
A Review of the Use of Data Analytics to Address Preeclampsia in Ecuador Between 2020 and 2024

 , , , , and
, , , , and
Abstract
1. Introduction
2. Related Work
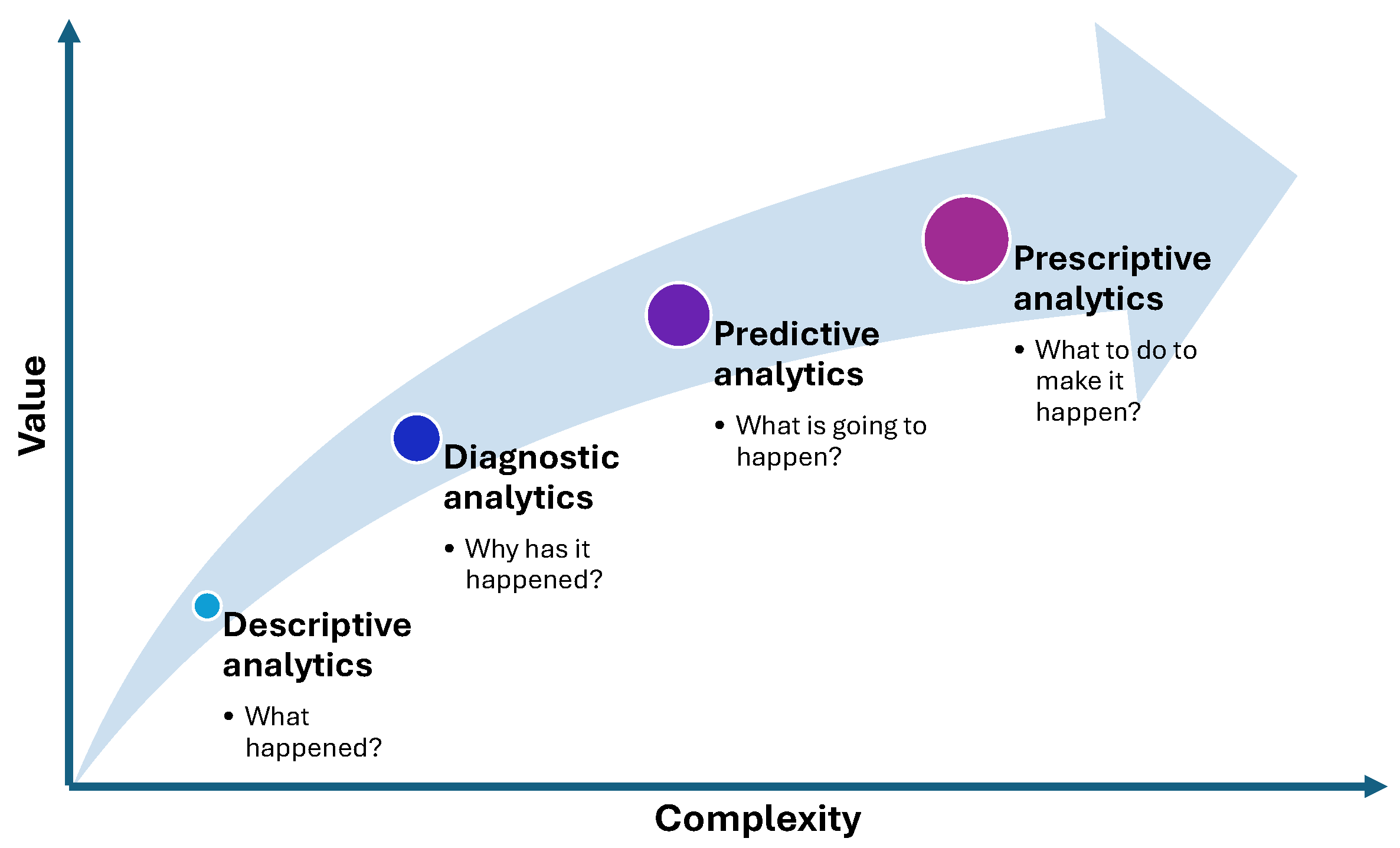
2.1. Data Analytics Approaches
2.2. Related Literature Reviews
- Adolescent pregnancies in Ecuador are associated with a high prevalence of complications, including hypertensive disorders, anemia, and low birth weight.
- Expectant care for severe preeclampsia remote from term may result in better neonatal outcomes, such as higher birth weight and lower rates of neonatal death and intensive care unit (ICU) admission.
- The prevalence of preeclampsia in Latin America and the Caribbean is estimated at 6.6%, with substantial heterogeneity across studies and regions.
- A higher frequency of preeclampsia and gestational hypertension is observed at higher altitudes, with complications such as lower birth weight, HELLP syndrome, and ICU hospitalization.
- Aspirin and calcium/vitamin D supplements are effective preventive measures for preeclampsia.
- Magnesium sulfate remains the most effective treatment for managing preeclampsia in Ecuador.
2.3. Motivation
- From the studies grouped by each analytical approach…
- −
- RQ1: What are the techniques used?
- −
- RQ2: What are the key findings?
- −
- RQ3: What are the public health implications?
- RQ4: Are the findings in line with what the world literature says?
- RQ5: What are the strengths and limitations of each analytical approach?
3. Methodology
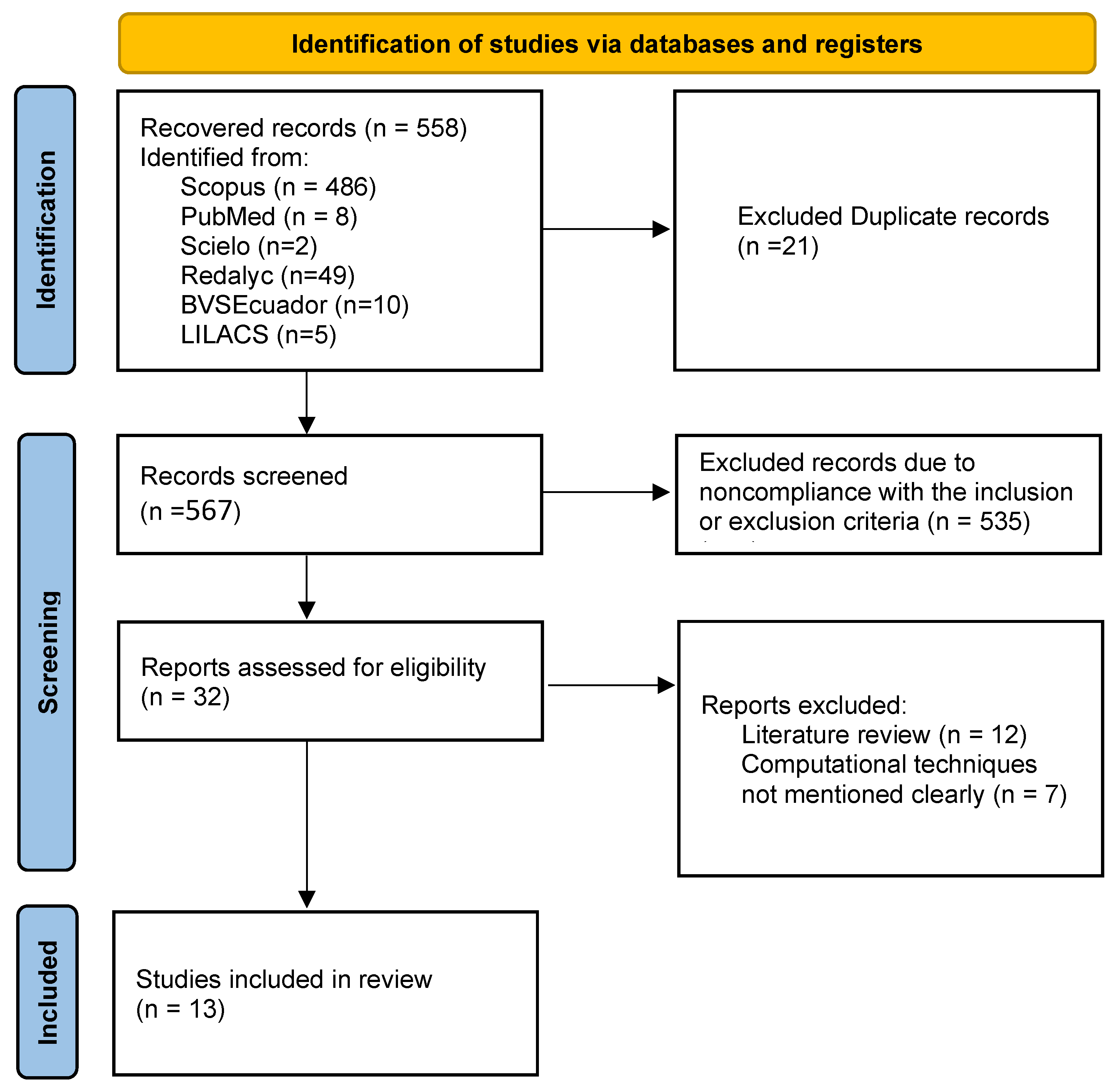
3.1. Databases and Search Strategy
3.2. Inclusion Criteria
- Studies published within the last five years.
