammatory bowel disease: Psychosocial, clinical, socioeconomic, and demographic predictors. J. Crohns Colitis 2013, 7, 467–473. [Google Scholar] [CrossRef]
- Hutchings, H.A.; Alrubiay, L.; Watkins, A.; Cheung, W.Y.; Seagrove, A.C.; Williams, J.G. Validation of the Crohn’s and Ulcerative Colitis questionnaire in patients with acute severe ulcerative colitis. UEG J. 2017, 5, 571–578. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER). Guidance for Industry Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. 2009. Available online: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM193282.pdf (accessed on 5 November 2019).
- Dinesen, L.C.; Walsh, A.J.; Protic, M.N.; Heap, G.; Cummings, F.; Warren, B.F.; George, B.; Mortensen, N.J.; Travis, S.P. The pattern and outcome of acute severe colitis. J. Crohns Colitis 2010, 4, 431–437. [Google Scholar] [CrossRef]
- Williams, J.G.; Alam, M.F.; Alrubaiy, L.; Clement, C.; Cohen, D.; Grey, M.; Hilton, M.; Hutchings, H.A.; Longo, M.; Morgan, J.M.; et al. Comparison Of iNfliximab and ciclosporin in STeroid Resistant Ulcerative Colitis: Pragmatic randomised Trial and economic evaluation (CONSTRUCT). Health Technol. Assess. 2016, 20, 1–320. [Google Scholar] [CrossRef]
- Laharie, D.; Bourreille, A.; Branche, J.; Allez, M.; Bouhnik, Y.; Filippi, J.; Zerbib, F.; Savoye, G.; Vuitton, L.; Moreau, J.; et al. Long-term outcome of patients with steroid-refractory acute severe UC treated with ciclosporin or infliximab. Gut 2018, 67, 237–243. [Google Scholar] [CrossRef]
- Chang, K.H.; Burke, J.P.; Coffey, J.C. Infliximab versus cyclosporine as rescue therapy in acute severe steroid-refractory ulcerative colitis: A systematic review and meta-analysis. Int. J. Colorectal Dis. 2013, 28, 287–293. [Google Scholar] [CrossRef]
- Jarnerot, G.; Rolny, P.; Sandberg-Gertzen, H. Intensive intravenous treatment of ulcerative colitis. Gastroenterology 1985, 89, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Holvoet, T.; Lobaton, T.; Hindryckx, P. Optimal Management of Acute Severe Ulcerative Colitis (ASUC): Challenges and Solutions. Clin. Exp. Gastroenterol. 2021, 14, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Seagrove, A.C.; Alam, M.F.; Alrubaiy, L.; Cheung, W.-J.; Clement, C.; Cohen, D.; Grey, M.; Hilton, M.; Hutchings, H.; Morgan, J.; et al. Randomised controlled trial. Comparison Of iNfliximab and ciclosporin in STeroid Resistant Ulcerative Colitis: Trial design and protocol (CONSTRUCT). BMJ Open 2014, 4, e005091. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.G.; Alam, M.F.; Alrubaiy, L.; Arnott, I.; Clement, C.; Cohen, D.; Gordon, J.N.; Hawthorne, A.B.; Hilton, M.; Hutchings, H.A.; et al. Infliximab versus ciclosporin for steroid-resistant acute severe ulcerative colitis (CONSTRUCT): A mixed methods, open-label, pragmatic randomised trial. Lancet Gastroenterol. Hepatol. 2016, 1, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Clement, C.; Rapport, F.; Seagrove, A.; Alrubaiy, L.; Williams, J. Healthcare professionals’ views of the use and administration of two salvage therapy drugs for acute ulcerative colitis: A nested qualitative study within the CONSTRUCT trial. BMJ Open 2017, 7, e014512. [Google Scholar] [CrossRef]
