
The Metabolic Score for Insulin Resistance (METS-IR) as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study among Korean without Diabetes



Abstract

1. Introduction
2. Materials and Methods
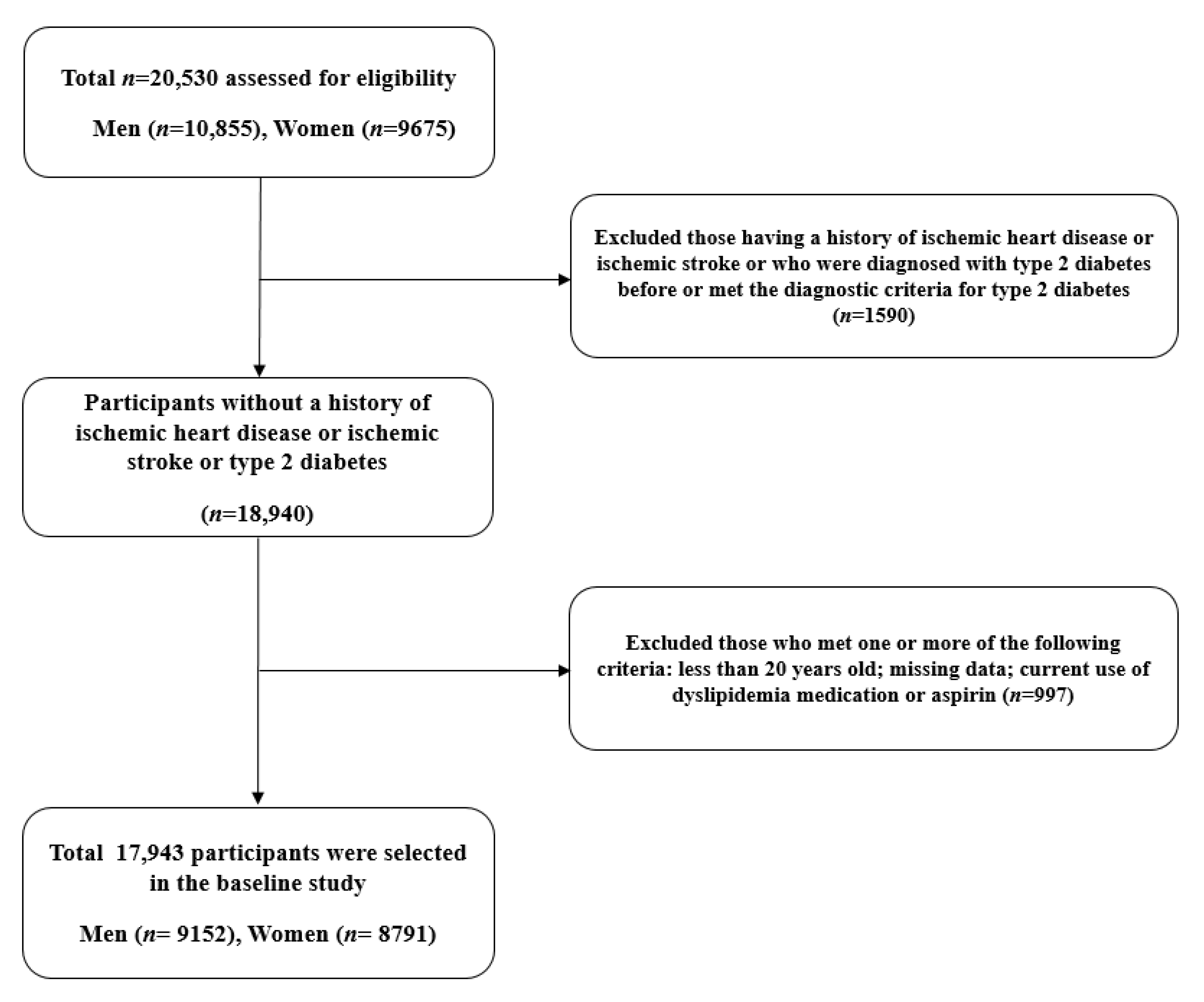
2.1. Study Population
2.2. Study Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Yusuf, S.; Reddy, S.; Ôunpuu, S.; Anand, S. Global burden of cardiovascular diseases: Part i: General considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001, 104, 2746–2753. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef]
- Fahed, M.; Jaoudeh, M.G.A.; Merhi, S.; Mosleh, J.M.B.; Ghadieh, R.; Al Hayek, S.; Fares, J.E.E.H. Evaluation of risk factors for insulin resistance: A cross sectional study among employees at a private university in Lebanon. BMC Endocr. Disord. 2020, 20, 1–14. [Google Scholar] [CrossRef]
- Vafaeimanesh, J.; Parham, M.; Norouzi, S.; Hamednasimi, P.; Bagherzadeh, M. Insulin resistance and coronary artery disease in non-diabetic patients: Is there any correlation? Casp. J. Intern. Med. 2018, 9, 121–126. [Google Scholar] [CrossRef]
- Evans, J.M.M.; Wang, J.; Morris, A.D. Comparison of cardiovascular risk between patients with type 2 diabetes and those who had had a myocardial infarction: Cross sectional and cohort studies. BMJ 2002, 324, 939. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.D.; Folsom, A.R.; Pankow, J.S.; Brancati, F.L. Cardiovascular events in diabetic and nondiabetic adults with or without history of myocardial infarction. Circulation 2004, 109, 855–860. [Google Scholar] [CrossRef]
- Bello-Chavolla, O.Y.; Almeda-Valdes, P.; Gómez-Velasco, D.; Viveros-Ruiz, T.; Cruz-Bautista, I.; Romo-Romo, A.; Sánchez-Lázaro, D.; Meza-Oviedo, D.; Vargas-Vazquez, A.; Campos, O.A.; et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur. J. Endocrinol. 2018, 178, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.Z.; Fan, J.; Pan, S.J. METS-IR, a novel simple insulin resistance indexes, is associated with hypertension in normal-weight Chinese adults. J. Clin. Hypertens. 2019, 21, 1075–1081. [Google Scholar] [CrossRef]
