Associations between IL-6 and Echo-Parameters in Patients with Early Onset Coronary Artery Disease

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study and Control Group
2.2. Blood Samples and Biochemical Measurements
2.3. Measurement of IL-6 Concentration
2.4. Anthropometric Parameters
2.5. Echocardiography
2.6. Doppler Ultrasound of Carotid and Peripheral Arteries
2.7. Statistical Analysis
3. Results
3.1. The Characteristics of the Group of Patients with Early Onset CAD
3.2. The Comparison of Biochemical Parameters of the Study and Control Groups
3.3. The Correlations between Plasma IL-6 Concentration and Biochemical and Clinical Parameters in Patients with Early Onset CAD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wainstein, M.V.; Mossmann, M.; Araujo, G.N.; Gonçalves, S.C.; Gravina, G.L.; Sangalli, M.; Veadrigo, F.; Matte, R.; Reich, R.; Costa, F.G.; et al. Elevated serum interleukin-6 is predictive of coronary artery disease in intermediate risk overweight patients referred for coronary angiography. Diabetol. Metab. Syndr. 2017, 9, 67. [Google Scholar] [CrossRef] [PubMed]
- Statistics Poland, Statistical Products Department. Death by causes. In Statistical Yearbook of the Republic of Poland 2018; Rozkrut, D., Ed.; Statistical Publishing Establishment: Warsaw, Poland, 2018; p. 221. [Google Scholar]
- Aggarwal, A.; Srivastava, S.; Velmurugan, M. Newer perspectives of coronary artery disease in young. World J. Cardiol. 2016, 8, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.H.; Miller, J.I., 3rd; Sperling, L.S.; Weintraub, W.S. Long-term follow-up of coronary artery disease presenting in young adults. J. Am. Coll. Cardiol. 2003, 41, 521–528. [Google Scholar] [CrossRef]
- Bacchiega, B.C.; Bacchiega, A.B.; Usnayo, M.J.; Bedirian, R.; Singh, G.; Pinheiro, G.D. Interleukin 6 inhibition and coronary artery disease in a high-risk population: A prospective community-based clinical study. J. Am. Heart Assoc. 2017, 6, e005038. [Google Scholar] [CrossRef]
- Hongmei, Y.; Yongping, J.; Jiyuan, L. Interleukin-6 polymorphisms and risk of coronary artery diseases in a Chinese population: A case-control study. Pak. J. Med. Sci. 2016, 32, 880–885. [Google Scholar] [CrossRef]
- Al Shahi, H.; Shimada, K.; Miyauchi, K.; Yoshihara, T.; Sai, E.; Shiozawa, T.; Naito, R.; Aikawa, T.; Ouchi, S.; Kadoguchi, T.; et al. Elevated circulating levels of inflammatory markers in patients with acute coronary syndrome. Int. J. Vasc. Med. 2015, 2015, 805375. [Google Scholar] [CrossRef]
- Tousoulis, D.; Economou, E.K.; Oikonomou, E.; Papageorgiou, N.; Siasos, G.; Latsios, G.; Kokkou, E.; Mourouzis, K.; Papaioannou, S.; Deftereos, S.; et al. The role and predictive value of cytokines in atherosclerosis and coronary artery disease. Curr. Med. Chem. 2015, 22, 2636–2650. [Google Scholar] [CrossRef]