- Rapport, F.; Clement, C.; Seagrove, A.C.; Alrubaiy, L.; Hutchings, H.A.; Williams, J.G. Patient views about the impact of ulcerative colitis and its management with drug treatment and surgery: A nested qualitative study within the CONSTRUCT trial. BMC Gastroenterol. 2019, 19, 166. [Google Scholar] [CrossRef]
- Alrubaiy, L.; Cheung, W.Y.; Dodds, P.; Hutchings, H.A.; Russell, I.T.; Watkins, A.; Williams, J.G. Development of a short questionnaire to assess the quality of life in Crohn’s disease and ulcerative colitis. J. Crohns Colitis 2015, 9, 66–76. [Google Scholar] [CrossRef]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef]
- Truelove, S.C.; Witts, L.J. Cortisone in ulcerative colitis; final report on a therapeutic trial. Br. Med. J. 1955, 2, 1041–1048. [Google Scholar] [CrossRef]
- Yarlas, A.; D’Haens, G.; Willian, M.K.; Teynor, M. Health-Related Quality of Life and Work-Related Outcomes for Patients With Mild-to-Moderate Ulcerative Colitis and Remission Status Following Short-Term and Long-Term Treatment With Multimatrix Mesalamine: A Prospective, Open-Label Study. Inflamm. Bowel Dis. 2018, 24, 450–463. [Google Scholar] [CrossRef]
- Hoivik, M.L.; Moum, B.; Solberg, I.C.; Cvancarova, M.; Hoie, O.; Vatn, M.H.; Bernklev, T.; IBSEN Study Group. Health-related quality of life in patients with ulcerative colitis after a 10-year disease course: Results from the IBSEN study. Inflamm. Bowel Dis. 2012, 18, 1540–1549. [Google Scholar] [CrossRef]
- Laharie, D.; Bourreille, A.; Branche, J.; Allez, M.; Bouhnik, Y.; Filippi, J.; Zerbib, F.; Savoye, G.; Nachury, M.; Moreau, J.; et al. Ciclosporin versus infliximab in patients with severe ulcerative colitis refractory to intravenous steroids: A parallel, open-label randomised controlled trial. Lancet 2012, 380, 1909–1915. [Google Scholar] [CrossRef] [PubMed]
- Narula, N.; Marshall, J.K.; Colombel, J.F.; Leontiadis, G.I.; Williams, J.G.; Muqtadir, Z.; Reinisch, W. Systematic Review and Meta-Analysis: Infliximab or Cyclosporine as Rescue Therapy in Patients with Severe Ulcerative Colitis Refractory to Steroids. Am. J. Gastroenterol. 2016, 111, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Irvine, E.J.; Yeh, C.H.; Ramsey, D.; Stirling, A.L.; Higgins, P.D. The effect of mesalazine therapy on quality of life in patients with mildly and moderately active ulcerative colitis. Aliment. Pharmacol Ther. 2008, 28, 1278–1286. [Google Scholar] [CrossRef]
- Janke, K.H.; Klump, B.; Gregor, M.; Meisner, C.; Haeuser, W. Determinants of life satisfaction in inflammatory bowel disease. Inflamm. Bowel Dis. 2005, 11, 272–286. [Google Scholar] [CrossRef]
- Salehimarzijarani, B.; Jalaly, N.Y.; Dadvar, Z.; Hemmasi, G.; Ashrafi, M.; Zali, M. Long-term quality of life after ileal pouch anal restorative proctocolectomy for ulcerative colitis. Indian J. Gastroenterol. 2013, 32, 49–53. [Google Scholar] [CrossRef]
