
Evaluation of the Proximity of the Maxillary Teeth Root Apices to the Maxillary Sinus Floor in Romanian Subjects: A Cone-Beam Computed Tomography Study

 ,
,
Abstract
1. Introduction
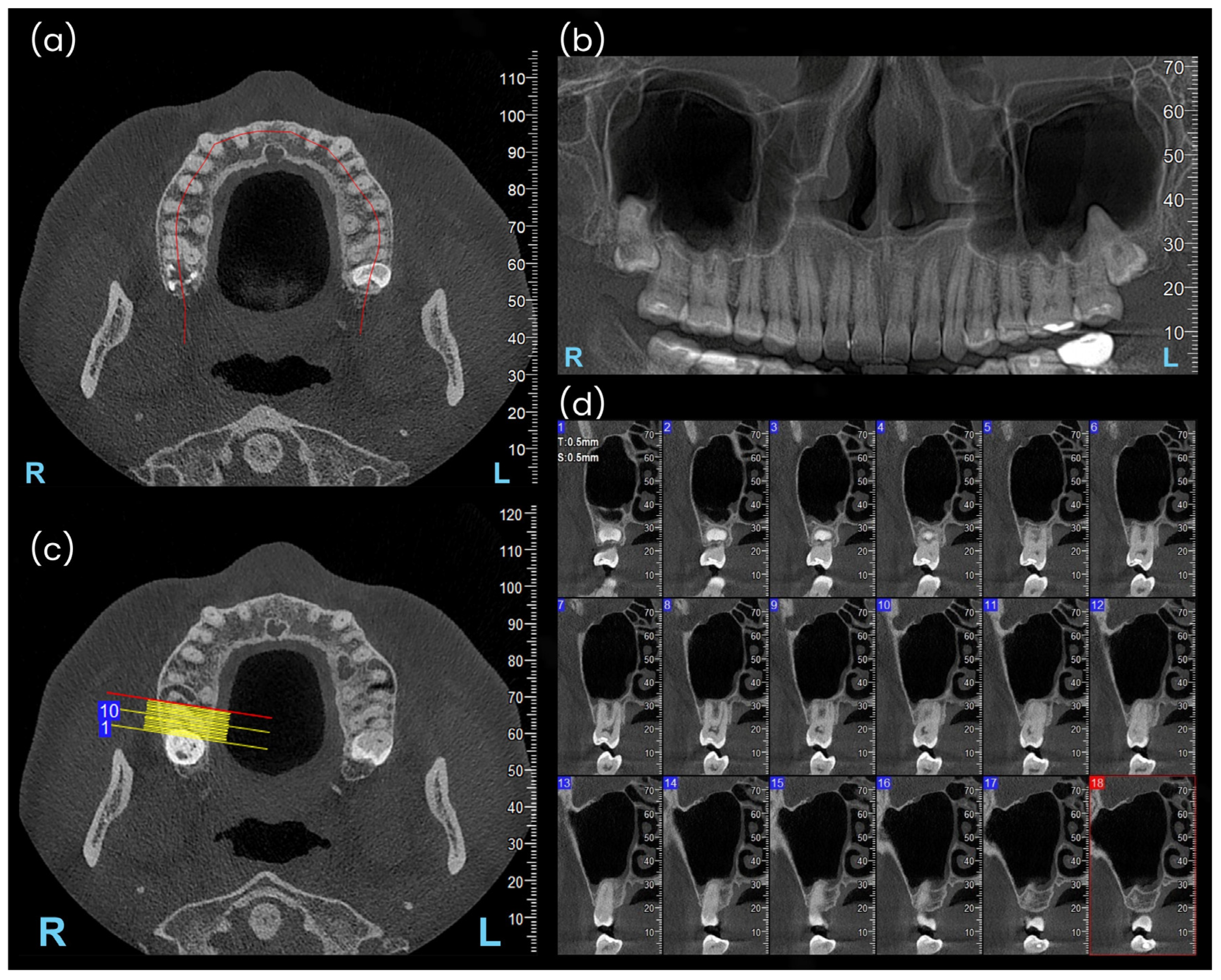
2. Materials and Methods
2.1. Study Design and Patient Selection
- Inclusion criteria
- -
- Patients who provided written informed consent at the time of their radiographic examination allowed for the potential use of their anonymized information in future scientific research publications.
- -
- Availability of CBCT scans including the maxillary sinuses, or at least their lower third.
- -
- Dentate adult subjects aged over 20 years.
- -
- Presence of fully erupted canines, premolars, and first and second molars in the dental arch.
- Exclusion criteria
- -
- Subjects with a diagnosis of chronic maxillary sinusitis.
- -
- Subjects presenting with chronic apical periodontitis or root resorption affecting the canines, premolars, or first and second molars.
- -
- History of non-surgical or surgical root canal treatment involving the aforementioned teeth.
- -
- History of orthodontic treatment or ongoing orthodontic therapy at the time of radiographic data acquisition.