- Research conducted in Ecuador in both public and private healthcare institutions.
- Studies involving sample sizes of over 100 patients.
- Articles published in indexed, peer-reviewed scientific journals.
- Papers that report on the use of descriptive, diagnostic, predictive, or prescriptive analytics in the context of preeclampsia.
3.3. Exclusion Criteria
- Studies with insufficient methodological detail for evaluation.
- Review articles or articles that do not directly address research on a hospital population.
- Research exclusive to unintended datasets (e.g., simulated data or case reports with sample sizes fewer than 100 patients).
- Articles not written in English or Spanish.
3.4. Data Extraction and Synthesis
4. Findings
4.1. Descriptive Analytics
4.1.1. Selected Descriptive Studies
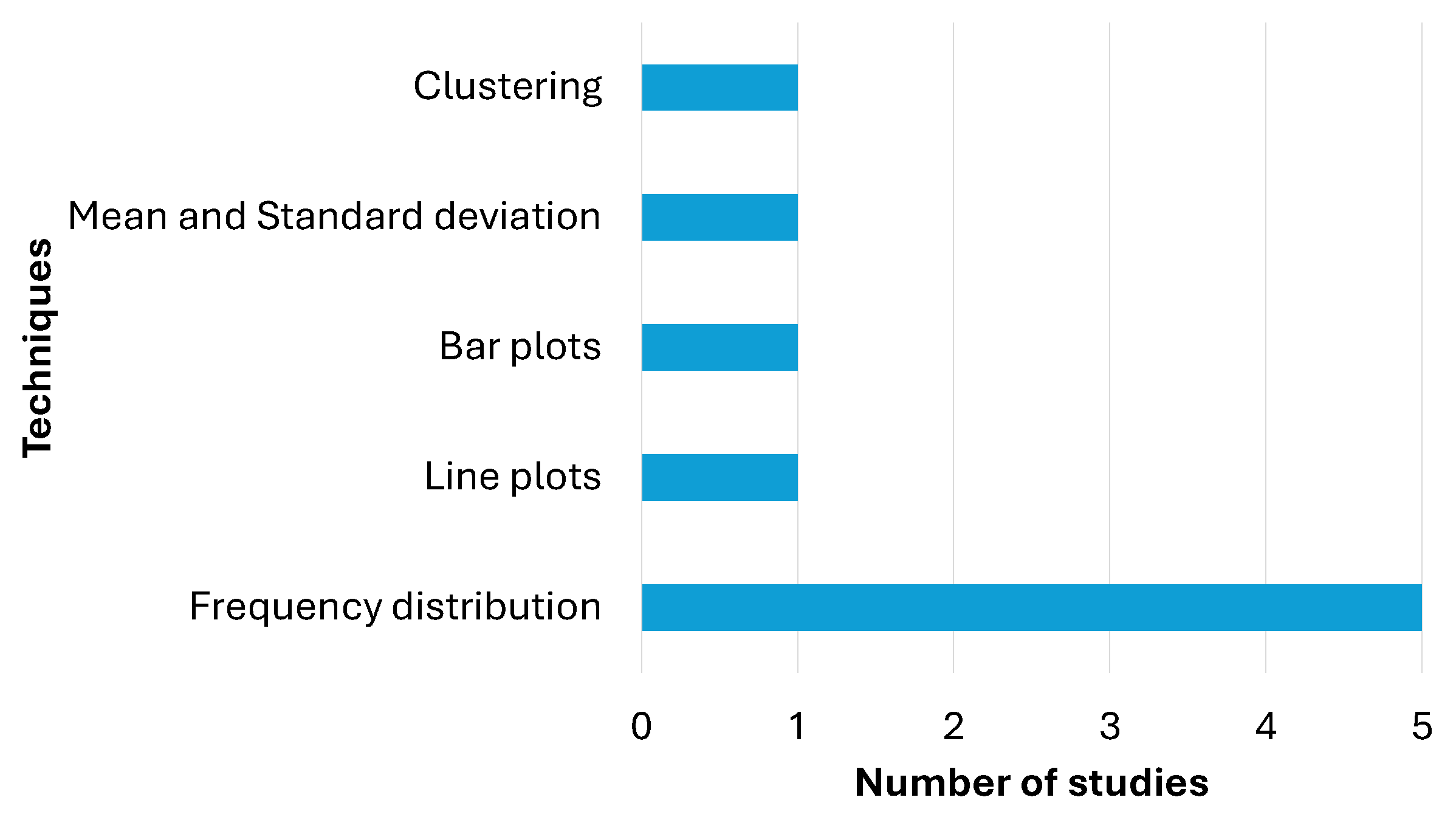
4.1.2. Techniques (RQ1)
4.1.3. Key Findings (RQ2)
- Incidence and Severity:
- Complications:
- Geographical and Ethnic Variations:
- −
- Preeclampsia is more prevalent in certain ethnic groups, such as Montubios and Afro-Ecuadorians, particularly at higher altitudes [4].
- −
4.1.4. Public Health Implications (RQ3)
4.1.5. Conclusion
4.2. Diagnostic Analytics
4.2.1. Selected Diagnostic Studies
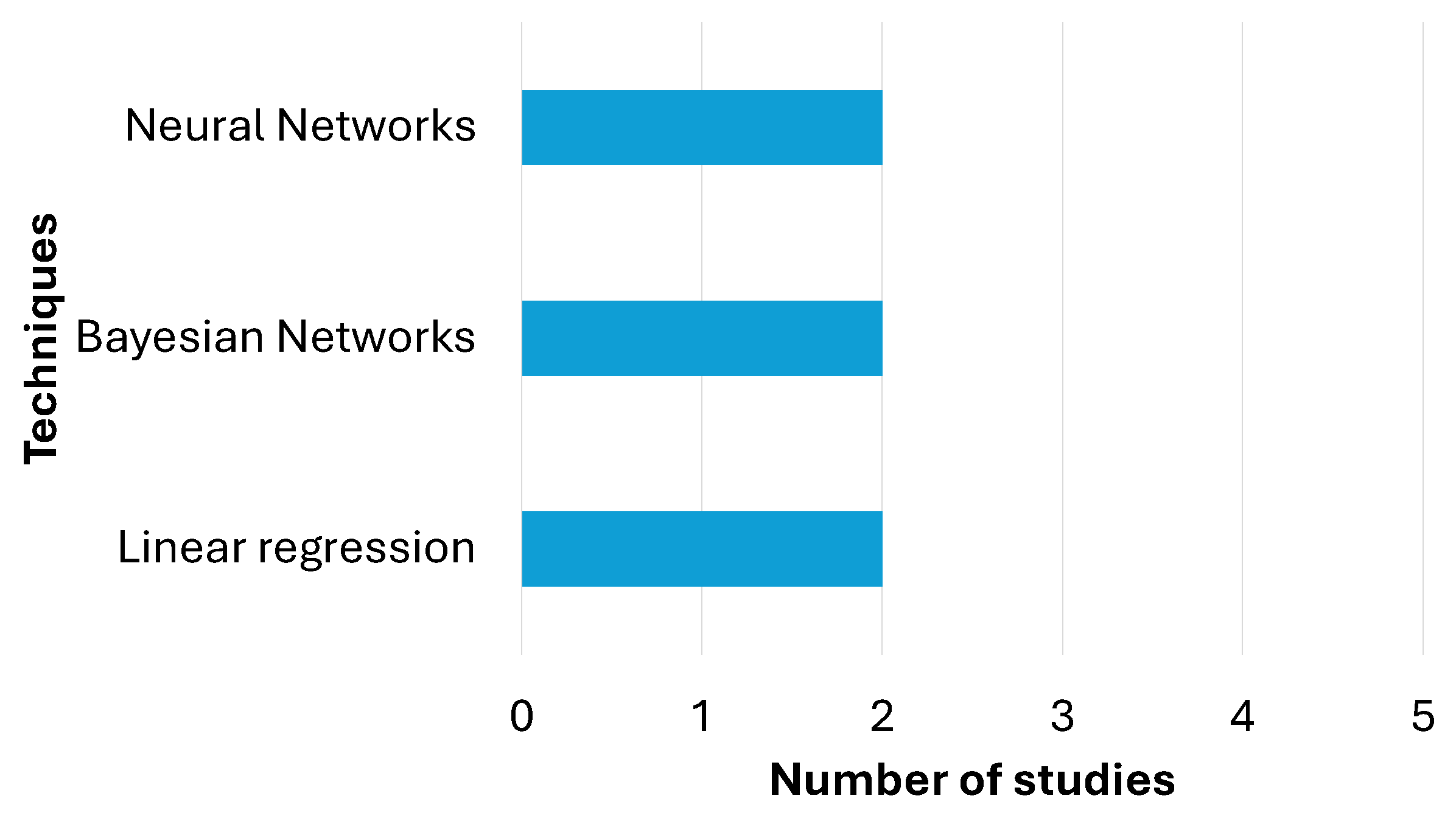
4.2.2. Techniques (RQ1)
4.2.3. Key Findings (RQ2)
- Risk Factors:
- −
- Ethnicity and Altitude: Montubio women living at middle or high altitudes have the highest risk of preeclampsia. Afro-Ecuadorians also show an increased risk associated with altitude [4].
