
Incidence of Adnexal Torsion in the Republic of Korea: A Nationwide Serial Cross-Sectional Study (2009–2018)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
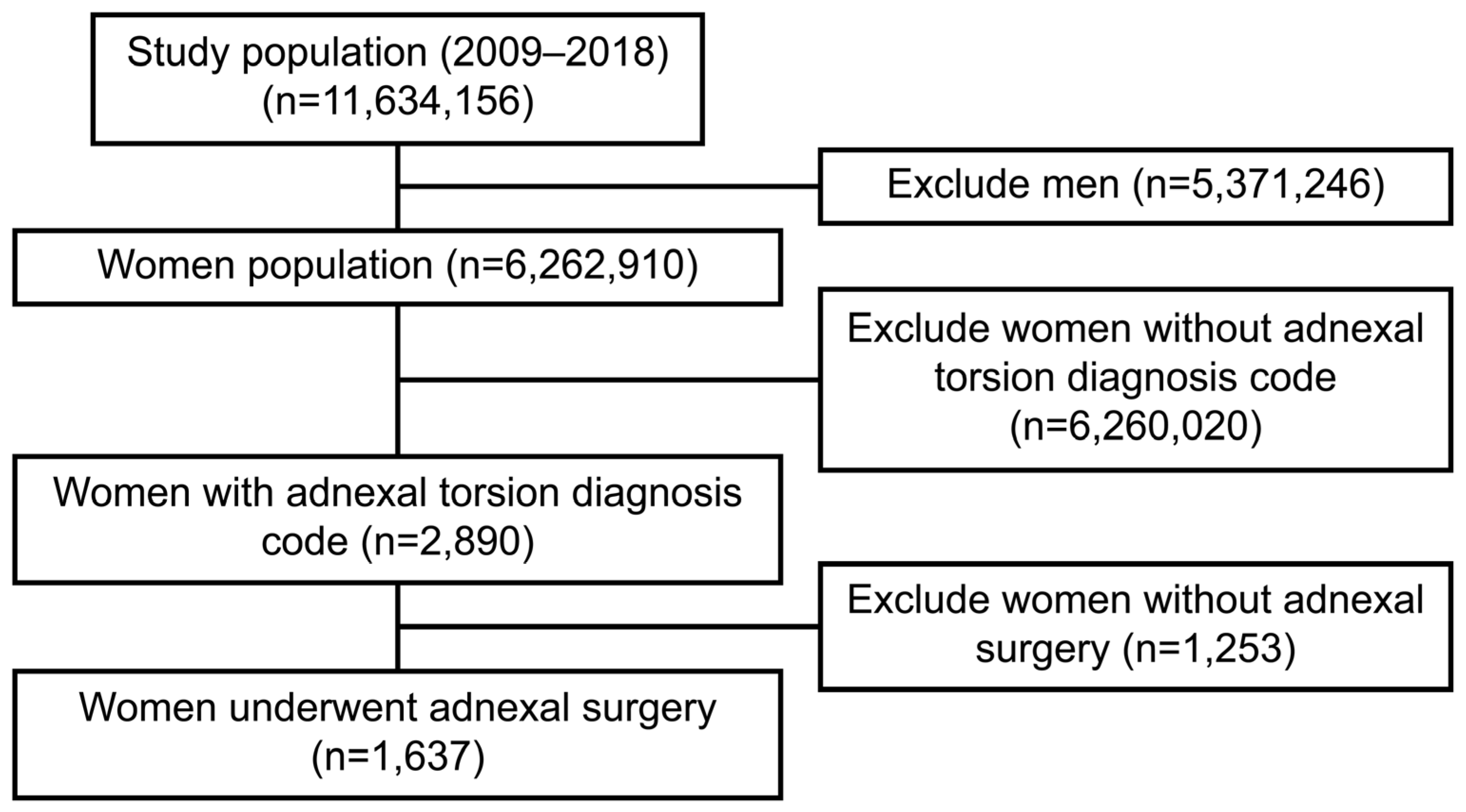
2.2. Patient Selection
2.3. Variables
2.4. Statistics
2.5. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berkkanoglu, M.; Coetzee, K.; Bulut, H.; Ozgur, K. Risk of ovarian torsion is reduced in GnRH agonist triggered freeze-all cycles: A retrospective cohort study. J. Obstet. Gynaecol. 2019, 39, 212–217. [Google Scholar] [CrossRef]
- Shah, A.A.; Likes, C.E.; Price, T.M. Early polycystic ovary syndrome as a possible etiology of unexplained premenarcheal ovarian torsion. J. Pediatr. Adolesc. Gynecol. 2009, 22, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Descargues, G.; Tinlot-Mauger, F.; Gravier, A.; Lemoine, J.P.; Marpeau, L. Adnexal torsion: A report on forty-five cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 98, 91–96. [Google Scholar] [CrossRef]
- Oelsner, G.; Shashar, D. Adnexal torsion. Clin. Obstet. Gynecol. 2006, 49, 459–463. [Google Scholar] [CrossRef]
- Bayer, A.I.; Wiskind, A.K. Adnexal torsion: Can the adnexa be saved? Am. J. Obstet. Gynecol. 1994, 171, 1506–1511. [Google Scholar] [CrossRef]
