


Psychiatric Symptoms in Parkinson’s Disease Patients before and One Year after Subthalamic Nucleus Deep Brain Stimulation Therapy: Role of Lead Positioning and Not of Total Electrical Energy Delivered

 , ,
, , 

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. IRB/Ethics Committee Approval and Informed Consent
2.2. Patient Population
2.3. Assessment
2.4. Treatment
2.5. Imaging
2.6. TEED Estimation
2.7. Statistical Analysis
3. Results
Gender Difference Analysis
4. Discussion
5. Study Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Aarsland, D.; Marsh, L.; Schrag, A. Neuropsychiatric symptoms in Parkinson’s disease. Mov. Disord. 2009, 24, 2175–2186. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA—J. Am. Med. Assoc. 2020, 323, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Buoli, M.; Caldiroli, A.; Altamura, A.C. Psychiatric Conditions in Parkinson Disease. J. Geriatr. Psychiatry Neurol. 2016, 29, 72–91. [Google Scholar] [CrossRef] [PubMed]
- Richard, I.H. Depression and Apathy in Parkinson’s Disease. Curr. Neurol. Neurosci. Rep. 2007, 7, 295–301. [Google Scholar] [CrossRef]
- Limousin, P.; Foltynie, T. Long-term outcomes of deep brain stimulation in Parkinson disease. Nat. Rev. Neurol. 2019, 15, 234–242. [Google Scholar] [CrossRef]
- Drapier, D.; Sauleau, P.; Haegelen, C.; Raoul, S.; Biseul, I.; Peron, J.; Lallement, F.; Rivier, I.; Reymann, J.; Edan, G.; et al. Does subthalamic nucleus stimulation induce apathy in Parkinson’s disease? J. Neurol. 2006, 253, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Accolla, E.A.; Pollo, C. Mood effects after deep brain stimulation for Parkinson’s disease: An update. Front. Neurol. 2019, 10, 617. [Google Scholar] [CrossRef]
- Nassery, A.; Palmese, C.A.; Sarva, H.; Groves, M.; Miravite, J.; Kopell, B.H. Psychiatric and Cognitive Effects of Deep Brain Stimulation for Parkinson’s Disease. Curr. Neurol. Neurosci. Rep. 2016, 16, 87. [Google Scholar] [CrossRef]
- Jahanshahi, M.; Obeso, I.; Baunez, C.; Alegre, M.; Krack, P. Parkinson’s disease, the subthalamic nucleus, inhibition, and impulsivity. Mov. Disord. 2015, 30, 128–140. [Google Scholar] [CrossRef]
- Leentjens, A.F.; Moonen, A.J.; Dujardin, K.; Marsh, L.; Martinez-Martin, P.; Richard, I.H.; Starkstein, S.E.; Köhler, S. Modeling depression in Parkinson disease: Disease-specific and nonspecific risk factors. Neurology 2013, 81, 1036–1043. [Google Scholar] [CrossRef]