- −
- Micronutrient Intake: Iron and folic acid consumption during pregnancy is protective [5].
- −
- −
- Geographical Distance: Women living more than 20 km from healthcare facilities have a higher risk of developing both preeclampsia and eclampsia [4].
- −
- Family History: A family history of preeclampsia increases the risk [45].
- −
- Obesity and Overweight: Higher BMI (≥25) is associated with an increased risk of preeclampsia [45].
- −
- Prenatal care: Adequate prenatal care (more than five visits starting in the first trimester) significantly reduces the risk of preeclampsia [5].
- −
- −
- Seasonal Variation: Preeclampsia cases tend to increase during the rainy (January to April) and summer (August to November) months in Guayaquil, Ecuador [26].
4.2.4. Public Health Implications (RQ3)
- Nutritional Support: Provide micronutrient supplementation (e.g., iron and folic acid) and education on healthy diets during pregnancy [5].
- Adolescent Health Programs: Develop targeted health programs for adolescent girls to reduce early pregnancies and improve access to prenatal care [45].
- Weight Management: Promote healthy weight management and nutrition programs for adolescents and pregnant women to reduce the risk of obesity-related complications [45].
- Reduce Geographical Barriers: Improve access to obstetric care, especially in rural and remote areas, to reduce the risk of preeclampsia and eclampsia [4].
- Community Health Programs: Strengthen community health programs to provide education and support for pregnant women, especially in high-risk areas [4].
- Seasonal Variation: Seasonal awareness campaigns and targeted interventions during high-risk periods can help mitigate the impact. For example, increased monitoring and resource allocation during these months could reduce complications.
4.2.5. Conclusion
4.3. Predictive Analytics
4.3.1. Selected Predictive Studies
4.3.2. Techniques (RQ1)
4.4. Key Findings (RQ2)
- Homocysteine as a Predictor: Homocysteine levels were not found to be a reliable predictor of preeclampsia in the first study, possibly due to widespread folic acid supplementation [48].
- Predictive Algorithms: The predictive algorithm from the Hospital Clinic of Barcelona demonstrated high accuracy in identifying preeclampsia risk, even without angiogenic biomarkers, making it suitable for low-resource settings [46].
- Machine Learning Models: Bayesian network classifiers, particularly the TANcl algorithm, showed high accuracy in predicting preeclampsia risk, with key risk factors including advanced maternal age, hypertension, and lifestyle factors [1].
Public Health Implications (RQ3)
4.5. Prescriptive Analytics
4.5.1. Selected Prescriptive Studies
4.5.2. Techniques (RQ1)
- Mathematical Optimization: Mathematical models are used to find the best possible solution within a set of constraints. For example, in the context of hospital beds, it can be used to determine how many beds to allocate to each department to maximize efficiency and minimize waiting times [26].
- Simulation: Virtual models can be created that mimic the behavior of a real system to test different scenarios and decisions. For example, the temporary closure of a hospital unit for preeclampsia can be simulated and its impact on patient care and referral capacity measured [26].
- Rule-Based Decision Models: Predefined rules (e.g., using fuzzy logic) can be defined to recommend specific actions based on particular conditions. For example, if the number of occupied beds exceeds 90% of capacity, refer patients to other hospitals or activate emergency protocols [49].
4.5.3. Key Findings (RQ2)
- Given the projected increase in preeclampsia hospitalizations, hospitals should allocate more inpatient beds during peak months.
- Early risk identification and intervention could lower the need for hospitalization.
- The study simulated the impact of closing the hospitalization unit in 2024, similar to the COVID-19 scenario. The closure would result in an average of 130.33 monthly referrals, highlighting the need for alternative strategies to manage bed occupancy during crises.
- The study suggests a possible link between preeclampsia incidence and respiratory/infectious diseases, warranting further research.
- The study highlights the importance of big data analytics in healthcare management.
4.5.4. Public Health Implications (RQ3)
- Enhancing Resource Allocation: Decision-makers should use predictive analytics to anticipate demand and optimize hospital capacity.
- Strengthening Non-Hospital Care Services: To reduce hospital burden, outpatient monitoring and community-based management programs should be expanded.
- Developing Emergency Response Plans: Future pandemics or disasters should not completely disrupt preeclampsia care. Policies should ensure that maternity services remain operational even during health emergencies.
- Addressing Potential Risk Factors: Public health campaigns should promote nutritional awareness, prenatal care, and lifestyle changes to mitigate risk factors such as obesity.
- Utilizing Data-Driven Decision Making: Integration of machine learning models into hospital management systems can improve patient outcomes and optimize resource use.
4.5.5. Conclusion
5. Discussion
5.1. Comparison with Global Literature on Preeclampsia (RQ4)
5.2. Evaluating the Strengths and Limitations of Each Analytics Approach (RQ5)
6. Conclusions
7. Implications for Future Research and Clinical Practice
- Enhanced Data Collection: Establishing standardized EMR systems across all institutions can mitigate data variability and improve the reliability of descriptive and predictive analytics. Past studies, such as those by [1,4,76], have highlighted the challenges of incomplete clinical records and regional variations in data collection. Based on these findings, future research should focus on creating unified data collection protocols that ensure consistency in urban and rural healthcare facilities.
- Advanced Model Validation: Future studies should incorporate rigorous external validation frameworks to ensure that predictive models are generalizable between different populations and regions. For example, in [46], the high accuracy of predictive models in urban settings is demonstrated, but their applicability in rural areas remains untested. Drawing from global studies, such as [72], which emphasize the importance of external validation, future research should aim to validate models in diverse Ecuadorian populations, including high-altitude and indigenous communities.
- Integrative Analytics Approaches: Combining descriptive, diagnostic, and predictive models can lead to more robust prescriptive analytics that inform practical treatment protocols. Past studies, such as [26], have shown the potential of integrating multiple analytics approaches to optimize hospital resource management. Future research should build on these findings by developing integrated decision support systems that leverage real-time data to provide actionable recommendations for clinicians.
- Technological Investments: Policy-makers and healthcare administrators must invest in modern diagnostic and computational infrastructure, particularly in under-resourced highland regions, to fully leverage the benefits of advanced analytics. Studies like [74] have documented the challenges of transitioning from paper-based to digital records in low-resource settings. Future research should explore cost-effective technological solutions that can be implemented in rural areas, ensuring that all regions of Ecuador benefit from advancements in data analytics.
- Community-Based Interventions: Past research, such as [44], has emphasized the importance of community health programs in reducing the burden of preeclampsia, particularly in underserved areas. Future studies should focus on developing and evaluating community-based interventions that combine education, nutritional support, and early screening to reduce the incidence of preeclampsia in high-risk populations.
- Longitudinal Studies: Although cross-sectional studies have provided valuable information on the risk factors and prevalence of preeclampsia, longitudinal studies are needed to understand the long-term impacts of the condition on maternal and child health. For example, the authors of [53] conducted a retrospective cohort study that highlighted the long-term effects of gestational hypertension on offspring. Similar studies in Ecuador could provide critical insight into the lifelong consequences of preeclampsia and inform targeted interventions.