- Park, B.; Lee, Y.-J.; Lee, H.S.; Jung, D.-H. The triglyceride-glucose index predicts ischemic heart disease risk in Koreans: A prospective study using National Health Insurance Service data. Cardiovasc. Diabetol. 2020, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Seung-Hyun Committee of Clinical Practice Guidelines, Korean Diabetes Association; Kim, B.-Y.; Kang, E.S.; Noh, J.; Kim, S.-K.; Park, S.-O.; Hur, K.Y.; Chon, S.; Moon, M.K.; et al. 2019 Clinical Practice Guidelines for Type 2 Diabetes Mellitus in Korea. Diabetes Metab. J. 2019, 43, 398–406. [Google Scholar] [CrossRef]
- Carretero, O.A.; Oparil, S. Essential hypertension: Part i: Definition and etiology. Circulation 2000, 101, 329–335. [Google Scholar] [CrossRef] [PubMed]
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 2003, 26, 3160–3167. [Google Scholar]
- Einhorn, D. American College of Endocrinology Position Statement on the Insulin Resistance Syndrome. Endocr. Pract. 2003, 9, 5–21. [Google Scholar] [CrossRef]
- Levey, A.S.; Eckardt, K.-U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; Zeeuw, D.D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef] [PubMed]
- Bornfeldt, K.E.; Tabas, I. Insulin Resistance, Hyperglycemia, and Atherosclerosis. Cell Metabol. 2011, 14, 575–585. [Google Scholar] [CrossRef]
- Yanase, M.; Takatsu, F.; Tagawa, T.; Kato, T.; Arai, K.; Koyasu, M.; Horibe, H.; Nomoto, S.; Takemoto, K.; Shimizu, S.; et al. Insulin Resistance and Fasting Hyperinsulinemia Are Risk Factors for New Cardiovascular Events in Patients with Prior Coronary Artery Disease and Normal Glucose Tolerance. Circ. J. 2004, 68, 47–52. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Karrowni, W.; Li, Y.; Jones, P.G.; Cresci, S.; Abdallah, M.S.; Lanfear, D.E.; Maddox, T.M.; McGuire, D.K.; Spertus, J.A.; Horwitz, P.A. Insulin resistance is associated with significant clinical atherosclerosis in nondiabetic patients with acute myocardial infarction. Arter. Thromb. Vasc. Biol. 2013, 33, 2245–2251. [Google Scholar] [CrossRef]
