
Prolonged Use of Carnitine-Orotate Complex (Godex®) Is Associated with Improved Mortality: A Nationwide Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Study Population
2.2. Definition and Classification of Carnitine-Orotate Complex Intake
2.3. Study Outcomes
2.4. Other Measurements and Definitions
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Study Subjects
3.2. The Risk of Mortality, LC, HCC, and the Composite Outcome According to the Duration of Carnitine-Orotate Complex Use
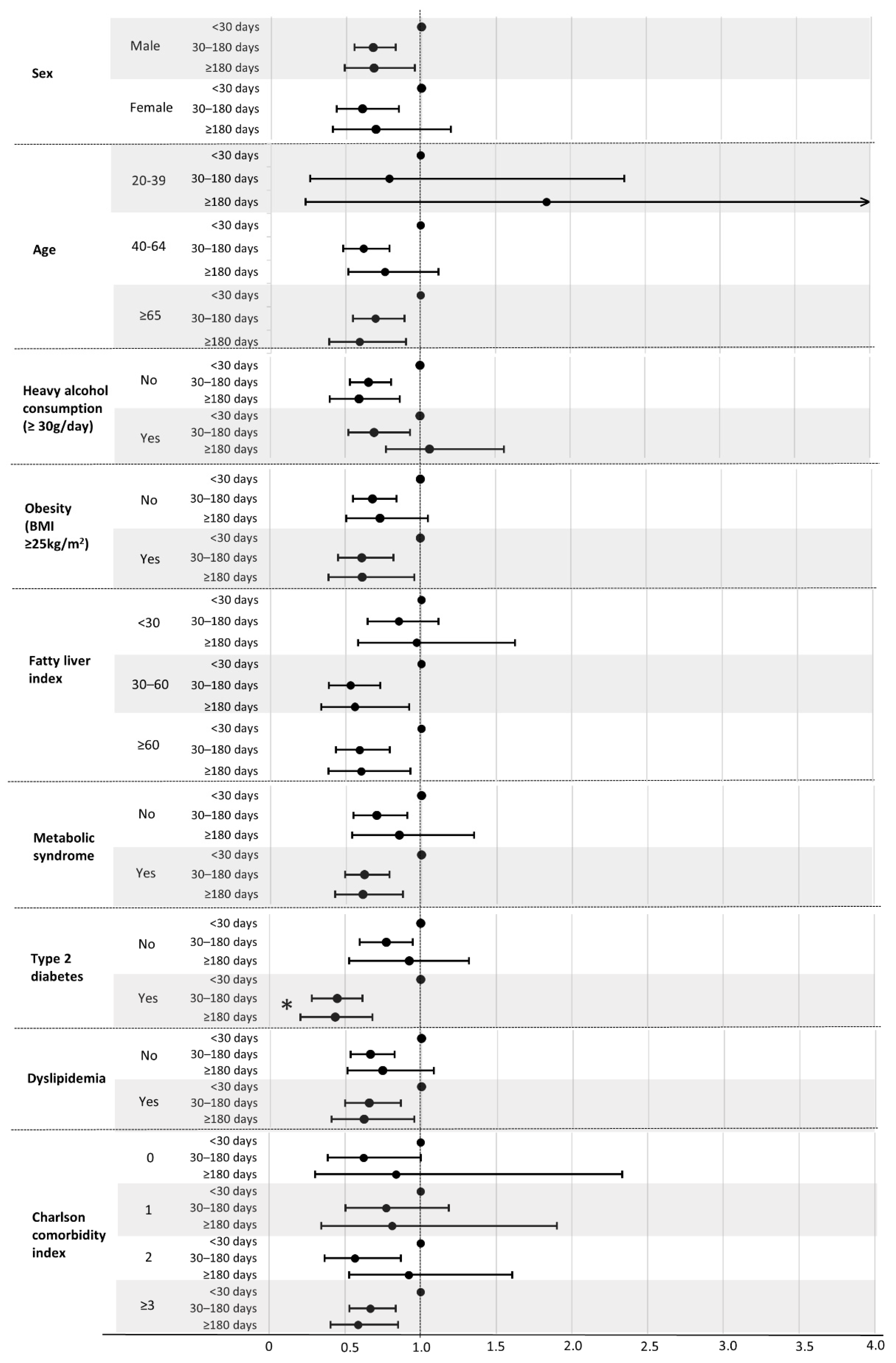
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Total (n) | Events (n) | Person Years | IR a | HR (95% CI) | |||
|---|---|---|---|---|---|---|---|
| Model 1 b | Model 2 c | Model 3 d | |||||
| Cardiovascular mortality | |||||||
| <30 days | 6246 | 65 | 27,311 | 2.38 | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 30 | 24,390 | 1.23 | 0.64 (0.42–1.00) | 0.64 (0.39–0.97) | 0.61 (0.39–0.97) |
| ≥180 days | 1382 | 6 | 5505 | 1.09 | 0.42 (0.18–0.96) | 0.38 (0.16–0.88) | 0.29 (0.11–0.72) |
| p for trend | 0.032 | 0.023 | 0.010 | ||||
| Respiratory mortality | |||||||
| <30 days | 6246 | 38 | 27,338 | 1.39 | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 13 | 24,528 | 0.53 | 0.51 (0.27–0.97) | 0.52 (0.27–0.99) | 0.54 (0.28–1.06) |
| ≥180 days | 1382 | 5 | 5495 | 0.91 | 0.60 (0.23–1.52) | 0.55 (0.21–1.43) | 0.53 (0.18–1.56) |
| p for trend | 0.091 | 0.094 | 0.157 | ||||
| HCC mortality | |||||||
| <30 days | 6246 | 22 | 27,160 | 0.81 | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 19 | 24,359 | 0.78 | 1.08 (0.58–2.00) | 1.11 (0.59–2.09) | 0.95 (0.50–1.8) |
| ≥180 days | 1382 | 6 | 5505 | 1.09 | 1.17 (0.48–2.89) | 1.15 (0.45–2.92) | 1.27 (0.48–3.38) |
| p for trend | 0.937 | 0.929 | 0.838 | ||||
| Lung cancer mortality | |||||||
| <30 days | 6246 | 39 | 27,273 | 1.43 | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 18 | 24,324 | 0.74 | 0.58 (0.33–1.02) | 0.65 (0.37–1.15) | 0.79 (0.44–1.43) |
| ≥180 days | 1382 | 5 | 5495 | 0.91 | 0.53 (0.21–1.34) | 0.61 (0.23–1.58) | 0.82 (0.29–2.35) |
| p for trend | 0.102 | 0.257 | 0.732 | ||||
References
- Jun, D.W.; Kim, B.I.; Cho, Y.K.; Kim, H.J.; Kwon, Y.O.; Park, S.Y.; Han, S.Y.; Baek, Y.H.; Jung, Y.J.; Kim, H.Y.; et al. Efficacy and Safety of Entecavir plus Carnitine Complex (GODEX®) Compared to Entecavir Monotherapy in Patient with ALT Elevated Chronic Hepatitis B: Randomized, Multicenter Open-Label Trials. The GOAL Study. Clin. Mol. Hepatol. 2013, 19, 165–172. [Google Scholar] [CrossRef]
- Sin, J.S.; Jung, E.Y.; Lee, M.H.; Kang, J.K. Therapeutic Effect of the Godex on the Liver Cirrhosis Induced by CCl4 and Ethanol in the Rat. J. Appl. Pharmacol. 2002, 10, 200–207. [Google Scholar]