Author Contributions
Funding
Conflicts of Interest
References
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Rodríguez-Larraburu, E.; Barzola-Monteses, J. ACME: A Classification Model for Explaining the Risk of Preeclampsia Based on Bayesian Network Classifiers and a Non-Redundant Feature Selection Approach. Informatics 2024, 11, 31. [Google Scholar] [CrossRef]
- Parrales-Bravo, F.; Saltos-Cedeño, J.; Tomalá-Esparza, J.; Barzola-Monteses, J. Clustering-based Approach for Characterization of Patients with Preeclampsia using a Non-Redundant Feature Selection. In Proceedings of the 2023 3rd International Conference on Electrical, Computer, Communications and Mechatronics Engineering (ICECCME), Tenerife, Canary Islands, Spain, 19–21 July 2023; pp. 1–6. [Google Scholar]
- Ministerio de Salud Pública del Ecuador. Gaceta de Muerte Materna SE14. 2020. Available online: https://bit.ly/3Poz79o (accessed on 11 September 2024).
- Tejera, E.; Sánchez, M.E.; Henríquez-Trujillo, A.R.; Pérez-Castillo, Y.; Coral-Almeida, M. A population-based study of preeclampsia and eclampsia in Ecuador: Ethnic, geographical and altitudes differences. BMC Pregnancy Childbirth 2021, 21, 116. [Google Scholar] [CrossRef]
- Tite-Tibanquiza, K.; Guzman-Chávez, I.; Dutan-Yupangui, L.; del Cisne Quito-Cabrera, M.; León-Santillán, E. Association between Prenatal Control and the Incidence of Preeclampsia in Ecuadorian Pregnant Women: A Cross-Sectional Study. J. Med. Health Stud. 2024, 5, 1–10. [Google Scholar] [CrossRef]
- Parrales Bravo, F.; Del Barrio García, A.A.; Gallego de la Sacristana, M.; López Manzanares, L.; Vivancos, J.; Ayala Rodrigo, J.L. Support system to improve reading activity in parkinson’s disease and essential tremor patients. Sensors 2017, 17, 1006. [Google Scholar] [CrossRef] [PubMed]
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Barzola-Monteses, J.; Guillén-Mirabá, J.; Guzmán-Bedor, O. Csm: A chatbot solution to manage student questions about payments and enrollment in university. IEEE Access 2024, 12, 74669–74680. [Google Scholar] [CrossRef]
- Barzola-Monteses, J.; Yanez-Pazmino, W.; Flores-Moran, E.; Parrales-Bravo, F. Comparisons of deep learning models to predict energy consumption of an educational building. In Proceedings of the 2022 IEEE International Conference on Machine Learning and Applied Network Technologies (ICMLANT), Soyapango, El Salvador, 15–16 December 2022; pp. 1–6. [Google Scholar]
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Barzola-Monteses, J.; Guillén-Mirabá, J.; Guzman-Bedor, O. Virtual Assistant Prototype to Answer Student Payment and Enrollment Questions Through Natural Language Processing and Machine Learning. In Proceedings of the 2024 IEEE International Conference on Advanced Systems and Emergent Technologies (IC_ASET), Hammamet, Tunisia, 27–29 April 2024; pp. 1–6. [Google Scholar]
- Dueñas-Espín, I.; Armijos-Acurio, L.; Espín, E.; Espinosa-Herrera, F.; Jimbo, R.; León-Cáceres, Á.; Nasre-Nasser, R.; Rivadeneira, M.F.; Rojas-Rueda, D.; Ruiz-Cedeño, L.; et al. Is a higher altitude associated with shorter survival among at-risk neonates? PLoS ONE 2021, 16, e0253413. [Google Scholar] [CrossRef]
- López-Pulles, R.; González-Andrade, F.; Durán-Rodas, M.; Ayala, J.; Carrillo, R.; Buitrón, L.R.; Chuga, J.; Moya, W. Assessment of genetic contributions to risk of preeclampsia in Ecuadorian women. Hypertens. Pregnancy 2010, 29, 410–418. [Google Scholar] [CrossRef]
- López-Jaramillo, P.; Casas, J.; Serrano, N. Preeclampsia: From epidemiological observations to molecular mechanisms. Braz. J. Med. Biol. Res. 2001, 34, 1227–1235. [Google Scholar] [CrossRef]
- Michita, R.T.; Kaminski, V.d.L.; Chies, J.A.B. Genetic variants in preeclampsia: Lessons from studies in Latin-American populations. Front. Physiol. 2018, 9, 1771. [Google Scholar] [CrossRef]
- Astudillo Carrera, A.S.; Cárdenas Vintimilla, M.I. Frecuencia de los Factores de Riesgo en Pacientes Preeclámpticas y no Preeclámpticas y Correlación entre los Valores Hemáticos de Laboratorio y la Gravedad de la Preeclampsia en Pacientes Hospitalizados en el Servicio de Obstetricia del Hospital Vicente Corral Moscoso, Cuenca-Ecuador, Octubre 2004–Marzo 2005. 2006. Available online: http://dspace.ucuenca.edu.ec/handle/123456789/22617 (accessed on 15 March 2025).
- Allauca Cali, A.; Bermúdez, V.; Rojas, J. Complicaciones obstetricas y perinatales en embarazadas con diabetes gestacional, pre-eclampsia severa o ambas, en el Hospital Enrique C. Sotomayor, Guayaquil-Ecuador. Diabetes Int. 2014, 6, 1–9. [Google Scholar]
- Kienast, C.; Moya, W.; Rodriguez, O.; Jijón, A.; Geipel, A. Predictive value of angiogenic factors, clinical risk factors and uterine artery Doppler for pre-eclampsia and fetal growth restriction in second and third trimester pregnancies in an Ecuadorian population. J. Matern.-Fetal Neonatal Med. 2016, 29, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Klinger, L.M.G.; Gómez, D.R.T.; Placencia, X.M.P.; Diaz, C.I.E.; Borja, J.E.N.; Zambrano, A.d.l.Á.M.; Cobeña, K.A.F.; Wong, M.E.F.; Vivas, M.P.C.; Asqui, A.P.C.; et al. Características clínicas y complicaciones asociadas a preeclampsia y eclampsia en pacientes del Hospital General del Norte de Guayaquil IESS Los Ceibos. Rev. Latinoam. Hipertens. 2019, 14, 201–204. [Google Scholar]
- Phoa, K.; Chedraui, P.; Pérez-López, F.; Wendte, J.; Ghiabi, S.; Vrijkotte, T.; Pinto, P. Perinatal outcome in singleton pregnancies complicated with preeclampsia and eclampsia in Ecuador. J. Obstet. Gynaecol. 2016, 36, 581–584. [Google Scholar] [CrossRef] [PubMed]
- Parra-Pingel, P.E.; Quisiguiña-Avellán, L.A.; Hidalgo, L.; Chedraui, P.; Pérez-López, F.R. Pregnancy outcomes in younger and older adolescent mothers with severe preeclampsia. Adolesc. Heal. Med. Ther. 2017, 8, 81–86. [Google Scholar] [CrossRef]
- De la altura en Ecuador, E. Iron, oxygen and placental development in the etiology of preeclampsia. Effects of high altitude in Ecuador. Rev. Méd. Chile 2006, 134, 491–498. [Google Scholar]
- Teran, E.; Chedraui, P.; Vivero, S.; Villena, F.; Duchicela, F.; Nacevilla, L. Plasma and placental nitric oxide levels in women with and without pre-eclampsia living at different altitudes. Int. J. Gynecol. Obstet. 2009, 104, 140–142. [Google Scholar] [CrossRef]
- González-Andrade, F.; Michelena, S.; Espinosa, D.E.; Romero, G.A. High Altitude and Congenital Heart Disease in Andean Highlands Populations: The Case of Ecuador. In Congenital Heart Disease: From Diagnosis to Treatment; Nova Science Publishers: Hauppauge, NY, USA, 2019; pp. 107–175. [Google Scholar]
- López-Jaramillo, P.; García, R.; Reyes, L.; Ruiz, S. Appropriate prenatal care system: The best way to prevent preeclampsia in Andean countries. Colomb. Médica 2009, 40, 226–230. [Google Scholar] [CrossRef]
- Yanez, P.; Vásquez, C.J.; Rodas, L.; Durán, A.; Chedraui, P.; Liem, K.H.; Pérez-López, F.R.; Teran, E. Erythrocyte folate content and serum folic acid and homocysteine levels in preeclamptic primigravidae teenagers living at high altitude. Arch. Gynecol. Obstet. 2013, 288, 1011–1015. [Google Scholar] [CrossRef]
- López-Jaramillo, P.; García, R.G.; López, M. Preventing pregnancy-induced hypertension: Are there regional differences for this global problem? J. Hypertens. 2005, 23, 1121–1129. [Google Scholar] [CrossRef]
- Parrales-Bravo, F.; Gómez-Rodríguez, V.; Barzola-Monteses, J.; Caicedo-Quiroz, R.; Tolozano-Benites, E.; Vasquez-Cevallos, L. From Descriptive to Prescriptive Analytics on Time Series: Studying the Number of Preeclampsia Inpatient Beds. IEEE Access 2024, 12, 131576–131590. [Google Scholar] [CrossRef]
- Guo, C.; Chen, J. Big data analytics in healthcare. In Knowledge Technology and Systems: Toward Establishing Knowledge Systems Science; Springer: Berlin/Heidelberg, Germany, 2023; pp. 27–70. [Google Scholar]