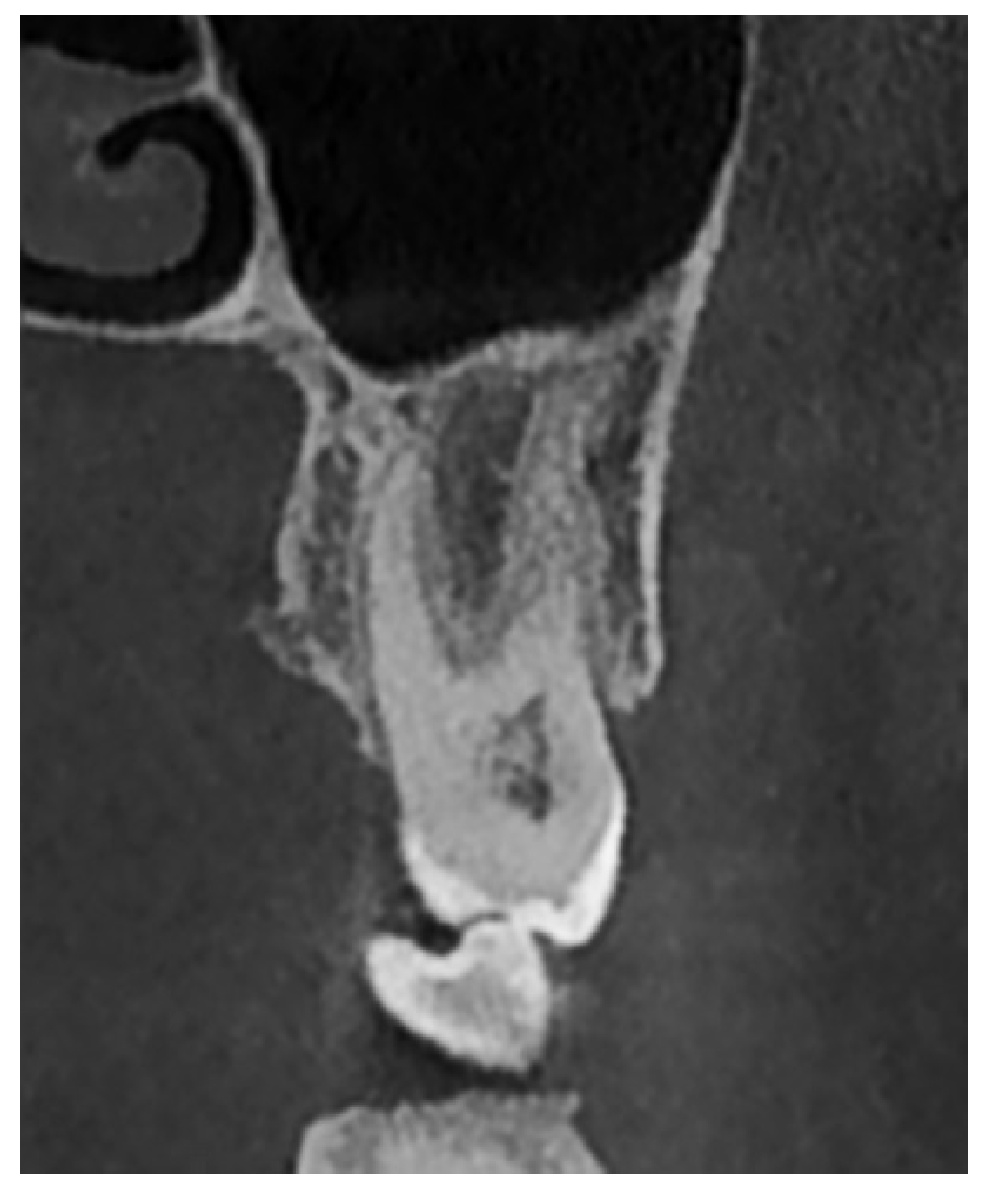
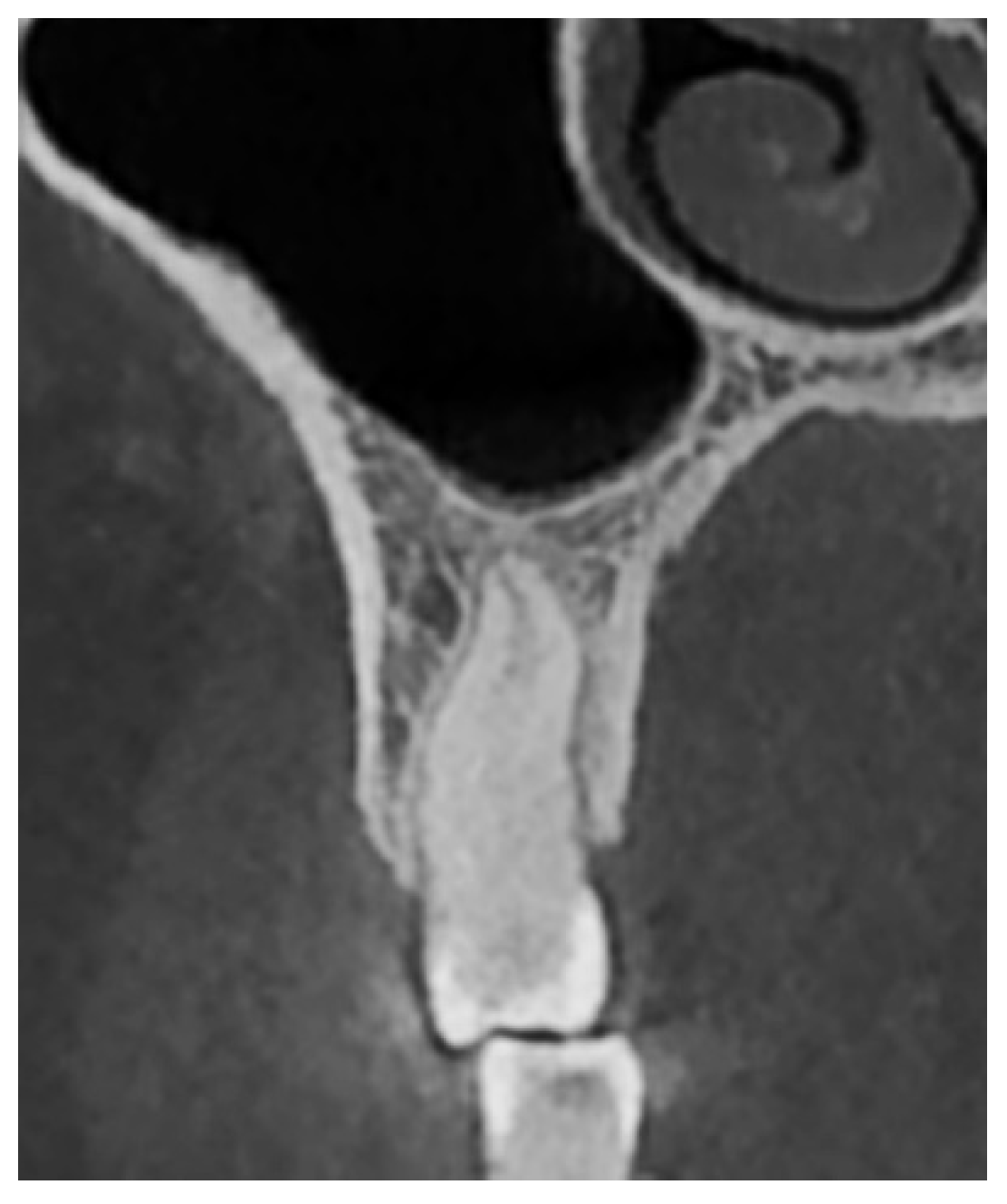
- Type I: Penetrating relationship—the tooth root extends into the maxillary sinus cavity (Figure 2).
- Type II: Tangential relationship—the tooth root is located 0–0.20 mm from the sinus floor (Figure 3).