- Park, M.-S.; Kang, J.-S.; Chon, C.-Y.; Paik, S.-W.; Rim, K.-S.; Kwak, M.-J.; Jeon, Y.-C.; Lee, M.-H. Oral Godex Capsule for Chronic Liver Disease:A Double-Blind, Randomized, Multicenter Controlled Trial. J. Korean Soc. Clin. Pharmacol. Ther. 2001, 9, 151–162. [Google Scholar] [CrossRef]
- Hong, E.S.; Kim, E.K.; Kang, S.M.; Khang, A.R.; Choi, S.H.; Park, K.S.; Jang, H.C.; Lim, S. Effect of Carnitine-Orotate Complex on Glucose Metabolism and Fatty Liver: A Double-Blind, Placebo-Controlled Study. J. Gastroenterol. Hepatol. 2014, 29, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.C.; Lee, W.Y.; Yoon, K.H.; Park, J.Y.; Son, H.S.; Han, K.A.; Lee, K.W.; Woo, J.T.; Ju, Y.C.; Lee, W.J.; et al. Improvement of Nonalcoholic Fatty Liver Disease with Carnitine-Orotate Complex in Type 2 Diabetes (CORONA): A Randomized Controlled Trial. Diabetes Care 2015, 38, 1245–1252. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.H.; Lee, M.K. Carnitine Orotate Complex Ameliorates Insulin Resistance and Hepatic Steatosis through Carnitine Acetyltransferase Pathway. Diabetes Metab. J. 2021, 45, 933–947. [Google Scholar] [CrossRef]
- Ringseis, R.; Keller, J.; Eder, K. Role of Carnitine in the Regulation of Glucose Homeostasis and Insulin Sensitivity: Evidence from in Vivo and in Vitro Studies with Carnitine Supplementation and Carnitine Deficiency. Eur. J. Nutr. 2012, 51, 1–18. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; Lavie, C.J.; Fares, H.; Menezes, A.R.; O’Keefe, J.H. L-Carnitine in the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-Analysis. Mayo Clin. Proc. 2013, 88, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Yahyapoor, F.; Pahlavani, N.; Karbin, K.; Sedaghat, A.; Khadem-rezaiyan, M.; Arabi, M.; Hejri Zarifi, S.; Norouzy, A. L-Carnitine Effects on Clinical Status and Mortality Rate in Septic Patients: A Systematic Literature Review. J. Nutr. Health 2020, 9, 14–22. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Sato, M.; Ohashi, H.; Araki, H.; Tadokoro, M.; Osumi, Y.; Ito, H.; Morita, H.; Amano, I. Effects of L-Carnitine Supplementation on Cardiac Morbidity in Hemodialyzed Patients. Am. J. Nephrol. 2000, 20, 201–207. [Google Scholar] [CrossRef]
- Miwa, T.; Hanai, T.; Nishimura, K.; Sakai, Y.; Imai, K.; Suetsugu, A.; Takai, K.; Shiraki, M.; Katsukura, N.; Shimizu, M. Survival Benefit of L-Carnitine Supplementation in Patients with Cirrhosis. J. Parenter. Enter. Nutr. 2022, 46, 1326–1334. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.Y.; Khang, Y.H.; Park, J.H.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Bang, J.H.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef] [Green Version]