- Defer, G.L.; Widner, H.; Marié, R.M.; Rémy, P.; Levivier, M. Core assessment program for surgical interventional therapies in Parkinson’s disease (CAPSIT-PD). Mov. Disord. 1999, 14, 572–584. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. Hamilton Anxiety Rating Scale (HAM-A). J. Med. 1959, 61, 601. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An Inventory for Measuring Clinical Anxiety: Psychometric Properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogullari, S. Reliability and validity of the apathy evaluation scale. Psychiatry Res. 1991, 38, 143–162. [Google Scholar] [CrossRef]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Beck, A.T.; Kovacs, M.; Weissman, A. Assessment of suicidal intention: The Scale for Suicide Ideation. J. Consult. Clin. Psychol. 1979, 47, 343–352. [Google Scholar] [CrossRef]
- Linehan, M.M.; Goodstein, J.L.; Nielsen, S.L.; Chiles, J.A. Reasons for staying alive when you are thinking of killing yourself: The reasons for living inventory. J. Consult. Clin. Psychol. 1983, 51, 276–286. [Google Scholar] [CrossRef]
- Bronstein, J.M.; Tagliati, M.; Alterman, R.L.; Lozano, A.M.; Volkmann, J.; Stefani, A.; Horak, F.B.; Okun, M.S.; Foote, K.D.; Krack, P.; et al. Deep brain stimulation for Parkinson disease an expert consensus and review of key issues. Arch. Neurol. 2011, 68, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, N.; Li, J.; Kou, H.; Wang, J.; Jing, J.; Su, M.; Li, Y.; Qu, L.; Wang, X. Optimized Deep Brain Stimulation Surgery to Avoid Vascular Damage: A Single-Center Retrospective Analysis of Path Planning for Various Deep Targets by MRI Image Fusion. Brain Sci. 2022, 12, 967. [Google Scholar] [CrossRef]
- Hell, F.; Palleis, C.; Mehrkens, J.H.; Koeglsperger, T.; Bötzel, K. Deep Brain Stimulation Programming 2.0: Future Perspectives for Target Identification and Adaptive Closed Loop Stimulation. Front. Neurol. 2019, 1, 314. [Google Scholar] [CrossRef] [PubMed]
- Merola, A.; Romagnolo, A.; Krishna, V.; Pallavaram, S.; Carcieri, S.; Goetz, S.; Mandybur, G.; Duker, A.P.; Dalm, B.; Rolston, J.D.; et al. Current Directions in Deep Brain Stimulation for Parkinson’s Disease-Directing Current to Maximize Clinical Benefit. Neurol. Ther. 2020, 9, 25–41. [Google Scholar] [CrossRef]
- Koss, A.M.; Alterman, R.L.; Tagliati, M.; Shils, J.L. Calculating total electrical energy delivered by deep brain stimulation systems (multiple letters). Ann. Neurol. 2005, 58, 168. [Google Scholar] [CrossRef]
- Benarroch, E.E. Subthalamic nucleus and its connections. Neurology 2008, 70, 1991–1995. [Google Scholar] [CrossRef] [PubMed]
- Parent, A.; Hazrati, L.N. Functional anatomy of the basal ganglia. II. The place of subthalamic nucleus and external pallidium in basal ganglia circuitry. Brain Res. Rev. 1995, 20, 128–154. [Google Scholar] [CrossRef]
- Sweet, J.A.; Pace, J.; Girgis, F.; Miller, J.P. Computational modeling and neuroimaging techniques for targeting during deep brain stimulation. Front. Neuroanat. 2016, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Emmi, A.; Antonini, A.; Macchi, V.; Porzionato, A.; de Caro, R. Anatomy and Connectivity of the Subthalamic Nucleus in Humans and Non-human Primates. Front. Neuroanat. 2020, 14, 13. [Google Scholar] [CrossRef]