- Mowafy, A.; El-Akabawy, H.; Hussein, A.; Abd El Hay, A. Prognostic value of IL6 in young adults presenting with acute coronary syndrome. Egypt. Heart J. 2015, 67, 151–158. [Google Scholar] [CrossRef][Green Version]
- Reiss, A.B.; Siegart, N.M.; De Leon, J. Interleukin-6 in atherosclerosis: Atherogenic or atheroprotective? Clin. Lipidol. 2017, 12, 14–23. [Google Scholar] [CrossRef]
- Yudkin, J.S.; Kumari, M.; Humphries, S.E.; Mohamed-Ali, V. Inflammation, obesity, stress and coronary heart disease: Is interleukin-6 the link? Atherosclerosis 2000, 148, 209–214. [Google Scholar] [CrossRef]
- Su, D.; Li, Z.; Li, X.; Chen, Y.; Zhang, Y.; Ding, D.; Deng, X.; Xia, M.; Qiu, J.; Ling, W. Association between serum interleukin-6 concentration and mortality in patients with coronary artery disease. Mediat. Inflamm. 2013, 2013, 726178. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Valdes-Marquez, E.; Hill, M.; Gordon, J.; Farrall, M.; Hamsten, A.; Watkins, H.; Hopewell, J.C. Plasma cytokines and risk of coronary heart disease in the PROCARDIS study. Open Heart 2018, 5, e000807. [Google Scholar] [CrossRef] [PubMed]
- Caselli, C.; De Graaf, M.A.; Lorenzoni, V.; Rovai, D.; Marinelli, M.; Del Ry, S.; Giannessi, D.; Bax, J.J.; Neglia, D.; Scholte, A.J. HDL cholesterol, leptin and interleukin-6 predict high risk coronary anatomy assessed by CT angiography in patients with stable chest pain. Atherosclerosis 2015, 241, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Min, X.; Lu, M.; Tu, S.; Wang, X.; Zhou, C.; Wang, S.; Pang, S.; Qian, J.; Ge, Y.; Guo, Y.; et al. Serum cytokine profile in relation to the severity of coronary artery disease. Biomed. Res. Int. 2017, 2017, 4013685. [Google Scholar] [CrossRef]
- Fan, Z.X.; Hua, Q.; Li, Y.P.; Liu, R.K.; Yang, Z. Interleukin-6, but not soluble adhesion molecules, predicts a subsequent mortality from cardiovascular disease in patients with acute ST-segment elevation myocardial infarction. Cell Biochem. Biophys. 2011, 61, 443–448. [Google Scholar] [CrossRef]
- Hudzik, B.; Szkodzinski, J.; Romanowski, W.; Danikiewicz, A.; Wilczek, K.; Lekston, A.; Polonski, L.; Zubelewicz-Szkodzinska, B. Serum interleukin-6 concentration reflects the extent of asymptomatic left ventricular dysfunction and predicts progression to heart failure in patients with stable coronary artery disease. Cytokine 2011, 54, 266–271. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- De Simone, G.; Daniels, S.R.; Devereux, R.B.; Meyer, R.A.; Roman, M.J.; de Divitiis, O.; Alderman, M.H. Left ventricular mass and body size in normotensive children and adults: Assessment of allometric relations and impact of overweight. J. Am. Coll. Cardiol. 1992, 20, 1251–1260. [Google Scholar] [CrossRef]
