
The Effects of Outdoor Activity on Patient-Reported Visual Outcomes Under Perioperative Management Using Cyclosporine and Rebamipide

 , , , , , ,
, , , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics and Biometric Parameters
3.2. Ocular Surface Parameters and Symptom Scores
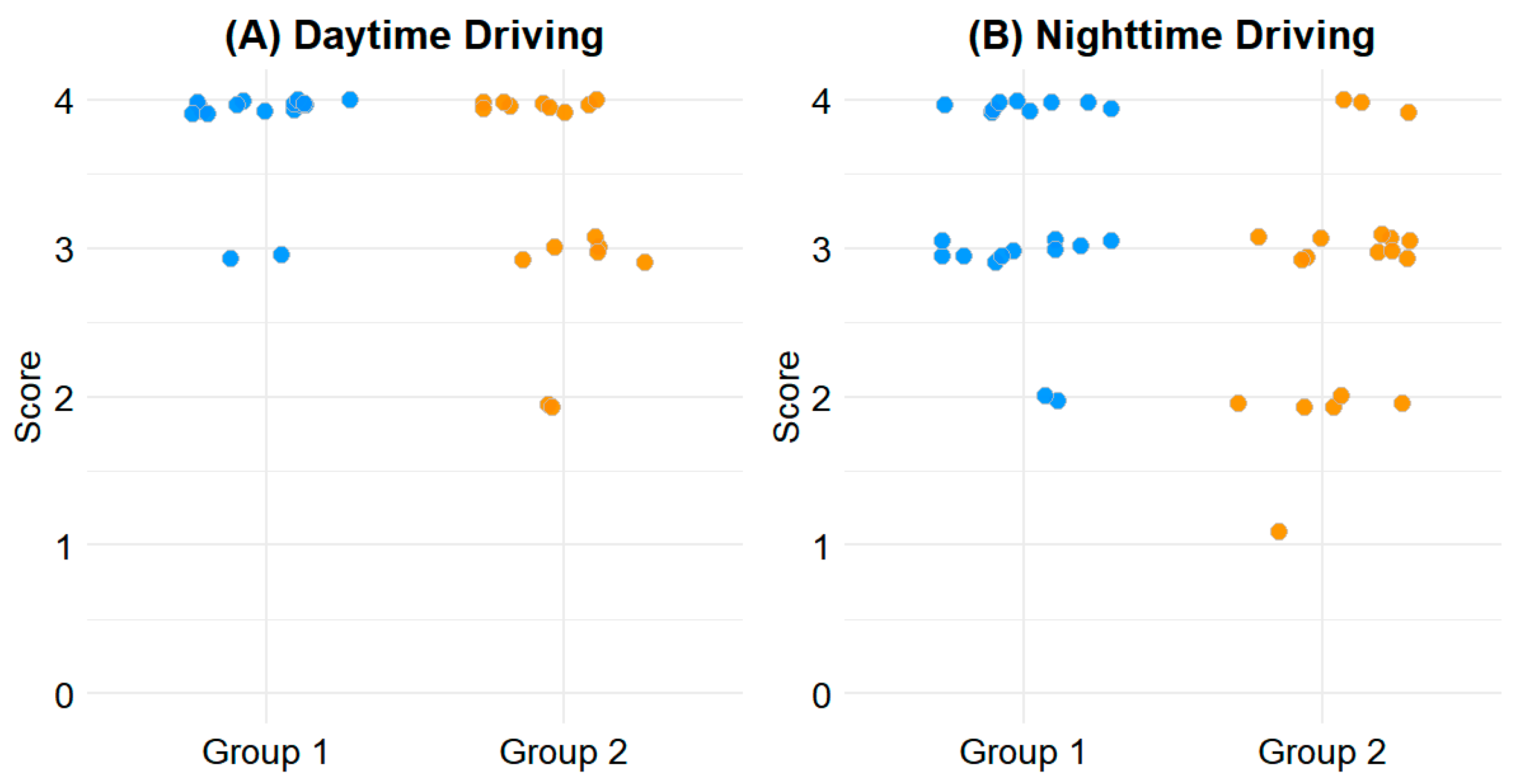
3.3. CVFQ Outcomes and Driving-Related Discomfort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BCVA | Best Corrected Visual Acuity |
| CVFQ | Cataract-related Visual Function Questionnaire |
| OSDI | Ocular Surface Disease Index |
| SE | Spherical Equivalent |
| SICCA | Sjögren’s International Collaborative Clinical Alliance |
| TBUT | Tear Break-Up Time |
| UDVA | Uncorrected Distance Visual Acuity |
| IOP | Intraocular Pressure |
| NRS | Numerical Rating Scale |
References
- Yoon, S.C.; Jung, J.W.; Sohn, H.J.; Shyn, K.H. Cataract and refractive surgery in; A survey of KSCRS members from 1995~2006. Korean J. Ophthalmol. 2009, 23, 142–147. [Google Scholar] [CrossRef]
- Gollogly, H.E.; Hodge, D.O.; St Sauver, J.L.; Erie, J.C. Increasing incidence of cataract surgery: Population-based study. J. Cataract Refract. Surg. 2013, 39, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Charlesworth, E.; Alderson, A.J.; de Juan, V.; Elliott, D.B. When is refraction stable following routine cataract surgery? A systematic review and meta-analysis. Ophthalmic Physiol. Opt. 2020, 40, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Dhoot, A.S.; Popovic, M.M.; Lee, S.; El-Defrawy, S.; Schlenker, M.B. Eye protection following cataract surgery: A systematic review. Can. J. Ophthalmol. 2023, 58, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Morrell, A. A nationwide survey of post-operative instructions following uncomplicated phacoemulsification cataract surgery. Eye 2001, 15, 723–727. [Google Scholar] [CrossRef]
- Braithwaite, T.; Calvert, M.; Gray, A.; Pesudovs, K.; Denniston, A.K. The use of patient-reported outcome research in modern ophthalmology: Impact on clinical trials and routine clinical practice. Patient Relat. Outcome Meas. 2019, 10, 9–24. [Google Scholar] [CrossRef]
- Hays, R.D.; MacRae, S.; Holladay, J.; Tarver, M.E.; Lum, F.; Stark, W.; Weidmer, B.; Kumar, N.; Lau, G.; Nguyen, T.; et al. Development of a Patient-Reported Outcome Measure to Assess Symptoms Associated with Cataract Surgery and Intraocular Lens Implants. Ophthalmology 2023, 130, 715–725. [Google Scholar] [CrossRef]
- Koh, E.J.; Lee, J.M.; Lim, D.H.; Kang, D.; Cho, J.; Song, M.K.; Chung, I.K.; Choi, H.J.; Chang, J.W.; Lee, J.H. Validation and Reliability of the Cataract-related Visual Function Questionnaire (CVFQ). J. Korean Ophthalmol. Soc. 2023, 64, 1030–1040. [Google Scholar] [CrossRef]