- Weinryb, R.M.; Liljeqvist, L.; Poppen, B.; Gustavsson, J.P. A longitudinal study of long-term quality of life after ileal pouch-anal anastomosis. Am. J. Surg. 2003, 185, 333–338. [Google Scholar] [CrossRef]
- Carcamo, L.; Miranda, P.; Zuniga, A.; Alexander, E.; Molina, M.E.; Urrejola, G.; Larach, T.; Miguieles, R.; Bellolio, F. Ileal pouch-anal anastomosis in ulcerative colitis: Outcomes, functional results, and quality of life in patients with more than 10-year follow-up. Int. J. Colorectal Dis. 2020, 35, 747–753. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Infliximab (n = 135) | Ciclosporin (n = 135) |
|---|---|---|
| Age at randomisation (years), mean (SD) (n) | 39.3 (15.5) (135) | 39.8 (15.0) (135) |
| Gender: proportion, n (%) | ||
| Female Male | 46/135 (34.1) 89/135 (65.9) | 54/135 (40.0) 81/135 (60.0) |
| Ethnicity: proportion, n (%) | ||
| White Asian or Asian British Black or Black British Other ethnic groups | 126/134 (94.0) 5/134 (3.7) 2/134 (1.5) 1/134 (0.7) | 134/133 (63.2) 7/133 (5.3) 1/133 (0.8) 1/133 (0.8) |
| Weight (kg), mean (SD) (n) | 74.3 (15.0) (135) | 73.9 (15.3) (134) |
| Smoking: proportion, n (%) | ||
| Never smoked/nonsmoker Current/ex-smoker | 58/130 (44.6) 72/130 (55.4) | 75/134 (56.0) 59/134 (44.0) |
| Family history: proportion, n (%) | ||
| Yes (any one of mother, father, siblings, child) No | 28/132 (21.2) 104/132 (78.8) | 19/135 (14.1) 116/135 (85.9) |
| Condition severity (using TrueLove and Witts criteria [19]): proportion, n (%) | ||
| Severe Not severe | 97/133 (72.9) 36/133 (27.1) | 95/131 (72.5) 36/131 (27.5) |
| Montreal score: proportion, n (%) | ||
| E1 E2 E3 | 7/124 (5.6) 64/124 (51.6) 53/124 (42.7) | 10/136 (7.9) 54/126 (42.8) 62/127 (49.2) |
| Mayo score, n (%) | ||
| 0 1 2 3 | 2/131 (1.5) 2/131 (1.5) 35/131 (26.7) 92/131 (70.2) | 1/128 (0.8) 2/128 (1.6) 35/128 (27.3) 90/128 (70.3) |
| Receiving any of azathioprine, 6-mercaptopurine or methotrexate at baseline, n (%) | ||
| At least one None | 16/135 (11.9) 119 (135 (88.1) | 26/135 (19.3) 69/135 (80.7) |
| Duration of symptoms for current episode (days), mean (SD) (n) | 37.6 (46.0) (135) | 41.4 (57.5) (131) |
| Quality of Life Measure_Timepoint_Months | Infliximab | Ciclosporin | ||||
|---|---|---|---|---|---|---|
| N | Mean | SD | N | Mean | SD | |
| EQ5D_VAS_0 | 129 | 47.88 | 22.63 | 133 | 44.20 | 21.72 |
| EQ5D_VAS_3 | 96 | 69.07 | 21.46 | 97 | 65.87 | 19.87 |
| EQ5D_VAS_6 | 100 | 70.86 | 22.28 | 96 | 68.69 | 23.10 |
| EQ5D_VAS_12 | 79 | 73.47 | 20.52 | 83 | 70.46 | 26.25 |
| EQ5D_VAS_18 | 50 | 74.18 | 21.90 | 40 | 74.40 | 14.61 |
| EQ5D_VAS_24 | 39 | 68.28 | 29.18 | 40 | 71.93 | 23.10 |
| EQ5D_VAS_30 | 24 | 84.25 | 10.41 | 16 | 78.94 | 15.95 |
| EQ5D_VAS_36 | 31 | 75.55 | 18.60 | 19 | 76.58 | 18.50 |
| EQ5D_VAS_48 | 35 | 79.40 | 15.38 | 26 | 75.81 | 15.61 |
| EQ5D_VAS_60 | 25 | 72.24 | 19.25 | 27 | 75.48 | 19.53 |
| EQ5D_VAS_72 | 15 | 81.47 | 12.88 | 15 | 69.13 | 15.11 |
| ED5D_VAS_84 | 3 | 72.33 | 25.33 | 2 | 85.00 | 7.07 |
| EQ5D score_0 | 131 | 0.5172 | 0.2964 | 134 | 0.5000 | 0.3174 |