- Wallace, T.M.; Matthews, D.R. The assessment of insulin resistance in man. Diabet. Med. 2002, 19, 527–534. [Google Scholar] [CrossRef]
- Rudvik, A.; Månsson, M. Evaluation of surrogate measures of insulin sensitivity—correlation with gold standard is not enough. BMC Med. Res. Methodol. 2018, 18, 64. [Google Scholar] [CrossRef]
- Manley, S.E.; Stratton, I.; Clark, P.M.; Luzio, S. Comparison of 11 Human Insulin Assays: Implications for Clinical Investigation and Research. Clin. Chem. 2007, 53, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Eeg-Olofsson, K.; Gudbjörnsdottir, S.; Eliasson, B.; Zethelius, B.; Cederholm, J. The triglycerides-to-HDL-cholesterol ratio and cardiovascular disease risk in obese patients with type 2 diabetes: An observational study from the Swedish National Diabetes Register (NDR). Diabetes Res. Clin. Pract. 2014, 106, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Tatsumi, Y.; Morimoto, A.; Asayama, K.; Sonoda, N.; Miyamatsu, N.; Ohno, Y.; Miyamoto, Y.; Izawa, S.; Ohkubo, T. Fasting Blood Glucose Predicts Incidence of Hypertension Independent of HbA1c Levels and Insulin Resistance in Middle-Aged Japanese: The Saku Study. Am. J. Hypertens. 2019, 32, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Reaven, G.M. Role of insulin resistance in human disease. Diabetes 1988, 37, 1595–1607. [Google Scholar] [CrossRef]
- Stout, R.W. Insulin and Atheroma: 20-Yr Perspective. Diabetes Care 1990, 13, 631–654. [Google Scholar] [CrossRef] [PubMed]
- Bonora, E.; Targher, G.; Formentini, G.; Calcaterra, F.; Lombardi, S.; Marini, F.; Zenari, L.; Saggiani, F.; Poli, M.; Perbellini, S.; et al. The Metabolic Syndrome is an independent predictor of cardiovascular disease in Type 2 diabetic subjects. Prospective data from the Verona Diabetes Complications Study. Diabet. Med. 2004, 21, 52–58. [Google Scholar] [CrossRef]
