
Ultrasound Evaluation of Internal Jugular Venous Insufficiency and Its Association with Cognitive Decline
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Clinical Assessments
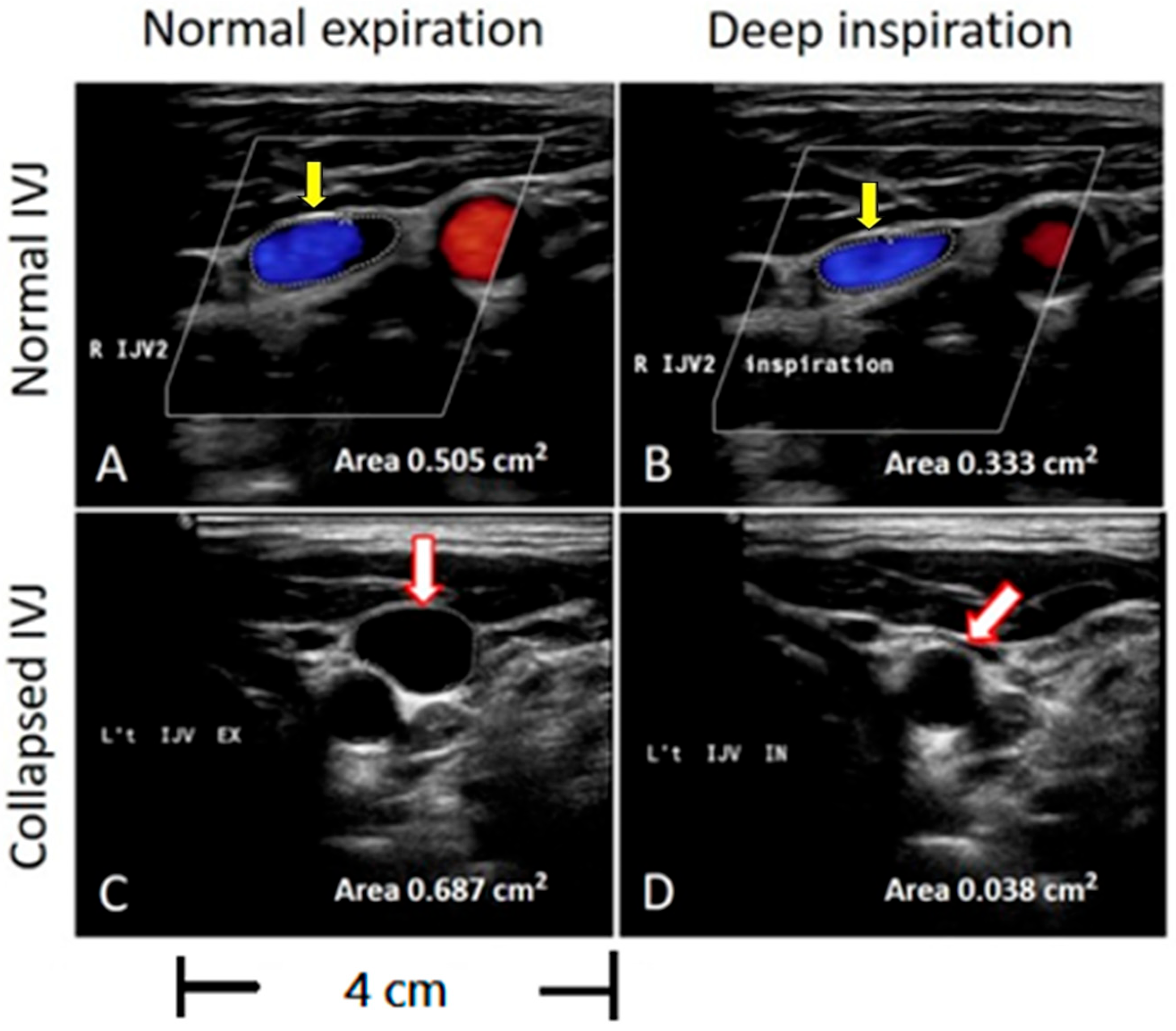
2.3. Color-Coded Duplex Ultrasonography
2.4. IJV Drainage Determination
2.5. Cognitive Function Assessment
2.6. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics of Impaired Cognition and Control Group
3.2. IJV Flow Velocity and Drainage Between Impaired Cognition and Control Group
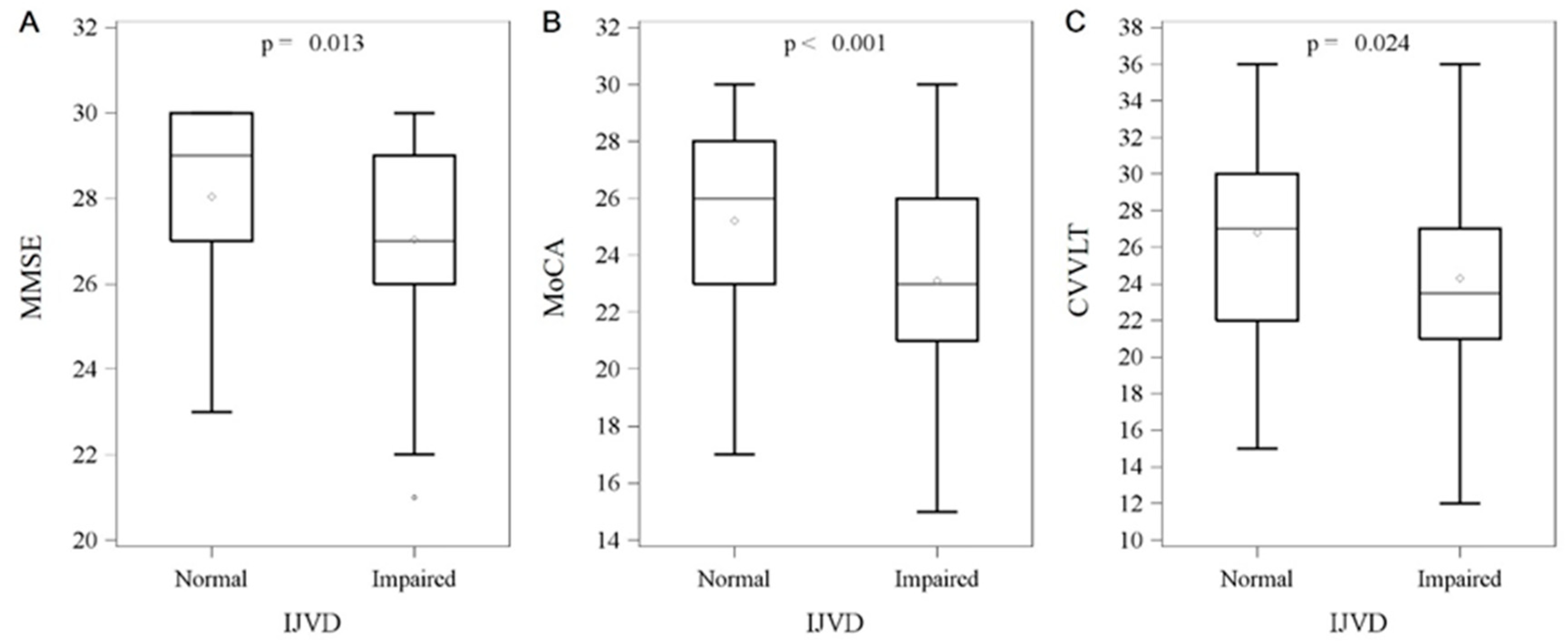
3.3. Comparison of Neuropsychological Tests Between Impaired IJV Drainage and Control Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IJV | Internal jugular vein. |
| AD | Alzheimer’s disease. |
| JVR | Jugular venous reflux. |
| VM | Valsalva maneuvers. |
| MCI | Mild cognitive impairment. |
| BMI | Body mass index. |
| DM | Diabetes mellitus. |
| CKD | Chronic kidney disease. |
| TAMV | Time-averaged mean velocity. |
| CSA | Cross-sectional area. |
| CCA | Common carotid artery. |
| ICA | Internal carotid artery. |
| VA | Vertebral artery. |
| MCA | Middle cerebral artery. |
| MMSE | Mini-Mental State Examination. |
| MoCA | Montreal Cognitive Assessment. |
| CVVLT | Chinese Version of the Verbal Learning Test. |
| IQR | Interquartile range. |
| OR | Odds ratio. |
| CI | Confidence interval. |
| PI | Pulsatility index. |
| TS | Transverse sinus. |
| BFV | Blood flow volume. |
References
- Fargen, K.M.; Midtlien, J.P.; Margraf, C.R.; Hui, F.K. Idiopathic intracranial hypertension pathogenesis: The jugular hypothesis. Interv. Neuroradiol. 2024, 15910199241270660. [Google Scholar] [CrossRef]
- Bai, C.; Wang, Z.; Stone, C.; Zhou, D.; Ding, J.; Ding, Y.; Ji, X.; Meng, R. Pathogenesis and Management in Cerebrovenous Outflow Disorders. Aging Dis. 2021, 12, 203–222. [Google Scholar] [CrossRef]
- Fulop, G.A.; Tarantini, S.; Yabluchanskiy, A.; Molnar, A.; Prodan, C.I.; Kiss, T.; Csipo, T.; Lipecz, A.; Balasubramanian, P.; Farkas, E.; et al. Role of age-related alterations of the cerebral venous circulation in the pathogenesis of vascular cognitive impairment. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H1124–H1140. [Google Scholar] [CrossRef]
- Chung, C.P.; Lin, Y.J.; Chao, A.C.; Lin, S.J.; Chen, Y.Y.; Wang, Y.J.; Hu, H.H. Jugular venous hemodynamic changes with aging. Ultrasound Med. Biol. 2010, 36, 1776–1782. [Google Scholar] [CrossRef]