| EQ5D score _3 | 95 | 0.7990 | 0.2121 | 98 | 0.7834 | 0.2354 |
| EQ5D score _6 | 100 | 0.7954 | 0.2397 | 97 | 0.8051 | 0.2263 |
| EQ5D score _12 | 80 | 0.8052 | 0.2259 | 83 | 0.8420 | 0.2279 |
| EQ5D score _18 | 50 | 0.8265 | 0.2193 | 40 | 0.8732 | 0.1274 |
| EQ5D score _24 | 39 | 0.8563 | 0.1815 | 39 | 0.8660 | 0.1850 |
| EQ5D score _30 | 25 | 0.8522 | 0.1312 | 16 | 0.8846 | 0.1688 |
| EQ5D score _36 | 31 | 0.8080 | 0.2218 | 20 | 0.8280 | 0.2333 |
| EQ5D score _48 | 36 | 0.8473 | 0.1958 | 26 | 0.7905 | 0.2543 |
| EQ5D score _60 | 25 | 0.8398 | 0.2000 | 27 | 0.8533 | 0.1913 |
| EQ5D score _72 | 17 | 0.8456 | 0.1553 | 15 | 0.8192 | 0.1408 |
| EQ5D score _84 | 3 | 0.9083 | 0.1588 | 2 | 1.0000 | 0.0000 |
| CUCQ/CUCQ+_0 | 134 | 0.3666 | 0.1332 | 133 | 0.3574 | 0.1325 |
| CUCQ/CUCQ+_3 | 99 | 0.7455 | 0.1830 | 103 | 0.7187 | 0.1855 |
| CUCQ/CUCQ+_6 | 101 | 0.7497 | 0.1952 | 99 | 0.7505 | 0.2083 |
| CUCQ/CUCQ+_12 | 82 | 0.7284 | 0.2110 | 86 | 0.7927 | 0.1738 |
| CUCQ/CUCQ+_18 | 52 | 0.7837 | 0.1769 | 39 | 0.8179 | 0.1321 |
| CUCQ/CUCQ+_24 | 37 | 0.8051 | 0.1706 | 40 | 0.8266 | 0.1255 |
| CUCQ/CUCQ+_30 | 25 | 0.7592 | 0.1601 | 15 | 0.7981 | 0.1216 |
| CUCQ/CUCQ+_36 | 32 | 0.6730 | 0.1531 | 20 | 0.6916 | 0.1739 |
| CUCQ/CUCQ+_48 | 35 | 0.6797 | 0.1548 | 26 | 0.6835 | 0.1579 |
| CUCQ/CUCQ+_60 | 23 | 0.6848 | 0.1672 | 26 | 0.6642 | 0.1498 |
| CUCQ/CUCQ+_72 | 18 | 0.6928 | 0.1272 | 17 | 0.6447 | 0.1498 |
| CUCQ/CUCQ+_84 | 4 | 0.6325 | 0.1401 | 1 | 0.6300 | 0 |
| F Value | Significance | ||
|---|---|---|---|
| EQ5D VAS | Group Time Group*Time | 0.23 29.73 0.54 | 0.63 0.00 * 0.88 |
| EQ5D score | Group Time Group*Time | 0.26 33.85 0.35 | 0.61 0.00 * 0.97 |
| CUCQ/CUCQ+ | Group Time Group*Time | 0.10 102.59 0.90 | 0.75 0.00 * 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alrubaiy, L.; Hutchings, H.A.; Louca, A.; Rapport, F.; Watkins, A.; Sebastian, S.; Williams, J.G. Quality of Life in Patients with Acute Severe Ulcerative Colitis: Long-Term Follow-Up Results from the CONSTRUCT Trial. J. Pers. Med. 2022, 12, 2039. https://doi.org/10.3390/jpm12122039
Alrubaiy L, Hutchings HA, Louca A, Rapport F, Watkins A, Sebastian S, Williams JG. Quality of Life in Patients with Acute Severe Ulcerative Colitis: Long-Term Follow-Up Results from the CONSTRUCT Trial. Journal of Personalized Medicine. 2022; 12(12):2039. https://doi.org/10.3390/jpm12122039
Chicago/Turabian StyleAlrubaiy, Laith, Hayley A. Hutchings, Andrea Louca, Frances Rapport, Alan Watkins, Shaji Sebastian, and John G. Williams. 2022. "Quality of Life in Patients with Acute Severe Ulcerative Colitis: Long-Term Follow-Up Results from the CONSTRUCT Trial" Journal of Personalized Medicine 12, no. 12: 2039. https://doi.org/10.3390/jpm12122039
APA StyleAlrubaiy, L., Hutchings, H. A., Louca, A., Rapport, F., Watkins, A., Sebastian, S., & Williams, J. G. (2022). Quality of Life in Patients with Acute Severe Ulcerative Colitis: Long-Term Follow-Up Results from the CONSTRUCT Trial. Journal of Personalized Medicine, 12(12), 2039. https://doi.org/10.3390/jpm12122039