- Haaxma, C.A.; Bloem, B.R.; Borm, G.F.; Oyen, W.J.G.; Leenders, K.L.; Eshuis, S.; Booij, J.; Dluzen, D.E.; Horstink, M.W.I.M. Gender differences in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2007, 78, 819–824. [Google Scholar] [CrossRef]
- Perrin, A.J.; Nosova, E.; Co, K.; Book, A.; Iu, O.; Silva, V.; Thompson, C.; McKeown, M.; Stoessl, A.J.; Farrer, M.J.; et al. Gender differences in Parkinson’s disease depression. Park. Relat. Disord. 2017, 36, 93–97. [Google Scholar] [CrossRef]
- Xie, Z.; Wen, F.; Tan, X.; Wei, J.; Zuo, B. The prevalence of psychiatric symptoms before the diagnosis of Parkinson’s disease in a nationwide cohort: A comparison to patients with cerebral infarction. PLoS ONE 2020, 15, e0236728. [Google Scholar] [CrossRef]
- Yoon, J.-E.; Kim, J.S.; Jang, W.; Park, J.; Oh, E.; Youn, J.; Park, S.; Cho, J.W. Gender Differences of Nonmotor Symptoms Affecting Quality of Life in Parkinson Disease. Neurodegener. Dis. 2017, 17, 276–280. [Google Scholar] [CrossRef]
- Chang, C.; Li, N.; Wu, Y.; Geng, N.; Ge, S.; Wang, J.; Wang, X.; Wang, X. Associations Between Bilateral Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) and Anxiety in Parkinson’s Disease Patients: A Controlled Study. J. Neuropsychiatry Clin. Neurosci. 2012, 24, 316–325. [Google Scholar] [CrossRef]
- Abbes, M.; Lhommée, E.; Thobois, S.; Klinger, H.; Schmitt, E.; Bichon, A.; Castrioto, A.; Xie, J.; Fraix, V.; Kistner, A.; et al. Subthalamic stimulation and neuropsychiatric symptoms in Parkinson’s disease: Results from a long-term follow-up cohort study. J. Neurol. Neurosurg. Psychiatry 2018, 89, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Kardous, R.; Joly, H.; Giordana, B.; Stefanini, L.; Mulliez, A.; Lemaire, J.-J.; Fontaine, D. Functional and dysfunctional impulsivities changes after subthalamic nucleus-deep brain stimulation in Parkinson disease. Neurochirurgie 2021, 67, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Combs, H.L.; Folley, B.S.; Berry, D.T.R.; Segerstrom, S.C.; Han, D.Y.; Anderson-Mooney, A.J.; Walls, B.D.; Van Horne, C. Cognition and Depression Following Deep Brain Stimulation of the Subthalamic Nucleus and Globus Pallidus Pars Internus in Parkinson’s Disease: A Meta-Analysis. Neuropsychol. Rev. 2015, 25, 439–454. [Google Scholar] [CrossRef] [PubMed]
- Buhmann, C.; Huckhagel, T.; Engel, K.; Gulberti, A.; Hidding, U.; Poetter-Nerger, M.; Goerendt, I.; Ludewig, P.; Braass, H.; Choe, C.-U.; et al. Adverse events in deep brain stimulation: A retrospective long-term analysis of neurological, psychiatric and other occurrences. PLoS ONE 2017, 12, e0178984. [Google Scholar] [CrossRef]
- Canesi, M.; Lavolpe, S.; Cereda, V.; Ranghetti, A.; Maestri, R.; Pezzoli, G.; Rusconi, M.L. Hypomania, depression, euthymia: New evidence in Parkinson’s disease. Behav. Neurol. 2020, 2020, 5139237. [Google Scholar] [CrossRef]