- WHO Expert Consultation. Appropriate Body-Mass Index for Asian Populations and Its Implications for Policy and Intervention Strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Shin, C.; Baik, I. Associations Between Alcohol Consumption and Leukocyte Telomere Length Modified by a Common Polymorphism of ALDH 2. Alcohol. Clin. Exp. Res. 2016, 40, 765–771. [Google Scholar] [CrossRef]
- Xin, X.; He, J.; Frontini, M.G.; Ogden, L.G.; Motsamai, O.I.; Whelton, P.K. Effects of Alcohol Reduction on Blood Pressure: A Meta-Analysis of Randomized Controlled Trials. Hypertension 2001, 38, 1112–1117. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.-Y.; Kang, S.M.; Kang, J.-H.; Kang, S.Y.; Kim, K.K.; Kim, K.-B.; Kim, B.; Kim, S.J.; Kim, Y.-H.; Kim, J.-H.; et al. 2020 Korean Society for the Study of Obesity Guidelines for the Management of Obesity in Korea. J. Obes. Metab. Syndr. 2021, 30, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A Simple and Accurate Predictor of Hepatic Steatosis in the General Population. BMC Gastroenterol. 2006, 6, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Bremer, J. Carnitine--Metabolism and Functions. Physiol. Rev. 1983, 63, 1420–1480. [Google Scholar] [CrossRef]
- Lemarie, A.; Huc, L.; Pazarentzos, E.; Mahul-Mellier, A.-L.; Grimm, S. Specific Disintegration of Complex II Succinate: Ubiquinone Oxidoreductase Links PH Changes to Oxidative Stress for Apoptosis Induction. Cell Death Differ. 2011, 18, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Giorgio, M.; Migliaccio, E.; Orsini, F.; Paolucci, D.; Moroni, M.; Contursi, C.; Pelliccia, G.; Luzi, L.; Minucci, S.; Marcaccio, M. Electron Transfer between Cytochrome c and P66Shc Generates Reactive Oxygen Species That Trigger Mitochondrial Apoptosis. Cell 2005, 122, 221–233. [Google Scholar] [CrossRef]
- Brdiczka, D.G.; Zorov, D.B.; Sheu, S.-S. Mitochondrial Contact Sites: Their Role in Energy Metabolism and Apoptosis. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2006, 1762, 148–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valko, M.; Izakovic, M.; Mazur, M.; Rhodes, C.J.; Telser, J. Role of Oxygen Radicals in DNA Damage and Cancer Incidence. Mol. Cell. Biochem. 2004, 266, 37–56. [Google Scholar] [CrossRef] [PubMed]
- Bakeeva, L.E.; Barskov, I.V.; Egorov, M.V.; Isaev, N.K.; Kapelko, V.I.; Kazachenko, A.V.; Kirpatovsky, V.I.; Kozlovsky, S.V.; Lakomkin, V.L.; Levina, S.B. Mitochondria-Targeted Plastoquinone Derivatives as Tools to Interrupt Execution of the Aging Program. 2. Treatment of Some ROS-and Age-Related Diseases (Heart Arrhythmia, Heart Infarctions, Kidney Ischemia, and Stroke). Biochemistry 2008, 73, 1288–1299. [Google Scholar] [CrossRef]