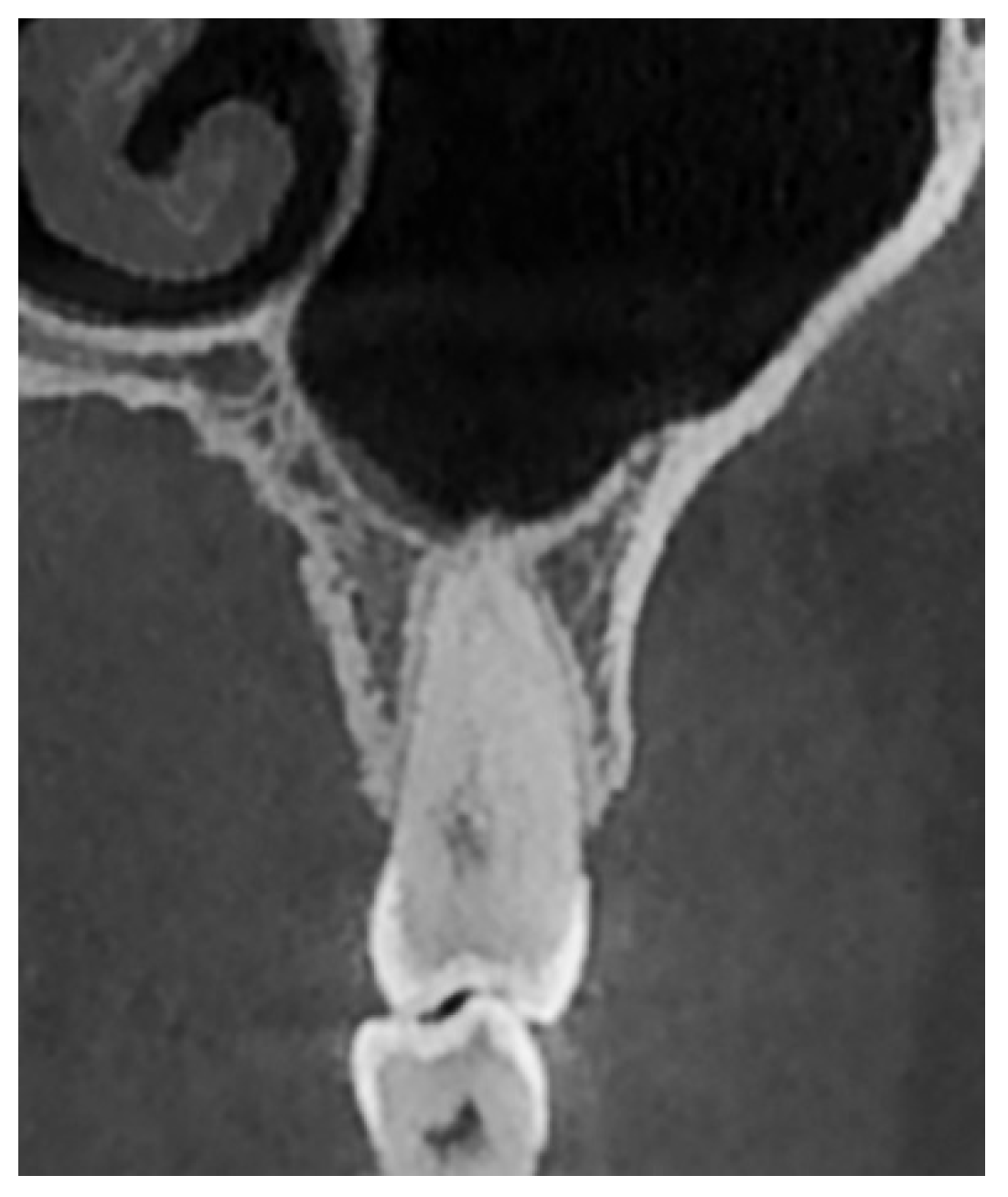
- Type III: Close relationship—the tooth root is located 0.21–2 mm from the sinus floor (Figure 4).
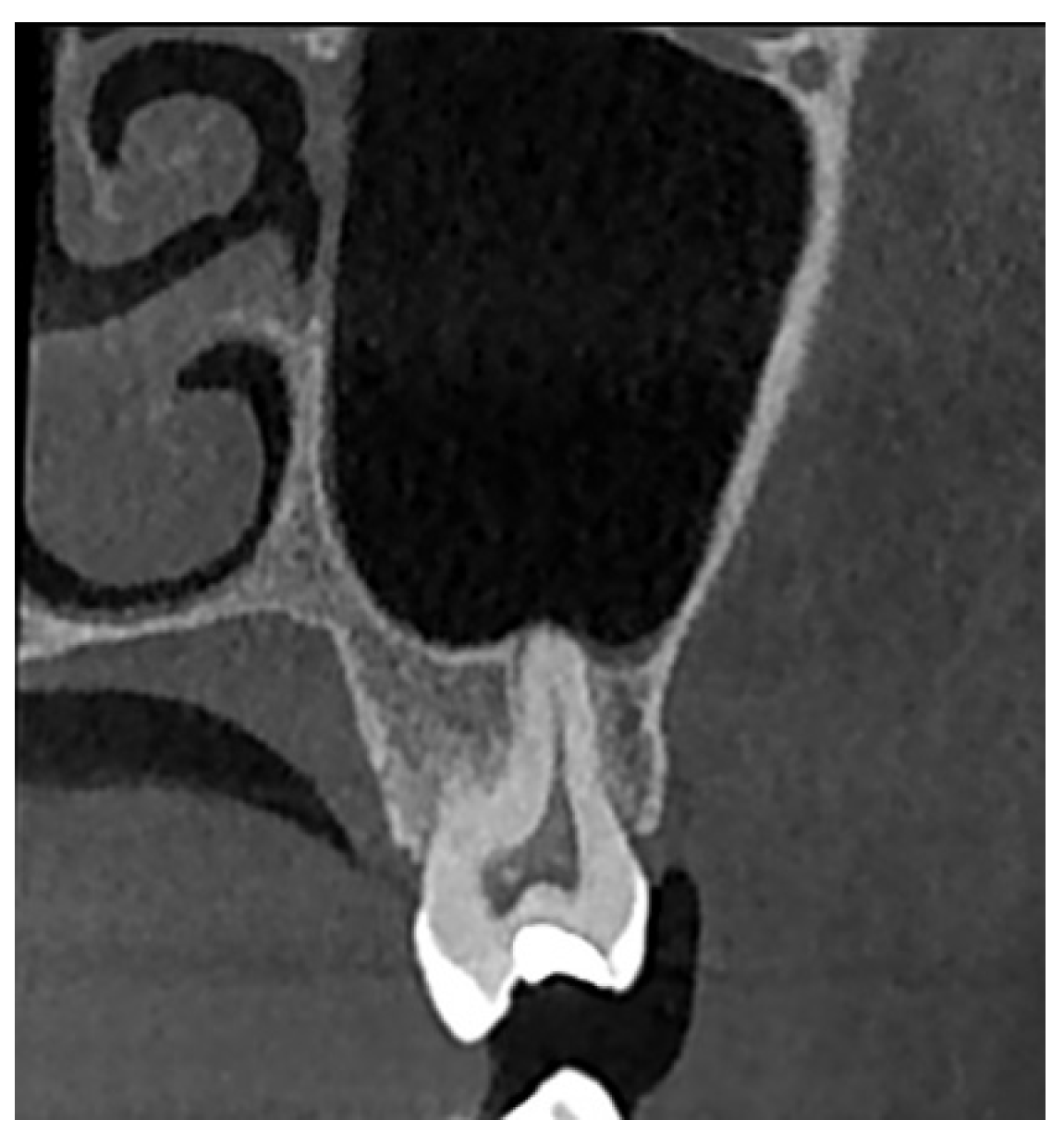
- Type IV: Spaced relationship—the tooth root is located more than 2 mm from the sinus floor (Figure 5).
