Anti-Inflammatory Effects of Amantadine and Memantine: Possible Therapeutics for the Treatment of Covid-19?

 ,
,  , and
, and 
Abstract
1. Introduction
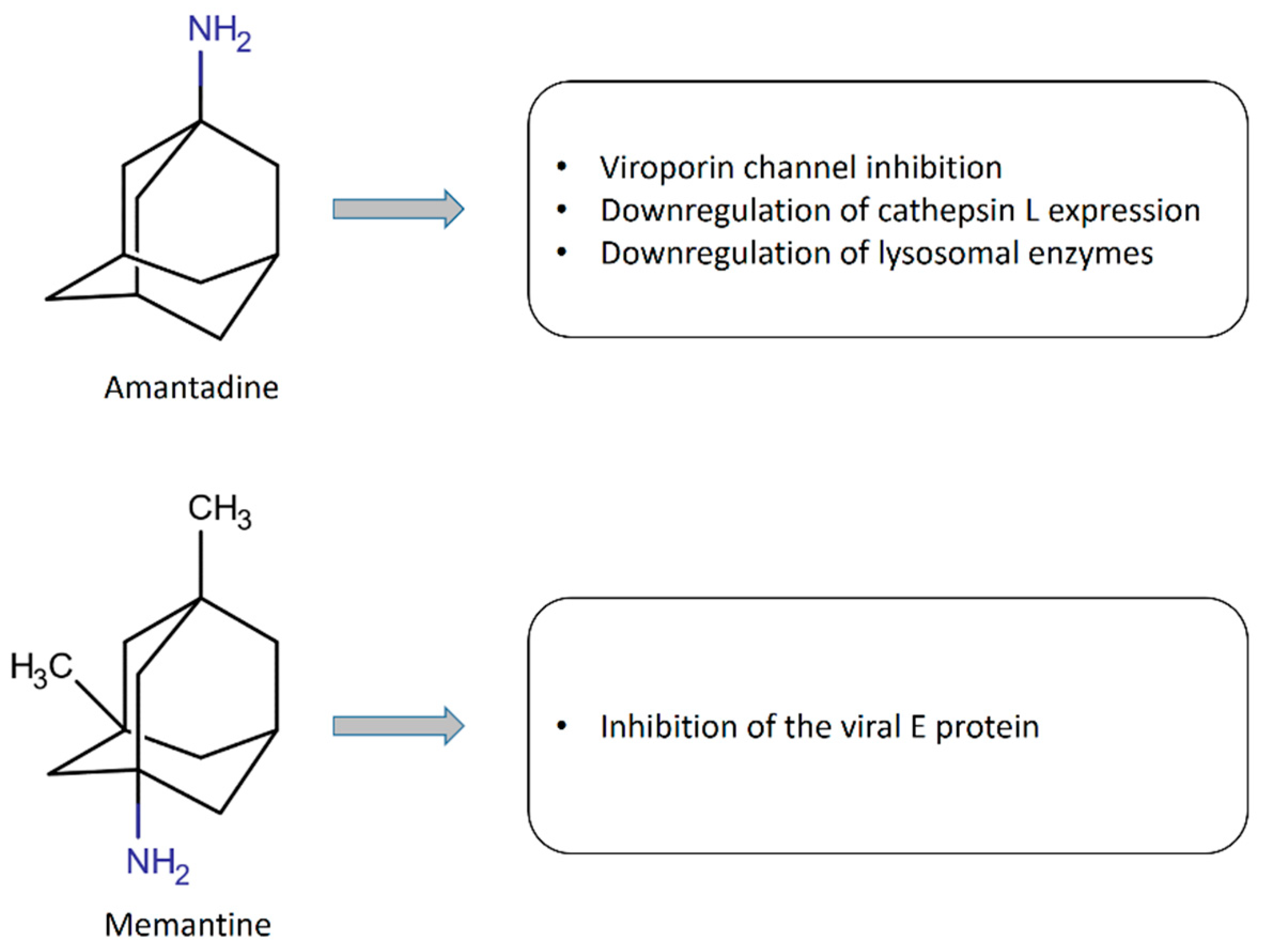
2. Anti-Inflammatory Effects of Amantadine
3. Anti-Inflammatory Effects of Memantine
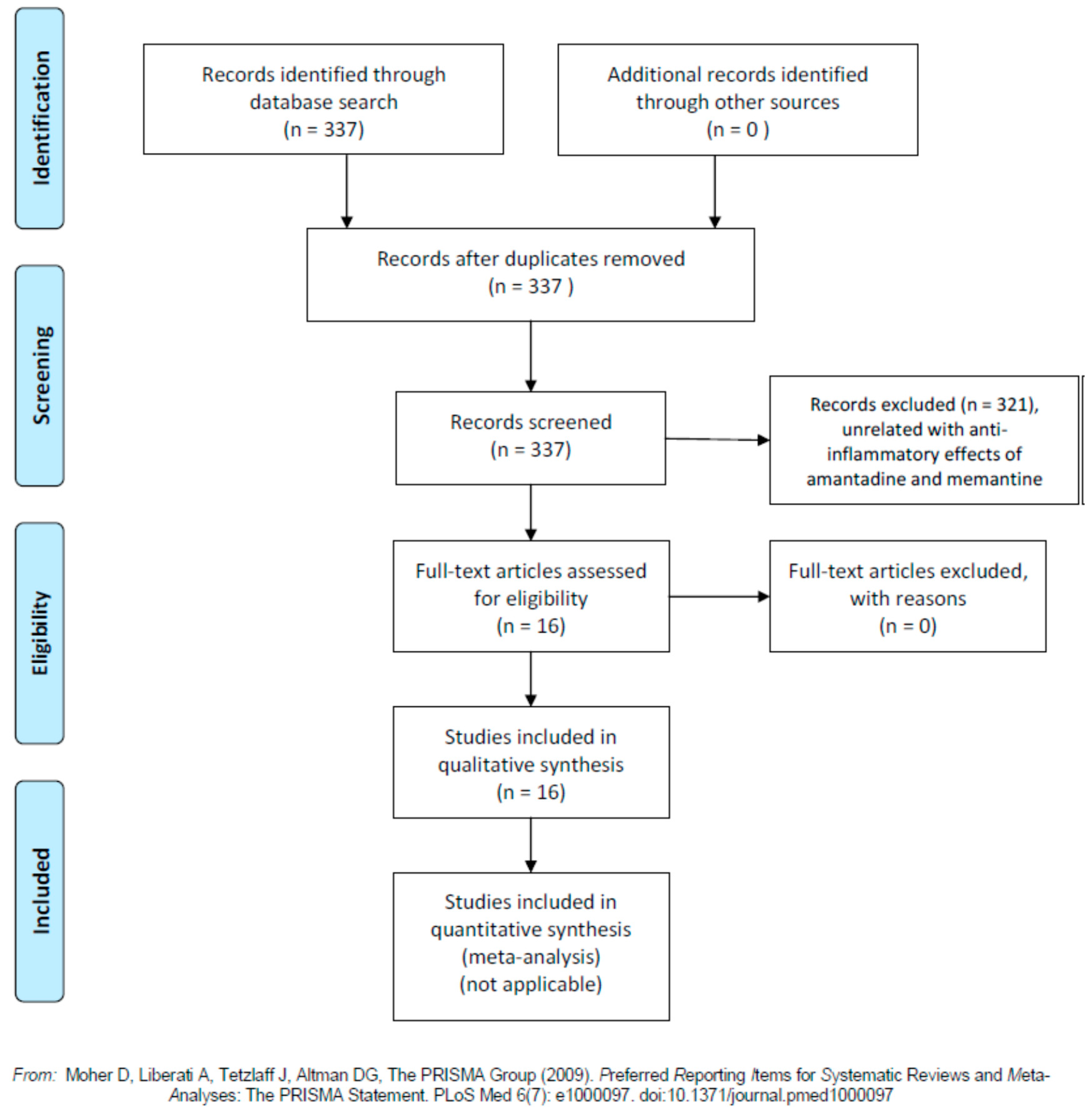
4. Amantadine, Memantine, and COVID-19
5. Discussion, Conclusions, and Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s disease |
| ALT | alanine aminotransferase |
| Arc | activity-regulated cytoskeletal associated associated protein |
| BBB | blood-brain barrier |
| BDNF | brain derived neurotrophic factor |
| CaMKIIα | calcium/calmodulin-dependent protein kinase II subunit α |
| CCK8 | cholecystokinin8 |
| CLP | cecal ligation and puncture |
| CREB protein | cyclic AMP-response element-binding protein |
| COVID-19 | coronavirus disease 2019 |
| CSF | Cerebrospinal fluid |
| CTSL | cathepsin L |
| CytC | Cytochrome C |
| DAT | Dopamine transporter |
| EAE | experimental allergic encephalomyelitis |
| ERK1/2 | extracellular signal-regulated kinase1/2 |
| ETR. | end-of-treatment response |
| GDNF | glial-derived neurotrophic factor |
| 5-HT | Serotonin |
| 5-HT3 | serotoninergic type 3 receptor |
| HBMVE | human brain microvascular endothelial |
| HSPP60 | heat shock protein 60 |
| ICAM-1 | intercellular adhesion molecule-1 |
| IFNα2b | interferon α2b |
| IFNγ | interferon γ |
| IL-1β | interleukin-1β |
| IL-6 | interleukin 6 |
| iNOS | Inducible nitric oxide synthase |
| JNK | c-Jun-NH2-terminal kinase |
| LDH | Lactic dehydrogenase |
| LPS | Lipopolysaccharide |
| mGLUr | metabotropic glutamatergic receptor |
| MPP+ | 1-methyl-phenyl-pyridinium ion |
| mRNA | messenger ribonucleic acid |
| NF-κB | nuclear factor-κB |
| NMDA | N-methyl-D-aspartate |
| NMDAR1 or NR1 | NMDA receptor 1 |
| Nurr77 | reversing nerve growth factor IB |
| 6-OHDA | 6-hydroxydopamine |
| PGE2 | Prostaglandin E2 |
| p38 MAP | p38 mitogen-activated protein |
| PD | Parkinson’s disease |
| PCR | polymerase chain reaction |
| PI3K | phosphatidylinositol 3 kinase |
| RANTES | regulated on activation normal T cell expressed and secreted |
| RT-PCR | real-time polymerase chain reaction |
| SARS-CoV | severe acute respiratory syndrome coronaviruses |
| SARS-CoV-2 | coronavirus responsible for COVID-19 |
| SCI | Spinal cord injury |
| STZ | streptozotocin |
| SVR | sustained virological response |
| TLRs | toll-like receptors |
| TNF-α | tumour necrosis α |
| VCAM-1 | vascular cell adhesion molecule-1 |
References
- Chang, C.; Ramphul, K. Amantadine. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Cady, S.D.; Schmidt-Rohr, K.; Wang, J.; Soto, C.S.; Degrado, W.F.; Hong, M. Structure of the amantadine binding site of influenza M2 proton channels in lipid bilayers. Nature 2010, 463, 689–692. [Google Scholar] [CrossRef]
- Müller, T.; Kuhn, W.; Möhr, J.D. Evaluating ADS5102 (amantadine) for the treatment of Parkinson’s disease patients with dyskinesia. Expert Opin. Pharmacother. 2019, 20, 1181–1187. [Google Scholar] [CrossRef]
