Evaluation of Ovarian Stromal Microvascularity and Clinical-Hormonal Associations in Reproductive-Aged Women with Polycystic Ovary Morphology



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.2.1. Inclusion Criteria
- Age ≥18 years (up to 49 years) at the time of imaging.
- Polycystic ovarian morphology (PCOM) on ultrasound, defined according to the most recent international guidelines as ≥20 follicles (2–9 mm in diameter) and/or ovarian volume >10 cm3 in at least one ovary [3].
- Availability of a complete hormonal profile (FSH, LH, total testosterone, free testosterone, DHEAS, estradiol), obtained on the same calendar day as the ultrasonographic assessment (specifically on menstrual cycle days 3–7, if applicable).
2.2.2. Exclusion Criteria
- Incomplete or missing hormonal data on the day of ultrasound.
- Recent use of hormonal medications (within six months) for menstrual regulation, contraception, or management of PCOS, as these may alter endogenous hormone levels and vascular measurements.
- Any clinical or ultrasound finding (e.g., large ovarian cysts, ovarian masses) that could confound measurement of the ovarian stroma or its vasculature.
- Inadequate image quality (e.g., absent or incomplete cine-loop recordings) precluding a precise vascularity index (VI) evaluation.
2.3. Imaging Protocol and Data Collection
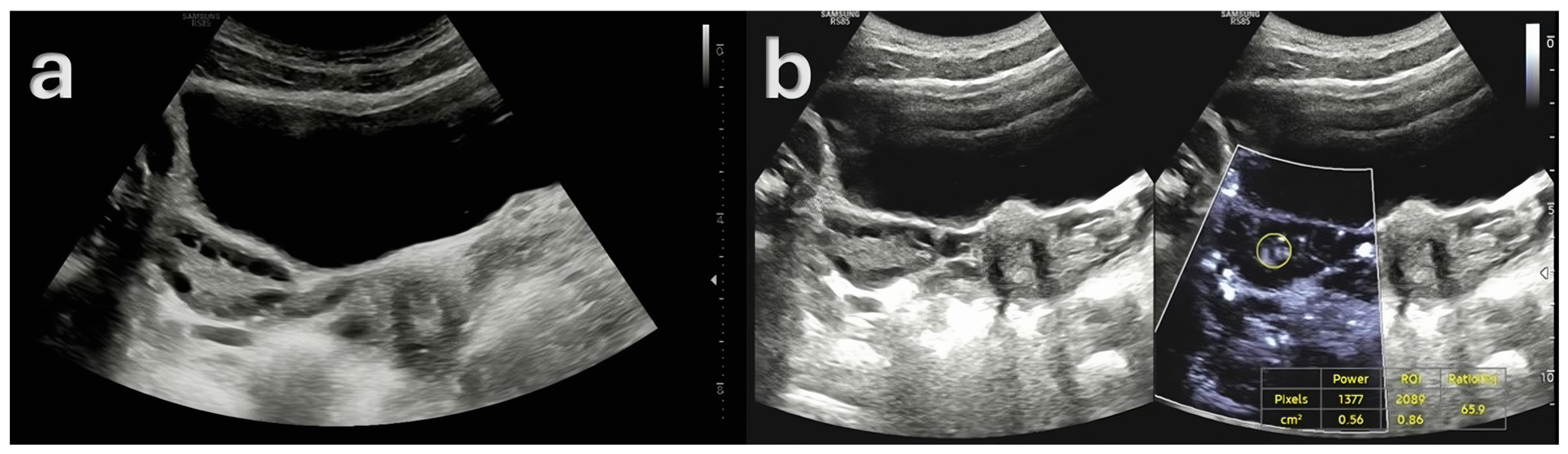
- Gray-Scale Ultrasonography (USG): A Samsung RS85 Prestige Ultrasound System (Samsung Medison) with a convex transducer (CA1-7A, 1–7 MHz) was utilized to perform gray-scale ultrasonographic assessment. The evaluation of each ovary involved a systematic examination for polycystic ovarian morphology (PCOM). This condition was characterized by either the presence of 20 or more follicles with diameters ranging from 2 to 9 mm, or an ovarian volume greater than 10 cm3.
