

A Preliminary Study of Interdisciplinary Approach with a Single-Stage Surgery in Children with Cleft Lip and Palate
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgical Techniques
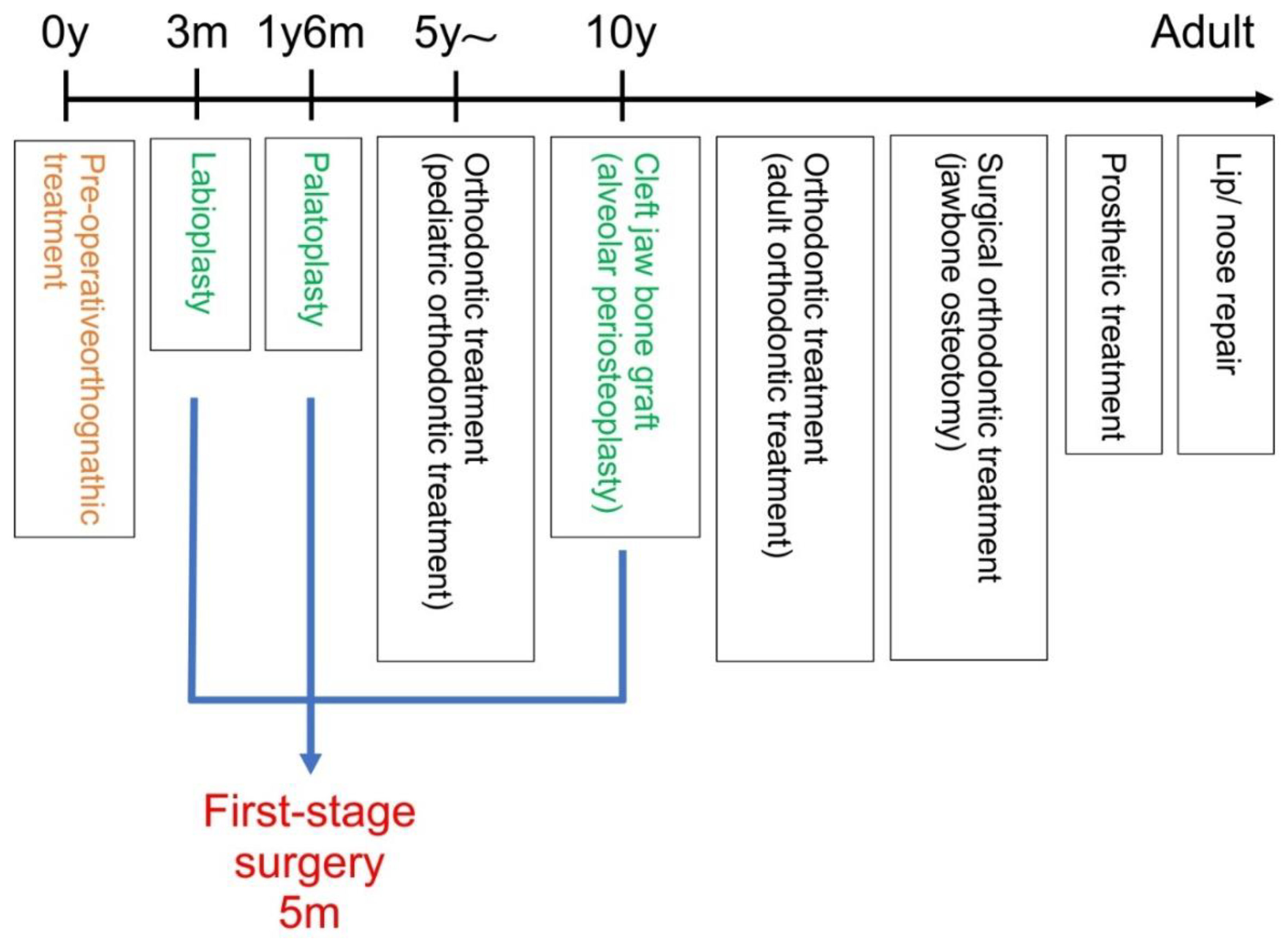
2.2.1. Single-Stage Surgery
2.2.2. Two-Stage Surgery
2.3. Preoperative Orthognathic Treatment
2.3.1. Intraoral: Molding Plate
2.3.2. Extraoral: Orthodontic Elastics and Medical Tape
2.4. Analyses
2.4.1. Measurement Points in the Lateral Cephalometric Radiographs (Figure 5)
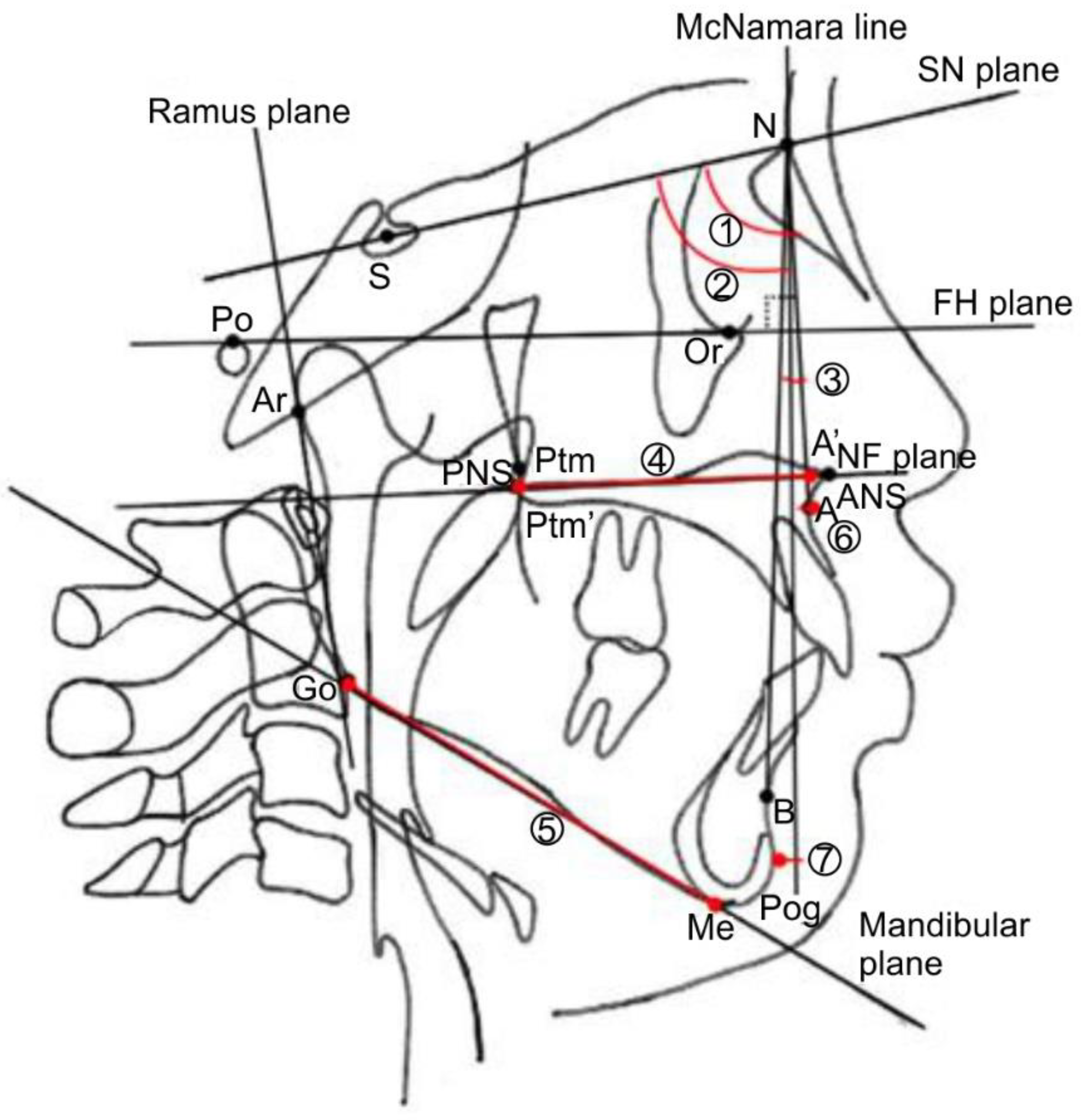
2.4.2. Measurement Planes in Lateral Cephalometric Radiographs (Figure 5)
2.4.3. Measurement Sites on Lateral Cephalometric Radiographs (Figure 5)
- ①
- SNA angle: angle between the SN plane and straight-line NA.
- ②
- SNB angle: angle between the SN plane and the straight-line NB.
- ③
- ANB angle: angle between the straight lines AN and NB.
- ④
- A’-Ptm’: maxillary length.
- ⑤
- Go-Me: mandibular body length.
- ⑥
- A to the McNamara line: distance from the McNamara line to point A.
- ⑦
- Pog to McNamara line: distance from the McNamara line to Pog.
2.4.4. Measurement Sites in the Dentition Model (Figure 6)
- ①
- Anterior width of the dental arch: distance between the maxillary left and right deciduous canines.
- ②
- Posterior width of the dental arch: distance between the maxillary left and right second deciduous molars.