- Perez, D.Q.; Espiritu, A.I.; Jamora, R.D.G. Efficacy and safety of amantadine for the treatment of fatigue in multiple sclerosis: A systematic review and meta-analysis. Neurodegener. Dis. Manag. 2020, 10, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Whyte, J.; Bagiella, E.; Kalmar, K.; Childs, N.; Khademi, A.; Eifert, B.; Long, D.; Katz, D.I.; Cho, S.; et al. Placebo-controlled trial of amantadine for severe traumatic brain injury. N. Engl. J. Med. 2012, 366, 819–826. [Google Scholar] [CrossRef]
- Gao, Y.; Zhang, Y.; Li, Z.; Ma, L.; Yang, J. Persistent vegetative state after severe cerebral hemorrhage treated with amantadine: A retrospective controlled study. Medicine 2020, 99, e21822. [Google Scholar] [CrossRef]
- Tanaka, M.; Bohár, Z.; Vécsei, L. Are kynurenines accomplices or principal villains in dementia? Maintenance of kynurenine metabolism. Molecules 2020, 25, 564. [Google Scholar] [CrossRef]
- Matsunaga, S.; Kishi, T.; Nomura, I.; Sakuma, K.; Okuya, M.; Ikuta, T.; Iwata, N. The efficacy and safety of memantine for the treatment of Alzheimer’s disease. Expert Opin. Drug Saf. 2018, 17, 1053–1061. [Google Scholar] [CrossRef]
- Kishi, T.; Matsunaga, S.; Iwata, N. Memantine treatment for Japanese patients with moderate to severe Alzheimer’s disease: A meta-analysis of double-blind, randomized, placebo-controlled trials. Neuropsychiatr. Dis. Treat. 2018, 14, 2915–2922. [Google Scholar] [CrossRef]
- Kumar, S. Memantine: Pharmacological properties and clinical uses. Neurol. India 2004, 52, 307–309. [Google Scholar]
- Kumar, M.; Taki, K.; Gahlot, R.; Sharma, A.; Dhangar, K. A chronicle of SARS-CoV-2: Part-I—Epidemiology, diagnosis, prognosis, transmission and treatment. Sci. Total Environ. 2020, 734, 139278. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Perrillo, R.P. The roles of amantadine, rimantadine, ursodeoxycholic acid, and NSAIDs, alone or in combination with alpha interferons, in the treatment of chronic hepatitis C. Semin. Liver Dis. 1999, 19 (Suppl. 1), 95–102. [Google Scholar]
- Malnick, S.D.; Beergabel, M.; Lurie, Y. Treatment of chronic hepatitis C virus infection. Ann. Pharmacother. 2000, 34, 1156–1164. [Google Scholar] [CrossRef]
- Gelderblom, H.C.; Reesink, H.W.; Beld, M.G.; Weegink, C.J.; Jansen, P.L.; Dijkgraaf, M.G.; Zaaijer, H.L. Low-level HCV viraemia after initial response during antiviral therapy: Transcription-mediated amplification predicts treatment failure. Antivir. Ther. 2007, 12, 423–427. [Google Scholar] [PubMed]
- Palabıyıkoğlu, M.; Ormeci, N.; Ekiz, F.; Beyler, A.R.; Erdem, H.; Dökmeci, A.; Ozkan, H.; Köklü, S.; Coban, S. Amantadine in non-responder patients with chronic hepatitis C: A randomized prospective study. Hepatogastroenterology 2012, 59, 1911–1914. [Google Scholar]
- Younossi, Z.M.; McCullough, A.C.; Barnes, D.S.; Post, A.; Ong, J.P.; O’Shea, R.; Martin, L.M.; Bringman, D.; Farmer, D.; Levinthal, G.; et al. Pegylated interferon alpha-2b, ribavirin and amantadine for chronic hepatitis C. Dig. Dis. Sci. 2005, 50, 970–975. [Google Scholar] [CrossRef]
- Parolin, M.B.; Lacerda, M.A.; Lopes, R.W. Amantadine-HCL in the treatment of chronic hepatitis C in non-responders to alpha-interferon. Effect on ALT serum levels and viral load. Arq. Gastroenterol. 1999, 36, 63–67. (In Portuguese) [Google Scholar]
- Kamar, N.; Rostaing, L.; Sandres-Saune, K.; Ribes, D.; Durand, D.; Izopet, J. Amantadine therapy in renal transplant patients with hepatitis C virus infection. J. Clin. Virol. 2004, 30, 110–114. [Google Scholar] [CrossRef]