- Ninomiya, T.; Kubo, M.; Doi, Y.; Yonemoto, K.; Tanizaki, Y.; Rahman, M.; Arima, H.; Tsuryuya, K.; Iida, M.; Kiyohara, Y. Impact of metabolic syndrome on the development of cardiovascular disease in a general japanese population: The hisayama study. Stroke 2007, 38, 2063–2069. [Google Scholar] [CrossRef]
- McNeill, A.M.; Rosamond, W.D.; Girman, C.J.; Golden, S.H.; Schmidt, M.I.; East, H.E.; Ballantyne, C.M.; Heiss, G. The Metabolic Syndrome and 11-Year Risk of Incident Cardiovascular Disease in the Atherosclerosis Risk in Communities Study. Diabetes Care 2005, 28, 385–390. [Google Scholar] [CrossRef]
- Ford, E.S. The metabolic syndrome and mortality from cardiovascular disease and all-causes: Findings from the national health and nutrition examination survey ii mortality study. Atherosclerosis 2004, 173, 307–312. [Google Scholar] [CrossRef]
- Mente, A.; Yusuf, S.; Islam, S.; McQueen, M.J.; Tanomsup, S.; Onen, C.L.; Rangarajan, S.; Gerstein, H.; Anand, S.S. Metabolic Syndrome and Risk of Acute Myocardial Infarction: A Case-Control Study of 26,903 Subjects From 52 Countries. J. Am. Coll. Cardiol. 2010, 55, 2390–2398. [Google Scholar] [CrossRef] [PubMed]
- Lakka, H.-M.; Laaksonen, D.E.; Lakka, T.; Niskanen, L.K.; Kumpusalo, E.; Tuomilehto, J.; Salonen, J.T. The Metabolic Syndrome and Total and Cardiovascular Disease Mortality in Middle-aged Men. JAMA 2002, 288, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Gaw, A.; Scherbakova, O.; Ford, I.; O’Reilly, D.S.; Haffner, S.M.; Isles, C.; Macfarlane, P.W.; Packard, C.J.; Cobbe, S.M.; et al. Metabolic Syndrome with and Without C-Reactive Protein as a Predictor of Coronary Heart Disease and Diabetes in the West of Scotland Coronary Prevention Study. Circulation 2003, 108, 414–419. [Google Scholar] [CrossRef]
- Malik, S.; Wong, N.D.; Franklin, S.S.; Kamath, T.V.; L’Italien, G.J.; Pio, J.R.; Williams, G.R. Impact of the Metabolic Syndrome on Mortality from Coronary Heart Disease, Cardiovascular Disease, and All Causes in United States Adults. Circulation 2004, 110, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Borg, R.; Kuenen, J.C.; Carstensen, B.; Zheng, H.; Nathan, D.M.; Heine, R.J.; Nerup, J.; Borchjohnsen, K.; Witte, D. HbA1c