- Celik, A.; Ergün, O.; Aldemir, H.; Ozcan, C.; Ozok, G.; Erdener, A.; Balýk, E. Long-term results of conservative management of adnexal torsion in children. J. Pediatr. Surg. 2005, 40, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, L.T. Adnexal torsion. Am. J. Obstet. Gynecol. 1985, 152, 456–461. [Google Scholar] [CrossRef]
- Yuk, J.S.; Kim, L.Y.; Shin, J.Y.; Choi, D.Y.; Kim, T.Y.; Lee, J.H. A national population-based study of the incidence of adnexal torsion in the Republic of Korea. Int. J. Gynaecol. Obstet. 2015, 129, 169–170. [Google Scholar] [CrossRef]
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, K.J.; Miller, C.E. Adnexal torsion: Review of the literature. J. Minim. Invasive Gynecol. 2014, 21, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Anteby, S.O.; Schenker, J.G.; Polishuk, W.Z. The value of laparoscopy in acute pelvic pain. Ann. Surg. 1975, 181, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Becker, J.H.; de Graaff, J.; Vos, M.C. Torsion of the ovary: A known but frequently missed diagnosis. Eur. J. Emerg. Med. 2009, 16, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, B.D.; Adler, M.D.; Powell, E.C. Incidence and trends of pediatric ovarian torsion hospitalizations in the United States, 2000–2006. Pediatrics 2010, 125, 532–538. [Google Scholar] [CrossRef]
- Bassi, A.; Czuzoj-Shulman, N.; Abenhaim, H.A. Effect of pregnancy on the management and outcomes of ovarian torsion: A population-based matched cohort study. J. Minim. Invasive Gynecol. 2018, 25, 1260–1265. [Google Scholar] [CrossRef]