- Batko, K.; Ślęzak, A. The use of Big Data Analytics in healthcare. J. Big Data 2022, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Ahmad, M.; Jeon, G.; Piccialli, F. A framework for pandemic prediction using big data analytics. Big Data Res. 2021, 25, 100190. [Google Scholar] [CrossRef]
- Bertsimas, D.; Boussioux, L.; Cory-Wright, R.; Delarue, A.; Digalakis, V.; Jacquillat, A.; Kitane, D.L.; Lukin, G.; Li, M.; Mingardi, L.; et al. From predictions to prescriptions: A data-driven response to COVID-19. Health Care Manag. Sci. 2021, 24, 253–272. [Google Scholar] [CrossRef]
- Balali, F.; Nouri, J.; Nasiri, A.; Zhao, T.; Balali, F.; Nouri, J.; Nasiri, A.; Zhao, T. Data analytics. In Data Intensive Industrial Asset Management: IoT-Based Algorithms and Implementation; Springer: Cham, Switzerland, 2020; pp. 105–113. [Google Scholar]
- Houtmeyers, K.C.; Jaspers, A.; Figueiredo, P. Managing the training process in elite sports: From descriptive to prescriptive data analytics. Int. J. Sport. Physiol. Perform. 2021, 16, 1719–1723. [Google Scholar] [CrossRef]
- Mosavi, N.S.; Santos, M.F. How prescriptive analytics influences decision making in precision medicine. Procedia Comput. Sci. 2020, 177, 528–533. [Google Scholar] [CrossRef]
- Barrera, G.E.F.; López, A.F.Á.; Córdova, F.A.Á.; López, C.I.Q.; Calle, M.E.V. Actualización en el manejo y tratamiento de la preclampsia: Artículo de Revisión. Cienc. Ecuad. 2024, 6, 1–21. [Google Scholar]
- Tite, L.M.T.; Conde, L.G.R. Análisis de las complicaciones materno fetales asociadas a la preeclamsia. Revisión de la literatura. Enferm. Cuid. 2024, 7, 42–52. [Google Scholar]
- Blanco, E.; Marin, M.; Nuñez, L.; Retamal, E.; Ossa, X.; Woolley, K.E.; Oludotun, T.; Bartington, S.E.; Delgado-Saborit, J.M.; Harrison, R.M.; et al. Adverse pregnancy and perinatal outcomes in Latin America and the Caribbean: Systematic review and meta-analysis. Rev. Panam. Salud Pública 2023, 46, e21. [Google Scholar] [CrossRef]
- Roman-Lazarte, V.; Roman, L.A.; Moncada-Mapelli, E.; Uribe-Cavero, L.J.; Marcelo-Armas, M.L. Clinical manifestations and complications of preeclampsia and eclampsia in populations residing at high altitudes and very high altitudes: A scoping review. Pregnancy Hypertens. 2024, 36, 101119. [Google Scholar] [CrossRef]
- Ledesma, D.V.B.; Pomasqui, C.A.P.; Saltos, Á.J.A. Literature review on prevention to reduce obstetric and perinatal challenges in adolescent pregnancies. Salud Cienc. Tecnol.-Ser. Conf. 2023, 2, 745. [Google Scholar]
- Quintero-Ortíz, M.A.; Grillo-Ardila, C.F.; Amaya-Guio, J. Expectant Versus Interventionist Care in the Management of Severe Preeclampsia Remote from Term: A Systematic Review. Rev. Bras. Ginecol. E Obstet./RBGO Gynecol. Obstet. 2021, 43, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Viteri-Hinojosa, A.S.; Espinosa-Yépez, K.R. Analysis of Morbidity due to Anesthetic Complications in Obstetric Patients in Ecuador (2018 to 2022). Soc. Port. Anestesiol. 2024, 33, 109–114. [Google Scholar]
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Vasquez-Cevallos, L.; Tolozano-Benites, E.; Charco-Aguirre, J.; Barzola-Monteses, J.; Cevallos-Torres, L. Supporting the Characterization of Preeclampsia Patients Through Descriptive and Clustering Analysis. Electronics 2024, 13, 4854. [Google Scholar] [CrossRef]
- Vargas-Vera, R.; Placencia-Ibadango, M.; Vargas-Silva, K. Pre-eclampsia Risk Factors in Patients Treated at Guayaquil University Hospital. Int. J. Obst. Gync. 2021, 1, 27–31. [Google Scholar]
- Hernández, Y.; Plasencia, A.R.; Vizuete, E.V. Risk Factors for Preeclampsia in Pregnant Women: Analysis for Nursing Intervention. Rev. Univ. Soc. 2021, 13, 181–187. [Google Scholar]
- Cho Vásquez, S.G.; Jaigua Rodríguez, M.S. Prevalencia y Factores Asociados de Preeclampsia, Eclampsia e Hipertensión Gestacional en Mujeres Adolescentes en el Periodo 2019–2020 en el Hospital Homero Castanier Crespo, Azogues, 2021. Available online: http://dspace.ucuenca.edu.ec/handle/123456789/37579 (accessed on 13 February 2025).
- Guerrero, K.D.D.; Abadie, P.M.D. Validación externa del modelo predictivo de preeclampsia del Hospital Clinic de Barcelona en una unidad de segundo nivel en Guayaquil, Ecuador. Actas Médicas (Ecuad.) 2024, 34, 120–124. [Google Scholar]
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Barzola-Monteses, J.; Cevallos-Torres, L. Prediction of emergency room arrivals of patients with preeclampsia disease using artificial neural network model. In Proceedings of the 2024 IEEE 4th International Conference on Electronic Communications, Internet of Things and Big Data (ICEIB), Taipei, Taiwan, 19–21 April 2024; pp. 34–39. [Google Scholar]
- Vargas-Vera, R.M.C.; Silva, K.S.V.; Silva, K.S.V. Predicción de pre eclampsia con la determinación de homocisteína sérica.: Un estudio observacional de centro único. Actas Médicas (Ecuad.) 2023, 33, 137–141. [Google Scholar] [CrossRef]
- Stoeck, T.; Mellouli, T. A Two-Dimensional Categorization Scheme for Simulation/Optimization-Based Decision Support in Hospitals Applied to Overall Bed Management in Interdependent Wards Under Flexibility. In Operations Research and Simulation in Healthcare; Springer: Cham, Switzerland, 2021; pp. 1–32. [Google Scholar]
- Phoswa, W.N.; Khaliq, O.P. The role of oxidative stress in hypertensive disorders of pregnancy (preeclampsia, gestational hypertension) and metabolic disorder of pregnancy (gestational diabetes mellitus). Oxidative Med. Cell. Longev. 2021, 2021, 5581570. [Google Scholar] [CrossRef]
- Ayyash, M.K.; McLaren, R.; Shaman, M.; Al-Kouatly, H.B. Trends in Preeclampsia Risk Factors in the US From 2010 to 2021. JAMA 2024, 332, 167–169. [Google Scholar] [CrossRef]
- Jawad, K.S. Incidence and Determinants of Hypertensive Disorders of Pregnancy in the US: Hospitalization Discharge Rate for Preeclampsia, Eclampsia, and Gestational Hypertensions, 2016–2018. Ph.D. Thesis, University of Louisville, Louisville, KY, USA, 2023. [Google Scholar]
- Kuciene, R.; Dulskiene, V. Associations of maternal gestational hypertension with high blood pressure and overweight/obesity in their adolescent offspring: A retrospective cohort study. Sci. Rep. 2022, 12, 3800. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.T.; Kuo, C.F.; Lin, C.P.; Huang, Y.T.; Chen, S.W.; Wu, H.M.; Chu, P.H. Association of family history with incidence and gestational hypertension outcomes of preeclampsia. Int. J. Cardiol. Hypertens. 2021, 9, 100084. [Google Scholar] [CrossRef] [PubMed]
- Kassa, B.G.; Asnkew, S.; Ayele, A.D.; Nigussie, A.A.; Demilew, B.C.; Mihirete, G.N. Preeclampsia and its determinants in Ethiopia: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0287038. [Google Scholar] [CrossRef]
- Moore, L.G. Hypoxia and reproductive health: Reproductive challenges at high altitude: Fertility, pregnancy and neonatal well-being. Reproduction 2021, 161, F81–F90. [Google Scholar] [CrossRef]
- Gonzalez-Candia, A.; Herrera, E.A. High altitude pregnancies and vascular dysfunction: Observations from Latin American studies. Front. Physiol. 2021, 12, 786038. [Google Scholar] [CrossRef]
- Ahrens, S.; Singer, D. Placental Adaptation to Hypoxia: The Case of High-Altitude Pregnancies. Int. J. Environ. Res. Public Health 2025, 22, 214. [Google Scholar] [CrossRef]
- Ngene, N.C.; Moodley, J. Preventing maternal morbidity and mortality from preeclampsia and eclampsia particularly in low-and middle-income countries. Best Pract. Res. Clin. Obstet. Gynaecol. 2024, 94, 102473. [Google Scholar] [CrossRef]
- Roberts, J.M.; Abimbola, S.; Bale, T.L.; Barros, A.; Bhutta, Z.A.; Browne, J.L.; Celi, A.C.; Dube, P.; Graves, C.R.; Hollestelle, M.J.; et al. Global inequities in adverse pregnancy outcomes: What can we do? AJOG Glob. Rep. 2024, 4, 100385. [Google Scholar] [CrossRef]