2.2. Statistical Analysis
3. Results
3.1. Sample Description
3.2. Relationship of Teeth to the Maxillary Sinus Floor
- Canines most frequently exhibited a spaced relationship with the maxillary sinus floor.
- First premolars predominantly had spaced relationships, less frequently close relationships, and very rarely tangential relationships; no penetrating relationships were observed.
- Second premolars most commonly showed close relationships, followed by spaced relationships. Tangential relationships were observed less frequently and penetrating relationships were not encountered.
- First molars most frequently exhibited close relationships with the sinus floor. Tangential relationships followed in frequency, and penetrating relationships were the rarest. No spaced relationships were observed.
- Second molars most frequently displayed close relationships with the sinus floor, followed by tangential relationships. Penetrating and spaced relationships occurred much less frequently.
- Penetrating and tangential relationships were observed in first and second molars, with their combined frequency increasing with distal positioning of the tooth in the dental arch. Penetrating relationships were more commonly associated with the first molars, while tangential relationships were more frequently observed in the second molars.
- Statistically significant correlations were observed for all pairs of posterior teeth analyzed.
- Stronger correlations were observed between the distance to the sinus floor of each tooth and that of the adjacent tooth positioned distally.
- The correlation strength between neighboring teeth was higher than between non-neighboring teeth.
- The correlation coefficients between adjacent teeth increased in strength with the distal positioning of the tooth.
3.3. Relationship with the Maxillary Sinus Floor of Homologous Teeth
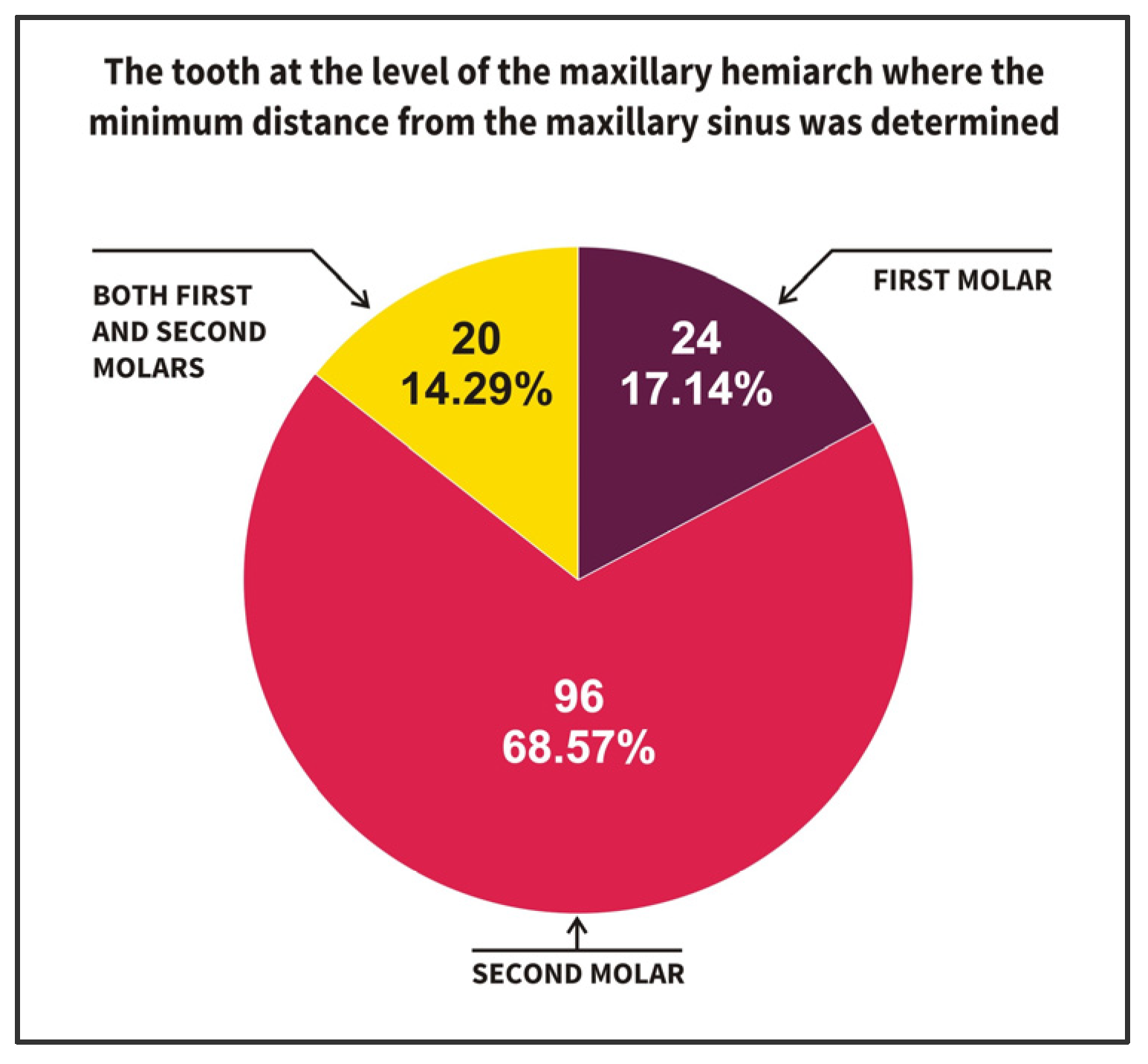
- The concordant tooth pairs were the majority, indicating symmetry between the left and right sides for the teeth closest to the sinus floor (referring to 49 concordant pairs, 7 + 38 + 4);
- Among the concordant pairs, the most frequently observed situation (n = 38 concordant pairs) was represented by the left and right second molars (n = 38; 54.3%).
- The number of discordant pairs was 21, with the most frequent situations being
- ○
- On the right dental hemiarch, the first molar was the closest tooth to the sinus floor, while on the left dental hemiarch, the second molar was the closest (7 pairs);
- ○
- On the right dental hemiarch, the second molar was the closest tooth to the sinus floor, while on the left side, the first and second molars were equally close (7 pairs).