- Todd, J.; Simpson, P.; Estis, J.; Torres, V.; Wub, A.H. Reference range and short- and long-term biological variation of interleukin (IL)-6, IL-17A and tissue necrosis factor-alpha using high sensitivity assays. Cytokine 2013, 64, 660–665. [Google Scholar] [CrossRef]
- Hennø, L.T.; Storjord, E.; Christiansen, D.; Bergseth, G.; Ludviksen, J.K.; Fure, H.; Barene, S.; Nielsen, E.W.; Mollnes, T.E.; Brekke, O.L. Effect of the anticoagulant, storage time and temperature of blood samples on the concentrations of 27 multiplex assayed cytokines—Consequences for defining reference values in healthy humans. Cytokine 2017, 97, 86–95. [Google Scholar] [CrossRef]
- Danesh, J.; Kaptoge, S.; Mann, A.G.; Sarwar, N.; Wood, A.; Angleman, S.B.; Wensley, F.; Higgins, J.P.; Lennon, L.; Eiriksdottir, G.; et al. Long-term interleukin-6 levels and subsequent risk of coronary heart disease: Two new prospective studies and a systematic review. PLoS Med. 2008, 5, e78. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Hao, M.; Tang, Y. Relationships among serum IL-6, TNF-α, CRP and coronary artery lesion in patients with acute myocardial infarction. Int. J. Clin. Exp. Med. 2018, 11, 6987–6992. [Google Scholar]
- Hartford, M.; Wiklund, O.; Hultén, L.M.; Perers, E.; Person, A.; Herlitz, J.; Hurt-Camejo, E.; Karlsson, T.; Caidahl, K. CRP, interleukin-6, secretory phospholipase A2 group IIA, and intercellular adhesion molecule-1 during the early phase of acute coronary syndromes and long-term follow-up. Int. J. Cardiol. 2006, 108, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Ziakas, A.; Gavrilidis, S.; Giannoglou, G.; Souliou, E.; Gemitzis, K.; Kalampalika, D.; Vayona, M.A.; Pidonia, I.; Parharidis, G.; Louridas, G. In-hospital and long-term prognostic value of fibrinogen, CRP, and IL-6 levels in patients with acute myocardial infarction treated with thrombolysis. Angiology 2006, 57, 283–293. [Google Scholar] [CrossRef]
- Groot, H.E.; Al Ali, L.; van der Horst, I.C.C.; Schurer, R.A.J.; van der Werf, H.W.; Lipsic, E.; van Veldhuisen, D.J.; Karper, J.C.; van der Harst, P. Plasma interleukin 6 levels are associated with cardiac function after ST-elevation myocardial infarction. Clin. Res. Cardiol. 2018, 57, 283–293. [Google Scholar] [CrossRef]
- Picciotto, S.; Forastiere, F.; Pistelli, R.; Koenig, W.; Lanki, T.; Ljungman, P.; Pitsavos, C.; Ruckerl, R.; Sunyer, J.; Peters, A. Determinants of plasma interleukin-6 levels among survivors of myocardial infarction. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 631–638. [Google Scholar] [CrossRef]
- Rezaie-Majd, A.; Maca, T.; Bucek, R.A.; Valent, P.; Müller, M.R.; Husslein, P.; Kashanipour, A.; Minar, E.; Baghestanian, M. Simvastatin reduces expression of cytokines interleukin-6, interleukin-8, and monocyte chemoattractant protein-1 in circulating monocytes from hypercholesterolemic patients. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1194–1199. [Google Scholar] [CrossRef]