- Doppler Examination (MV-Flow, MVI): Ovarian stromal vascularity was evaluated using the same ultrasound equipment and transducer (Samsung RS85 Prestige with CA1-7A, 1–7 MHz). MV-Flow Doppler imaging was performed consistently in the longitudinal plane to maintain anatomical standardization. Cine-loop clips of at least 3 s duration were captured and stored. For vascularity index measurements, the optimal frame demonstrating clear vascular flow was selected from the stored cine-loop clips. In the ovarian stroma, three circular regions of interest (ROIs) were centrally positioned. These ROIs, each with a fixed 5 mm diameter, were carefully selected to exclude dominant follicles and peripheral vascular structures. The ROI dimensions and MV-Flow Doppler imaging parameters, including pulse repetition frequency (PRF), gain, and wall filter, were maintained consistently throughout the duration of the study.
- Hormonal Parameters: The acquisition of hormonal measurements was facilitated through the retrieval of data from the hospital’s electronic repository. The extracted parameters encompassed a comprehensive array of endocrine markers, including FSH, LH, total testosterone, free testosterone, DHEAS, and estradiol. All hormonal samples were collected on the same day as the ultrasonographic evaluation, specifically between days 3 and 7 of the menstrual cycle, in the morning hours, to minimize variability and ensure temporal consistency between imaging and biochemical assessments.
- Index Test and Reference Standard: The index test in this study was advanced microvascular Doppler imaging (MV-Flow), used to quantify ovarian stromal vascularity. The reference standards included an ultrasound-based assessment of ovarian morphology to identify polycystic changes and a biochemical analysis of hormonal levels reflecting hyperandrogenism and gonadotropin status. These hormonal assays were used to characterize the endocrine profiles of the patients and to classify polycystic ovary syndrome (PCOS) phenotypes.
- Reading Strategy and Observer Blinding: Initial imaging was performed by one of two radiologists with 10 and 7 years of experience, respectively, during routine clinical care, with partial access to clinical and laboratory data in accordance with standard workflow. For study purposes, all cine-loops and images were anonymized by removing DICOM identifiers, and the same two radiologists independently re-evaluated the stored cine-loops to measure the vascularity index (VI) while being blinded to clinical and biochemical results.
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| CA1-7A | Convex array transducer (1–7 MHz) |
| CI | Confidence interval |
| DHEAS | Dehydroepiandrosterone sulfate |
| FSH | Follicle-stimulating hormone |
| ICC | Intraclass correlation coefficient |
| IRB | Institutional Review Board |
| IQR | Interquartile range |
| LH | Luteinizing hormone |
| MVI | Microvascular imaging |
| MV-Flow | Microvascular flow Doppler |
| PCOM | Polycystic ovarian morphology |
| PCOS | Polycystic ovary syndrome |
| PRF | Pulse repetition frequency |
| ROI | Region of interest |
| SD | Standard deviation |
| SMI | Superb microvascular imaging |
| US | Ultrasonography |
| VEGF | Vascular endothelial growth factor |
| VI | Vascularity Index |
| SMI | Superb microvascular imaging |
References
- Ehrmann, D.A. Polycystic ovary syndrome. N. Engl. J. Med. 2005, 352, 1223–1236. [Google Scholar] [CrossRef] [PubMed]
- Makled, A.K.; El Sherbiny, M.; Elkabarity, R. Assessment of ovarian stromal blood flow after metformin treatment in women with polycystic ovary syndrome. Arch. Gynecol. Obstet. 2014, 289, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Christ, J.P.; Cedars, M.I. Current Guidelines for Diagnosing PCOS. Diagnostics 2023, 13, 1113. [Google Scholar] [CrossRef]