- Yagura, M.; Harada, H. Treatment of chronic hepatitis C patients with amantadine. J. Gastroenterol. 2001, 36, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Asai, Y.; Hashimoto, S.; Kujime, K.; Gon, Y.; Mizumura, K.; Shimizu, K.; Horie, T. Amantadine inhibits RANTES production by influenzavirus-infected human bronchial epithelial cells. Br. J. Pharmacol. 2001, 132, 918–924. [Google Scholar] [CrossRef]
- Sulkowski, G.; Dąbrowska-Bouta, B.; Chalimoniuk, M.; Strużyńska, L. Effects of antagonists of glutamate receptors on pro-inflammatory cytokines in the brain cortex of rats subjected to experimental autoimmune encephalomyelitis. J. Neuroimmunol. 2013, 261, 67–76. [Google Scholar] [CrossRef]
- Xing, W.; Huang, P.; Lu, Y.; Zeng, W.; Zuo, Z. Amantadine attenuates sepsis-induced cognitive dysfunction possibly not through inhibiting toll-like receptor 2. J. Mol. Med. 2018, 96, 391–402. [Google Scholar] [CrossRef]
- Dogan, G.; Karaca, O. N-methyl-D-aspartate receptor antagonists may ameliorate spinal cord injury by inhibiting oxidative stress: An experimental study in rats. Turk. Neurosurg. 2020, 30, 60–68. [Google Scholar] [CrossRef]
- Ossola, B.; Schendzielorz, N.; Chen, S.H.; Bird, G.S.; Tuominen, R.K.; Männistö, P.T.; Hong, J.S. Amantadine protects dopamine neurons by a dual action: Reducing activation of microglia and inducing expression of GDNF in astroglia. Neuropharmacology 2011, 61, 574–582. [Google Scholar] [CrossRef]
- Rosi, S.; Vazdarjanova, A.; Ramirez-Amaya, V.; Worley, P.F.; Barnes, C.A.; Wenk, G.L. Memantine protects against LPS-induced neuroinflammation, restores behaviorally-induced gene expression and spatial learning in the rat. Neuroscience 2006, 142, 1303–1315. [Google Scholar] [CrossRef]
- Wei, X.; Gao, H.; Zou, J.; Liu, X.; Chen, D.; Liao, J.; Xu, Y.; Ma, L.; Tang, B.; Zhang, Z.; et al. Contra-directional coupling of Nur77 and Nurr1 in neurodegeneration: A novel mechanism for memantine-induced anti-inflammation and anti-mitochondrial impairment. Mol. Neurobiol. 2016, 53, 5876–5892. [Google Scholar] [CrossRef]
- Wang, F.; Zou, Z.; Gong, Y.; Yuan, D.; Chen, X.; Sun, T. Regulation of human brain microvascular endothelial cell adhesion and barrier functions by memantine. J. Mol. Neurosci. 2017, 62, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Q.; Fang, L.; Feng, D.; Tang, S.; Yue, S.; Huang, Y.; Han, J.; Lan, J.; Liu, W.; Gao, L.; et al. Memantine ameliorates pulmonary inflammation in a mice model of COPD induced by cigarette smoke combined with LPS. Biomed. Pharmacother. 2019, 109, 2005–2013. [Google Scholar] [CrossRef]
- Mishra, S.K.; Hidau, M.; Rai, S. Memantine and Ibuprofen pretreatment exerts anti-inflammatory effect against streptozotocin-induced astroglial inflammation via modulation of NMDA receptor-associated downstream calcium ion signaling. Inflammopharmacology 2020. [Google Scholar] [CrossRef]
- Tipton, P.W.; Wszolek, Z.K. What can Parkinson’s disease teach us about COVID-19? Neurol. Neurochir. Pol. 2020, 54, 204–206. [Google Scholar] [CrossRef]
- Smieszek, S.P.; Przychodzen, B.P.; Polymeropoulos, M.H. Amantadine disrupts lysosomal gene expression: A hypothesis for COVID19 treatment. Int. J. Antimicrob. Agents 2020, 2020, 106004. [Google Scholar] [CrossRef]