and mean blood glucose show stronger associations with cardiovascular disease risk factors than do postprandial glycaemia or glucose variability in persons with diabetes: The A1C-Derived Average Glucose (ADAG) study. Diabetology 2010, 54, 69–72. [Google Scholar] [CrossRef]
- Meigs, J.B.; Wilson, P.W.F.; Fox, C.S.; Vasan, R.S.; Nathan, D.M.; Sullivan, L.; D’Agostino, R.B. Body Mass Index, Metabolic Syndrome, and Risk of Type 2 Diabetes or Cardiovascular Disease. J. Clin. Endocrinol. Metab. 2006, 91, 2906–2912. [Google Scholar] [CrossRef]
- St-Pierre, A.C.; Cantin, B.; Mauriège, P.; Bergeron, J.; Dagenais, G.R.; Després, J.-P.; Lamarche, B. Insulin resistance syndrome, body mass index and the risk of ischemic heart disease. Can. Med. Assoc. J. 2005, 172, 1301–1305. [Google Scholar] [CrossRef]
- Chopra, A.K. Metabolic Syndrome or Insulin Resistance: Evolution, Controversies and Association with Cardiovascular Disease Risk. Indian J. Clin. Cardiol. 2020, 1, 77–85. [Google Scholar] [CrossRef]
- Lim, J.; Kim, J.; Koo, S.H.; Kwon, G.C. Comparison of triglyceride glucose index, and related parameters to predict insulin resistance in Korean adults: An analysis of the 2007-2010 Korean National Health and Nutrition Examination Survey. PLoS ONE 2019, 14, e0212963. [Google Scholar] [CrossRef]
- Jin, J.-L.; Cao, Y.-X.; Wu, L.-G.; You, X.-D.; Guo, Y.-L.; Wu, N.-Q.; Zhu, C.-G.; Gao, Y.; Dong, Q.-T.; Zhang, H.-W.; et al. Triglyceride glucose index for predicting cardiovascular outcomes in patients with coronary artery disease. J. Thorac. Dis. 2018, 10, 6137–6146. [Google Scholar] [CrossRef] [PubMed]
- Collaboration, A.P.C.S. A comparison of lipid variables as predictors of cardiovascular disease in the asia pacific region. Ann. Epidemiol. 2005, 15, 405–413. [Google Scholar]
- Yang, W.; Ma, R.; Zhang, X.; Guo, H.; He, J.; Mao, L.; Mu, L.; Hu, Y.; Yan, Y.; Liu, J.; et al. Comparison Between Metabolic Syndrome and the Framingham Risk Score as Predictors of Cardiovascular Diseases Among Kazakhs in Xinjiang. Sci. Rep. 2018, 8, 16474. [Google Scholar] [CrossRef]