- Barale, C.; Frascaroli, C.; Senkeev, R.; Cavalot, F.; Russo, I. Simvastatin effects on inflammation and platelet activation markers in hypercholesterolemia. Biomed. Res. Int. 2018, 2018, 6508709. [Google Scholar] [CrossRef]
- Xia, W.; Zhang, A.; Jia, Z.; Gu, J.; Chen, H. Klotho contributes to pravastatin effect on suppressing IL-6 production in endothelial cells. Mediat. Inflamm. 2016, 2016, 2193210. [Google Scholar] [CrossRef]
- Loppnow, H.; Zhang, L.; Buerke, M.; Lautenschläger, M.; Chen, L.; Frister, A.; Schlitt, A.; Luther, T.; Song, N.; Hofmann, B.; et al. Statins potently reduce the cytokine-mediated IL-6 release in SMC/MNC cocultures. J. Cell. Mol. Med. 2011, 15, 994–1004. [Google Scholar] [CrossRef]
- Jameel, A.; Ooi, K.G.; Jeffs, N.R.; Galatowicz, G.; Lightman, S.L.; Calder, V.L. Statin modulation of human T-cell proliferation, IL-1β and IL-17 production, and IFN-γ T cell expression: Synergy with conventional immunosuppressive agents. Int. J. Inflamm. 2013, 2013, 434586. [Google Scholar] [CrossRef] [PubMed]
- Schultz, N.E.Ø.; Hasseldam, H.; Rasmussen, R.S.; Vindegaard, N.; McWilliam, O.; Iversen, H.K.; Johansen, F.F. Statin treatment before stroke reduces pro-inflammatory cytokine levels after stroke. Neurol. Res. 2019, 41, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Schieffer, B.; Bünte, C.; Witte, J.; Hoeper, K.; Böger, R.H.; Schwedhelm, E.; Drexler, H. Comparative effects of AT1-antagonism and angiotensin-converting enzyme inhibition on markers of inflammation and platelet aggregation in patients with coronary artery disease. J. Am. Coll. Cardiol. 2004, 44, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Undas, A.; Brummel-Ziedins, K.E.; Potaczek, D.P.; Stobierska-Dzierzek, B.; Bryniarski, L.; Szczeklik, A.; Mann, K.G. Atorvastatin and quinapril inhibit blood coagulation in patients with coronary artery disease following 28 days of therapy. J. Thromb. Haemost. 2006, 4, 2397–2404. [Google Scholar] [CrossRef]
- Walther, C.; Möbius-Winkler, S.; Linke, A.; Bruegel, M.; Thiery, J.; Schuler, G.; Halbrecht, R. Regular exercise training compared with percutaneous intervention leads to a reduction of inflammatory markers and cardiovascular events in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 107–112. [Google Scholar] [CrossRef]
- Gerin, F.; Durmuş, E.; Yaman, A.; Sünbül, M.; Mammadov, C.; Bozbay, M.; Sarı, I.; Kıvrak, T. Relation of interleukin-6 level with coronary artery disease severity in patients undergoing coronary angiography. Eur. J. Ther. 2017, 23, 117–121. [Google Scholar] [CrossRef]