- Varras, M.; Tsikini, A.; Polyzos, D.; Samara, C.; Hadjopoulos, G.; Akrivis, C. Uterine adnexal torsion: Pathologic and gray-scale ultrasonographic findings. Clin. Exp. Obstet. Gynecol. 2004, 31, 34–38. [Google Scholar]
- Houry, D.; Abbott, J.T. Ovarian torsion: A fifteen-year review. Ann. Emerg. Med. 2001, 38, 156–159. [Google Scholar] [CrossRef]
- White, M.; Stella, J. Ovarian torsion: 10-year perspective. Emerg. Med. Australas. 2005, 17, 231–237. [Google Scholar] [CrossRef]
- Humayun, A.; Saeed, A. The relative frequency and histopathological pattern of ovarian masses. Biomed. Pak. 2012. [Google Scholar] [CrossRef]
- Oltmann, S.C.; Fischer, A.; Barber, R.; Huang, R.; Hicks, B.; Garcia, N. Cannot exclude torsion—A 15-year review. J. Pediatr. Surg. 2009, 44, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Raman, S.; Sivanesaratnam, V. Torsion of ovarian tumors: A clinicopathological study. Int. J. Gynaecol. Obstet. 1989, 28, 21–25. [Google Scholar] [CrossRef]
- Ngo, A.V.; Otjen, J.P.; Parisi, M.T.; Ferguson, M.R.; Otto, R.K.; Stanescu, A.L. Pediatric ovarian torsion: A pictorial review. Pediatr. Radiol. 2015, 45, 1845–1855. [Google Scholar] [CrossRef]
- Lee, E.J.; Kwon, H.C.; Joo, H.J.; Suh, J.H.; Fleischer, A.C. Diagnosis of ovarian torsion with color Doppler sonography: Depiction of twisted vascular pedicle. J. Ultrasound Med. 1998, 17, 83–89. [Google Scholar] [CrossRef]