- Liu, J.; Zhao, N.; Wang, W.; Sun, J.-Y.; Liu, J.; Wang, M.; Qin, L.-P.; Wu, Z.-S. Incidence risk of cardiovascular diseases associated with specific combinations regarding the metabolic syndrome components. Zhonghua Liu Xing Bing Xue Za Zhi 2008, 29, 652–655. [Google Scholar] [PubMed]
- Woodward, M.; Tunstall-Pedoe, H. The metabolic syndrome is not a sensible tool for predicting the risk of coronary heart disease. Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Knuiman, M.W.; Hung, J.; Divitini, M.L.; Davis, T.M.; Beilby, J. Utility of the metabolic syndrome and its components in the prediction of incident cardiovascular disease: A prospective cohort study. Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 235–241. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| METS-IR Quartiles | ||||||
|---|---|---|---|---|---|---|
| Q1 n = 4456 | Q2 n = 4504 | Q3 n = 4424 | Q4 n = 4559 | p Value 1 | Post Hoc 2 | |
| METS-IR | ≤28.9 | 29.0–33.2 | 33.3–37.9 | ≥38.0 | ||
| Age (years) | 40.7 ± 10.4 | 45.4 ± 10.3 | 46.7 ± 10.1 | 46.0 ± 10.1 | <0.001 | a,b,c,d,e,f |
| Male sex (%) | 20.5 | 42.5 | 64.0 | 76.6 | <0.001 | - |
| Body mass index (kg/m2) | 19.8 ± 1.4 | 22.3 ± 1.3 | 24.1 ± 1.4 | 26.8 ± 2.3 | <0.001 | a,b,c,d,e,f |
| Systolic blood pressure (mmHg) | 113 ± 13 | 119 ± 14 | 124 ± 14 | 130 ± 14 | <0.001 | a,b,c,d,e,f |
| Diastolic blood pressure (mmHg) | 70 ± 9 | 74 ± 9 | 77 ± 9 | 81 ± 9 | <0.001 | a,b,c,d,e,f |
| Mean arterial pressure (mmHg) | 84 ± 10 | 89 ± 10 | 93 ± 10 | 97 ± 10 | <0.001 | a,b,c,d,e,f |
| Fasting plasma glucose (mg/dL) | 86.3 ± 8.4 | 89.9 ± 8.5 | 92.4 ± 9.2 | 95.6 ± 10.3 | <0.001 | a,b,c,d,e,f |
| Total cholesterol (mg/dL) | 180 ± 31 | 186 ± 32 | 191 ± 33 | 197 ± 34 | <0.001 | a,b,c,e,f |
| Triglyceride (mg/dL) | 73 ± 26 | 95 ± 39 | 125 ± 57 | 193 ± 117 | <0.001 | a,b,c,d,e,f |
| HDL-cholesterol (mg/dL) | 65 ± 11 | 56 ± 10 | 49 ± 8 | 43 ± 7 | <0.001 | a,b,c,d,e,f |