- Habib, S.S.; Al Masri, A.A. Relationship of high sensitivity C-reactive proteinwith presence and severity of coronary artery disease. Pak. J. Med. Sci. 2013, 29, 1425–1429. [Google Scholar] [CrossRef]
- Tajfard, M.; Tavakoly Sany, S.B.; Avan, A.; Latiff, L.A.; Rahimi, H.R.; Moohebati, M.; Hasanzadeh, M.; Ghazizadeh, H.; Esmaeily, H.; Doosti, H.; et al. Relationship between serum high sensitivity C-reactive protein with angiographic severity of coronary arterydisease and traditional cardiovascular risk factors. J. Cell. Physiol. 2019, 234, 10289–10299. [Google Scholar] [CrossRef]
- Eltoft, A.; Arntzen, K.A.; Wilsgaard, T.; Mathiesen, E.B.; Johnsen, S.H. Interleukin-6 is an independent predictor of progressive atherosclerosis in the carotid artery: The Tromsø Study. Atherosclerosis 2018, 271, 1–8. [Google Scholar] [CrossRef]
- Puz, P.; Lasek-Bal, A. Repeated measurements of serum concentrations of TNF-alpha, interleukin-6 and interleukin-10 in the evaluation of internal carotid artery stenosis progression. Atherosclerosis 2017, 263, 97–103. [Google Scholar] [CrossRef]
- Thakore, A.H.; Guo, C.Y.; Larson, M.G.; Corey, D.; Wang, T.J.; Vasan, R.S.; D’Agostino, R.B.; Lipinska, I.; Keaney, J.F., Jr.; Benjamin, E.J.; et al. Association of multiple inflammatory markers with carotid intimal medial thickness and stenosis (from the Framingham Heart Study). Am. J. Cardiol. 2007, 99, 1598–1602. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Caviezel, S.; Teynor, A.; Erbel, R.; Mahabadi, A.A.; Schmidt-Trucksass, A. Carotid intima-media thickness as a biomarker of subclinical atherosclerosis. Swiss Med. Wkly. 2012, 142, w13705. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.Y.; Allison, M.A.; Kim, D.J.; Song, C.H.; Barrett-Connor, E. Association of interleukin-6 and C-reactive protein with subclinical carotid atherosclerosis (the Rancho Bernardo Study). Am. J. Cardiol. 2007, 99, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Q.; Li, J.; Chen, J.Y.; Zhou, Y.L.; Cai, A.P.; Huang, C.; Feng, Y.Q. The association of circulating MiR-29b and interleukin-6 with subclinical atherosclerosis. Cell. Physiol. Biochem. 2017, 44, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, I.M.; de Maat, M.P.; Bots, M.L.; Breteler, M.M.; Meijer, J.; Kiliaan, A.J.; Hofman, A.; Witteman, J.C. Inflammatory mediators and cell adhesion molecules as indicators of severity of atherosclerosis: The Rotterdam Study. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.M.; Beilby, J.P.; McQuillan, B.M.; Thompson, P.L.; Hung, J. Monocyte count, but not C-reactive protein or interleukin-6, is an independent risk marker for subclinical carotid atherosclerosis. Stroke 2004, 35, 1619–1624. [Google Scholar] [CrossRef]