- Fasanya, H.O.; Hsiao, C.J.; Armstrong-Sylvester, K.R.; Beal, S.G. A critical review on the use of race in understanding racial disparities in preeclampsia. J. Appl. Lab. Med. 2021, 6, 247–256. [Google Scholar] [CrossRef]
- Moungmaithong, S.; Wang, X.; Tai, A.S.; Feng, Q.; Sahota, D.; Leung, T.Y.; Poon, L.C. First trimester screening for preeclampsia: An asian perspective. Matern.-Fetal Med. 2021, 3, 116–123. [Google Scholar] [CrossRef]
- Conklin, M.B.; Wells, B.M.; Doe, E.M.; Strother, A.M.; Tarasiewicz, M.E.B.; Via, E.R.; Conrad, L.B.; Farias-Eisner, R. Understanding Health Disparities in Preeclampsia: A Literature Review. Am. J. Perinatol. 2024, 41, e1291–e1300. [Google Scholar] [CrossRef] [PubMed]
- Flores-Yallico, G.L.; Avila-Sánchez, G.A.; de María Sánchez-Aguirre, F.; Vásquez-Pajuelo, L.; Méndez-Ilizarbe, G.S.; Andrade-Díaz, E.M.; Rodriguez-Barboza, J.R. Addressing Maternal Perinatal Mortality: State Responsibility in Primary Health Care in Perú. Int. J. Relig. 2024, 5, 412–423. [Google Scholar] [CrossRef]
- Soundararajan, R.; Khan, T.; von Dadelszen, P. Pre-eclampsia Challenges and Care in Low and Middle-Income Countries: Understanding Diagnosis, Management, and Health Impacts in Remote and Developing Regions. Best Pract. Res. Clin. Obstet. Gynaecol. 2024, 96, 102525. [Google Scholar] [CrossRef]
- Hahka, T.M.; Slotkowski, R.A.; Akbar, A.; VanOrmer, M.C.; Sembajwe, L.F.; Ssekandi, A.M.; Namaganda, A.; Muwonge, H.; Kasolo, J.N.; Nakimuli, A.; et al. Hypertension Related Co-Morbidities and Complications in Women of Sub-Saharan Africa: A Brief Review. Circ. Res. 2024, 134, 459–473. [Google Scholar] [CrossRef]
- Graves, C.R.; Firoz, T.; Smith, S.N.; Hernandez, N.; Haley, S.; Smith, K.; D’Oria, R.; Celi, A.C. Addressing Racial Disparities in the Hypertensive Disorders in Pregnancy: A Plan for Action from the Preeclampsia Foundation’s Racial Disparities Task Force. J. Racial Ethn. Health Disparities 2024, 1–10. [Google Scholar] [CrossRef]
- Weinger, M.B.; Slagle, J.; Jain, S.; Ordonez, N. Retrospective data collection and analytical techniques for patient safety studies. J. Biomed. Inform. 2003, 36, 106–119. [Google Scholar] [CrossRef]
- Zhou, X.H.; Obuchowski, N.A.; McClish, D.K. Statistical Methods in Diagnostic Medicine; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Wolniak, R.; Grebski, W. The concept of diagnostic analytics. Silesian Univ. Technol. Sci. Pap. Organ. Manag. Ser. 2023, 175, 650–669. [Google Scholar]
- Bandi, M.; Masimukku, A.K.; Vemula, R.; Vallu, S. Predictive Analytics in Healthcare: Enhancing Patient Outcomes through Data-Driven Forecasting and Decision-Making. Int. Numer. J. Mach. Learn. Robot. 2024, 8, 1–20. [Google Scholar]
- Cabitza, F.; Campagner, A.; Soares, F.; de Guadiana-Romualdo, L.G.; Challa, F.; Sulejmani, A.; Seghezzi, M.; Carobene, A. The importance of being external. methodological insights for the external validation of machine learning models in medicine. Comput. Methods Programs Biomed. 2021, 208, 106288. [Google Scholar] [CrossRef]
- Tupsakhare, P. Data Science for Proactive Patient Care: From Descriptive to Prescriptive Analytics. N. Am. J. Eng. Res. 2024, 5, 1610–1617. [Google Scholar] [CrossRef]
- Shrestha, P. Challenges and Impact of Transforming Paper-Based Nursing Documentation into Electronic Form: A Study in Nepal. Master’s Thesis, UiT Norges Arktiske Universitet, Tromsø, Norway, 2016. [Google Scholar]
- Ara, A.; Maraj, M.A.A.; Rahman, M.A.; Bari, M.H. The Impact Of Machine Learning On Prescriptive Analytics For Optimized Business Decision-Making. Int. J. Manag. Inf. Syst. Data Sci. 2024, 1, 7–18. [Google Scholar]
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Tolozano-Benitez, E.; Gómez-Rodríguez, V.; Cevallos-Torres, L.; Charco-Aguirre, J.; Vasquez-Cevallos, L. OUCH: Oversampling and Undersampling Cannot Help Improve Accuracy in Our Bayesian Classifiers That Predict Preeclampsia. Mathematics 2024, 12, 3351. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Countries of Study | Goal | Main Findings | Limitations |
|---|---|---|---|---|---|
| Barrera et al. [34] | 2024 | Ecuador | Analyze new studies on the management and care of pregnant women with preeclampsia to improve prognoses and treatment efficiency. | Magnesium sulfate remains the most effective treatment. Aspirin and calcium/vitamin D supplements are effective preventive measures. Early screening and intervention are recommended. | Limited sample size; reliance on secondary sources; need for further clinical trials to validate findings. |
| Tite et al. [35] | 2024 | Ecuador | Identify maternal–fetal complications associated with preeclampsia. | Women aged 20–34 years are at higher risk. Early detection is essential, especially in low-resource settings. Aspirin and calcium are suggested for high-risk women. | Limited to open-access articles, potential selection bias. Only 10 studies reviewed in the last 5 years. |
| Blanco et al. [36] | 2022 | Argentina, Bolivia, Brazil, Chile, Colombia, Dominican Republic, Ecuador, Guatemala, Guadeloupe, Haiti, Honduras, Mexico, Nicaragua, Panama, Paraguay, Peru, Puerto Rico, Trinidad and Tobago, Uruguay, Venezuela | To estimate the point prevalence of pregnancy-induced hypertension, preeclampsia, gestational diabetes, low birth weight, and preterm delivery in Latin America and the Caribbean, and evaluate the heterogeneity of the estimates. | Incidences: preeclampsia: 6.6%, gestational diabetes: 8.5%, low birth weight: 8.5% preterm birth: 10.0%, substantial heterogeneity observed in prevalence estimates across studies and by study design. | Limited to 20 out of 43 countries in the region, potentially underestimating heterogeneity. Focused on meta-analyses using all available studies regardless of bias level, which may affect the reliability of estimates. Lack of universally accepted diagnostic criteria for gestational diabetes limits cross-regional comparisons. |
| Román-Lazarte [37] | 2024 | Bolivia, Ecuador, Perú, Turquía | To synthesize the evidence on the clinical manifestations and complications of preeclampsia in pregnant women residing at high and very high altitudes. | A higher frequency of preeclampsia and gestational hypertension is observed at higher altitudes. Complications such as lower birth weight, higher frequency of HELLP syndrome and ICU hospitalization are reported. | The review includes studies with low quality of evidence. Specific questions were not asked, which led to mixed results. Databases from some regions such as China were not included, which may have excluded relevant information. |
| Ledesma et al. [38] | 2023 | Ecuador | To examine the presence and recurrence of obstetric and perinatal complications in pregnant adolescents in Ecuador, and propose components of a comprehensive prevention program to reduce maternal and perinatal complications. | High prevalence of complications such as anemia, abortion, hypertensive disorders, postpartum hemorrhages, and low birth weight. Need for comprehensive prevention programs including education, emotional support, and access to sexual education and contraceptive methods. Persistent challenges in maternal and neonatal health despite existing prevention programs. | Focused on meta-analyses using all available studies regardless of bias level, which may affect the reliability of estimates. Lack of universally accepted diagnostic criteria for gestational diabetes limits cross-regional comparisons. |