3.4. Distance from the Root Apices to the Sinus Floor in Relation to Gender and Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CBCT | Cone-beam computed tomography |
| 1st M | First molar |
| 2nd M | Second molar |
| CT | Computed tomography |
| OPG | Orthopantomography |
References
- Blanton, P.L.; Biggs, N.L. Eighteen hundred years of controversy: The paranasal sinuses. Am. J. Anat. 1969, 124, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Stammberger, H. History of rhinology: Anatomy of the paranasal sinuses. Rhinology 1989, 27, 197–210. [Google Scholar]
- Mavrodi, A.; Paraskevas, G. Evolution of the paranasal sinuses’ anatomy through the ages. Anat. Cell Biol. 2013, 46, 235–238. [Google Scholar] [CrossRef]
- Mehra, P.; Jeong, D. Maxillary sinusitis of odontogenic origin. Curr. Allergy Asthma Rep. 2009, 9, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Psillas, G.; Papaioannou, D.; Petsali, S.; Dimas, G.G.; Constantinidis, J. Odontogenic maxillary sinusitis: A comprehensive review. J. Dent. Sci. 2021, 16, 474–481. [Google Scholar] [CrossRef]
- Hauman, C.H.; Chandler, N.P.; Tong, D.C. Endodontic implications of the maxillary sinus: A review. Int. Endod. J. 2002, 35, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, V.I.; Nimigean, V.; Nimigean, V.R.; Georgescu, L.; Preoteasa, C.T. Maxillary sinus implications in endodontics and implant dentistry—A literature review. Rom. J. Oral Rehabil. 2024, 16, 147–161. [Google Scholar] [CrossRef]
- Kilic, C.; Kamburoglu, K.; Yuksel, S.P.; Ozen, T. An assessment of the relationship between the maxillary sinus floor and the maxillary posterior teeth root tips using dental cone-beam computerized tomography. Eur. J. Dent. 2010, 4, 462–467. [Google Scholar]
- Jung, Y.H.; Cho, B.H. Assessment of the relationship between the maxillary molars and adjacent structures using cone beam computed tomography. Imaging Sci. Dent. 2012, 42, 219–224. [Google Scholar] [CrossRef]
- Gaudin, R.A.; Hoehle, L.P.; Smeets, R.; Heiland, M.; Caradonna, D.S.; Gray, S.T.; Sedaghat, A.R. Impact of odontogenic chronic rhinosinusitis on general health-related quality of life. Eur. Arch. Otorhinolaryngol. 2018, 275, 1477–1482. [Google Scholar] [CrossRef]
- Ariji, Y.; Obayashi, N.; Goto, M.; Izumi, M.; Naitoh, M.; Kurita, K.; Shimozato, K.; Ariji, E. Roots of the maxillary first and second molars in horizontal relation to alveolar cortical plates and maxillary sinus: Computed tomography assessment for infection spread. Clin. Oral Investig. 2006, 10, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M. Definition and management of odontogenic maxillary sinusitis. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 13. [Google Scholar] [CrossRef]
- Legert, K.G.; Zimmerman, M.; Stierna, P. Sinusitis of odontogenic origin: Pathophysiological implications of early treatment. Acta Otolaryngol. 2004, 124, 655–663. [Google Scholar] [CrossRef]
- Masood, A.; Moumoulidis, I.; Panesar, J. Acute rhinosinusitis in adults: An update on current management. Postgrad. Med. J. 2007, 83, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Sharan, A.; Madjar, D. Correlation between maxillary sinus floor topography and related root position of posterior teeth using panoramic and cross-sectional computed tomography imaging. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.H.; Park, H.D.; Yoon, H.R.; Kang, M.K.; Koh, K.S.; Kim, H.J. Topographic anatomy of the inferior wall of the maxillary sinus in Koreans. Int. J. Oral Maxillofac. Surg. 2004, 33, 382–388. [Google Scholar] [CrossRef]
- Mattar, E.; Hammad, L.; Faden, A.; Khalil, H. Relation of maxillary teeth to the maxillary sinus in normal Saudi individuals living in Riyadh. Biosci. Biotechnol. Res. Asia 2010, 7, 695–700. [Google Scholar]
- Shaul Hameed, K.; Abd Elaleem, E.; Alasmari, D. Radiographic evaluation of the anatomical relationship of maxillary sinus floor with maxillary posterior teeth apices in the population of Al-Qassim, Saudi Arabia, using cone beam computed tomography. Saudi Dent. J. 2021, 33, 769–774. [Google Scholar] [CrossRef]
- Abdulwahed, A.; Mustafa, M.; Karobari, M.I.; Alomran, A.; Alasimi, K.; Alsayeg, A.; Alsakaker, A.; Alamri, H.M. Anatomical Evaluation of Posterior Maxillary Roots in Relation to the Maxillary Sinus Floor in a Saudi Sub-Population: A Cross-Sectional Cone-Beam Computed Tomography Study. Healthcare 2023, 11, 150. [Google Scholar] [CrossRef]
- Akotiya, B.R.; Surana, A.; Chauhan, P.; Saha, S.G.; Agarwal, R.S.; Vashisht, A. Morphometric analysis of the relationship between maxillary posterior teeth and maxillary sinus floor in central Indian population: A cone-beam computed tomography study. J. Conserv. Dent. Endod. 2024, 27, 373–377. [Google Scholar] [CrossRef]
- Tian, X.M.; Qian, L.; Xin, X.Z.; Wei, B.; Gong, Y. An Analysis of the Proximity of Maxillary Posterior Teeth to the Maxillary Sinus Using Cone-beam Computed Tomography. J. Endod. 2016, 42, 371–377. [Google Scholar] [CrossRef]
- Pei, J.; Liu, J.; Chen, Y.; Liu, Y.; Liao, X.; Pan, J. Relationship between maxillary posterior molar roots and the maxillary sinus floor: Cone-beam computed tomography analysis of a western Chinese population. J. Int. Med. Res. 2020, 48, 300060520926896. [Google Scholar] [CrossRef] [PubMed]
- Georgiev, T.; Peev, S.; Arnautska, H. Relationship between root apices of maxillary posterior teeth and the maxillary sinus floor in patients from the Varna Region. J. Med. Dent. Pract. 2015, 2, 300–309. [Google Scholar] [CrossRef]
- Tafakhori, Z.; Sheykhfathollahi, M.; Nemati, S. Evaluating the distance between posterior teeth and the maxillary sinus floor using cone beam computed tomography. J. Dentomaxillofacial Radiol. Pathol. Surg. 2018, 7, 145–150. [Google Scholar]
- Pagin, O.; Centurion, B.S.; Rubira-Bullen, I.R.; Alvares Capelozza, A.L. Maxillary sinus and posterior teeth: Accessing close relationship by cone-beam computed tomographic scanning in a Brazilian population. J. Endod. 2013, 39, 748–751. [Google Scholar] [CrossRef]