- Okazaki, S.; Sakaguchi, M.; Miwa, K.; Furukado, S.; Yamagami, H.; Yagita, Y.; Mochizuki, H.; Kitagawa, K. Association of interleukin-6 with the progression of carotid atherosclerosis: A 9-year follow-up study. Stroke 2014, 45, 2924–2929. [Google Scholar] [CrossRef]
- Kablak-Ziembicka, A.; Tracz, W.; Przewlocki, T.; Pieniazek, P.; Sokolowski, A.; Konieczynska, M. Association of increased carotid intima-media thickness with the extent of coronary artery disease. Heart 2004, 90, 1286–1290. [Google Scholar] [CrossRef]
- Mahjoob, M.P.; Sadeghi, S.; Khanaman, H.F.; Naderian, M.; Khaheshi, I. Comparison of coronary risk factors and angiographic findings in younger and older patients with significant coronary artery disease. Rom. J. Intern. Med. 2018, 56, 90–95. [Google Scholar] [CrossRef]
- Li, W.; Jin, D.; Takai, S.; Hayakawa, T.; Ogata, J.; Yamanishi, K.; Yamanishi, H.; Okamura, H. Impaired function of aorta and perivascular adipose tissue in IL-18-deficient mice. Am. J. Physiol. Heart Circ. Physiol. 2019. [Google Scholar] [CrossRef]
- Shah, N.; Kelly, A.M.; Cox, N.; Wong, C.; Soon, K. Myocardial infarction in the “Young”: Risk factors, presentation, management and prognosis. Heart Lung Circ. 2016, 25, 955–960. [Google Scholar] [CrossRef] [PubMed]
- Yan, A.T.; Yan, R.T.; Cushman, M.; Redheuil, A.; Tracy, R.P.; Arnett, D.K.; Rosen, B.D.; McClelland, R.L.; Bluemke, D.A.; Lima, J.A. Relationship of interleukin-6 with regional and global left-ventricular function in asymptomatic individuals without clinical cardiovascular disease: Insights from the Multi-Ethnic Study of Atherosclerosis. Eur. Heart J. 2010, 31, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.; Dominic, E.A.; Fink, J.C.; Ojo, A.O.; Barrows, I.R.; Reilly, M.P.; Townsend, R.R.; Joffe, M.M.; Rosas, S.E.; Wolman, M.; et al. Association between inflammation and cardiac geometry in chronic kidney disease: Findings from the CRIC Study. PLoS ONE 2015, 10, e0124772. [Google Scholar] [CrossRef] [PubMed]
- Fontes, J.A.; Rose, N.R.; Čiháková, D. The varying faces of IL-6: From cardiacprotection to cardiac failure. Cytokine 2015, 74, 62–68. [Google Scholar] [CrossRef]
- Sydykov, A.; Mamazhakypov, A.; Petrovic, A.; Kosanovic, D.; Sarybaev, A.S.; Weissmann, N.; Ghofrani, H.A.; Schermuly, R.T. Inflammatory mediators drive adverse right ventricular remodeling and dysfunction and serve as potential biomarkers. Front. Physiol. 2018, 9, 609. [Google Scholar] [CrossRef]
- Prins, K.W.; Archer, S.L.; Pritzker, M.; Rose, L.; Sharma, A.; Thenappan, T. Interleukin-6 is independently associated with right ventricular function in pulmonary arterial hypertension. J. Heart Lung Transplant. 2018, 37, 376–384. [Google Scholar] [CrossRef]
- Harhay, M.O.; Tracy, R.P.; Bagiella, E.; Barr, R.G.; Pinder, D.; Hundley, W.G.; Bluemke, D.A.; Kronmal, R.A.; Lima, J.A.; Kawut, S.M. Relationship of CRP, IL-6, and fibrinogen with right ventricular structure and function: The MESA-Right Ventricle Study. Int. J. Cardiol. 2013, 168, 3818–3824. [Google Scholar] [CrossRef]