| Quintero-Ortiz [39] | 2021 | Egypt, South Africa, United States, Colombia, England, Iraq, Japan, Turkey, Panama, Guatemala, Peru, Mexico, Ecuador, Venezuela | To compare the effects of expectant versus interventionist care in the management of pregnant women with severe preeclampsia remote from term. | Expectant care may result in lower incidence of Apgar scores < 7 at 5 min and higher average birth weight. Expectant care may decrease rates of neonatal death, hyaline membrane disease, and admission to the NICU. No significant differences in maternal mortality, eclampsia, HELLP syndrome, placental abruption, pulmonary edema, or renal failure. Expectant care extended pregnancy by an average of 1 week. | Low quality of evidence due to the nature of included studies. Imprecision in some outcomes. Limited number of studies included, making publication bias assessment unfeasible. High risk of bias in non-randomized studies (NRSs). |
| Database | Company/Organization | Address | Software |
|---|---|---|---|
| PubMed | NCBI/NLM (USA) | 8600 Rockville Pike, Bethesda, MD, USA | https://pubmed.ncbi.nlm.nih.gov/advanced/ (accessed on 20 February 2025) |
| Scopus | Elsevier | Radarweg 29, Amsterdam, Netherlands (HQ); 230 Park Ave, New York, NY, USA | https://scopus.com/ (accessed on 20 February 2025) |
| SciELO | FAPESP/SciELO Network | Rua Dr. Diogo de Faria 1087, São Paulo, SP, Brazil | https://search.scielo.org/advanced/?lang=es (accessed on 20 February 2025) |
| Redalyc | UAEMex | Instituto de Ciencias Agropecuarias y Rurales, Toluca, Estado de México, Mexico | https://www.redalyc.org/home.oa (accessed on 20 February 2025) |
| LILACS | BIREME/PAHO/WHO | Rua Botucatu 862, São Paulo, SP, Brazil | https://lilacs.bvsalud.org/es/ (accessed on 20 February 2025) |
| BVS-Ecuador | BIREME/PAHO + Ecuadorian institutions | Varies (typically Quito, Ecuador) | https://bvs-ecuador.bvsalud.org/ (accessed on 20 February 2025) |
| Analytic Approach | Search Strategy | Database | Results |
|---|---|---|---|
| Descriptive | (“preeclampsia” OR “pre-eclampsia”) AND (“Ecuador” OR “Ecuadorian”) AND (“descriptive” OR “incidence” OR “frequency” OR “prevalence”) | Scopus | 210 |
| PubMed | 3 | ||
| Scielo | 2 | ||
| Redalyc | 24 | ||
| BVS-Ecuador | 7 | ||
| LILACS | 4 | ||
| Diagnostic | (“preeclampsia” OR “pre-eclampsia”) AND (“Ecuador” OR “Ecuadorian”) AND (“diagnostic” OR “regression” OR “causal”) | Scopus | 142 |
| PubMed | 3 | ||
| Scielo | 0 | ||
| Redalyc | 18 | ||
| BVS-Ecuador | 1 | ||
| LILACS | 0 | ||
| Predictive | (“preeclampsia” OR “pre-eclampsia”) AND (“Ecuador” OR “Ecuadorian”) AND (“predictive” OR “prediction” OR “classification” OR “classifying”) | Scopus | 130 |
| PubMed | 2 | ||
| Scielo | 0 | ||
| Redalyc | 7 | ||
| BVS-Ecuador | 2 | ||
| LILACS | 1 | ||
| Prescriptive | (“preeclampsia” OR “pre-eclampsia”) AND (“Ecuador” OR “Ecuadorian”) AND “prescriptive” | Scopus | 4 |
| PubMed | 0 | ||
| Scielo | 0 | ||
| Redalyc | 0 | ||
| BVS-Ecuador | 0 | ||
| LILACS | 0 | ||
| Total | 558 |
| Authors/Year | Goal | n | Data | Technique | Contribution |
|---|---|---|---|---|---|
| Tejera et al.(2021) [4] | To study ethnic, geographical, and altitude differences in the incidence of preeclampsia and eclampsia in Ecuador. | 15,390 | A population-based retrospective study using data from the Ecuadorian National Institute of Statistics and Census (INEC) and the Ministry of Health (2015–2017) | Frequency distribution in absolute and relative values | This study highlights the importance of ethnicity, altitude, and geographical access to healthcare in the prevalence of preeclampsia and eclampsia in Ecuador. It provides valuable insights for targeted public health interventions. |
| Viteri-Hinojosa and Espinosa-Yépez (2024) [41] | To analyze morbidity due to anesthetic complications in obstetric patients in Ecuador (2018 to 2022) | 304 | A cross-sectional descriptive study using data from the National Institute of Statistics and Census (INEC) hospital discharge records (2018–2022). | Line plots, bar plots, mean | This study underscores the need for continuous monitoring and training in obstetric anesthesia to reduce complications. It also highlights the impact of external factors, such as the pandemic, on maternal health outcomes. |
| Parrales et al. (2024) [42] | To characterize preeclampsia patients using descriptive and clustering analysis to aid in the distribution of clinical care and prevention policies. | 6406 | Electronic medical records (EMRs) from the IESS Los Ceibos Hospital, collected from May 2017 to December 2023. | Frequency distribution in absolute and relative values, clustering | The findings highlight the importance of age and diagnostic profiles in understanding the prevalence and severity of preeclampsia. |
| Vargas et al. (2021) [43] | To determine the risk factors of hypertensive pregnancy disorders in pregnant women who attended prenatal care at the Universitary Hospital of the City of Guayaquil | 104 | Pregnant patients who attended the prenatal check-up at the Universitary Hospital of Guayaquil-Ecuador, from January 2019 to January 2020. | Frequency distribution in absolute and relative values | This study highlights that personal and family history of hypertensive disorders was a relevant risk factor, as well as nutrition, first parity, and change of partner. |
| Hernández et al. (2021) [44] | To determine the risk factors for preeclampsia in pregnant women from communities attended at the Hospital General Puyo. | 150 | direct observation, review of medical records of 150 pregnant women and survey applied during the period from January 2021 to April 2021. | Frequency distribution in absolute and relative values | This study highlights that the main factor influencing the risk of preeclampsia was the lack of knowledge on the part of the pregnant women due to their low level of education. |
| Authors/Year | Goal | n | Data | Technique | Contribution |
|---|---|---|---|---|---|
| Tejera et al. (2021) [4] | To study ethnic, geographical, and altitude differences in the incidence of preeclampsia and eclampsia in Ecuador. | 15,390 | A population-based retrospective study using data from the Ecuadorian National Institute of Statistics and Census (INEC) and the Ministry of Health (2015–2017) | Logistic regression and geospatial analysis were used to assess risk factors and spatial clusters of preeclampsia and eclampsia | This study highlights the importance of ethnicity, altitude, and geographical access to healthcare in the prevalence of preeclampsia and eclampsia in Ecuador. It provides valuable insights for targeted public health interventions. |
| Cho et al. (2021) [45] | To examine the prevalence and associated factors of preeclampsia, eclampsia, and gestational hypertension in adolescent women in the period 2019–2020 at the Homero Castanier Crespo Hospital in Azogues, 2021 | 298 | Retrospective data of adolescent women (aged 11 to 19 years) in the period 2019–2020 at the Homero Castanier Crespo Hospital in Azogues. | Association between preeclampsia and risk factors was determined with statistical measures such as odds ratio, chi-square, 95% confidence interval, and p-value less than 0.05. | This work highlights that the prevalence of hypertensive disorders in adolescents is high. Its causes may be low level of education, primiparous mothers, family history of preeclampsia, overweight and obesity. |
| Tite et al. (2024) [5] | To investigate the relationship between prenatal care and the incidence of preeclampsia among pregnant women in Ecuador. | 20,648 | The study uses data from the National Health and Nutrition Survey (ENSANUT) 2018, which includes a nationally representative sample of 20,648 mothers. | Use of binary logistic regression and multicollinearity tests. | The study finds that adequate prenatal care (more than five visits starting in the first trimester) significantly reduces the risk of preeclampsia. It also highlights that women from rural areas, with lower income, and with lower educational attainment are more susceptible to preeclampsia. |