- Junqueira, R.B.; Souza-Nunes, L.A.; Scalioni, F.A.R.; Damasceno, N.N.L.; Verner, F.S.; Carvalho, A.C.P.; Paula, M.V.Q.; Devito, K.L. Anatomical evaluation of the relationship between the maxillary posterior teeth and maxillary sinus. Gen. Dent. 2020, 68, 66–71. [Google Scholar]
- Shrestha, B.; Dunn, L. The Declaration of Helsinki on Medical Research involving Human Subjects: A Review of Seventh Revision. J. Nepal Health Res. Counc. 2020, 17, 548–552. [Google Scholar] [CrossRef]
- Nimigean, V.; Nimigean, V.R.; Măru, N.; Sălăvăstru, D.I.; Bădiţă, D.; Ţuculină, M.J. The maxillary sinus floor in the oral implantology. Rom. J. Morphol. Embryol. 2008, 49, 485–489. [Google Scholar]
- Oishi, S.; Ishida, Y.; Matsumura, T.; Kita, S.; Sakaguchi-Kuma, T.; Imamura, T.; Ikeda, Y.; Kawabe, A.; Okuzawa, M.; Ono, T. A cone-beam computed tomographic assessment of the proximity of the maxillary canine and posterior teeth to the maxillary sinus floor: Lessons from 4778 roots. Am. J. Orthod. Dentofacial. Orthop. 2020, 157, 792–802. [Google Scholar] [CrossRef]
- Khojastepour, L.; Movahhedian, N.; Zolghadrpour, M.; Mahjoori-Ghasrodashti, M. Assessment of the relationship between the maxillary sinus and the canine root tip using cone beam computed tomography. BMC Oral Health 2021, 21, 338. [Google Scholar] [CrossRef]
- Regnstrand, T.; Torres, A.; Petitjean, E.; Lambrechts, P.; Benchimol, D.; Jacobs, R. CBCT-based assessment of the anatomic relationship between maxillary sinus and upper teeth. Clin. Exp. Dent. Res. 2021, 7, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.J.; Gamba, T.O.; Bertinato, J.V.; Freitas, D.Q. Comparison of panoramic radiography and CBCT to identify maxillary posterior roots invading the maxillary sinus. Dentomaxillofac. Radiol. 2016, 45, 20160043. [Google Scholar] [CrossRef]
- Gu, Y.; Sun, C.; Wu, D.; Zhu, Q.; Leng, D.; Zhou, Y. Evaluation of the relationship between maxillary posterior teeth and the maxillary sinus floor using cone-beam computed tomography. BMC Oral Health 2018, 18, 164. [Google Scholar] [CrossRef]
- Razumova, S.; Brago, A.; Howijieh, A.; Manvelyan, A.; Barakat, H.; Baykulova, M. Evaluation of the relationship between the maxillary sinus floor and the root apices of the maxillary posterior teeth using cone-beam computed tomographic scanning. J. Conserv. Dent. 2019, 22, 139–143. [Google Scholar] [CrossRef]
- Altaweel, A.A.; Saad Sowairi, S.M.; Saaduddin Sapri, A.M.; Saeedi, S.A.; Alamri, A.H.; Alnobi, A.A.; Fahad ALSharif, M.; Mohsen A Altokhi, A.; Abbas, H. Assessment of the Relationship between Maxillary Posterior Teeth and Maxillary Sinus Using Cone-Beam Computed Tomography. Int. J. Dent. 2022, 2022, 6254656. [Google Scholar] [CrossRef]
- Sarilita, E.; Muhammad, R.M.; Nugraha, H.G.; Murniati, N.; Yusuf, H.Y.; Takeshita, Y.; Asaumi, J. Anatomical relationship between maxillary posterior teeth and the maxillary sinus in an Indonesian population: A CT scan study. BMC Oral Health 2024, 24, 1014. [Google Scholar] [CrossRef]
- Ok, E.; Güngör, E.; Colak, M.; Altunsoy, M.; Nur, B.G.; Ağlarci, O.S. Evaluation of the relationship between the maxillary posterior teeth and the sinus floor using cone-beam computed tomography. Surg. Radiol. Anat. 2014, 36, 907–914. [Google Scholar] [CrossRef]
- von Arx, T.; Fodich, I.; Bornstein, M.M. Proximity of premolar roots to maxillary sinus: A radiographic survey using cone-beam computed tomography. J. Endod. 2014, 40, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- Ariji, Y.; Kuroki, T.; Moriguchi, S.; Ariji, E.; Kanda, S. Age changes in the volume of the human maxillary sinus: A study using computed tomography. Dentomaxillofac. Radiol. 1994, 23, 163–168. [Google Scholar] [CrossRef]
- Scheid, R.C.; Weiss, G. Morphology of permanent molars. In Woelfel’s Dental Anatomy, 9th ed.; Scheid, R.C., Weiss, G., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2017; pp. 135–181. [Google Scholar]
- Stoica, S.N.; Nimigean, V.; Vîrlan, M.J.R.; Nimigean, V.R. The Pathology of the First Permanent Molar during the Mixed Dentition Stage—Review. Appl. Sci. 2023, 13, 483. [Google Scholar] [CrossRef]
- Kuroda, S.; Wazen, R.; Moffatt, P.; Tanaka, E.; Nanci, A. Mechanical stress induces bone formation in the maxillary sinus in a short-term mouse model. Clin. Oral Investig. 2013, 17, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Motiwala, M.A.; Arif, A.; Ghafoor, R. A CBCT based evaluation of root proximity of maxillary posterior teeth to sinus floor in a subset of Pakistani population. J. Pak. Med. Assoc. 2021, 71, 1992–1995. [Google Scholar] [CrossRef]
- Robaian, A.; Alqhtani, N.R.; Alghomlas, Z.I.; Alzahrani, A.; Almalki, A.K.; Al Rafedah, A.; Al Abdulsalam, A.; Alzahrani, K.M. Vertical relationships between the divergence angle of maxillary molar roots and the maxillary sinus floor: A cone-beam computed tomography (CBCT) study. Saudi Dent. J. 2021, 33, 958–964. [Google Scholar] [CrossRef]
- Rodríguez, M.; Marshall, M.; Godoy, C.; Richa, R.; Niklander, S.E. Orthopantomography Versus Cone Beam Computed Tomography for the Assessment of the Proximity of Posterior Maxillary Apexes with the Maxillary Sinus: A Cross-sectional Study. Curr. Med. Imaging 2024, 20, 1–7. [Google Scholar] [CrossRef]
- Amani, R.; Noroozi, M.; Ashrafi, M.M.S. Assessment of the relationships between posterior root apices and the maxillary sinus floor: A comparison of panoramic radiography and cone beam computed tomography. Gen. Dent. 2023, 71, 58–63. [Google Scholar]
- Ahmed, A.; Sajad, M.; Malik, I.; Singh, A.; Anjum, G. Topographic Relationship of Maxillary Sinus Floor with the Posterior Teeth Roots Using Panoramic Radiography and Cone Beam Computed Tomography (CBCT). Ann. Int. Med. Den. Res. 2018, 4, DE82–DE86. Available online: https://www.aimdrjournal.com/wp-content/uploads/2021/09/DE18_OA_Anies-edit.pdf (accessed on 21 February 2025).