- Abreu, G.E.A.; Aguilar, M.E.H.; Covarrubias, D.H.; Durán, F.R. Amantadine as a drug to mitigate the effects of COVID-19. Med. Hypotheses 2020, 140, 109755. [Google Scholar] [CrossRef]
- Singh Tomar, P.P.; Arkin, I.T. SARS-CoV-2 E protein is a potential ion channel that can be inhibited by Gliclazide and Memantine. Biochem. Biophys. Res. Commun. 2020, 530, 10–14. [Google Scholar] [CrossRef]
- Rejdak, K.; Grieb, P. Adamantanes might be protective from COVID-19 in patients with neurological diseases, multiple sclerosis, parkinsonism and cognitive impairment. Mult. Scler. Relat. Disord. 2020, 42, 102163. [Google Scholar] [CrossRef] [PubMed]
- Aranda-Abreu, G.E.; Aranda-Martínez, J.D.; Araújo, R.; Hernández-Aguilar, M.E.; Herrera-Covarrubias, D.; Rojas-Durán, F. Observational study of people infected with SARS-Cov-2, treated with amantadine. Pharmacol. Rep. 2020, 1–4. [Google Scholar] [CrossRef]
- Konstantinidou, S.K.; Papanastasiou, I.P. Repurposing current therapeutic regimens against SARS-CoV-2 (Review). Exp. Ther. Med. 2020, 20, 1845–1855. [Google Scholar] [CrossRef]
- Sarkar, C.; Mondal, M.; Torequl Islam, M.; Martorell, M.; Docea, A.O.; Maroyi, A.; Sharifi-Rad, J.; Calina, D. Potential therapeutic options for COVID-19: Current status, challenges, and future perspectives. Front. Pharmacol. 2020, 11, 572870. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in hospitalized patients with Covid-19—Preliminary report. N. Engl. J. Med. 2020, NEJMoa2021436. [Google Scholar] [CrossRef]
- Budhathoki, P.; Shrestha, D.B.; Rawal, E.; Khadka, S. Corticosteroids in COVID-19: Is it rational? A Systematic review and meta-analysis. SN Compr. Clin. Med. 2020, 1–21. [Google Scholar] [CrossRef]
- Million, M.; Lagier, J.C.; Gautret, P.; Hocquart, M.; Morgane, M.; Esteves-Vieira, V.; Doudier, B.; Aubry, C.; Correard, F.; Giraud-Gatineau, A.; et al. Early treatment of COVID-19 patients with hydroxychloroquine and azithromycin: A retrospective analysis of 1061 cases in Marseille, France. Travel Med. Infect. Dis. 2020, 37, 101738. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado-Lavín, A.; Olmos, J.M.; Cifrian, J.M.; Gimenez, T.; Gandarillas, M.A.; García-Saiz, M.; Rebollo, M.H.; Martínez-Taboada, V.; López-Hoyos, M.; Fariñas, M.C.; et al. Controlled, double-blind, randomized trial to assess the efficacy and safety of hydroxychloroquine chemoprophylaxis in SARS CoV2 infection in healthcare personnel in the hospital setting: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 472. [Google Scholar]



{kind=link}
{kind=link}
| Authors, Year [Ref] | Country | Model | Study Design | Main Findings |
|---|---|---|---|---|
| Gelderblom et al., 2007 [14] | The Netherlands | Human hepatitis C | Open-label, single-arm study. 57 patients with initial viral response to IFNα2b but with the reappearance of low-level HCV RNA at weeks 16 to 20. Initial induction therapy with amantadine, IFNα2b, and ribavirin during 6 weeks, and substitution of IFNα2b for pegylated IFNα2b later with a follow-up period of 24–48 weeks | 34 patients (59.6%) showed sustained virological response (SVR) and the other 23 (40.4%) showed breakthrough or relapse. |