- Chang, H.C.; Bhatt, S.; Dogra, V.S. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics 2008, 28, 1355–1368. [Google Scholar] [CrossRef] [PubMed]
- Multani, J.; Kives, S. Dermoid cysts in adolescents. Curr. Opin. Obstet. Gynecol. 2015, 27, 315–319. [Google Scholar] [CrossRef]
- Powell, J.K. Benign adnexal masses in the adolescent. Adolesc. Med. Clin. 2004, 15, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, A.; Bukulmez, O.; Genc, C.; Karamursel, B.S.; Ayhan, A. Mature cystic teratomas of the ovary: Case series from one institution over 34 years. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 88, 153–157. [Google Scholar] [CrossRef]
- Hasson, J.; Tsafrir, Z.; Azem, F.; Bar-On, S.; Almog, B.; Mashiach, R.; Seidman, D.; Lessing, J.B.; Grisaru, D. Comparison of adnexal torsion between pregnant and nonpregnant women. Am. J. Obstet. Gynecol. 2010, 202, 536.e1–536.e6. [Google Scholar] [CrossRef]
- Yuk, J.S.; Shin, J.Y.; Park, W.I.; Kim, D.W.; Shin, J.W.; Lee, J.H. Association between pregnancy and adnexal torsion: A population-based, matched case-control study. Med. (Baltim.) 2016, 95, e3861. [Google Scholar] [CrossRef]
- Tsafrir, Z.; Hasson, J.; Levin, I.; Solomon, E.; Lessing, J.B.; Azem, F. Adnexal torsion: Cystectomy and ovarian fixation are equally important in preventing recurrence. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 162, 203–205. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AT | ||||