- Mozos, I.; Malainer, C.; Horbańczuk, J.; Gug, C.; Stoian, D.; Luca, C.T.; Atanasov, A.G. Inflammatory markers for arterial stiffness in cardiovascular diseases. Front. Immunol. 2017, 8, 1058. [Google Scholar] [CrossRef]
- Mozos, I.; Stoian, D.; Caraba, A.; Malainer, C.; Horbańczuk, J.O.; Atanasov, A.G. Lycopene and vascular health. Front. Pharmacol. 2018, 9, 521. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Gender (% males) | 75% |
| Age of patients (years) | 49.9 ± 5.91 |
| Waist (cm) | 98.3 ± 12.5 |
| Hip (cm) | 103 ± 9 |
| WHR | 0.96 ± 0.09 |
| BMI (kg/m2) | 28.1 ± 4.0 |
| Systolic BP (mmHg) | 127 ± 14.0 |
| Diastolic BP (mmHg) | 77.0 ± 9.0 |
| MAP (mmHg) | 93.8 ± 9.4 |
| History of hypertension | 66% |
| Age at diagnosis of hypertension (years) | 42.6 ± 8.6 |
| Past MI | 70% |
| Age of the first MI (years) | 44.0 ± 5.6 |
| Time since diagnosis of MI to joining the program (years) | 3.20 ± 0.74 |
| Current smoking | 15% |
| Past smoking | 89% |
| Years smoking | 18.9 ± 9.8 |
| Past PTCA | 71% |
| Past CABG | 37% |
| ACEI | 80% |
| ARB | 17% |
| Beta-blockers | 88% |
| Diuretics | 31% |
| Calcium channel blockers | 18% |
| Statins | 96% |
| Parameter | Study Group (Mean ± SD) | Control Group (Mean ± SD) | p-Value |
|---|---|---|---|
| IL-6 (pg/mL) | 1.69 ± 2.77 | 1.47 ± 0.33 | 0.194419 |
| WBC (G/L) | 6.80 ± 0.22 | 5.50 ± 0.16 | 0.000660 |
| RBC (T/L) | 4.96 ± 0.04 | 4.64 ± 0.06 | 0.000205 * |
| Hemoglobin (g/dL) | 15.0 ± 0.12 | 13.7 ± 0.15 | 0.000001 * |
| Hematocrit (%) | 43.9 ± 0.33 | 41.4 ± 0.43 | 0.000011 * |
| MCV (fL) | 89.5 ± 0.45 | 90.0 ± 0.72 | 0.964125 |
| MCH (pg/erythrocyte) | 30.1 ± 0.18 | 30.0 ± 0.27 | 0.314198 |
| MCHC (g/dL) | 33.7 ± 0.09 | 33.3 ± 0.13 | 0.008262 |
| Platelets (G/L) | 216 ± 4.58 | 223 ± 11.2 | 0.599570 |
| Neutrophils (%WBC) | 54.5 ± 0.92 | 54.4 ± 1.48 | 0.476875 |
| Lymphocytes (%WBC) | 33.3 ± 0.82 | 34.1 ± 1.43 | 0.616375 |
| Monocytes (%WBC) | 9.10 ± 0.20 | 8.50 ± 0.27 | 0.078655 |
| Eosinophils (%WBC) | 2.10 ± 0.19 | 2.90 ± 0.43 | 0.021493 |
| Basophils (%WBC) | 0.30 ± 0.02 | 0.50 ± 0.04 | 0.001138 |
| RDW | 13.3 ± 0.11 | 13.5 ± 0.13 | 0.205517 |
| PDW | 13.1 ± 0.23 | 12.4 ± 0.31 | 0.001486 |
| MPV | 10.6 ± 0.09 | 10.3 ± 0.14 | 0.006729 |
| PCT | 0.23 ± 0.01 | 0.22 ± 0.01 | 0.616375 |
| PLCR | 30.5 ± 0.62 | 27.6 ± 1.00 | 0.003356 |
| hsCRP (mg/L) | 1.20 ± 0.27 | 2.10 ± 0.26 | 0.002557 |
| Glucose (mg/dL) | 101 ± 2.49 | 96.0 ± 4.07 | 0.121613 |
| Total cholesterol (mg/dL) | 163 ± 4.06 | 217 ± 6.36 | 0.000002 * |
| HDL (mg/dL) | 47.0 ± 1.16 | 66.0 ± 2.15 | 0.000001 * |
| LDL (mg/dL) | 93.0 ± 3.64 | 126 ± 5.74 | 0.000680 |
| TG (mg/dL) | 128 ± 5.74 | 110 ± 8.52 | 0.051383 |