- Ye, J.; Li, J.; Yu, Y.; Wei, Q.; Deng, W.; Yu, L. L-Carnitine Attenuates Oxidant Injury in HK-2 Cells via ROS-Mitochondria Pathway. Regul. Pept. 2010, 161, 58–66. [Google Scholar] [CrossRef]
- El-Beshbishy, H.A. The Effect of Dimethyl Dimethoxy Biphenyl Dicarboxylate (DDB) against Tamoxifen-Induced Liver Injury in Rats: DDB Use Is Curative or Protective. BMB Rep. 2005, 38, 300–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morsy, M.A.; Ibrahim, M.A.; Abd-Elghany, M.I. Dimethyl Dimethoxy Biphenyl Dicarboxylate Attenuates Hepatic and Metabolic Alterations in High Fructose-Fed Rats. Toxicol. Ind. Health 2016, 32, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Szendroedi, J.; Schmid, A.I.; Chmelik, M.; Toth, C.; Brehm, A.; Krssak, M.; Nowotny, P.; Wolzt, M.; Waldhausl, W.; Roden, M. Muscle Mitochondrial ATP Synthesis and Glucose Transport/Phosphorylation in Type 2 Diabetes. PLoS Med. 2007, 4, e154. [Google Scholar] [CrossRef]
- Abdelmalek, M.F.; Lazo, M.; Horska, A.; Bonekamp, S.; Lipkin, E.W.; Balasubramanyam, A.; Bantle, J.P.; Johnson, R.J.; Diehl, A.M.; Clark, J.M. Higher Dietary Fructose Is Associated with Impaired Hepatic Adenosine Triphosphate Homeostasis in Obese Individuals with Type 2 Diabetes. Hepatology 2012, 56, 952–960. [Google Scholar] [CrossRef] [Green Version]
- Gariani, K.; Menzies, K.J.; Ryu, D.; Wegner, C.J.; Wang, X.; Ropelle, E.R.; Moullan, N.; Zhang, H.; Perino, A.; Lemos, V. Eliciting the Mitochondrial Unfolded Protein Response by Nicotinamide Adenine Dinucleotide Repletion Reverses Fatty Liver Disease in Mice. Hepatology 2016, 63, 1190–1204. [Google Scholar] [CrossRef]
- Matilainen, J.; Mustonen, A.-M.; Rilla, K.; Käkelä, R.; Sihvo, S.P.; Nieminen, P. Orotic Acid-Treated Hepatocellular Carcinoma Cells Resist Steatosis by Modification of Fatty Acid Metabolism. Lipids Health Dis. 2020, 19, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, X.; Liu, C.; Xue, Y.; Wang, J.; Xue, C.; Yanagita, T.; Gao, X.; Wang, Y. Long-Term Fatty Liver-Induced Insulin Resistance in Orotic Acid-Induced Nonalcoholic Fatty Liver Rats. Biosci. Biotechnol. Biochem. 2016, 80, 735–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, S.M. Hypertriglyceridemia, Insulin Resistance, and the Metabolic Syndrome. Am. J. Cardiol. 1999, 83, 25–29. [Google Scholar] [CrossRef]
- Kendall, D.M.; Harmel, A.P. The Metabolic Syndrome, Type 2 Diabetes, and Cardiovascular Disease: Understanding the Role of Insulin Resistance. Am. J. Manag. Care 2002, 8, S635–S653. [Google Scholar] [PubMed]