|---|---|---|---|---|
| Non-AT (N = 6,261,273) | AT (N = 1637) | Total (N = 6,269,910) | p | |
| Age (years) | 34 [20;51] | 30 [20;41] | 34 [20;51] | <0.001 a |
| Low SES | 0.312 | |||
| Absent | 5,925,197 (94.6) | 1570 (95.9) | 5,926,767 (94.6) | |
| Present | 336,076 (5.4) | 67 (4.1) | 336,143 (5.4) | |
| CCI | 0.026 | |||
| 0 | 3,887,857 (62.1) | 1245 (76.1) | 3,889,102 (62.1) | |
| 1 | 1,133,071 (18.1) | 224 (13.7) | 1,133,295 (18.1) | |
| 2 | 730,774 (11.7) | 118 (7.2) | 730,892 (11.7) | |
| 3~ | 509,571 (8.1) | 50 (3.1) | 509,621 (8.1) | |
| Follicular cyst | <0.001 | |||
| Absent | 6,254,427 (99.9) | 1588 (97) | 6,256,015 (99.9) | |
| Present | 6846 (0.1) | 49 (3) | 6895 (0.1) | |
| Corpus luteal cyst | <0.001 | |||
| Absent | 6,211,163 (99.2) | 1153 (70.4) | 6,212,316 (99.2) | |
| Present | 50,110 (0.8) | 484 (29.6) | 50,594 (0.8) | |
| Benign neoplasm of ovary | <0.001 | |||
| Absent | 6,190,807 (98.9) | 760 (46.4) | 6,191,567 (98.9) | |
| Present | 70,466 (1.1) | 877 (53.6) | 71,343 (1.1) | |
| Right | 21,481 (0.3) | 353 (21.6) | 21,834 (0.3) | |
| Left | 19,523 (0.3) | 224 (13.7) | 19,747 (0.3) | |
| Unspecified | 26,528 (0.4) | 245 (15) | 26,773 (0.4) | |
| Pregnancy | <0.001 | |||
| Absent | 5,671,790 (90.6) | 1492 (91.1) | 5,673,282 (90.6) | |