| Palabıyıkoğlu et al., 2012 [15] | Turkey | Human hepatitis C | Randomized controlled trial involving 43 patients who did not respond previously to the combination IFNα-2a plus ribavirin for 48 weeks. Treatment with pegylated IFN-α2a (180 μg/kg /week) plus ribavirin (1000–1200 mg/day) and amantadine (200mg/day, 21 patients) or with amantadine alone (200mg/day, 22 patients) for 48 weeks | Significantly higher frequency of SVR in a group of 21 patients treated with pegylated IFN-α2a + ribavirin + amantadine than in the other group of 22 patients treated with amantadine alone. |
| Younossi et al., 2005 [16] | United States of America | Human hepatitis C | Multi-centre, open-label clinical trial involving 168 patients (69 drug-naïve and 99 non-responders to previous therapy, 32 of them to IFN-α only and 67 to IFN-α plus ribavirin). Both groups started therapy with pegylated IFN-α2b (1.5 μg/kg week), ribavirin (1000–1200 mg/day), and amantadine (200 mg/day), for 4 weeks, followed by pegylated IFN-α2b (0.5 μg/kg week ribavirin (1000–1200 mg/day), and amantadine (200 mg/day), for another 20 weeks. Patients with undetectable HCV RNA at week 24 continued this regimen for a total of 48 weeks and were followed for another 24 weeks. Patients with undetectable virus (<50 IU/mL) after 24 weeks of follow-up were considered to have SVR. | Of the entire cohort, 35 (21%) discontinued early due to side effects or loss to follow-up. SVR and end-of-treatment virological response (ETR) in 47.8% 34.3% and of patients of the drug-naïve group vs in 28.6% and 19.4% for the group who had previously failed to respond to a course of treatment (p = 0.01). |
| Parolin et al., 1999 [17] | Brazil | Human hepatitis C | Open-label study involving 18 patients with hepatitis C non-responders to IFN-α. Treatment with amantadine 200 mg/day. | No significant reduction of serum alanine aminotransferase levels and of viral load between baseline and final values |
| Kamar et al., 2004 [18] | France | Human hepatitis C | Open pilot study involving 8 hepatitis C virus-positive renal-transplant patients with chronic active hepatitis and increased alanine aminotransferase (ALT) levels. Treatment with amantadine 200 mg/day. Follow-up of 6 months. | Non-significant decrease in hepatitis C viremia, in aspartate aminotransferase activity, and no changes in liver histology. Significant decrease in ALT activity |
| Yagura & Harada, 2001 [19] | Japan | Human hepatitis C | Open-label prospective study involving 25 drug-naïve and 33 non-responders to IFN-α. Treatment with amantadine 100 mg/day during 4 months and 200 mg/day during the subsequent 2 months. | Reduction of ALT levels in 75% of patients at 4 months and 85% at 6 months after therapy. HCV RNA levels did not modify during the treatment period. |
| Asai et al., 2001 [20] | Japan | Bronchial epithelial cells cultures | Infection of bronchial epithelial cells in culture with influenza virus and amantadine. Measurement of p38 MAP kinase and JNK activation in the cells and RANTES concentrations in the culture supernatants | Amantadine-induced inhibition of virus replication decreased p38 MAP kinase and JNK activity and expression of RANTES in infected cells. Amantadine did not inhibit p38 MAP kinase and JNK activation induced by tumour necrosis factor α (TNF-α). |