- Faouzi, J.; Corvol, J.C.; Mariani, L.L. Impulse control disorders and related behaviors in Parkinson’s disease: Risk factors, clinical and genetic aspects, and management. Curr. Opin. Neurol. 2021, 34, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Giannini, G.; Francois, M.; Lhommée, E.; Polosan, M.; Schmitt, E.; Fraix, V.; Castrioto, A.; Ardouin, C.; Bichon, A.; Pollak, P.; et al. Suicide and suicide attempts after subthalamic nucleus stimulation in Parkinson disease. Neurology 2019, 93, e97–e105. [Google Scholar] [CrossRef]
- Thobois, S.; Ardouin, C.; Lhommée, E.; Klinger, H.; Lagrange, C.; Xie, J.; Fraix, V.; Braga, M.C.C.; Hassani, R.; Kistner, A.; et al. Non-motor dopamine withdrawal syndrome after surgery for Parkinson’s disease: Predictors and underlying mesolimbic denervation. Brain 2010, 133, 1111–1127. [Google Scholar] [CrossRef]
- Hälbig, T.D.; Tse, W.; Frisina, P.G.; Baker, B.R.; Hollander, E.; Shapiro, H.; Tagliati, M.; Koller, W.C.; Olanow, C.W. Subthalamic deep brain stimulation and impulse control in Parkinson’s disease. Eur. J. Neurol. 2009, 16, 493–497. [Google Scholar] [CrossRef]
- Santangelo, G.; Barone, P.; Cuoco, S.; Raimo, S.; Pezzella, D.; Picillo, M.; Erro, R.; Moccia, M.; Pellecchia, M.T.; Amboni, M.; et al. Apathy in untreated, de novo patients with Parkinson’s disease: Validation study of Apathy Evaluation Scale. J. Neurol. 2014, 261, 2319–2328. [Google Scholar] [CrossRef] [PubMed]
- Mimura, M. Depression and apathy in Parkinson disease. Brain Nerve 2007, 59, 935–942. Available online: www.clinicaltrials.gov (accessed on 18 February 2022). [PubMed]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Okun, M.S.; Foote, K.D. Parkinson’s disease DBS: What, when, who and why? The time has come to tailor DBS targets. Expert Rev. Neurother. 2010, 10, 1847–1857. [Google Scholar] [CrossRef]
- Timmermann, L.; Jain, R.; Chen, L.; Maarouf, M.; Barbe, M.T.; Allert, N.; Brücke, T.; Kaiser, I.; Beirer, S.; Sejio, F.; et al. Multiple-source current steering in subthalamic nucleus deep brain stimulation for Parkinson’s disease (the VANTAGE study): A non-randomised, prospective, multicentre, open-label study. Lancet Neurol. 2015, 14, 693–701. [Google Scholar] [CrossRef]
- van Gaalen, M.M.; van Koten, R.; Schoffelmeer, A.N.M.; Vanderschuren, L.J.M.J. Critical involvement of dopaminergic neurotransmission in impulsive decision making. Biol. Psychiatry 2006, 60, 66–73. [Google Scholar] [CrossRef]
- York, M.K.; Wilde, E.A.; Simpson, R.; Jankovic, J. Relationship between neuropsychological outcome and DBS surgical trajectory and electrode location. J. Neurol. Sci. 2009, 287, 159–171. [Google Scholar] [CrossRef]