| Present | 589,483 (9.4) | 145 (8.9) | 589,628 (9.4) | |
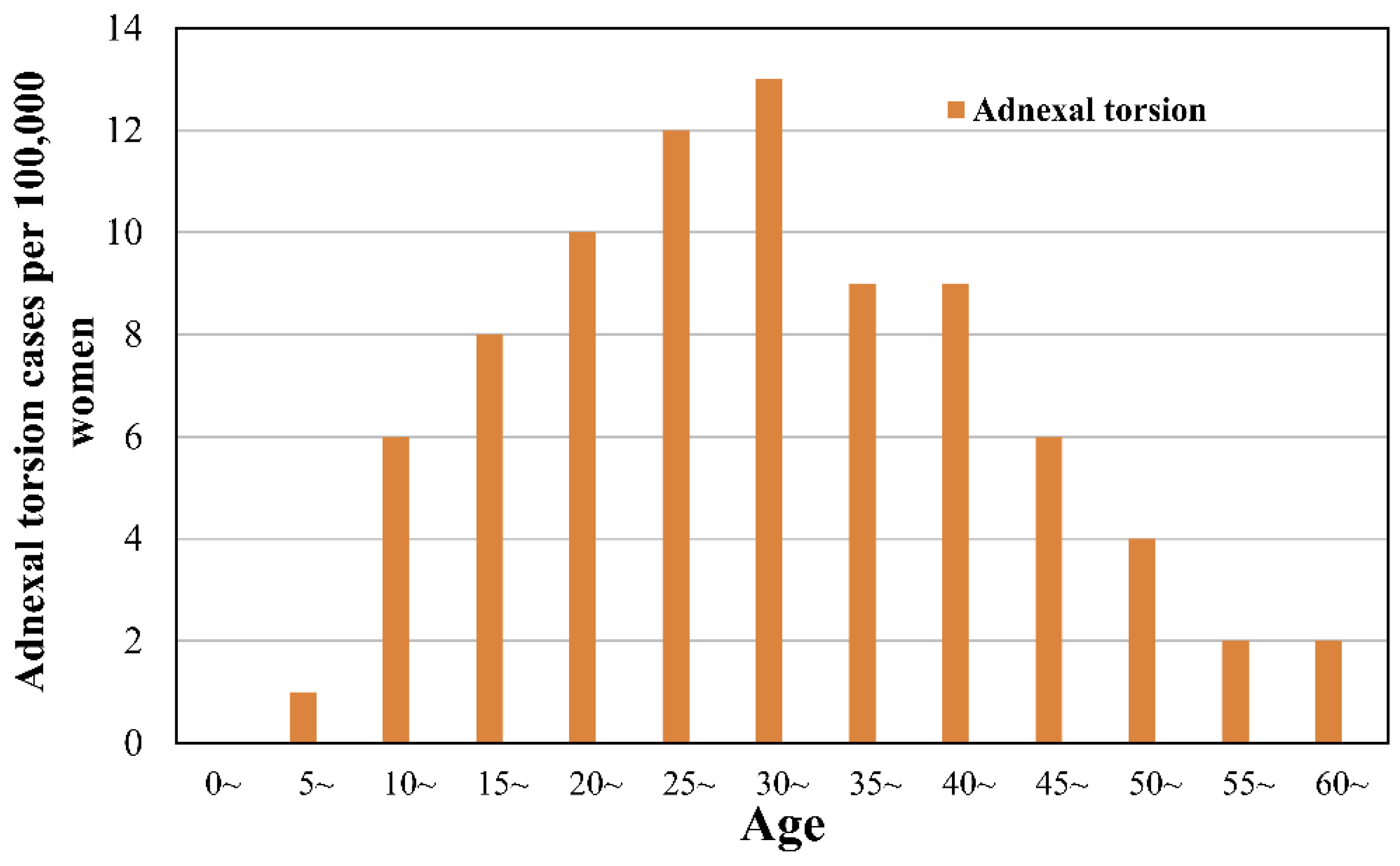
| Age | Adnexectomy | Oophorectomy or Benign Tumor Removal | Oophorectomy of Malignant Tumor | Ovarian Wedge Resection | Vaginal Drainage of Ovarian Cyst | Total | Adnexal Torsion per 100,000 Women |
|---|---|---|---|---|---|---|---|
| (N = 290) | (N = 1284) | (N = 8) | (N = 41) | (N = 14) | (N = 1637) | ||
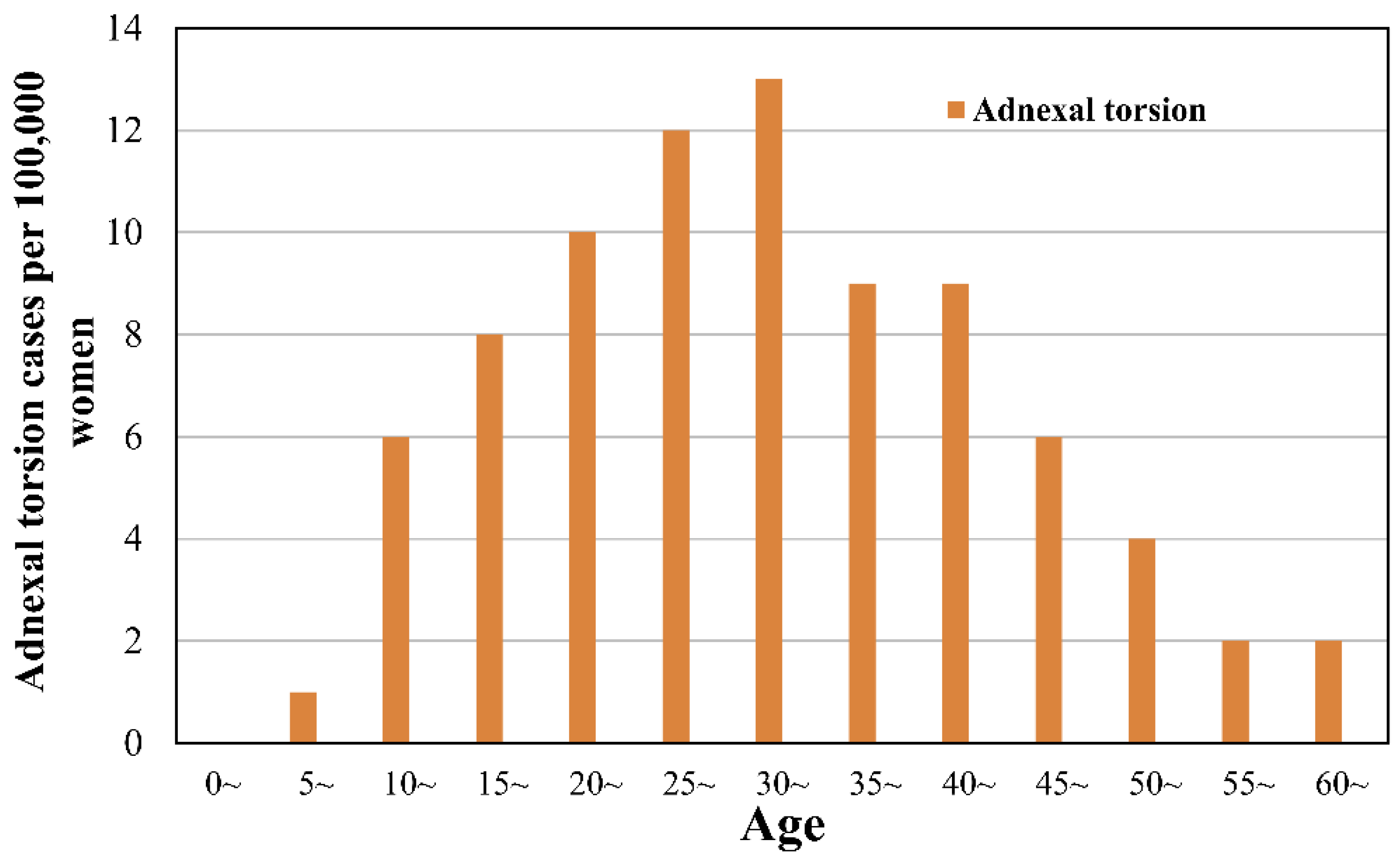
| ≤4 | 1 (0.3%) | 2 (0.2%) | 0 (0%) | 0 (0%) | 0 (0%) | 3 (0.2%) | 0 (0–1) |
| 5–9 | 1 (0.3%) | 14 (1.1%) | 0 (0%) | 0 (0%) | 0 (0%) | 15 (0.9%) | 1 (1–2) |
| 10–14 | 11 (3.8%) | 71 (5.5%) | 2 (25%) | 3 (7.3%) | 0 (0%) | 87 (5.3%) | 6 (5–7) |
| 15–19 | 10 (3.4%) | 111 (8.6%) | 2 (25%) | 4 (9.8%) | 3 (21.4%) | 130 (7.9%) | 8 (7–9) |
| 20–24 | 18 (6.2%) | 148 (11.5%) | 0 (0%) | 4 (9.8%) | 0 (0%) | 170 (10.4%) | 10 (9–12) |
| 25–29 | 31 (10.7%) | 178 (13.9%) | 2 (25%) | 8 (19.5%) | 1 (7.1%) | 220 (13.4%) | 12 (10–14) |
| 30–34 | 29 (10%) | 222 (17.3%) | 0 (0%) | 12 (29.3%) | 4 (28.6%) | 267 (16.3%) | 13 (11–14) |
| 35–39 | 42 (14.5%) | 137 (10.7%) | 1 (12.5%) | 6 (14.6%) | 2 (14.3%) | 188 (11.5%) | 9 (7–10) |
| 40–44 | 55 (19%) | 136 (10.6%) | 0 (0%) | 2 (4.9%) | 1 (7.1%) | 194 (11.9%) | 9 (7–10) |
| 45–49 | 38 (13.1%) | 94 (7.3%) | 0 (0%) | 1 (2.4%) | 2 (14.3%) | 135 (8.2%) | 6 (5–7) |
| 50–54 | 26 (9%) | 71 (5.5%) | 0 (0%) | 1 (2.4%) | 0 (0%) | 98 (6%) | 4 (3–5) |