| LPa (mg/dL) | 20.3 ± 4.96 | 23.2 ± 9.83 | 0.532188 |
| ApoA1 (mg/dL) | 146 ± 3.85 | 177 ± 5.16 | 0.000012 * |
| ApoB (mg/dL) | 74.0 ± 2.25 | 92.0 ± 3.78 | 0.003908 |
| ApoB/ApoA1 | 0.52 ± 0.02 | 0.51 ± 0.03 | 0.965446 |
| Parameter | Correlations for CAD Patients (n = 100) | Correlations for Males (n = 75) | Correlations for Females (n = 25) | Correlations for Patients Post-MI (n = 70) | Correlations for Patients without MI (n = 30) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Rs | p-value | Rs | p-value | Rs | p-value | Rs | p-value | Rs | p-value | |
| Time since the onset of MI | 0.09 | 0.48 | −0.08 | 0.58 | 0.61 | 0.021 | 0.09 | 0.48 | - | - |
| WBC | 0.46 | 0.000003 * | 0.53 | 0.000003 * | 0.27 | 0.19 | 0.46 | 0.0001 | 0.46 | 0.009 |
| MCHC | −0.32 | 0.001 | −0.33 | 0.005 | −0.12 | 0.58 | −0.27 | 0.031 | −0.47 | 0.007 |
| hsCRP | 0.52 | 0.000001 * | 0.55 | 0.000001 * | 0.40 | 0.062 | 0.47 | 0.0002 | 0.62 | 0.0002 |
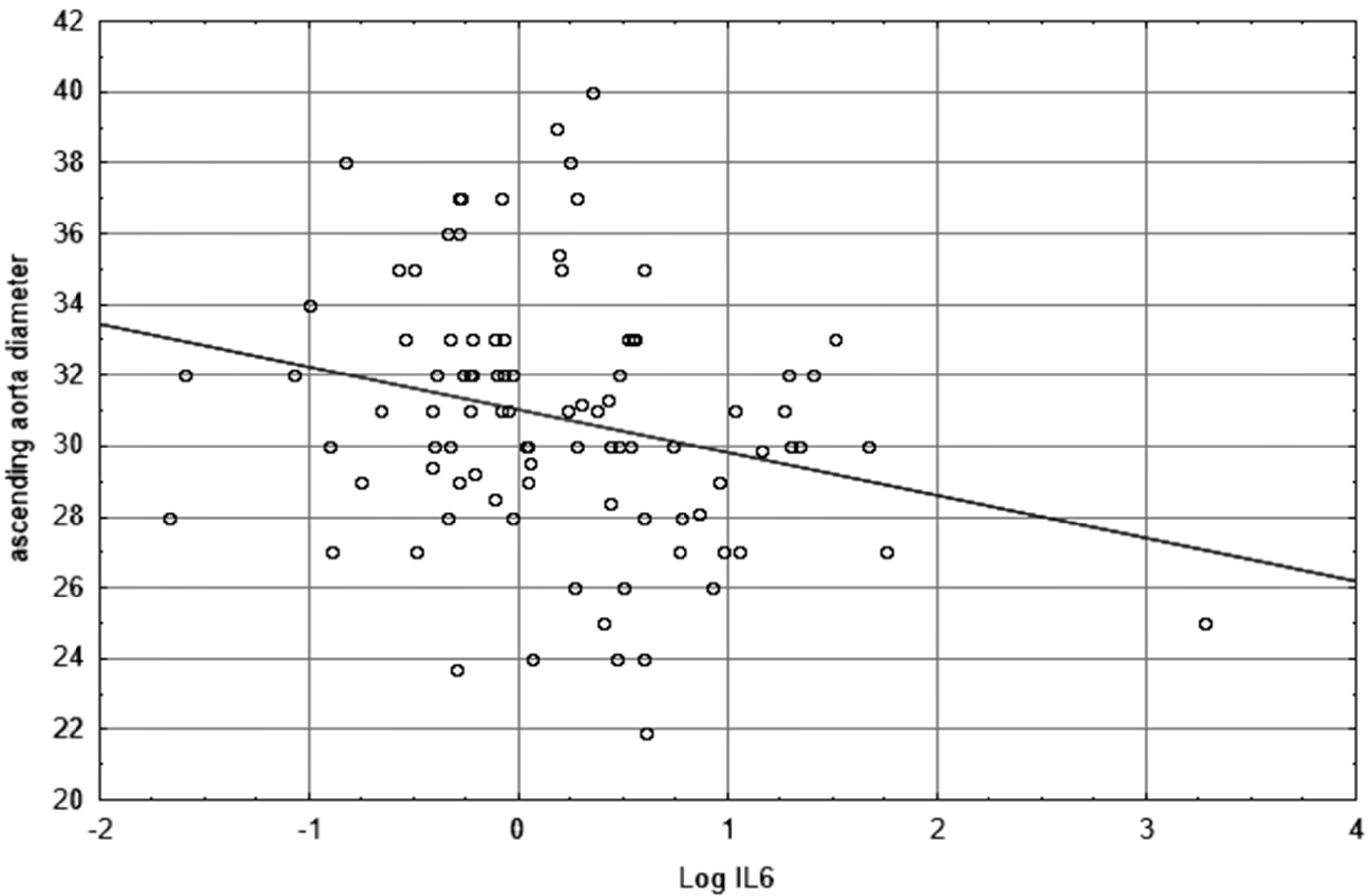
| Ascending aorta diameter | −0.26 | 0.011 | −0.26 | 0.032 | −0.04 | 0.84 | −0.26 | 0.043 | −0.31 | 0.09 |
| RVEDD | −0.21 | 0.041 | −0.12 | 0.33 | −0.29 | 0.17 | −0.30 | 0.019 | −0.04 | 0.84 |
| LVEF | −0.19 | 0.07 | −0.22 | 0.07 | −0.10 | 0.64 | −0.13 | 0.30 | −0.38 | 0.034 |
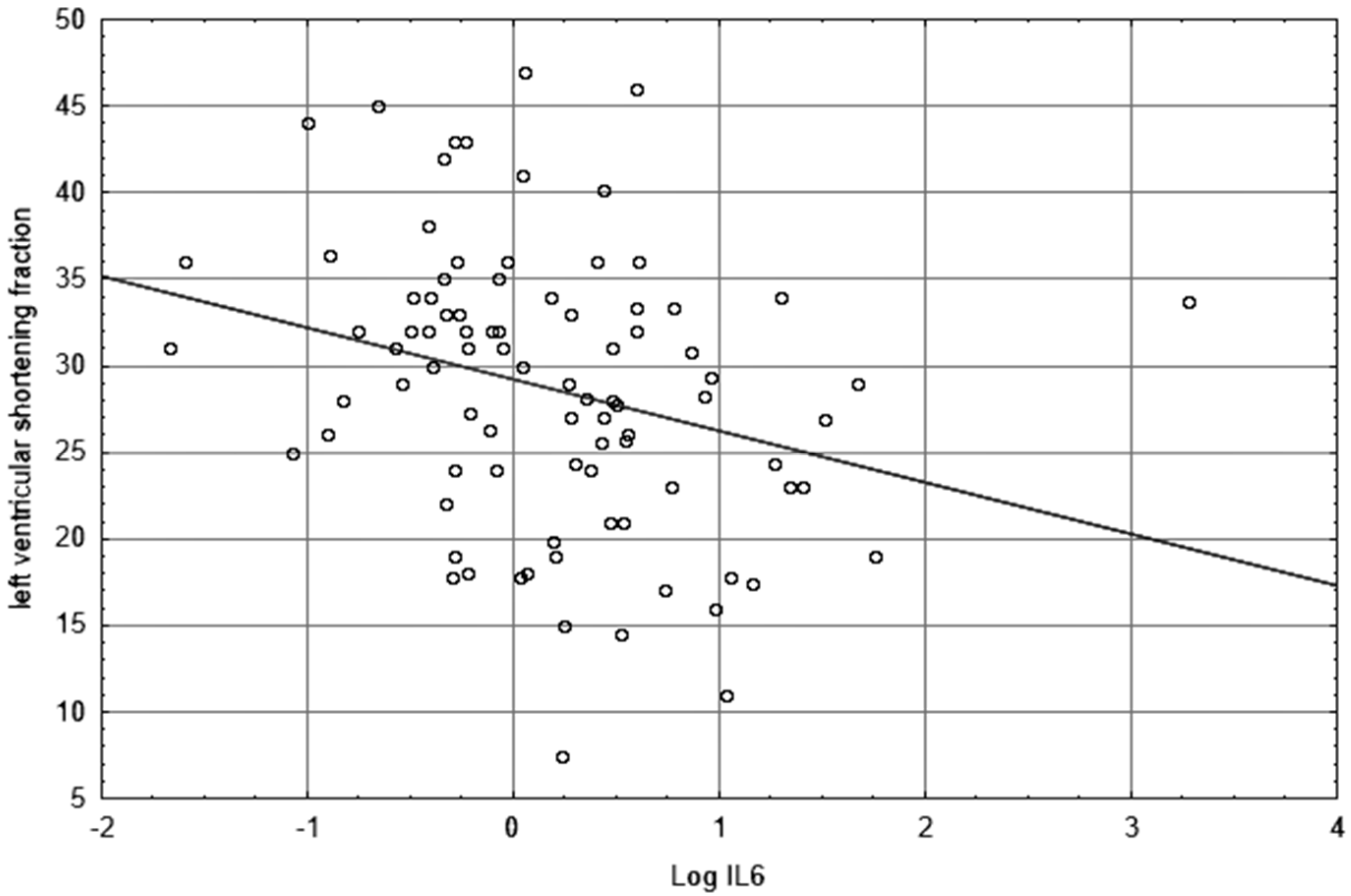
| LVSF | −0.34 | 0.001 | −0.33 | 0.006 | −0.30 | 0.16 | −0.37 | 0.004 | −0.37 | 0.034 |
| IMC lba mean | −0.30 | 0.015 | −0.13 | 0.39 | −0.27 | 0.27 | −0.28 | 0.06 | −0.37 | 0.09 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pauli, N.; Puchałowicz, K.; Kuligowska, A.; Krzystolik, A.; Dziedziejko, V.; Safranow, K.; Rać, M.; Chlubek, D.; Ewa Rać, M. Associations between IL-6 and Echo-Parameters in Patients with Early Onset Coronary Artery Disease. Diagnostics 2019, 9, 189. https://doi.org/10.3390/diagnostics9040189
Pauli N, Puchałowicz K, Kuligowska A, Krzystolik A, Dziedziejko V, Safranow K, Rać M, Chlubek D, Ewa Rać M. Associations between IL-6 and Echo-Parameters in Patients with Early Onset Coronary Artery Disease. Diagnostics. 2019; 9(4):189. https://doi.org/10.3390/diagnostics9040189
Chicago/Turabian StylePauli, Natalia, Kamila Puchałowicz, Agnieszka Kuligowska, Andrzej Krzystolik, Violetta Dziedziejko, Krzysztof Safranow, Michał Rać, Dariusz Chlubek, and Monika Ewa Rać. 2019. "Associations between IL-6 and Echo-Parameters in Patients with Early Onset Coronary Artery Disease" Diagnostics 9, no. 4: 189. https://doi.org/10.3390/diagnostics9040189
APA StylePauli, N., Puchałowicz, K., Kuligowska, A., Krzystolik, A., Dziedziejko, V., Safranow, K., Rać, M., Chlubek, D., & Ewa Rać, M. (2019). Associations between IL-6 and Echo-Parameters in Patients with Early Onset Coronary Artery Disease. Diagnostics, 9(4), 189. https://doi.org/10.3390/diagnostics9040189