- Kuriyama, N.; Tokuda, T.; Miyamoto, J.; Takayasu, N.; Kondo, M.; Nakagawa, M. Retrograde jugular flow associated with idiopathic normal pressure hydrocephalus. Ann. Neurol. 2008, 64, 217–221. [Google Scholar] [CrossRef]
- Han, K.; Hu, H.H.; Chao, A.C.; Chang, F.C.; Chung, C.P.; Hsu, H.Y.; Sheng, W.Y.; Wu, J. Transient Global Amnesia Linked to Impairment of Brain Venous Drainage: An Ultrasound Investigation. Front. Neurol. 2019, 10, 67. [Google Scholar] [CrossRef]
- Kapadia, A.; Dmytriw, A.A. Venous dysfunction plays a critical role in “normal” white matter disease of aging. Med. Hypotheses 2021, 146, 110457. [Google Scholar] [CrossRef]
- Chung, C.P.; Wang, P.N.; Wu, Y.H.; Tsao, Y.C.; Sheng, W.Y.; Lin, K.N.; Lin, S.J.; Hu, H.H. More severe white matter changes in the elderly with jugular venous reflux. Ann. Neurol. 2011, 69, 553–559. [Google Scholar] [CrossRef]
- Anderson, N.D. State of the science on mild cognitive impairment (MCI). CNS Spectr. 2019, 24, 78–87. [Google Scholar] [CrossRef]
- Adachi, U.; Toi, S.; Hosoya, M.; Hoshino, T.; Seki, M.; Yoshizawa, H.; Tsutsumi, Y.; Maruyama, K.; Kitagawa, K. Association of Age-Related Spontaneous Internal Jugular Vein Reflux with Cognitive Impairment and Incident Dementia. J. Alzheimers Dis. 2023, 96, 1221–1230. [Google Scholar] [CrossRef]
- Zivadinov, R.; Bastianello, S.; Dake, M.D.; Ferral, H.; Haacke, E.M.; Haskal, Z.J.; Hubbard, D.; Liasis, N.; Mandato, K.; Sclafani, S.; et al. Recommendations for multimodal noninvasive and invasive screening for detection of extracranial venous abnormalities indicative of chronic cerebrospinal venous insufficiency: A position statement of the International Society for Neurovascular Disease. J. Vasc. Interv. Radiol. 2014, 25, 1785–1794.e17. [Google Scholar] [CrossRef]
- Matsuzono, K.; Suzuki, M.; Miura, K.; Ozawa, T.; Mashiko, T.; Koide, R.; Tanaka, R.; Fujimoto, S. Internal Jugular Vein Velocity and Spontaneous Echo Contrast Correlate with Alzheimer’s Disease and Cognitive Function. J. Alzheimers Dis. 2021, 84, 787–796. [Google Scholar] [CrossRef]
- Marr, K.; Jakimovski, D.; Mancini, M.; Carl, E.; Zivadinov, R. Jugular Venous Flow Quantification Using Doppler Sonography. Ultrasound Med. Biol. 2018, 44, 1762–1769. [Google Scholar] [CrossRef]