| 55–59 | 8 (2.8%) | 31 (2.4%) | 0 (0%) | 0 (0%) | 0 (0%) | 39 (2.4%) | 2 (1–3) |
| 60–64 | 7 (2.4%) | 21 (1.6%) | 1 (12.5%) | 0 (0%) | 0 (0%) | 29 (1.8%) | 2 (1–3) |
| 65–69 | 4 (1.4%) | 14 (1.1%) | 0 (0%) | 0 (0%) | 0 (0%) | 18 (1.1%) | 1 (1–2) |
| 70–74 | 3 (1%) | 16 (1.2%) | 0 (0%) | 0 (0%) | 1 (7.1%) | 20 (1.2%) | 2 (1–3) |
| ≥75 | 6 (2.1%) | 18 (1.4%) | 0 (0%) | 0 (0%) | 0 (0%) | 24 (1.5%) | 1 (1–2) |
| Adnexal Torsion | ||||
|---|---|---|---|---|
| Unadjusted OR (95% CI) | p | Adjusted OR (95% CI) | p | |
| Model 1 a | ||||
| Age per 5 years | 0.922 (0.879–0.948) | <0.001 | 0.91 (0.88–0.94) | <0.001 |
| Low SES | 1.337 (0.59–3.029) | 0.487 | 1.58 (0.7–3.56) | 0.268 |
| CCI | ||||
| 1 | 0.636 (0.371–1.092) | 0.101 | 0.67 (0.39–1.15) | 0.144 |
| 2 | 1.18 (0.663–2.098) | 0.574 | 0.67 (0.39–1.15) | 0.144 |
| 3~ | 0.752 (0.277–2.04) | 0.575 | 1.72 (0.94–3.17) | 0.079 |
| Pregnancy | 1.834 (0.809–4.155) | 0.146 | 1.66 (0.73–3.76) | 0.228 |
| Model 2 b | ||||
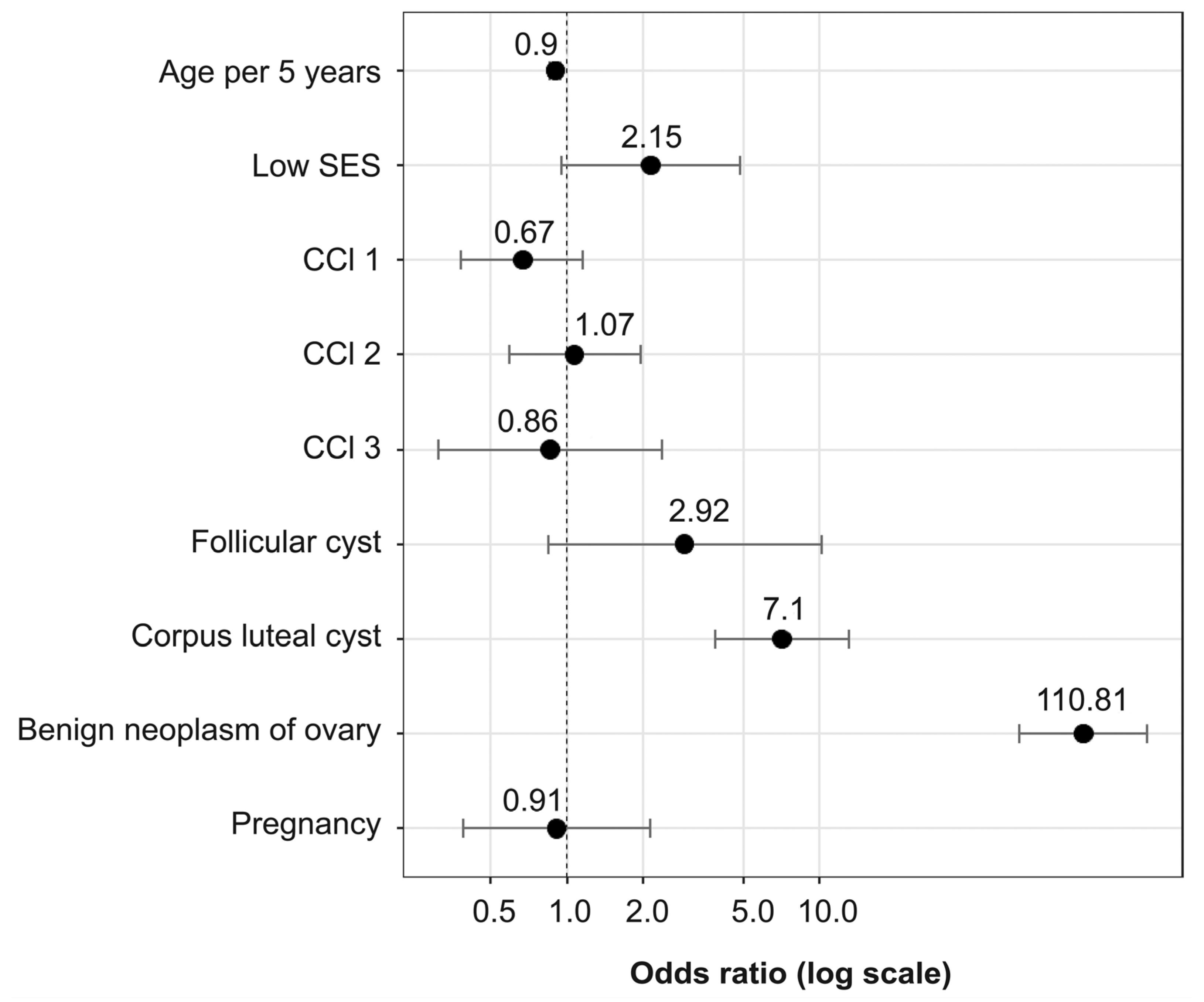
| Age per 5 years | 0.922 (0.879–0.948) | <0.001 | 0.9 (0.85–0.94) | <0.001 |
| Low SES | 1.337 (0.59–3.029) | 0.487 | 2.15 (0.95–4.83) | 0.066 |
| CCI | ||||
| 1 | 0.636 (0.371–1.092) | 0.101 | 0.67 (0.38–1.16) | 0.149 |
| 2 | 1.18 (0.663–2.098) | 0.574 | 1.07 (0.59–1.96) | 0.826 |
| 3~ | 0.752 (0.277–2.04) | 0.575 | 0.86 (0.31–2.37) | 0.772 |