- Dayal, V.; Limousin, P.; Foltynie, T. Subthalamic nucleus deep brain stimulation in Parkinson’s disease: The effect of varying stimulation parameters. J. Park. Dis. 2017, 7, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Guidetti, M.; Marceglia, S.; Loh, A.; Harmsen, I.E.; Meoni, S.; Foffani, G.; Lozano, A.M.; Moro, E.; Volkmann, J.; Priori, A. Clinical perspectives of adaptive deep brain stimulation. Brain Stimul. 2021, 14, 1238–1247. [Google Scholar] [CrossRef]
- Arlotti, M.; Colombo, M.; Bonfanti, A.; Mandat, T.; Lanotte, M.M.; Pirola, E.; Borellini, L.; Rampini, P.; Eleopra, R.; Rinaldo, S.; et al. A New Implantable Closed-Loop Clinical Neural Interface: First Application in Parkinson’s Disease. Front. Neurosci. 2021, 15, 763235. [Google Scholar] [CrossRef]
- Gilbert, F.; Viaña, J.N.M.; Ineichen, C. Deflating the “DBS causes personality changes” bubble. Neuroethics 2021, 14, 1–17. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects (n) | 14 (7 males, 7 females) |
| Sex (M:F) | 1:1 |
| Age (Years) | 55.7 ± 9, 12 |
| Duration of Disease (Years) | 9.78 ± 2, 51 |
| Test | Mean ± SD | % Change | p-Value | |
|---|---|---|---|---|
| T0 | T1 | |||
| HAM-D | 10.64 ± 6.11 | 8.78 ± 6.67 | −17.49 | 0.424 |
| BDI | 12.64 ± 5.27 | 10.5 ± 6.58 | −16.93 | 0.285 |
| HAM-A | 14.36 ± 6.40 | 10.29 ± 5.46 | −28.35 | 0.041 |
| HAM-A (C) | 8.43 ± 4.18 | 6.50 ± 3.13 | −22.90 | 0.211 |
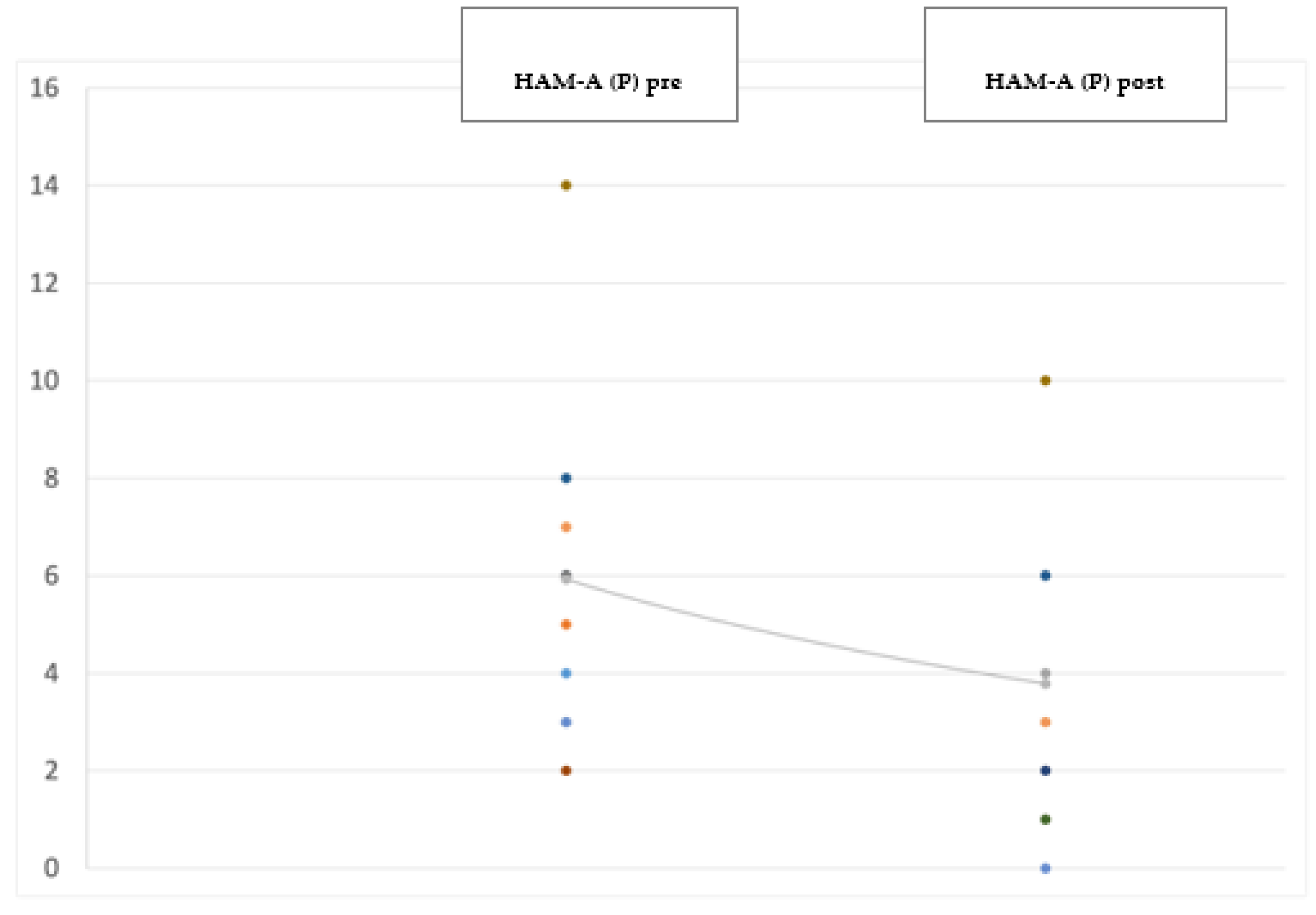
| HAM-A (P) | 5.93 ± 3.07 | 3.78 ± 2.72 | −36.26 | <0.001 * |
| BAI | 15 ± 6.67 | 11.71 ± 8.79 | −21.33 | 0.171 |
| AES | 29.35 ± 6.68 | 29.71 ± 6.68 | 1.22 | 0.878 |
| BIS-11 | 60.14 ± 8.72 | 66.07 ± 8.76 | 8.98 | 0.048 * |
| BIS-11 (A) | 14.93 ± 3.29 | 17.28 ± 3.34 | 13.6 | 0.05 * |
| BIS-11 (M) | 20.64 ± 2.98 | 22.93 ± 3.75 | 9.99 | 0.081 |
| BIS-11 (NP) | 24.57 ± 4.99 | 25.86 ± 4.15 | 4.99 | 0.433 |
| SSI | 0.5 ± 1.87 | 0.36 ± 0.63 | −28 | 0.800 |
| RFL-48 | 4.64 ± 0.47 | 4.47 ± 0.35 | −3.66 | 0.251 |
| Case | Total UPDRS | HAM-D | BDI | HAM-A | HAM-A (C) | HAM-A (P) | BAI | AES | BIS-11 | BIS-11 (A) | BIS-11 (M) | BIS-11 (NP) | SSI | RFL-48 | Lead | Positioning | TEED |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | ∆ % | left | right | ||
| 1 | −37.2 | −60 | 33.3 | −58.8 | −63.6 | −50.0 | −17.6 | 33.3 | 18.5 | 16.7 | 4.3 | 33.3 | / | 0.9 | PL | PL | 0.0301 |
| 2 | 6.1 | −50 | 73.3 | −56.25 | −54.5 | −60.0 | −30.0 | 18.2 | 18.6 | 33.3 | 13.6 | 16.0 | / | −14.5 | PL | PL | 0.0288 |
| 3 | −36.8 | 109.1 | −43.75 | −16.7 | 20.0 | −42.9 | 100.0 | 85.0 | −1.8 | −6.7 | −5.0 | 4.5 | / | −17.1 | M | C | 0.0298 |
| 4 | −48.9 | −46.1 | −50.0 | −26.7 | 0 | −57.1 | −64.7 | 10.0 | 9.1 | 37.5 | 11.8 | −13.6 | / | −5.7 | PL | PL | 0.0304 |
| 5 | −37.2 | −47.8 | 27.8 | −40.625 | −50.0 | −28.6 | −30.3 | 20.0 | 9.7 | 18.8 | 15.8 | 0 | / | −0.9 | PL | C | 0.0277 |
| 6 | −48.6 | 216.7 | 100.0 | 28.5 | 140.0 | −25.0 | 100.0 | 2.4 | −4.1 | −18.2 | 33.3 | −19.4 | / | −13.9 | M | M | 0.0286 |