- Jones, D.W.; Hall, J.E. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure and evidence from new hypertension trials. Hypertension 2004, 43, 1–3. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33 (Suppl. 1), S62–S69. [Google Scholar] [CrossRef]
- Levey, A.S.; Eckardt, K.U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; De Zeeuw, D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef]
- Rugge, J.B.; Bougatsos, C.; Chou, R. Screening and treatment of thyroid dysfunction: An evidence review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2015, 162, 35–45. [Google Scholar] [CrossRef]
- Chao, A.C.; Han, K.; Chang, F.C.; Hsu, H.Y.; Chung, C.P.; Sheng, W.Y.; Chan, L.; Wu, J.; Hu, H.H. Ultrasound diagnosis of transverse sinus hypoplasia using flow profiles of the internal jugular vein. PLoS ONE 2017, 12, e0181119. [Google Scholar] [CrossRef]
- Zamboni, P.; Morovic, S.; Menegatti, E.; Viselner, G.; Nicolaides, A.N. Screening for chronic cerebrospinal venous insufficiency (CCSVI) using ultrasound--recommendations for a protocol. Int. Angiol. 2011, 30, 571–597. [Google Scholar]
- Tsao, Y.C.; Chung, C.P.; Hsu, H.Y.; Cheng, C.Y.; Chao, A.C.; Sheng, W.Y.; Hu, H.H.; Hong, C.J.; Wu, J.C. Collapsed Jugular Vein and abnormal cerebral blood flow changes in patients of Panic Disorder. J. Psychiatr. Res. 2014, 58, 155–160. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Chang, C.C.; Kramer, J.H.; Lin, K.N.; Chang, W.N.; Wang, Y.L.; Huang, C.W.; Lin, Y.T.; Chen, C.; Wang, P.N. Validating the Chinese version of the Verbal Learning Test for screening Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2010, 16, 244–251. [Google Scholar] [CrossRef]
- Brucki, S.M.D.; Nitrini, R. Cognitive impairment in individuals with low educational level and homogeneous sociocultural background. Dement. Neuropsychol. 2014, 8, 345–350. [Google Scholar] [CrossRef]
- Kim, R.; Chung, W. Effect of Aging on Educational Differences in the Risk of Cognitive Impairment: A Gender-Specific Analysis Using Korean Longitudinal Study of Aging (2006–2016). Healthcare 2022, 10, 1062. [Google Scholar] [CrossRef]
- Nova-Baeza, P.; Valenzuela-Fuenzalida, J.J.; Valdivia-Arroyo, R.; Becerra-Rodríguez, E.S.; Escalona-Manzo, C.; Castaño-Gallego, Y.T.; Luque-Bernal, R.M.; Oyanedel-Amaro, G.; Suazo-Santibáñez, A.; Orellana-Donoso, M.; et al. Systematic Review and Meta-Analysis of Internal Jugular Vein Variants and Their Relationship to Clinical Implications in the Head and Neck. Diagnostics 2024, 14, 2765. [Google Scholar] [CrossRef]