- Kinnear, H.M.; Tomaszewski, C.E.; Chang, A.L.; Moravek, M.B.; Xu, M.; Padmanabhan, V.; Shikanov, A. The ovarian stroma as a new frontier. Reproduction 2020, 160, R25–R39. [Google Scholar] [CrossRef]
- Singh, S.; Pal, N.; Shubham, S.; Sarma, D.K.; Verma, V.; Marotta, F.; Kumar, M. Polycystic ovary syndrome: Etiology, current management, and future therapeutics. J. Clin. Med. 2023, 12, 1454. [Google Scholar] [CrossRef]
- Lizneva, D.; Suturina, L.; Walker, W.; Brakta, S.; Gavrilova-Jordan, L.; Azziz, R. Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil. Steril. 2016, 106, 6–15. [Google Scholar] [CrossRef]
- Emekçi Özay, Ö.; Özay, A.C.; Gün, İ. Comparison of stromal thickness and doppler findings in polycystic ovary syndrome and healthy women with ultrasonographic evidence of polycystic ovaries? A cross-sectional study. J. Obstet. Gynaecol. 2022, 42, 2367–2372. [Google Scholar] [CrossRef]
- Ramírez Martín, N.; Romeu, M.; Martínez, J.; Peinado, I.; Chico-Sordo, L.; Buigues, A.; Soriano, M.J.; Pellicer, N.; Pellicer, A.; Herraiz, S. P-647 Underlying mechanisms in clinical manifestations of polycystic ovarian morphology (PCOM) and PCOS women. Hum. Reprod. 2023, 38, dead093.975. [Google Scholar] [CrossRef]
- Azziz, R.; Sanchez, L.A.; Knochenhauer, E.S.; Moran, C.; Lazenby, J.; Stephens, K.C.; Taylor, K.; Boots, L.R. Androgen Excess in Women: Experience with Over 1000 Consecutive Patients. J. Clin. Endocrinol. Metab. 2004, 89, 453–462. [Google Scholar] [CrossRef]
- Rosenfield, R.L.; Ehrmann, D.A. The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited. Endocr. Rev. 2016, 37, 467–520. [Google Scholar] [CrossRef]
- Abbott, D.H.; Vepraskas, S.H.; Horton, T.H.; Terasawa, E.; Levine, J.E. Accelerated Episodic Luteinizing Hormone Release Accompanies Blunted Progesterone Regulation in PCOS-like Female Rhesus Monkeys (Macaca mulatta) Exposed to Testosterone during Early-to-Mid Gestation. Neuroendocrinology 2018, 107, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Fedeli, V.; Unfer, V.; Dinicola, S.; Laganà, A.S.; Canipari, R.; Monti, N.; Querqui, A.; Galante, E.; Laurenzi, G.; Bizzarri, M. Inositol Restores Appropriate Steroidogenesis in PCOS Ovaries Both In Vitro and In Vivo Experimental Mouse Models. Cells 2024, 13, 1171. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.M.; Nivya, P.S.; Devika, C.S.; Reddy, M.S.; Poornima, N.; Roopesh, K.R.; Kolageri, S. A review of hyperandrogenism state in polycystic ovarian syndrome. Int. J. Reprod. Contracept. Obstet. Gynecol. 2023, 12, 3714–3721. [Google Scholar] [CrossRef]
- Xiang, Y.; Wang, H.; Ding, H.; Xu, T.; Liu, X.; Huang, Z.; Wu, H.; Ge, H. Hyperandrogenism drives ovarian inflammation and pyroptosis: A possible pathogenesis of PCOS follicular dysplasia. Int. Immunopharmacol. 2023, 125, 111141. [Google Scholar] [CrossRef]
- Agrawal, R.; Conway, G.; Sladkevicius, P.; Tan, S.L.; Engmann, L.; Payne, N.; Bekir, J.; Campbell, S.; Jacobs, H. Serum Vascular Endothelial Growth Factor and Doppler Blood Flow Velocities in In Vitro Fertilization: Relevance to Ovarian Hyperstimulation Syndrome and Polycystic Ovaries. Obstet. Gynecol. Surv. 1999, 54, 181–183. [Google Scholar] [CrossRef]
- Agrawal, R.; Sladkevicius, P.; Engmann, L.; Conway, G.S.; Payne, N.N.; Bekis, J.; Tan, S.L.; Campbell, S.; Jacobs, H.S. Serum vascular endothelial growth factor concentrations and ovarian stromal blood flow are increased in women with polycystic ovaries. Hum. Reprod. 1998, 13, 651–655. [Google Scholar] [CrossRef]