| Sulkowski et al. 2013 [21] | Poland | Female rats with experimental allergic encephalomyelitis (EAE) | Screening analysis of inflammatory mediators (cytokines and chemokines) in control rats, rats with untreated EAE, and groups rats of EAE treated with amantadine (100 mg/kg b.w./day), memantine (60 mg/kg b.w./day), LY 367385 (10 mg/kg b.w./day, an antagonist of mGluR1) or MPEP (10 mg/kg b.w./day, an mGluR5 antagonist) | Amantadine and memantine suppressed neurological symptoms of disease in EAE rats and reduced expression of pro-inflammatory cytokines in the brain, while antagonists of metabotropic glutamate receptors (mGluR) did not affect the inflammatory process and the neurological symptoms of EAE rats. |
| Xing et al., 2018 [22] | United States of America and China | Experimental model of sepsis-induced cognitive dysfunction by caecal ligation and puncture (CLP) in male mice | Measurements of learning and memory, and brain cortex expression of several mediators of inflammation in mice controls (not being exposed to surgery or any drugs), mice treated with amantadine, CLP, or CLP plus amantadine 1 (the first dose of amantadine was given intraperitoneally 15 min before the surgery to create CLP), and CLP plus amantadine 2 (the first dose of amantadine was given intraperitoneally 6 h after the creation of CLP). | Amantadine attenuated CLP-induced neuroinflammation in the hippocampus (i.e., interleukin (IL-1β and IL-6 levels) and dysfunction of learning and memory, but did not have significant effects on the expression of toll-like receptors (TLRs) |
| Dogan & Karaka, 2020 [23] | Turkey | Experimental spinal cord injury in male rats | Spinal cord injury (SCI) induced by removing spinous processes and laminar arcs of T5–12 followed by laminectomy T11-T12 and compression with a clip for 60 s at this level. Measurement of oxidative stress, inflammation, and angiogenesis markers (histological examination of spinal cord sections) in control rats, rats with SCI, and rats with SCI treated with amantadine. | Amantadine had an inhibitory effect of oxidative stress, inflammation, and apoptosis, and ameliorated SCI effects by inducing angiogenesis. |
| Ossola et al., 2011 [24] | Finland and the United States of America | Primary cultures with different composition of neurons, microglia, and astroglia obtained from the mesencephalon of female rats | Treatment of primary cultures with two dopaminergic neurotoxins: lipopolysaccharides (LPS) and 1-methyl-phenylpyridinim ion (MPP+). Measurement of production of tumour necrosis factor-alpha, Prostaglandin E2 (PGE2) release, nitric oxide (NO) production, glial-derived neurotrophic factor (GDNF) gene expression, and changes in intracellular Ca2+. | Amantadine protected rat midbrain cultures from MPP+ and LPS toxicity by inhibiting the release of microglial pro-inflammatory factors, and increasing the expression of GDNF in astroglia, while NMDA receptor inhibition was not related to the neuroprotective effect. |
| Authors, Year [Ref] | Country | Model | Study Design | Main Findings |
|---|---|---|---|---|