- Yoon, H.; Seo, J.; Yoo, S.K.; Kim, P.J.; Park, J.; Choe, Y.; Yang, W. Updated general exposure factors for risk assessment in the Korean population. J. Expo. Sci. Environ. Epidemiol. 2023, 33, 1013–1020. [Google Scholar] [CrossRef]
- Bron, A.J.; Evans, V.E.; Smith, J.A. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea 2003, 22, 640–650. [Google Scholar] [CrossRef]
- Whitcher, J.P.; Shiboski, C.H.; Shiboski, S.C.; Heidenreich, A.M.; Kitagawa, K.; Zhang, S.; Hamann, S.; Larkin, G.; McNamara, N.A.; Greenspan, J.S.; et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren’s Syndrome International Registry. Am. J. Ophthalmol. 2010, 149, 405–415. [Google Scholar] [CrossRef]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematic review of the pain scales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Lundström, M.; Pesudovs, K. Catquest-9SF patient outcomes questionnaire: Nine-item short-form Rasch-scaled revision of the Catquest questionnaire. J. Cataract Refract. Surg. 2009, 35, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, E.P.; Tielsch, J.M.; Schein, O.D.; Javitt, J.C.; Sharkey, P.; Cassard, S.D.; Legro, M.W.; Diener-West, M.; Bass, E.B.; Damiano, A.M.; et al. The VF-14. An index of functional impairment in patients with cataract. Arch. Ophthalmol. 1994, 112, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Javitt, J.C.; Jacobson, G.; Schiffman, R.M. Validity and reliability of the Cataract TyPE Spec: An instrument for measuring outcomes of cataract extraction. Am. J. Ophthalmol. 2003, 136, 285–290. [Google Scholar] [CrossRef]
- Superstein, R. Indications for cataract surgery. Curr. Opin. Ophthalmol. 2001, 12, 58–62. [Google Scholar] [CrossRef]
- Owsley, C.; McGwin, G., Jr. Vision and driving. Vis. Res. 2010, 50, 2348–2361. [Google Scholar] [CrossRef]
- Charlesworth, E.; Ursell, P.; Ho, K.C.; Keay, L.; Elliott, D.B. Developing refractive management recommendations for patients undergoing cataract surgery: A Delphi study. Ophthalmic Physiol. Opt. 2023, 43, 150–159. [Google Scholar] [CrossRef]
- Decina, L.E.; Staplin, L. Retrospective evaluation of alternative vision screening criteria for older and younger drivers. Accid. Anal. Prev. 1993, 25, 267–275. [Google Scholar] [CrossRef]
- Maguire, E.A.; Woollett, K.; Spiers, H.J. London taxi drivers and bus drivers: A structural MRI and neuropsychological analysis. Hippocampus 2006, 16, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Patoine, A.; Mikula, L.; Mejía-Romero, S.; Michaels, J.; Keruzoré, O.; Chaumillon, R.; Bernardin, D.; Faubert, J. Increased visual and cognitive demands emphasize the importance of meeting visual needs at all distances while driving. PLoS ONE 2021, 16, e0247254. [Google Scholar] [CrossRef] [PubMed]