| 7 | −51.6 | −57.1 | −36.4 | −10.0 | 0 | −33.3 | −90.0 | −33.3 | −1.6 | 7.1 | 0 | −7.4 | / | 3.1 | C | MA | 0.0284 |
| 8 | −38.0 | / | −50.0 | −37.5 | −33.3 | −50.0 | −57.1 | −12.5 | 0 | 0 | −9.5 | 9.1 | / | −8.9 | PL | PL | 0.0304 |
| 9 | −58.8 | 18.2 | 100.0 | 0 | 0 | 0 | −16.7 | −24.3 | 46.3 | 110.0 | 73.3 | 10.3 | / | −12.2 | L | CA | 0.0291 |
| 10 | −45.1 | 500 | 12.5 | 240.0 | 1000 | 50.0 | 45.5 | 27.0 | 45.3 | 40.0 | 23.8 | 76.5 | / | −16.6 | C | M | 0.0295 |
| 11 | −58.8 | −46.7 | −26.7 | −29.4 | −33.3 | −25.0 | −54.2 | −16.7 | 4.2 | 33.3 | 16.0 | −18.8 | / | −1.2 | CA | PL | 0.0285 |
| 12 | −59.0 | −41.2 | −12.5 | −62.5 | −61.5 | −66.7 | −56.3 | 19.2 | −16.4 | −21.1 | 41.2 | −23.3 | −100.0 | 13.3 | LA | LA | 0.0291 |
| 13 | −37.2 | −100.0 | −89.5 | −100.0 | −100.0 | −100.0 | −53.8 | −40.5 | 27.9 | 30.0 | 43.8 | 11.8 | / | 22.9 | PL | PL | 0.0279 |
| 14 | −16.1 | −16.7 | −25.0 | −52.9 | −50.0 | −57.1 | −53.8 | 22.7 | 3.6 | 0 | −30.4 | 47.4 | / | 10.2 | P | PL | 0.0306 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somma, T.; Esposito, F.; Scala, M.R.; Scelzo, A.; Baiano, C.; Patti, S.; Meglio, V.; Iasevoli, F.; Cavallo, L.M.; Solari, D.; et al. Psychiatric Symptoms in Parkinson’s Disease Patients before and One Year after Subthalamic Nucleus Deep Brain Stimulation Therapy: Role of Lead Positioning and Not of Total Electrical Energy Delivered. J. Pers. Med. 2022, 12, 1643. https://doi.org/10.3390/jpm12101643
Somma T, Esposito F, Scala MR, Scelzo A, Baiano C, Patti S, Meglio V, Iasevoli F, Cavallo LM, Solari D, et al. Psychiatric Symptoms in Parkinson’s Disease Patients before and One Year after Subthalamic Nucleus Deep Brain Stimulation Therapy: Role of Lead Positioning and Not of Total Electrical Energy Delivered. Journal of Personalized Medicine. 2022; 12(10):1643. https://doi.org/10.3390/jpm12101643
Chicago/Turabian StyleSomma, Teresa, Felice Esposito, Maria Rosaria Scala, Antonio Scelzo, Cinzia Baiano, Sara Patti, Vincenzo Meglio, Felice Iasevoli, Luigi M. Cavallo, Domenico Solari, and et al. 2022. "Psychiatric Symptoms in Parkinson’s Disease Patients before and One Year after Subthalamic Nucleus Deep Brain Stimulation Therapy: Role of Lead Positioning and Not of Total Electrical Energy Delivered" Journal of Personalized Medicine 12, no. 10: 1643. https://doi.org/10.3390/jpm12101643
APA StyleSomma, T., Esposito, F., Scala, M. R., Scelzo, A., Baiano, C., Patti, S., Meglio, V., Iasevoli, F., Cavallo, L. M., Solari, D., De Bartolomeis, A., Cappabianca, P., & D’Urso, G. (2022). Psychiatric Symptoms in Parkinson’s Disease Patients before and One Year after Subthalamic Nucleus Deep Brain Stimulation Therapy: Role of Lead Positioning and Not of Total Electrical Energy Delivered. Journal of Personalized Medicine, 12(10), 1643. https://doi.org/10.3390/jpm12101643