- Magnano, C.; Belov, P.; Krawiecki, J.; Hagemeier, J.; Beggs, C.; Zivadinov, R. Internal Jugular Vein Cross-Sectional Area Enlargement Is Associated with Aging in Healthy Individuals. PLoS ONE 2016, 11, e0149532. [Google Scholar] [CrossRef]
- Laganà, M.M.; Pelizzari, L.; Scaccianoce, E.; Dipasquale, O.; Ricci, C.; Baglio, F.; Cecconi, P.; Baselli, G. Assessment of Internal Jugular Vein Size in Healthy Subjects with Magnetic Resonance and Semiautomatic Processing. Behav. Neurol. 2016, 2016, 9717210. [Google Scholar] [CrossRef]
- Schaller, B. Physiology of cerebral venous blood flow: From experimental data in animals to normal function in humans. Brain Res. Rev. 2004, 46, 243–260. [Google Scholar] [CrossRef]
- Conn, R.D.; O’Keefe, J.H. Simplified evaluation of the jugular venous pressure: Significance of inspiratory collapse of jugular veins. Mo. Med. 2012, 109, 150–152. [Google Scholar]
- Bérczi, V.; Molnár, A.A.; Apor, A.; Kovács, V.; Ruzics, C.; Várallyay, C.; Hüttl, K.; Monos, E.; Nádasy, G.L. Non-invasive assessment of human large vein diameter, capacity, distensibility and ellipticity in situ: Dependence on anatomical location, age, body position and pressure. Eur. J. Appl. Physiol. 2005, 95, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J. Psychiatr. Res. 2009, 43, 411–431. [Google Scholar] [CrossRef] [PubMed]
- Gluhm, S.; Goldstein, J.; Loc, K.; Colt, A.; Liew, C.V.; Corey-Bloom, J. Cognitive performance on the mini-mental state examination and the montreal cognitive assessment across the healthy adult lifespan. Cogn. Behav. Neurol. 2013, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- De Roeck, E.E.; De Deyn, P.P.; Dierckx, E.; Engelborghs, S. Brief cognitive screening instruments for early detection of Alzheimer’s disease: A systematic review. Alzheimers Res. Ther. 2019, 11, 21. [Google Scholar] [CrossRef]
- Zamboni, P.; Menegatti, E.; Weinstock-Guttman, B.; Dwyer, M.G.; Schirda, C.V.; Malagoni, A.M.; Hojnacki, D.; Kennedy, C.; Carl, E.; Bergsland, N.; et al. Hypoperfusion of brain parenchyma is associated with the severity of chronic cerebrospinal venous insufficiency in patients with multiple sclerosis: A cross-sectional preliminary report. BMC Med. 2011, 9, 22. [Google Scholar] [CrossRef]