- Webber, K.J.; Fylan, F.; Wood, J.M.; Elliott, D.B. Experiences following cataract surgery—Patient perspectives. Ophthalmic Physiol. Opt. 2020, 40, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Echieh, C.I.; Etim, B.A.; Echieh, C.P.; Oyeniyi, T.; Ajewole, J. A comparative assessment of dry eye disease among outdoor street sweepers and indoor office cleaners. BMC Ophthalmol. 2021, 21, 265. [Google Scholar] [CrossRef]
- Mandell, J.T.; Idarraga, M.; Kumar, N.; Galor, A. Impact of Air Pollution and Weather on Dry Eye. J. Clin. Med. 2020, 9, 3740. [Google Scholar] [CrossRef]
- Suh, J.H.; Chung, S.K. The Effect of Topical Rebamipide 2% in Managing Dry Eye Following Cataract Surgery. J. Korean Ophthalmol. Soc. 2024, 65, 589–595. [Google Scholar] [CrossRef]
- Hamada, S.; Moore, T.C.; Moore, J.E.; Al-Dreihi, M.G.; Anbari, A.; Shah, S. Assessment of the effect of cyclosporine-A 0.05% emulsion on the ocular surface and corneal sensation following cataract surgery. Cont. Lens Anterior Eye 2016, 39, 15–19. [Google Scholar] [CrossRef]

{kind=link}
| Parameters | Outdoor Time ≤ 3 h/d (Group 1; n = 57) | Outdoor Time > 3 h/d (Group 2; n = 33) | p Value |
|---|---|---|---|
| Age (Years) | 68.74 ± 12.74 (21–87) | 64.15 ± 13.02 (34–82) | 0.110 |
| Gender (male/female) | 19 (33.3%)/38 (66.7%) | 16 (48.5%)/17 (51.5%) | 0.231 |
| Preoperative | |||
| UDVA (LogMAR) | 0.32 ± 0.22 (0.03–0.80) | 0.33 ± 0.23 (0.00–0.70) | 0.898 |
| BCVA (LogMAR) | 0.55 ± 0.25 (0.05–1.00) | 0.47 ± 0.25 (0.01–0.80) | 0.209 |
| IOP (mmHg) | 16.67 ± 2.05 (12–21) | 17.36 ± 1.97 (15–21) | 0.115 |
| SE, manifest refraction (D) | −2.73 ± 5.83 (−27.00–5.50) | −2.93 ± 4.52 (−19.00–2.75) | 0.302 |
| Mean keratometry (D) | 43.72 ± 2.02 (36.38–47.63) | 43.81 ± 1.83 (38.00–46.25) | 0.834 |
| Postoperative | |||
| UDVA (logMAR) | 0.76 ± 0.19 (0.20–1.00) | 0.77 ± 0.21 (0.40–1.20) | 0.767 |
| BCVA (logMAR) | 0.92 ± 0.12 (0.70–1.00) | 0.91 ± 0.11 (0.70–1.00) | 0.593 |
| IOP (mmHg) | 14.98 ± 2.80 (10–21) | 15.33 ± 2.31 (12–20) | 0.524 |
| SE, manifest refraction (D) | −0.68 ± 0.98 (−6.00–0.50) | −0.73 ± 0.74 (−2.50–1.00) | 0.287 |
| Mean keratometry (D) | 43.86 ± 2.02 (36.88–47.75) | 43.85 ± 1.87 (37.63–46.38) | 0.981 |
| Parameters | Outdoor Time ≤ 3 h/d (Group 1; n = 57) | Outdoor Time > 3 h/d (Group 2; n = 33) | p Value |
|---|---|---|---|
| TBUT (sec) | 4.63 ± 1.40 (2–8) | 4.33 ± 1.80 (2–9) | 0.452 |
| Cornea staining score | |||
| Oxford score (0–5) | 0.46 ± 0.58 (0–2) | 0.48 ± 0.85 (0–3) | 0.534 |
| SICCA score (0–3) | 1.25 ± 1.38 (0–5) | 1.30 ± 1.84 (0–7) | 0.540 |
| OSDI | |||
| Physical symptoms score (0–4) | 0.60 ± 0.55 (0.00–2.20) | 0.76 ± 0.62 (0.00–2.20) | 0.177 |