| Dueñas et al. (2021) [10] | To investigates the relationship between altitude and neonatal survival among at-risk neonates in Ecuador. | 3016 | Data from the Ecuadorian Ministry of Public Health’s Surveillance System of Neonatal Mortality, including neonatal deaths registered between January 2014 and September 2017 across 126 public and private healthcare facilities. | The study used Cox proportional hazards models to estimate hazard ratios (HRs) for different altitude strata, adjusting for individual variables (e.g., birth weight, gestational age, Apgar score) and contextual variables (e.g., type of healthcare facility, level of care). | The study highlights the importance of considering altitude as a critical factor in neonatal health, particularly in high-altitude regions. The findings suggest that healthcare interventions and policies should take into account the challenges posed by high altitudes, especially for at-risk neonates. |
| Parrales et al. (2024b) [26] | To analyze the monthly occupancy of inpatient beds for preeclampsia care at the IESS Los Ceibos Hospital in Guayaquil, Ecuador, from May 2017 to December 2023 | 6406 | Electronic medical records (EMRs) from the IESS Los Ceibos Hospital, collected from May 2017 to December 2023. | Mann–Kendall test to see any consistent upward trend in preeclampsia care. | The study highlights seasonal fluctuations. It also presents anomalies in the increasing trend in the number of preeclampsia care cases due to COVID-19. |
| Authors/Year | Goal | n | Data | Technique | Contribution |
|---|---|---|---|---|---|
| Guerrero, K. and Abadie, P. (2024) [46] | To evaluate the operational capacity of the Hospital Clinic de Barcelona predictive model for the detection of preeclampsia (PE) risk in a cohort of women treated at IESS Los Ceibos Hospital in Guayaquil, Ecuador. | 304 | The study used 304 pregnant women at IESS Los Ceibos Hospital in Guayaquil, Ecuador, between August 2018 and August 2019. | Linear regression models from the Hospital Clinic de Barcelona were used for the detection of early and late risk of preeclampsia | The study suggests stratified screening with biomarkers in high-risk subgroups to optimize accuracy without universal screening, adapting resources to local needs in resource-limited settings like Ecuador. The model showed high predictive capacity with an AUC of 0.924, sensitivity of 88.46%, and specificity of 91.37%. |
| Parrales et al. (2024b) [26] | To analyze the monthly occupancy of inpatient beds for preeclampsia care at the IESS Los Ceibos Hospital in Guayaquil, Ecuador, from May 2017 to December 2023 | 6406 | Electronic medical records (EMRs) from the IESS Los Ceibos Hospital, collected from May 2017 to December 2023. | Techniques such as Dynamic Bayesian Networks (DBNs), Multilayer Perceptron (MLP), and Long Short-Term Memory (LSTM) were used for forecasting the inpatient bed occupancy. | The study highlights the need for better hospital resource management, especially during high-demand periods, and suggests strategies like clinical process redesign and capacity enhancement to reduce inpatient bed demand. The MLP model achieved the lowest MAPE (11.58%) and predicted peaks of 274 and 258 inpatient beds in September and November 2024, respectively. |
| Parrales et al. (2024c) [47] | To predict emergency room arrivals for preeclampsia at the IESS Hospital del Día Sur Valdivia. | 2926 | The data included 2926 EMRs on gynecological emergency care carried out between 2019 and 2023. | Techniques such as Extreme Learning Machine (ELM), Multilayer Perceptron (MLP), and Dynamic Bayesian Networks (DBN) were employed. | The study emphasizes the importance of predictive analytics in managing emergency care for preeclampsia, allowing hospitals to allocate resources more effectively and improve patient outcomes. The MLP model achieved the lowest MAPE (17.21%), with an RMSE of 4.21 and MAE of 2.74. It predicted 11 to 13 emergency arrivals due to preeclampsia for September to November 2024. |
| Parrales et al. (2024d) [1] | To predict and explain the risk of suffering preeclampsia at the IESS Los Ceibos Hospital. | 6406 | Electronic medical records (EMRs) from the IESS Los Ceibos Hospital, collected from May 2017 to December 2023. | Bayesian network classifiers (BNCs) including Naïve Bayes (NB), Tree-Augmented Naïve Bayes (TANcl), and Semi Naïve Bayes (FSSJ) were used. | The study suggests that early identification of high-risk patients (e.g., those with hypertension, tobacco use, and diabetes family history) can lead to timely interventions, reducing the incidence of preeclampsia and improving maternal health outcomes. The TANcl model achieved the highest accuracy (close to 90%) and was effective in predicting preeclampsia risk. The F1 score and specificity were also high, indicating good performance in identifying both positive and negative cases. |
| Vargas et al. (2023) [48] | To evaluate the role of serum homocysteine as a predictor of preeclampsia in pregnant women between 12 to 20 weeks of gestation. | 312 | Patients treated in the outpatient service of the Gynecology and Obstetrics service of the University Hospital of Guayaquil, in Guayaquil-Ecuador. The study period was from 1 October 2018 to 30 October 2019. | Inferential statistics were used for comparative analysis between groups. Categorical data were formed and chi-square was used to establish the association or difference. | The study contributes to the ongoing debate about the role of homocysteine in predicting preeclampsia. Although the results did not support homocysteine as a predictor, the findings are valuable for guiding future research and clinical practice, particularly in low-resource settings where preeclampsia is a significant public health issue. |
| Authors/Year | Goal | n | Data | Technique | Contribution |
|---|---|---|---|---|---|
| Parrales et al. (2024b) [26] | To quantify the effects of a closure on the number of inpatient beds needed for preeclampsia care during 2024 at the IESS Los Ceibos Hospital in Guayaquil, Ecuador | 6406 | Electronic medical records (EMRs) from the IESS Los Ceibos Hospital, collected from May 2017 to December 2023. | Bayesian structural time-series models. | The study simulated the impact of closing the hospitalization unit in 2024, similar to the COVID-19 scenario. The closure would result in an average of 130.33 monthly referrals, highlighting the need for alternative strategies to manage bed occupancy during crises. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parrales-Bravo, F.; Cevallos-Torres, L.; Vasquez-Cevallos, L.; Caicedo-Quiroz, R.; Tolozano-Benites, R.; Gómez-Rodríguez, V. A Review of the Use of Data Analytics to Address Preeclampsia in Ecuador Between 2020 and 2024. Diagnostics 2025, 15, 978. https://doi.org/10.3390/diagnostics15080978
Parrales-Bravo F, Cevallos-Torres L, Vasquez-Cevallos L, Caicedo-Quiroz R, Tolozano-Benites R, Gómez-Rodríguez V. A Review of the Use of Data Analytics to Address Preeclampsia in Ecuador Between 2020 and 2024. Diagnostics. 2025; 15(8):978. https://doi.org/10.3390/diagnostics15080978
Chicago/Turabian StyleParrales-Bravo, Franklin, Lorenzo Cevallos-Torres, Leonel Vasquez-Cevallos, Rosangela Caicedo-Quiroz, Roberto Tolozano-Benites, and Víctor Gómez-Rodríguez. 2025. "A Review of the Use of Data Analytics to Address Preeclampsia in Ecuador Between 2020 and 2024" Diagnostics 15, no. 8: 978. https://doi.org/10.3390/diagnostics15080978
APA StyleParrales-Bravo, F., Cevallos-Torres, L., Vasquez-Cevallos, L., Caicedo-Quiroz, R., Tolozano-Benites, R., & Gómez-Rodríguez, V. (2025). A Review of the Use of Data Analytics to Address Preeclampsia in Ecuador Between 2020 and 2024. Diagnostics, 15(8), 978. https://doi.org/10.3390/diagnostics15080978