| Sulkowski et al. 2013 [21] | Poland | Female rats with experimental allergic encephalomyelitis (EAE) | Screening analysis of inflammatory mediators (cytokines and chemokines) in control rats, rats with untreated EAE, and groups rats of EAE treated with amantadine (100 mg/kg b.w./day), memantine (60 mg/kg b.w./day), LY 367385 (10 mg/kg b.w./day, an antagonist of mGluR1) or MPEP (10 mg/kg b.w./day, an mGluR5 antagonist) | Amantadine and memantine suppressed neurological symptoms of disease in EAE rats and reduced expression of pro-inflammatory cytokines in the brain, while antagonists of metabotropic glutamate receptors (mGluR) did not affect the inflammatory process and the neurological symptoms of EAE rats. |
| Rosi et al. 2006 [25] | Italy | Neuroinflammation induced by chronic LPS infusion into the 4th ventricle of rats | Behavioural testing, histological examination, immunofluorescence studies, fluorescence in situ hybridization and confocal microscopy in the dorsal hippocampus in two groups: (LPS-infused; LPS-infused + memantine; and CSF-infused) and caged control groups (LPS-infused; LPS-infused + memantine; and artificial CSF-infused) | Memantine treatment attenuated LPS-induced spatial learning and memory impairments, reduced the number of activated microglia in the hippocampus without affecting resident microglia, and returned Arc (activity-regulated cytoskeletal associated protein) expressing neuronal populations to control levels after LPS-infusion |
| Wei et al., 2016 [26] | China | 6-hydroxydopamine (OHDA)-lesioned PC12 cells | 4 experimental groups treated with either Dulbecco’s modified Eagle’s medium), memantine (10 μM), 6-OHDA (100 μM), or 6-OHDA (100 μM) plus memantine (10 μM). Quantification of PC12 cell death (via the CCK8 and the apoptotic cells) and measurement of lactic dehydrogenase (LDH), glutamate, IL-6, and TNF-α; immunofluorescence for Nurr1, Nur77, Cyt c, and HSP60; and protein extraction for Nurr1, Nur77, tyrosine hydroxylase (TH), dopamine transporter (DAT), brain-derived neurotrophic factor (BDNF), phosphatidylinositol 3 kinase (PI3K)/p-PI3K, AKT/p-AKT, Cyt c, Lamin B1, and β-actin. Inhibition of the extracellular signal-regulated protein kinases (ERK), c-JunN-terminal kinase (JNK) and p38 mitogen-activated protein kinases (MAPKs) | Memantine incubation prevented the increase of inflammatory mediators (IL-6, TNF-α) and oxidative predictors (glutamate and LDH release), reversed the decrease in the total level of Nurr1, and attenuated in a dose-dependent manner the increased level of Nur77, all induced by 6-OHDA in PC12 cells. Memantine decreased Cyt c and HSP60 release from mitochondria of PC12 cells. Memantine restored the reduced cell viability, attenuated the increased apoptosis, and restored the reduction in the levels of TH and DAT in 6-OHDA-lesioned PC12 cells |
| Wang et al., 2017 [27] | China | Primary human brain microvascular endothelial (HBMVE) cells cultures | Pre-treatment of HBMVEs with 10 or 20 μM memantine for 12 h (or 24 h) and incubation with 5 ng/mL TNF-α for another 12 h (or 24 h). Measurement of adhesion of Human monocytic leukaemia cell line THP-1 cells. | Pre-treatment with memantine caused an important suppression of TNF-α-induced binding of THP-1 cells to HBMVEs in a dose-dependent manner; rescued TNF-α-induced disruption and interfered with THP-1 cells transmigration across a blood-brain BBB model, and prevented the increased expression of cell adhesion molecules (ICAM-1, VCAM-1, and E-selectin) induced by TNF-α. |