| Follicular cyst | 58.922 (21.573–160.932) | <0.001 | 2.92 (0.84–10.17) | 0.092 |
| Corpus luteal cyst | 101.877 (71.53–145.1) | <0.001 | 7.1 (3.87–13.01) | <0.001 |
| Benign neoplasm of ovary | 202.915 (144.76–284.434) | <0.001 | 110.81 (61.77–198.80) | <0.001 |
| Pregnancy | 1.834 (0.809–4.155) | 0.146 | 0.91 (0.39–2.14) | 0.828 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuk, J.-S.; Yang, S.-W.; Lee, M.-H.; Kyung, M.-S. Incidence of Adnexal Torsion in the Republic of Korea: A Nationwide Serial Cross-Sectional Study (2009–2018). J. Pers. Med. 2021, 11, 743. https://doi.org/10.3390/jpm11080743
Yuk J-S, Yang S-W, Lee M-H, Kyung M-S. Incidence of Adnexal Torsion in the Republic of Korea: A Nationwide Serial Cross-Sectional Study (2009–2018). Journal of Personalized Medicine. 2021; 11(8):743. https://doi.org/10.3390/jpm11080743
Chicago/Turabian StyleYuk, Jin-Sung, Seung-Woo Yang, Myung-Hwa Lee, and Min-Sun Kyung. 2021. "Incidence of Adnexal Torsion in the Republic of Korea: A Nationwide Serial Cross-Sectional Study (2009–2018)" Journal of Personalized Medicine 11, no. 8: 743. https://doi.org/10.3390/jpm11080743
APA StyleYuk, J.-S., Yang, S.-W., Lee, M.-H., & Kyung, M.-S. (2021). Incidence of Adnexal Torsion in the Republic of Korea: A Nationwide Serial Cross-Sectional Study (2009–2018). Journal of Personalized Medicine, 11(8), 743. https://doi.org/10.3390/jpm11080743