- ③
- Anterior length of the dental arch: distance from the labial surface of the maxillary central incisor to the maxillary left and right deciduous canines.
- ④
- Posterior length of dental arch: distance from the labial surface of the maxillary central incisor to the maxillary left and right second deciduous molars.

2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Preoperative Orthognathic Treatment
4.2. Single-Stage Surgery
4.3. Efficacy Compared with Two-Stage Surgery Based on Measurement Results
4.4. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torikai, K.; Hirakawa, T.; Kijima, T.; Oomura, S.; Yamamoto, M.; Naganishi, H. Primary alveolar bone grafting and gingivoperiosteoplasty or gingivomucoperiosteal flap at the time of 1-stage repair of unilateral cleft lip and palate. J. Craniofac. Surg. 2009, 20, 1729–1732. [Google Scholar] [CrossRef]
- Grayson, B.H.; Santiago, P.E.; Brecht, L.E.; Cutting, C.B. Presurgical nasoalveolar molding in infants with cleft lip and palate. Cleft Palate Craniofac. J. 1999, 36, 486–498. [Google Scholar] [CrossRef] [PubMed]
- McNeil, C.K. Oral and Facial Deformity; Pitman Medical Publishers: London, UK, 1954. [Google Scholar]
- Barillas, I.; Dec, W.; Warren, S.M.; Cutting, C.B.; Grayson, B.H. Nasoalveolar molding improves long-term nasal symmetry in complete unilateral cleft lip-cleft palate patients. Plast. Reconstr. Surg. 2009, 123, 1002–1006. [Google Scholar] [CrossRef]
- Bongaarts, C.A.M.; Prahl-Andersen, B.; Bronkhorst, E.M.; Spauwen, P.H.M.; Mulder, J.W.; Vaandrager, J.M.; Kuijpers-Jagtman, A.M. Effect of infant orthopedics on facial appearance of toddlers with complete unilateral cleft lip and palate (Dutchcheft). Cleft Palate Craniofac. J. 2008, 45, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Furlow, L.T., Jr. Cleft palate repair by double opposing Z-plasty. Plast. Reconstr. Surg. 1986, 78, 724–738. [Google Scholar] [CrossRef] [PubMed]
- Santiago, P.E.; Grayson, B.H.; Cutting, C.B.; Gianoutsos, M.P.; Brecht, L.E.; Kwon, S.M. Reduced need for alveolar bone grafting by presurgical orthopedics and primary gingivoperiosteoplasty. Cleft Palate Craniofac. J. 1998, 35, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Millard, D.R.; Latham, R.; Huifen, X.; Spiro, S.; Morovic, C. Cleft lip and palate treated by presurgical orthopedics, gingivoperiosteoplasty, and lip adhesion (POPLA) compared with previous lip adhesion method: A preliminary study of serial dental casts. Plast. Reconstr. Surg. 1999, 103, 1630–1644. [Google Scholar] [CrossRef]
- Kaplan, E.N. Soft palate repair by levator muscle reconstruction and a buccal mucosal flap. Plast. Reconstr. Surg. 1975, 56, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Cronin, T.D.; Brauer, R.O.; Alexander, J.T.; Taylor, W.G. Push-back repair using nasal muscosal flaps: Results. Cleft Palate J. 1964, 35, 269–274. [Google Scholar]
- Bongaarts, C.A.M.; Kuijpers-Jagtman, A.M.; van’t Hof, M.A.; Prahl-Andersen, B. The effect of infant orthopedics on the occlusion of the deciduous dentition in children with complete unilateral cleft lip and palate (Dutchcleft). Cleft Palate Craniofac. J. 2004, 41, 633–641. [Google Scholar] [CrossRef]
- Prahl, C.; Prahl-Andersen, B.; Van’t Hof, M.A.; Kuijpers-Jagtman, A.M. Presurgical orthopedics and satisfaction in motherhood: A randomized clinical trial (Dutchcleft). Cleft Palate Craniofac. J. 2008, 45, 284–288. [Google Scholar] [CrossRef]
- Bongaarts, C.A.M.; van ’t Hof, M.A.; Prahl-Andersen, B.; Dirks, I.V.; Kuijpers-Jagtman, A.M. Infant orthopedics has no effect on maxillary arch dimensions in the deciduous dentition of children with complete unilateral cleft lip and palate (Dutchcleft). Cleft Palate Craniofac. J. 2006, 43, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Bongaarts, C.A.M.; Prahl-Andersen, B.; Bronkhorst, E.M.; Prahl, C.; Ongkosuwito, E.M.; Borstlap, W.A.; Kuijpers-Jagtman, A.M. Infant orthopedics and facial growth in complete unilateral cleft lip and palate until six years of age (Dutchcleft). Cleft Palate Craniofac. J. 2009, 46, 654–663. [Google Scholar] [CrossRef]