- Kirkham-Ali, K.; La, M.; Sher, J.; Sholapurkar, A. Comparison of cone-beam computed tomography and panoramic imaging in assessing the relationship between posterior maxillary tooth roots and the maxillary sinus: A systematic review. J. Investig. Clin. Dent. 2019, 10, e12402. [Google Scholar] [CrossRef]
- Jung, Y.H.; Cho, B.H.; Hwang, J.J. Comparison of panoramic radiography and cone-beam computed tomography for assessing radiographic signs indicating root protrusion into the maxillary sinus. Imaging Sci. Dent. 2020, 50, 309–318. [Google Scholar] [CrossRef]
- Chaves, L.L.V.; Lopes Rosado, L.P.; Piccolo, S.M.; Ferreira, L.M.; Kamburoglu, K.; Junqueira, R.B.; Aquino de Castro, M.A.; Verner, F.S. Evaluation of the Maxillary Sinus of Patients with Maxillary Posterior Implants: A CBCT Cross-Sectional Study. Diagnostics 2022, 12, 3169. [Google Scholar] [CrossRef]
- Morgan, N.; Meeus, J.; Shujaat, S.; Cortellini, S.; Bornstein, M.M.; Jacobs, R. CBCT for Diagnostics, Treatment Planning and Monitoring of Sinus Floor Elevation Procedures. Diagnostics 2023, 13, 1684. [Google Scholar] [CrossRef]
- Kuligowski, P.; Jaroń, A.; Preuss, O.; Gabrysz-Trybek, E.; Bladowska, J.; Trybek, G. Association between Odontogenic and Maxillary Sinus Conditions: A Retrospective Cone-Beam Computed Tomographic Study. J. Clin. Med. 2021, 10, 2849. [Google Scholar] [CrossRef]
- Alghofaily, M.; Alsufyani, N.; Althumairy, R.I.; AlSuhaibani, A.; Alfawzan, F.; AlSadhan, L. Odontogenic Factors Associated with Maxillary Sinus Schneiderian Membrane Thickness and their Relationship to Chronic Sinonasal Symptoms: An Ambispective Cohort Study. Diagnostics 2023, 13, 2710. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, M.A.; Szczygielski, K.; Chloupek, A.; Szczupak, P.; Jurkiewicz, D. Clinical characteristics of odontogenic sinusitis with periapical lesions. Am. J. Otolaryngol. 2022, 43, 103338. [Google Scholar] [CrossRef]
- Nimigean, V.R.; Nimigean, V.; Maru, N.; Andressakis, D.; Balatsouras, D.G.; Danielidis, V. The maxillary sinus and its endodontic implications: Clinical study and review. B-ENT 2006, 2, 167–175. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tooth | Distance | |||
|---|---|---|---|---|
| Type I (Penetrating Relationship) | Type II (Tangential Relationship) | Type III (Close Relationship) | Type IV (Spaced Relationship) | |
| Canine | n = 0; 0% | n = 0; 0% | n = 3; 37.5% | n = 5; 62.5% |
| 1st Premolar | n = 0; 0% | n = 1; 0.7% | n = 32; 23.4% | n = 104; 75.9% |
| 2nd Premolar | n = 0; 0% | n = 11; 7.9% | n = 72; 51.8% | n = 56; 40.3% |
| 1st Molar | n = 9; 6.5% | n = 33; 23.9% | n = 96; 69.6% | n = 0; 0% |
| 2nd Molar | n = 4; 2.9% | n = 47; 33.6% | n = 85; 60.7% | n = 4; 2.9% |
| Tooth | Distance to the Sinus Floor Median (Interquartile Range) | p-Value 1 | p-Value 2 | ||
|---|---|---|---|---|---|
| 2nd Premolar | 1st Molar | 2nd Molar | |||
| Canine | 2.93 (1.04; 5.79) mm | ||||
| 1st Premolar | 3.68 (2.05; 5.13) mm | <0.001 | <0.001 | <0.001 | <0.001 |
| 2nd Premolar | 1.45 (0.62; 2.54) mm | <0.001 | <0.001 | ||
| 1st Molar | 0.50 (0.20; 0.15) mm | 0.002 | |||
| 2nd Molar | 0.34 (0.15; 0.80) mm | ||||
| 1st Premolar | 2nd Premolar | 1st Molar | 2nd Molar | ||
|---|---|---|---|---|---|
| Canine | Correlation coefficient | 0.810 | 0.536 | 0.886 | 0.759 |
| p | 0.015 | 0.215 | 0.019 | 0.029 | |
| n | 8 | 7 | 6 | 8 | |
| 1st Premolar | Correlation coefficient | 0.682 | 0.483 | 0.444 | |
| p | <0.001 | <0.001 | <0.001 | ||
| n | 134 | 129 | 135 | ||
| 2nd Premolar | Correlation coefficient | 0.724 | 0.606 | ||
| p | <0.001 | <0.001 | |||
| n | 127 | 133 | |||
| 1st Molar | Correlation coefficient | 0.840 | |||
| p | <0.001 | ||||
| n | 129 | ||||
| Indicator | Minimum Distance | |
|---|---|---|
| Mean | 0.56 | |
| Median | 0.295 | |
| Minimum | 0.00 | |
| Maximum | 3.02 | |
| Quartile | 1 | 0.14 |
| 2 | 0.295 | |
| 3 | 0.77 | |
| Tooth | Side | Type I Relationship | Type II Relationship | Type III Relationship | Type IV Relationship | p-Value |
|---|---|---|---|---|---|---|
| Canine | Right | n = 0; 0% | n = 0; 0% | n = 1; 20% | n = 4; 80% | 0.464 |
| Left | n = 0; 0% | n = 0; 0% | n = 2; 66.7% | n = 1; 33.3% | ||
| 1st Premolar | Right | n = 0; 0% | n = 0; 0% | n = 17; 24.6% | n = 52; 75.4% | 0.572 |
| Left | n = 0; 0% | n = 1; 1.5% | n = 15; 22.1% | n = 52; 76.5% | ||
| 2nd Premolar | Right | n = 0; 0% | n = 7; 10% | n = 34; 48.6% | n = 29; 41.4% | 0.576 |
| Left | n = 0; 0% | n = 4; 5.8% | n = 38; 55.1% | n = 27; 39.1% | ||
| 1st Molar | Right | n = 6; 8.8% | n = 19; 27.9% | n = 43; 63.2% | n = 0; 0% | 0.284 |
| Left | n = 3; 4.3% | n = 14; 20% | n = 53; 75.7% | n = 0; 0% | ||
| 2nd Molar | Right | n = 2; 2.9% | n = 22; 31.4% | n = 45; 64.3% | n = 1; 1.4% | 0.738 |
| Left | n = 2; 2.9% | n = 25; 35.7% | n = 40; 57.1% | n = 3; 4.3% |
| Homologous Teeth | Right Side (Median) | Left Side (Median) | p-Value |
|---|---|---|---|
| Canine | 5.58 | 1.20 | 0.180 |
| 1st Premolar | 2.32 | 0.61 | 0.078 |