| Cheng et al., 2019 [28] | China | Chronic obstruction pulmonary disease induced in mice by cigarette-smoking and LPS and Raw264.7 cells cultures | Four experimental groups for mice: controls, cigarette-smoking plus LPS, memantine, and cigarette-smoking plus LPS plus memantine. Determinations in plasma, bronchoalveolar lavage fluid, and lung tissues. Two experimental groups for Raw265.7 for cells: cigarette-smoking exposure plus LPS, and cigarette-smoking exposure plus LPS plus memantine. Measurement of Ca2+ influx, glutamate content, cytokines (TNF-α, IL-6, and IFN-γ) and proteins (p-ERK42/44, ERK1/2, p-AKT, NMDAR-1, xCT, GADPH) | Memantine attenuated significantly the increase in the release of cytokines (TNF-α, IL-6, and IFN-γ) and glutamate, and the increase of protein levels of NR-1 and xCT and Ca2+ influx, and the activation of the ERK1/2 pathway in the two models |
| Mishra et al., 2020 [29] | India | Neuroinflammation and memory impairment induced by intracerebroventricular injection of streptozotocin (STZ) in rats. | Experimental groups: controls, STZ, STZ plus ibuprofen (200 μM), and STZ plus memantine (5 µM). Measurement of the expression of NMDAR1, NMDAR2A, NMDAR2B, calcium/calmodulin-dependent protein kinase II subunit α (CaMKIIα), cyclic AMP-response element-binding (CREB) protein, Calpain, and Caspase 3; and levels of glial fibrillary acidic protein (GFAP), TNF-α, inducible nitric oxide synthase (iNOS), and IL-10. | Memantine (and not Ibuprofen) was able to prevent the increase in the expression of NMDAR1, NMDAR2B, Calpain, and Caspase 3 expression, and the decrease in the level of NMDAR2A, CaMKIIα, and CREB protein expression induced by STZ treatment. Memantine and ibuprofen restored the increase in the level of GFAP, TNF-α, and iNOS), and the decrease in the level of IL-10 induced by STZ treatment. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Jiménez, F.J.; Alonso-Navarro, H.; García-Martín, E.; Agúndez, J.A.G. Anti-Inflammatory Effects of Amantadine and Memantine: Possible Therapeutics for the Treatment of Covid-19? J. Pers. Med. 2020, 10, 217. https://doi.org/10.3390/jpm10040217
Jiménez-Jiménez FJ, Alonso-Navarro H, García-Martín E, Agúndez JAG. Anti-Inflammatory Effects of Amantadine and Memantine: Possible Therapeutics for the Treatment of Covid-19? Journal of Personalized Medicine. 2020; 10(4):217. https://doi.org/10.3390/jpm10040217
Chicago/Turabian StyleJiménez-Jiménez, Félix Javier, Hortensia Alonso-Navarro, Elena García-Martín, and José A. G. Agúndez. 2020. "Anti-Inflammatory Effects of Amantadine and Memantine: Possible Therapeutics for the Treatment of Covid-19?" Journal of Personalized Medicine 10, no. 4: 217. https://doi.org/10.3390/jpm10040217
APA StyleJiménez-Jiménez, F. J., Alonso-Navarro, H., García-Martín, E., & Agúndez, J. A. G. (2020). Anti-Inflammatory Effects of Amantadine and Memantine: Possible Therapeutics for the Treatment of Covid-19? Journal of Personalized Medicine, 10(4), 217. https://doi.org/10.3390/jpm10040217