| C-reactive protein (mg/L) | 0.8 ± 2.7 | 1.2 ± 3.5 | 1.6 ± 4.6 | 1.9 ± 4.0 | <0.001 | a,b,c,d,e,f |
| eGFR (mL/min/1.73 m2) | 86.6 ± 14.7 | 83.9 ± 13.3 | 82.7 ± 13.0 | 82.0 ± 12.6 | <0.001 | a,b,c,d,e |
| Current smoker (%) | 14.6 | 20.5 | 26.6 | 37.4 | <0.001 | - |
| Alcohol drinking (%) | 35.1 | 40.5 | 48.2 | 51.6 | <0.001 | - |
| Regular exercise (%) | 26.5 | 33.6 | 33.2 | 27.8 | <0.001 | - |
| Hypertension (%) | 6.3 | 13.5 | 23.3 | 35.5 | <0.001 | - |
| Impaired fasting glucose (%) | 5.6 | 12.0 | 19.4 | 31.5 | <0.001 | - |
| Metabolic syndrome (%) | 0.1 | 1.5 | 7.5 | 36.5 | <0.001 | - |
| METS-IR Quartiles | |||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | p Trend | |
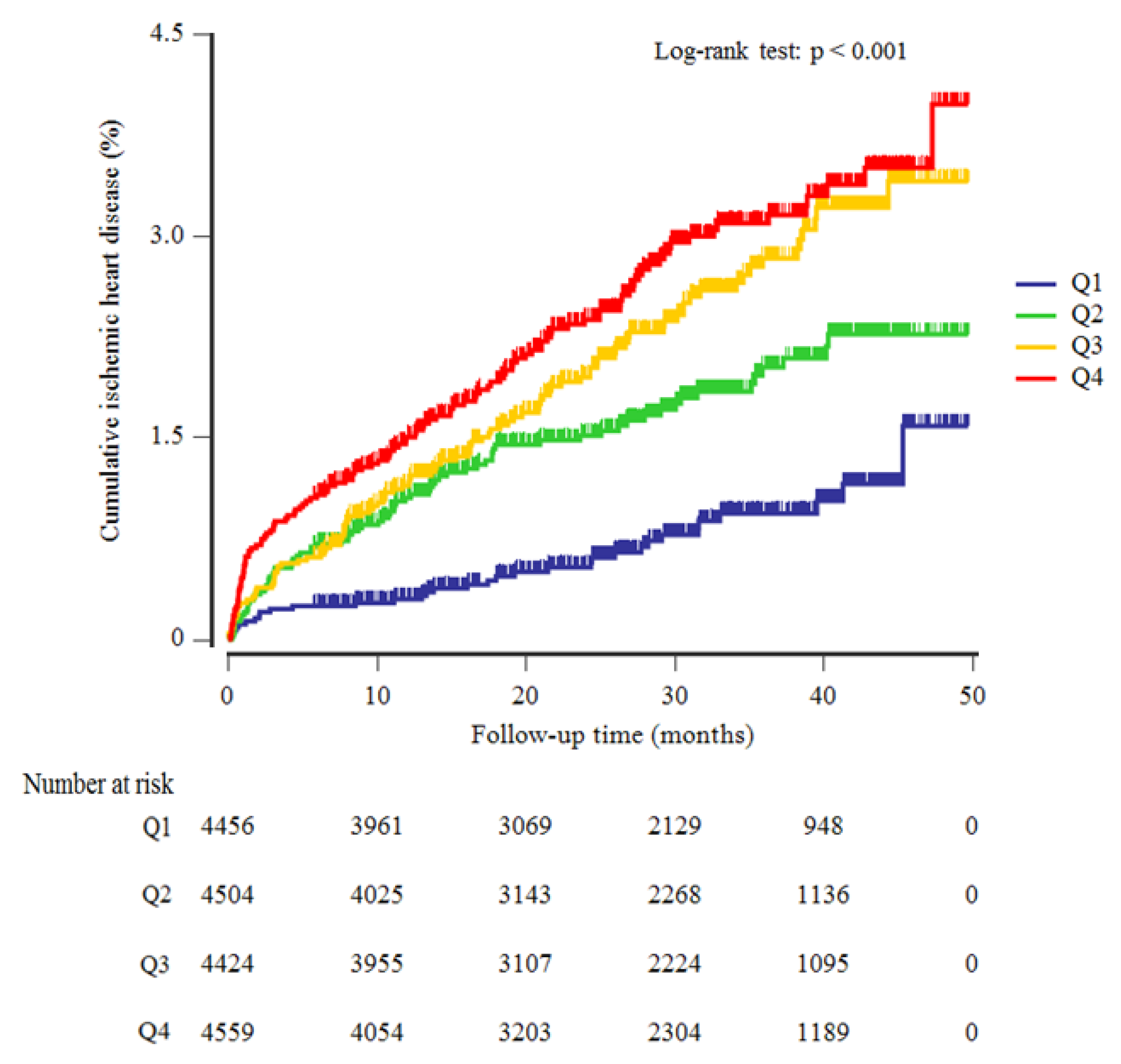
| New cases of ischemic heart disease, n | 33 | 76 | 102 | 121 | |
| Mean follow-up, years | 2.3 ± 1.0 | 2.4 ± 1.1 | 2.4 ± 1.1 | 2.4 ± 1.1 | |
| Person-years of follow-up | 10,311 | 10,646 | 10,521 | 10,853 | |
| Incidence rate/1000 person-years | 3.2 | 7.1 | 9.7 | 11.1 | |
| Model 1 | 1.00 (reference) | 1.60 (1.06–2.41) | 1.91 (1.28–2.86) | 2.25 (1.51–3.35) | <0.001 |
| Men | 1.00 (reference) | 1.55 (0.80–3.04) | 2.00 (1.06–3.77) | 2.26 (1.21–4.24) | 0.031 |
| Women | 1.00 (reference) | 1.62 (0.95–2.75) | 1.71 (0.97–3.00) | 2.13 (1.20–3.79) | 0.080 |
| Model 2 | 1.00 (reference) | 1.65 (1.06–2.58) | 2.00 (1.30–3.01) | 2.34 (1.52–3.59) | 0.001 |
| Men | 1.00 (reference) | 1.47 (0.75–2.88) | 1.78 (0.94–3.37) | 2.14 (1.14–4.03) | 0.050 |
| Women | 1.00 (reference) | 1.73 (0.95–3.15) | 2.05 (1.10–3.81) | 2.05 (1.06–3.96) | 0.111 |
| Model 3 | 1.00 (reference) | 1.63 (1.04–2.54) | 1.94 (1.25–3.01) | 2.22 (1.43–3.47) | 0.004 |
| Men | 1.00 (reference) | 1.42 (0.72–2.80) | 1.70 (0.89–3.25) | 2.04 (1.07–3.87) | 0.095 |
| Women | 1.00 (reference) | 1.78 (0.98–3.25) | 2.10 (1.12–3.93) | 2.11 (1.06–4.20) | 0.103 |
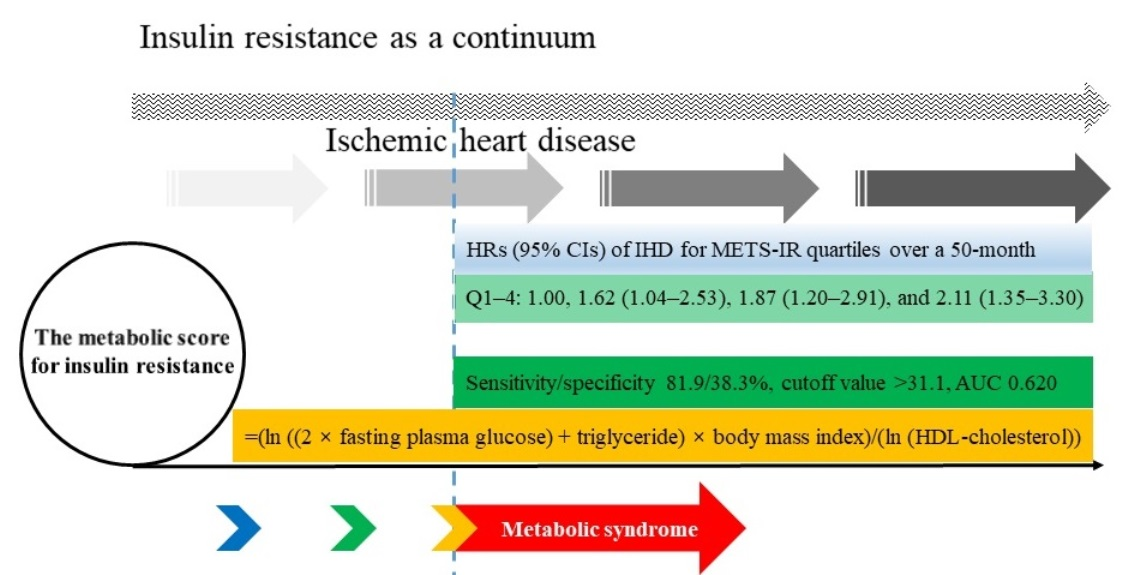
| Model 4 | 1.00 (reference) | 1.62 (1.04–2.53) | 1.87 (1.20–2.91) | 2.11 (1.35–3.30) | 0.010 |
| Men | 1.00 (reference) | 1.39 (0.70–2.73) | 1.61 (0.84–3.07) | 1.90 (1.00–3.61) | 0.169 |