| Discomfort during daily activities (0–4) | 0.53 ± 0.67 (0.00–2.67) | 0.45 ± 0.50 (0.00–2.00) | 0.872 |
| Aggravation by environmental factors (0–4) | 0.78 ± 0.76 (0.00–2.67) | 0.65 ± 0.83 (0.00–3.00) | 0.259 |
| Total OSDI score (25–100) | 15.53 ± 13.13 (0.00–55.56) | 15.92 ± 13.47 (0.00–56.25) | 0.895 |
| Numerical Rating Scale (0–10) | 0.45 ± 1.08 (0–5) | 0.50 ± 0.88 (0–3) | 0.309 |
| Parameters | Outdoor Time ≤ 3 h/d (Group 1; n = 57) | Outdoor Time > 3 h/d (Group 2; n = 33) | p Value |
|---|---|---|---|
| CVFQ | |||
| Overall visual quality (0–4) | 3.28 ± 0.73 (2.00–4.00) | 3.15 ± 0.67 (2.00–4.00) | 0.345 |
| Overall visual function (0–4) | 3.53 ± 0.66 (1.00–4.00) | 3.55 ± 0.56 (2.00–4.00) | 0.931 |
| Distance visual difficulties (0–4) | 3.81 ± 0.30 (2.75–4.00) | 3.78 ± 0.31 (3.00–4.00) | 0.732 |
| Near visual difficulties (0–4) | 3.43 ± 0.60 (1.20–4.00) | 3.38 ± 0.57 (2.00–4.00) | 0.702 |
| Glare symptoms | |||
| Daytime driving (0–4) | 3.93 ± 0.26 (3–4) | 3.60 ± 0.65 (2–4) | 0.020 |
| Walking outside on a sunny day (0–4) | 3.46 ± 0.76 (1–4) | 3.44 ± 0.76 (1–4) | 0.824 |
| Night-time driving (0–4) | 3.48 ± 0.64 (2–4) | 3.00 ± 0.85 (1–4) | 0.037 |
| Looking at the street lights (0–4) | 3.71 ± 0.46 (3–4) | 3.57 ± 0.68 (2–4) | 0.494 |
| Total CVFQ score (25–100) | 89.90 ± 8.52 (70.00–100.00) | 86.38 ± 10.29 (65.75–100.00) | 0.530 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.M.; Kim, N.; Kim, M.Y.; Park, N.; Lee, Y.E.; Han, J.; Lee, H.; Eah, K.S.; Jeon, Y.Y.; Chung, H.S.; et al. The Effects of Outdoor Activity on Patient-Reported Visual Outcomes Under Perioperative Management Using Cyclosporine and Rebamipide. Diagnostics 2025, 15, 1629. https://doi.org/10.3390/diagnostics15131629
Lee CM, Kim N, Kim MY, Park N, Lee YE, Han J, Lee H, Eah KS, Jeon YY, Chung HS, et al. The Effects of Outdoor Activity on Patient-Reported Visual Outcomes Under Perioperative Management Using Cyclosporine and Rebamipide. Diagnostics. 2025; 15(13):1629. https://doi.org/10.3390/diagnostics15131629
Chicago/Turabian StyleLee, Chung Min, Nahee Kim, Min Young Kim, Nahyun Park, Yea Eun Lee, Jeewon Han, Hayoung Lee, Kyu Sang Eah, Yoo Young Jeon, Ho Seok Chung, and et al. 2025. "The Effects of Outdoor Activity on Patient-Reported Visual Outcomes Under Perioperative Management Using Cyclosporine and Rebamipide" Diagnostics 15, no. 13: 1629. https://doi.org/10.3390/diagnostics15131629
APA StyleLee, C. M., Kim, N., Kim, M. Y., Park, N., Lee, Y. E., Han, J., Lee, H., Eah, K. S., Jeon, Y. Y., Chung, H. S., Kim, J. Y., & Lee, H. (2025). The Effects of Outdoor Activity on Patient-Reported Visual Outcomes Under Perioperative Management Using Cyclosporine and Rebamipide. Diagnostics, 15(13), 1629. https://doi.org/10.3390/diagnostics15131629