- Zhang, L.; Keung, W.; Samokhvalov, V.; Wang, W.; Lopaschuk, G.D. Role of Fatty Acid Uptake and Fatty Acid β-Oxidation in Mediating Insulin Resistance in Heart and Skeletal Muscle. Biochim. Biophys. Acta (BBA)-Mol. Cell Biol. Lipids 2010, 1801, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Portincasa, P.; Grattagliano, I.; Palmieri, V.O.; Palasciano, G. Nonalcoholic Steatohepatitis: Recent Advances from Experimental Models to Clinical Management. Clin. Biochem. 2005, 38, 203–217. [Google Scholar] [CrossRef]
- M Victor, V.; Rocha, M.; Herance, R.; Hernandez-Mijares, A. Oxidative Stress and Mitochondrial Dysfunction in Type 2 Diabetes. Curr. Pharm. Des. 2011, 17, 3947–3958. [Google Scholar] [CrossRef]
- Mingrone, G. Carnitine in Type 2 Diabetes. Ann. N. Y. Acad. Sci. 2004, 1033, 99–107. [Google Scholar] [CrossRef] [PubMed]
- OKUDA, Y.; KAWAI, K.; MURAYAMA, Y.; YAMASHITA, K. Postprandial Changes in Plasma Ketone Body and Carnitine Levels in Normal and Non-Insulin-Dependent Diabetic Subjects. Endocrinol. Jpn. 1987, 34, 415–422. [Google Scholar] [CrossRef] [Green Version]
- Onishi, H.; Yoshida, I. Rapid Change in Japanese Medical Education. Med. Teach. 2004, 26, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Arduini, A.; Bonomini, M.; Savica, V.; Amato, A.; Zammit, V. Carnitine in Metabolic Disease: Potential for Pharmacological Intervention. Pharmacol. Ther. 2008, 120, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Demarquoy, J.; Georges, B.; Rigault, C.; Royer, M.-C.; Clairet, A.; Soty, M.; Lekounoungou, S.; Le Borgne, F. Radioisotopic Determination of L-Carnitine Content in Foods Commonly Eaten in Western Countries. Food Chem. 2004, 86, 137–142. [Google Scholar] [CrossRef]
- Kępka, A.; Zwierz, P.; Chojnowska, S.; Ochocińska, A.; Skorupa, E.; Szczepański, M.; Szajda, S.D.; Waszkiewicz, N. Relation of Plasma Carnitine and Aminotransferases to Alcohol Dose and Time of Dependence. Alcohol 2019, 81, 62–69. [Google Scholar] [CrossRef] [PubMed]


| Duration of Carnitine-Orotate Complex Use | p-Value | ||||
|---|---|---|---|---|---|
| Total | <30 Days | 30–180 Days | ≥180 Days | ||
| n | 13,413 | 6246 | 5785 | 1382 | |
| Age, years | 51.97 ± 12.94 | 52.27 ± 13.79 | 51 ± 12.24 | 54.63 ± 11.26 | <0.001 |
| Age, n (%) | <0.001 | ||||
| 20–39 | 2390 (17.8) | 1210 (19.4) | 1059 (18.3) | 121 (8.8) | |
| 40–64 | 8770 (65.4) | 3833 (61.4) | 3932 (68.0) | 1005 (72.7) | |
| ≥65 | 2253 (16.8) | 1203 (19.2) | 794 (13.7) | 256 (18.5) | |
| Male sex, n (%) | 8769 (65.4) | 3794 (60.7) | 3985 (68.9) | 990 (71.6) | <0.001 |