- Garaci, F.G.; Marziali, S.; Meschini, A.; Fornari, M.; Rossi, S.; Melis, M.; Fabiano, S.; Stefanini, M.; Simonetti, G.; Centonze, D.; et al. Brain hemodynamic changes associated with chronic cerebrospinal venous insufficiency are not specific to multiple sclerosis and do not increase its severity. Radiology 2012, 265, 233–239. [Google Scholar] [CrossRef]
- Fulop, G.A.; Ahire, C.; Csipo, T.; Tarantini, S.; Kiss, T.; Balasubramanian, P.; Yabluchanskiy, A.; Farkas, E.; Toth, A.; Nyúl-Tóth, Á.; et al. Cerebral venous congestion promotes blood-brain barrier disruption and neuroinflammation, impairing cognitive function in mice. Geroscience 2019, 41, 575–589. [Google Scholar] [CrossRef]
- Houck, A.L.; Gutierrez, J.; Gao, F.; Igwe, K.C.; Colon, J.M.; Black, S.E.; Brickman, A.M. Increased Diameters of the Internal Cerebral Veins and the Basal Veins of Rosenthal Are Associated with White Matter Hyperintensity Volume. AJNR Am. J. Neuroradiol. 2019, 40, 1712–1718. [Google Scholar] [CrossRef]
- Ungvari, Z.; Tarantini, S.; Kirkpatrick, A.C.; Csiszar, A.; Prodan, C.I. Cerebral microhemorrhages: Mechanisms, consequences, and prevention. Am. J. Physiol. Heart Circ. Physiol. 2017, 312, H1128–H1143. [Google Scholar] [CrossRef]
- Molnár, A.; Nádasy, G.L.; Dörnyei, G.; Patai, B.B.; Delfavero, J.; Fülöp, G.; Kirkpatrick, A.C.; Ungvári, Z.; Merkely, B. The aging venous system: From varicosities to vascular cognitive impairment. Geroscience 2021, 43, 2761–2784. [Google Scholar] [CrossRef]
- Zhou, D.; Ding, J.Y.; Ya, J.Y.; Pan, L.Q.; Yan, F.; Yang, Q.; Ding, Y.C.; Ji, X.M.; Meng, R. Understanding jugular venous outflow disturbance. CNS Neurosci. Ther. 2018, 24, 473–482. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| All | Cognitive Impairment | Normal Cognition | p-Value | |
|---|---|---|---|---|
| n = 106 | n = 50 | n = 56 | ||
| Age (years old) | 71.5 ± 8.0 | 73.4 ± 7.0 | 69.8 ± 8.5 | 0.0503 |
| Gender (F/M) | 67/39 | 33/17 | 34/22 | 0.3732 |
| Education (years) | 13.1 ± 3.8 | 11.3 ± 4.5 | 14.4 ± 2.9 | 0.0003 * |
| BMI (kg/m2) | 24.3 ± 3.2 | 23.9 ± 3.1 | 24.7 ± 3.2 | 0.2195 |
| Hypertension (%) | 51 (48%) | 22 (44%) | 29 (52%) | 0.4232 |
| DM (%) | 20 (19%) | 12 (24%) | 8 (14%) | 0.2019 |
| Dyslipidemia (%) | 42 (40%) | 14 (29%) | 28 (50%) | 0.0208 * |
| CKD (%) | 4 (4%) | 1 (2%) | 3 (5%) | 0.3652 |
| Thyroid dysfunction(%) | 15 (14%) | 7 (14%) | 8 (14%) | 0.9664 |
| History of stroke (%) | 11(10%) | 4 (8%) | 7 (13%) | 0.4482 |
| History of MI (%) | 1 (1%) | 0 | 1 (2%) | 0.3424 |