| 2nd Premolar | 1.24 | 0.61 | 0.239 |
| 1st Molar | 0.15 | 0.12 | 0.250 |
| 2nd Molar | 0.40 | 0.10 | 0.250 |
| Concordance Analysis | Minimum Distance from the Sinus Floor on the Left Dental Hemiarch | |||
|---|---|---|---|---|
| 1st Molar | 2nd Molar | 1st Molar and 2nd Molar the Same | ||
| Minimum Distance from the Sinus Floor on the Right Dental Hemiarch | 1st Molar | 7 | 7 | 1 |
| 2nd Molar | 2 | 38 | 7 | |
| 1st Molar and 2nd Molar the same | 0 | 4 | 4 | |
| Indicator | Minimum Distance on the Right Dental Hemiarch | Minimum Distance on the Left Dental Hemiarch | p-Value | |
|---|---|---|---|---|
| Mean | 0.605 | 0.5076 | 0.007 | |
| Median | 0.365 | 0.280 | ||
| Minimum | 0.0 | 0.0 | ||
| Maximum | 2.93 | 3.02 | ||
| Quartile | 1 | 0.1475 | 0.120 | |
| 2 | 0.365 | 0.280 | ||
| 3 | 0.885 | 0.690 | ||
| Homologous Teeth | Absolute Difference in the Distance from the Sinus Floor of Homologous Teeth Compared to the Value of 0 (Left/Right Difference) | p-Value | |
|---|---|---|---|
| Median | Mean | ||
| 14–24 | 0.40 | 0.79 | <0.001 |
| 15–25 | 0.31 | 0.52 | <0.001 |
| 16–26 | 0.12 | 0.23 | <0.001 |
| 17–27 | 0.13 | 0.23 | <0.001 |
| Tooth | Sex of the Subjects | Type of Relationship with the Sinus | Total | ||||
|---|---|---|---|---|---|---|---|
| Type I | Type II | Type III | Type IV | ||||
| Canine | Male | n | 0 | 0 | 3 | 2 | 5 |
| % | 0% | 0% | 60% | 40% | 100% | ||
| Female | n | 0 | 0 | 0 | 3 | 3 | |
| % | 0% | 0% | 0% | 100% | 100% | ||
| 1st Premolar | Male | n | 0 | 1 | 21 | 46 | 68 |
| % | 0% | 1.5% | 30.9% | 67.6% | 100% | ||
| Female | n | 0 | 0 | 11 | 58 | 69 | |
| % | 0% | 0% | 15.9% | 84.1% | 100% | ||
| 2nd Premolar | Male | n | 0 | 5 | 40 | 22 | 67 |
| % | 0% | 7.5% | 59.7% | 32.8% | 100% | ||
| Female | n | 0 | 6 | 32 | 34 | 72 | |
| % | 0 | 8.3% | 44.4% | 47.2% | 100% | ||
| 1st Molar | Male | n | 4 | 19 | 44 | 0 | 67 |
| % | 6.0% | 28.4% | 65.7% | 0% | 100% | ||
| Female | n | 5 | 14 | 52 | 0 | 71 | |
| % | 7% | 19.7% | 73.2% | 0% | 100% | ||
| 2nd Molar | Male | n | 1 | 28 | 38 | 1 | 68 |
| % | 1.5% | 41.2% | 55.9% | 1.5% | 100% | ||
| Female | n | 3 | 19 | 47 | 3 | 72 | |
| % | 4.2% | 26.4% | 65.3% | 4.2% | 100% | ||
| Distance from the Sinus (Median) | Male | Female | p-Value |
|---|---|---|---|
| Canine | 1.2 | 5.58 | 0.143 |
| 1st Premolar | 3.32 | 4.1 | 0.054 |
| 2nd Premolar | 1.3 | 1.64 | 0.522 |
| 1st Molar | 0.39 | 0.55 | 0.462 |
| 2nd Molar | 0.26 | 0.45 | 0.038 |
| Tooth | Age (Median) Corresponding to the Different Types of Relationships with the Maxillary Sinus | p-Value | |||
|---|---|---|---|---|---|
| Type I | Type II | Type III | Type IV | ||
| Canine | - | - | 34 | 34 | >0.999 |
| 1st Premolar | - | 39 | 40 | 41 | 0.951 |
| 2nd Premolar | - | 45 | 36 | 45 | 0.503 |
| 1st Molar | 31 | 40 | 43 | - | 0.039 |
| 2nd Molar | 34 | 36 | 43 | 36 | 0.536 |
| 1st Premolar | 2nd Premolar | 1st Molar | 2nd Molar | Teeth with Minimum Distance at Dental Hemiarch Level | ||
|---|---|---|---|---|---|---|
| Age (years) | Correlation coefficient | −0.063 | 0.007 | 0.044 | 0.083 | 0.139 |
| p-Value | 0.466 | 0.933 | 0.621 | 0.340 | 0.101 | |
| Number of teeth | 137 | 139 | 138 | 140 | 140 | |
| The Level Where the Minimum Distance Was Registered |
Age (Median) | p-Value 1 | Pairwise Comparisons | p-Value 2 |
|---|---|---|---|---|
| 1st M | 34 | 0.024 | Minimum distance at 1st M—Minimum distance at 2nd M | 0.027 |
| 2nd M | 41.5 | Minimum distance at 1st M—Minimum distance the same for 1st M and 2nd M | 0.084 | |
| Minimum distance the same for 1st M and 2nd M | 41 | Minimum distance at 2nd M—Minimum distance the same for 1st M and 2nd M | >0.999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iliescu, V.I.; Nimigean, V.R.; Preoteasa, C.T.; Georgescu, L.; Nimigean, V. Evaluation of the Proximity of the Maxillary Teeth Root Apices to the Maxillary Sinus Floor in Romanian Subjects: A Cone-Beam Computed Tomography Study. Diagnostics 2025, 15, 1741. https://doi.org/10.3390/diagnostics15141741
Iliescu VI, Nimigean VR, Preoteasa CT, Georgescu L, Nimigean V. Evaluation of the Proximity of the Maxillary Teeth Root Apices to the Maxillary Sinus Floor in Romanian Subjects: A Cone-Beam Computed Tomography Study. Diagnostics. 2025; 15(14):1741. https://doi.org/10.3390/diagnostics15141741
Chicago/Turabian StyleIliescu, Vlad Ionuţ, Vanda Roxana Nimigean, Cristina Teodora Preoteasa, Lavinia Georgescu, and Victor Nimigean. 2025. "Evaluation of the Proximity of the Maxillary Teeth Root Apices to the Maxillary Sinus Floor in Romanian Subjects: A Cone-Beam Computed Tomography Study" Diagnostics 15, no. 14: 1741. https://doi.org/10.3390/diagnostics15141741
APA StyleIliescu, V. I., Nimigean, V. R., Preoteasa, C. T., Georgescu, L., & Nimigean, V. (2025). Evaluation of the Proximity of the Maxillary Teeth Root Apices to the Maxillary Sinus Floor in Romanian Subjects: A Cone-Beam Computed Tomography Study. Diagnostics, 15(14), 1741. https://doi.org/10.3390/diagnostics15141741