| Current smoker, n (%) | 3833 (28.6) | 1710 (27.4) | 1720 (29.7) | 403 (29.2) | <0.001 |
| Heavy alcohol drinker, n (%) | 1844 (13.8) | 715 (11.5) | 888 (15.4) | 241 (17.4) | <0.001 |
| Regular exerciser, n (%) | 2542 (19.0) | 1190 (19.1) | 1103 (19.1) | 249 (18.0) | 0.645 |
| Low income, n (%) | 2064 (15.4) | 976 (15.6) | 859 (14.9) | 229 (16.6) | 0.218 |
| BMI, kg/m2 | 25.6 ± 3.9 | 24.9 ± 3.7 | 25.99 ± 3.83 | 26.6 ± 4.04 | <0.001 |
| Waist circumference, cm | 85.85 ± 9.79 | 84.07 ± 9.57 | 87.02 ± 9.66 | 89.05 ± 9.77 | <0.001 |
| Systolic BP, mmHg | 126.64 ± 15.2 | 125.42 ± 15.32 | 127.2 ± 14.9 | 129.77 ± 15.32 | <0.001 |
| Diastolic BP, mmHg | 78.99 ± 10.39 | 78.09 ± 10.34 | 79.59 ± 10.37 | 80.56 ± 10.33 | <0.001 |
| Total cholesterol, mg/dL | 200.2 ± 42.93 | 199.67 ± 40.91 | 202.97 ± 43.94 | 190.94 ± 46.11 | <0.001 |
| Triglycerides, mg/dL a | 141 (95–210) | 127 (86–189) | 152 (104–223) | 156 (109–232) | <0.001 |
| HDL cholesterol, mg/dL | 52.88 ± 17.58 | 54.0 ± 17.8 | 51.9 ± 18 | 51.4 ± 14.3 | <0.001 |
| LDL cholesterol, mg/dL | 114.77 ± 40.25 | 115.7 ± 37.5 | 116.4 ± 42.3 | 103.7 ± 41.5 | <0.001 |
| Fasting glucose, mg/dL | 108.2 ± 32.44 | 104.1 ± 28.9 | 110 ± 33.5 | 119.4 ± 38.8 | <0.001 |
| Aspartate transaminase, U/L a | 35 (25–54) | 31 (19–58) | 53 (30–82) | 51 (28–80) | <0.001 |
| Alanine transferase, U/L a | 42 (23–72) | 29 (22–43) | 40 (28–60) | 47 (33–68) | <0.001 |
| Metabolic syndrome | 7837 (58.4) | 3072 (49.2) | 3674 (63.5) | 1091 (78.9) | <0.001 |
| Hypertension | 6125 (45.7) | 2480 (39.7) | 2722 (47.1) | 923 (66.8) | <0.001 |
| Diabetes mellitus | 3042 (22.7) | 1028 (16.5) | 1408 (24.3) | 606 (43.9) | <0.001 |
| Dyslipidemia | 5733 (42.7) | 2194 (35.1) | 2698 (46.6) | 841 (60.9) | <0.001 |
| Fatty liver index | <0.001 | ||||
| 0–30 | 4009 (29.9) | 2580 (41.31) | 1239 (21.42) | 190 (13.75) | |
| 30–60 | 3863 (28.8) | 1763 (28.23) | 1722 (29.77) | 378 (27.35) | |
| ≥60 | 5541 (41.3) | 1903 (30.47) | 2824 (48.82) | 814 (58.9) | |
| Charlson comorbidity index | <0.001 | ||||
| 0 | 2796 (20.9) | 1592 (25.5) | 1092 (18.9) | 112 (8.1) | |
| 1 | 3306 (24.7) | 1527 (24.5) | 1531 (26.5) | 248 (18.0) | |
| 2 | 2738 (20.4) | 1151 (18.4) | 1245 (21.5) | 342 (24.8) | |
| ≥3 | 4573 (34.1) | 1976 (31.6) | 1917 (33.1) | 680 (49.1) | |
| Use of carnitine-orotate complex within 1-year prior to the health check-up, n (%) | 1879 (14.0) | 346 (5.5) | 914 (15.8) | 619 (44.8) | |
| Total (n) | Events (n) | Person Years | IR a | HR (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| Model 1 b | Model 2 c | Model 3 d | Model 4 e | |||||
| All-cause mortality | ||||||||