| MoCA | 24.3 ± 3.4 | 21.1 ± 2.4 | 26.9 ± 1.4 | <0.0001 * |
| MMSE | 27.6 ± 2.1 | 26.2 ± 1.9 | 28.9 ± 1.2 | <0.0001 * |
| TAMV, cm/s | Cognitive Impairment (n = 50) No. (%) | Normal Cognition (n = 56) No. (%) | p-Value |
|---|---|---|---|
| LJ2 < 4 cm/s | 17 (34%) | 14 (25%) | 0.3092 |
| LJ3 < 4 cm/s | 17 (34%) | 10 (18%) | 0.0569 |
| RJ2 < 4 cm/s | 5 (10%) | 5 (9%) | 0.8342 |
| RJ3 < 4 cm/s | 6 (12%) | 1 (2%) | 0.0321 |
| LVV < 0.05 cm/s | 11 (22%) | 14 (26%) | 0.6397 |
| RVV < 0.05 cm/s | 7 (15%) | 8 (15%) | 0.9425 |
| LJ2 and LJ3 < 4 cm/s | 15 (30%) | 8 (14%) | 0.0501 |
| RJ2 and RJ3 < 4 cm/s | 4 (8%) | 1 (2%) | 0.1319 |
| Impaired outflow * | 17 (34%) | 9 (16%) | 0.0322 |
| CSA collapse ** | |||
| LJ2 | 18 (36%) | 13 (23%) | 0.1486 |
| RJ2 | 10 (20%) | 6 (11%) | 0.1825 |
| Impaired IJVD *** | 34 (68%) | 17 (30%) | 0.0001 |
| Univariate Analysis | Multivariate Analysis # | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age | 2.46 | 1.02~5.92 | 0.0445 | 1.07 | 1.00~1.13 | 0.0394 |
| Education | 0.79 | 0.70~0.90 | 0.0002 | 0.76 | 0.67~0.88 | 0.0001 |
| MCA PI | 12.35 | 1.12~136.5 | 0.0403 | |||
| Dyslipidemia | 0.39 | 0.17~0.87 | 0.022 | |||
| Impaired IJVD | 2.78 | 1.00~7.71 | 0.0495 | 3.84 | 1.33~11.09 | 0.0130 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yin, J.-H.; Chi, N.-F.; Sheng, W.-Y.; Wang, P.-N.; Sung, Y.-F.; Peng, G.-S.; Hu, H.-H. Ultrasound Evaluation of Internal Jugular Venous Insufficiency and Its Association with Cognitive Decline. Diagnostics 2025, 15, 1427. https://doi.org/10.3390/diagnostics15111427
Yin J-H, Chi N-F, Sheng W-Y, Wang P-N, Sung Y-F, Peng G-S, Hu H-H. Ultrasound Evaluation of Internal Jugular Venous Insufficiency and Its Association with Cognitive Decline. Diagnostics. 2025; 15(11):1427. https://doi.org/10.3390/diagnostics15111427
Chicago/Turabian StyleYin, Jiu-Haw, Nai-Fang Chi, Wen-Yung Sheng, Pei-Ning Wang, Yueh-Feng Sung, Giia-Sheun Peng, and Han-Hwa Hu. 2025. "Ultrasound Evaluation of Internal Jugular Venous Insufficiency and Its Association with Cognitive Decline" Diagnostics 15, no. 11: 1427. https://doi.org/10.3390/diagnostics15111427
APA StyleYin, J.-H., Chi, N.-F., Sheng, W.-Y., Wang, P.-N., Sung, Y.-F., Peng, G.-S., & Hu, H.-H. (2025). Ultrasound Evaluation of Internal Jugular Venous Insufficiency and Its Association with Cognitive Decline. Diagnostics, 15(11), 1427. https://doi.org/10.3390/diagnostics15111427