| Women | 1.00 (reference) | 1.80 (0.99–3.28) | 2.07 (1.10–3.88) | 2.07 (1.04–4.12) | 0.116 |
| Pairwise Comparison of AUC | ||||||
|---|---|---|---|---|---|---|
| Difference | 95% CI | p Value | ||||
| METS-IR vs. MetS | 0.069 | 0.04 to 0.9 | <0.001 | |||
| METS-IR vs. N of MetS components | 0.004 | −0.02 to 0.03 | 0.733 | |||
| N of MetS components vs. MetS | 0.064 | 0.04 to 0.09 | <0.001 | |||
| Prediction for Ischemic Heart Disease | ||||||
| Sensitivity (%) | Specificity (%) | Cutoff Value | AUC | Youden’s Index | p Value | |
| METS-IR | 81.9 | 38.3 | >31.1 | 0.620 | 0.202 | <0.001 |
| Men | 84.4 | 25.4 | >32.3 | 0.554 | 0.097 | 0.005 |
| Women | 71.9 | 55.5 | >30.9 | 0.657 | 0.274 | <0.001 |
| MetS | 22.7 | 88.7 | >0 | 0.552 | 0.104 | <0.001 |
| N of MetS components | 78.6 | 39.0 | >0 | 0.616 | 0.176 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, J.; Jung, D.; Lee, Y.; Park, B. The Metabolic Score for Insulin Resistance (METS-IR) as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study among Korean without Diabetes. J. Pers. Med. 2021, 11, 742. https://doi.org/10.3390/jpm11080742
Yoon J, Jung D, Lee Y, Park B. The Metabolic Score for Insulin Resistance (METS-IR) as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study among Korean without Diabetes. Journal of Personalized Medicine. 2021; 11(8):742. https://doi.org/10.3390/jpm11080742
Chicago/Turabian StyleYoon, Jihyun, Donghyuk Jung, Yongjae Lee, and Byoungjin Park. 2021. "The Metabolic Score for Insulin Resistance (METS-IR) as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study among Korean without Diabetes" Journal of Personalized Medicine 11, no. 8: 742. https://doi.org/10.3390/jpm11080742
APA StyleYoon, J., Jung, D., Lee, Y., & Park, B. (2021). The Metabolic Score for Insulin Resistance (METS-IR) as a Predictor of Incident Ischemic Heart Disease: A Longitudinal Study among Korean without Diabetes. Journal of Personalized Medicine, 11(8), 742. https://doi.org/10.3390/jpm11080742