| <30 days | 6246 | 441 | 27,299 | 16.15 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 203 | 24,317 | 8.35 | 0.51 (0.44–0.61) | 0.59 (0.50–0.70) | 0.63 (0.52–0.74) | 0.66 (0.55–0.79) |
| ≥180 days | 1382 | 64 | 5501 | 11.63 | 0.72 (0.55–0.93) | 0.63 (0.48–0.82) | 0.64 (0.49–0.84) | 0.69 (0.51–0.92) |
| p for trend | <0.001 | <0.001 | <0.001 | <0.001 | ||||
| LC | ||||||||
| <30 days | 6246 | 137 | 26,862 | 5.10 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 163 | 23,855 | 6.83 | 1.34 (1.06–1.68) | 1.37 (1.09–1.72) | 1.44 (1.14–1.81) | 1.14 (0.90–1.44) |
| ≥180 days | 1382 | 72 | 5310 | 13.56 | 2.64 (1.98–3.51) | 2.35 (1.77–3.13) | 2.49 (1.84–3.37) | 1.61 (1.17–2.21) |
| p for trend | <0.001 | <0.001 | <0.001 | 0.015 | ||||
| HCC | ||||||||
| <30 days | 6246 | 28 | 27,237 | 1.03 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 26 | 24,256 | 1.07 | 1.05 (0.62–1.79) | 1.08 (0.63–1.84) | 1.12 (0.65–1.92) | 0.85 (0.49–1.47) |
| ≥180 days | 1382 | 20 | 5462 | 3.66 | 3.61 (2.04–6.41) | 2.94 (1.65–5.22) | 2.99 (1.63–5.49) | 2.13 (1.11–4.08) |
| p for trend | <0.001 | <0.001 | <0.001 | 0.015 | ||||
| Composite all-cause mortality, LC, and HCC | ||||||||
| <30 days | 6246 | 559 | 26,828 | 20.84 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| 30–180 days | 5785 | 348 | 23,827 | 14.61 | 0.70 (0.61–0.80) | 0.77 (0.67–0.88) | 0.81 (0.71–0.93) | 0.76 (0.66–0.87) |
| ≥180 days | 1382 | 123 | 5293 | 23.24 | 1.10 (0.91–1.34) | 0.97 (0.80–1.18) | 0.99 (0.82–1.22) | 0.84 (0.67–1.04) |
| p for trend | <0.001 | 0.001 | 0.008 | 0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.-Y.; Hong, S.; Kim, K.-S.; Han, K.; Park, C.-Y. Prolonged Use of Carnitine-Orotate Complex (Godex®) Is Associated with Improved Mortality: A Nationwide Cohort Study. J. Pers. Med. 2022, 12, 1970. https://doi.org/10.3390/jpm12121970
Park K-Y, Hong S, Kim K-S, Han K, Park C-Y. Prolonged Use of Carnitine-Orotate Complex (Godex®) Is Associated with Improved Mortality: A Nationwide Cohort Study. Journal of Personalized Medicine. 2022; 12(12):1970. https://doi.org/10.3390/jpm12121970
Chicago/Turabian StylePark, Kye-Yeung, Sangmo Hong, Kyung-Soo Kim, Kyungdo Han, and Cheol-Young Park. 2022. "Prolonged Use of Carnitine-Orotate Complex (Godex®) Is Associated with Improved Mortality: A Nationwide Cohort Study" Journal of Personalized Medicine 12, no. 12: 1970. https://doi.org/10.3390/jpm12121970
APA StylePark, K.-Y., Hong, S., Kim, K.-S., Han, K., & Park, C.-Y. (2022). Prolonged Use of Carnitine-Orotate Complex (Godex®) Is Associated with Improved Mortality: A Nationwide Cohort Study. Journal of Personalized Medicine, 12(12), 1970. https://doi.org/10.3390/jpm12121970