- Koželj, V. Experience with presurgical nasal molding in infants with cleft lip and nose deformity. Plast. Reconstr. Surg. 2007, 120, 738–745. [Google Scholar] [CrossRef]
- Broadbent, B.H. A new X-ray technique and its application to orthodontia. Angle Orthod. 1931, 1, 45–66. [Google Scholar] [CrossRef]
- Downs, W.B. Variations in facial relationships; their significance in treatment and prognosis. Am. J. Orthod. 1948, 34, 812–840. [Google Scholar] [CrossRef]
- Graber, T.M. New horizons in case analysis—Clinical cephalometrics. Am. J. Orthod. 1952, 38, 603–624. [Google Scholar] [CrossRef]
- Hofrath, H. Die Bendeutung der Rontgenfern-und Abstandsaufnahme fur die Diagnostik der Kieferanomaline. Fortschr. Orthod. 1931, 1, 232–258. [Google Scholar]
- Atack, N.E.; Hathorn, I.S.; Semb, G.; Dowell, T.; Sandy, J.R. A new index for assessing surgical outcome in unilateral cleft lip and palate subjects aged five: Reproducibility and validity. Cleft Palate Craniofac. J. 1997, 34, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Nakamura, S.; Misaki, K.; Kudoh, M.; Fukuda, H.; Yoshida, S. Scar tissue distribution on palates and its relation to maxillary dental arch form. Cleft Palate Craniofac. J. 1998, 35, 313–319. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement Item | Single-Stage Surgery (n = 10) | Two-Stage Surgery (n = 10) | p-Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| SNA (°) | 78.92 | 1.61 | 76.78 | 2.70 | 0.035 * |
| SNB (°) | 77.45 | 3.49 | 77.43 | 3.39 | n.s. |
| ANB (°) | 1.49 | 1.95 | 4.9 | 1.95 | n.s. |
| A’–Ptm’ (mm) | 43.41 | 2.24 | 43.25 | 1.4 | 0.004 * |
| Go–Me (mm) | 53.47 | 3.72 | 61.19 | 4.08 | 0.001 * |
| A to McNamara line (mm) | −3.71 | 1.53 | −5.55 | 2.20 | 0.043 * |
| Pog to McNamara line (mm) | −10.92 | 5.67 | −9.41 | 5.59 | n.s. |
| Measurement Item | Single-Stage Surgery (n = 10) | Two-Stage Surgery (n = 10) | p-Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Anterior width of dental arch (mm) | 28.06 | 1.57 | 25.53 | 4.04 | n.s. |
| Posterior width of dental arch (mm) | 48.31 | 2.46 | 42.80 | 1.19 | 0.001 * |
| Anterior length of dental arch (mm) | 4.48 | 0.84 | 4.50 | 1.21 | n.s. |
| Posterior length of dental arch (mm) | 19.31 | 1.58 | 17.40 | 1.49 | 0.029 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumura, T.; Kawanabe, H.; Nemoto, N.; Ogino, S.; Fukui, K.; Oyama, A.; Okamoto, T. A Preliminary Study of Interdisciplinary Approach with a Single-Stage Surgery in Children with Cleft Lip and Palate. J. Pers. Med. 2022, 12, 1741. https://doi.org/10.3390/jpm12101741
Matsumura T, Kawanabe H, Nemoto N, Ogino S, Fukui K, Oyama A, Okamoto T. A Preliminary Study of Interdisciplinary Approach with a Single-Stage Surgery in Children with Cleft Lip and Palate. Journal of Personalized Medicine. 2022; 12(10):1741. https://doi.org/10.3390/jpm12101741
Chicago/Turabian StyleMatsumura, Takashi, Hitoshi Kawanabe, Naoko Nemoto, Saki Ogino, Kazunori Fukui, Akihiko Oyama, and Toru Okamoto. 2022. "A Preliminary Study of Interdisciplinary Approach with a Single-Stage Surgery in Children with Cleft Lip and Palate" Journal of Personalized Medicine 12, no. 10: 1741. https://doi.org/10.3390/jpm12101741
APA StyleMatsumura, T., Kawanabe, H., Nemoto, N., Ogino, S., Fukui, K., Oyama, A., & Okamoto, T. (2022). A Preliminary Study of Interdisciplinary Approach with a Single-Stage Surgery in Children with Cleft Lip and Palate. Journal of Personalized Medicine, 12(10), 1741. https://doi.org/10.3390/jpm12101741