- Guzmán, A.; Hernández-Coronado, C.G.; Gutiérrez, C.G.; Rosales-Torres, A.M. The vascular endothelial growth factor (VEGF) system as a key regulator of ovarian follicle angiogenesis and growth. Mol. Reprod. Dev. 2023, 90, 201–217. [Google Scholar] [CrossRef]
- Liu, M.M.; Chen, X.H.; Lu, X.M.; Wang, F.F.; Wang, C.; Liu, Y.; Li, P.L.; Du, B.T.; Liang, S.; Gong, P.D.; et al. Variations in the Profiles of Vascular-Related Factors Among Different Sub-Types of Polycystic Ovarian Syndrome in Northern China. Front. Endocrinol. 2020, 11, 527592. [Google Scholar] [CrossRef]
- Senyuva, I.; Turan, C.O.; Yuksel, G.Y.; Senturk, S. Superb Microvascular Imaging Doppler Technique in the Evaluation of Ovarian Stromal Vascularity in Women with Polycystic Ovary Syndrome. J. Pak. Med. Assoc. 2023, 73, 1992–1996. [Google Scholar] [CrossRef]
- Fulghesu, A.M.; Angioni, S.; Frau, E.; Belosi, C.; Apa, R.; Mioni, R.; Xamin, N.; Capobianco, G.P.; Dessole, S.; Fruzzetti, F.; et al. Ultrasound in polycystic ovary syndrome—The measuring of ovarian stroma and relationship with circulating androgens: Results of a multicentric study. Hum. Reprod. 2007, 22, 2501–2508. [Google Scholar] [CrossRef]
- Yildiz, B.O.; Azziz, R. The adrenal and polycystic ovary syndrome. Rev. Endocr. Metab. Disord. 2007, 8, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Khaira, H.K.; Kaur, M.; Sinha, S. A Comparative Study on Quantitative Assessment of Blood Flow and Vascularization in Polycystic Ovary Syndrome Patients and Normal Women Using Three-Dimensional Power Doppler Ultrasonography. J. Obstet. Gynaecol. India 2018, 68, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.H.; Chan, C.C.; Yeung, W.S.; Ho, P.C. Comparison of ovarian stromal blood flow between fertile women with normal ovaries and infertile women with polycystic ovary syndrome. Hum. Reprod. 2005, 20, 1881–1886. [Google Scholar] [CrossRef]
- Alcázar, J.L.; Kudla, M.J. Ovarian stromal vessels assessed by spatiotemporal image correlation–high definition flow in women with polycystic ovary syndrome: A case–control study. Ultrasound Obstet. Gynecol. 2012, 40, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, C.; Battaglia, B.; Morotti, E.; Paradisi, R.; Zanetti, I.; Meriggiola, M.C.; Venturoli, S. Two- and Three-Dimensional Sonographic and Color Doppler Techniques for Diagnosis of Polycystic Ovary Syndrome. J. Ultrasound Med. 2012, 31, 1015–1024. [Google Scholar] [CrossRef]
- Wang, W.-Q.; Chu, G.-H.; Hou, X.-X. A comparison of Doppler measures of ovarian blood flow between women with and without ovarian dysfunction and correlations of Doppler indices with ovarian dysfunction markers: A meta-analysis. Ann. Transl. Med. 2023, 11, 110. [Google Scholar] [CrossRef]
- Dolz, M.; Osborne, N.G.; Blanes, J.; Raga, F.; Abad-Velasco, L.; Villalobos, A.; Pellicer, A.; Bonilla-Musoles, F. Polycystic ovarian syndrome: Assessment with color Doppler angiography and three-dimensional ultrasonography. J. Ultrasound Med. 1999, 18, 303–313. [Google Scholar] [CrossRef]
- Omar Hassan, P.; Faruq Jamal, A. Intra-ovarian Doppler artery indices values in cases with polycystic ovarian syndrome: A case control study. Zanco J. Med. Sci. 2024, 28, 223–234. [Google Scholar] [CrossRef]
- Catteau-Jonard, S.; Bancquart, J.; Poncelet, E.; Lefebvre-Maunoury, C.; Robin, G.; Dewailly, D. Polycystic ovaries at ultrasound: Normal variant or silent polycystic ovary syndrome? Ultrasound Obstet. Gynecol. 2012, 40, 223–229. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 111) | Non-PCOS (n = 13) | Phenotype A (n = 50) | Phenotype C (n = 25) | Phenotype D (n = 23) | p-Value |
|---|---|---|---|---|---|---|
| Age (years), median (IQR) | 23 (21–26) | 22 (21–24) | 23 (21–26) | 24 (21–27) | 24 (22–26) | 0.665 |
| Mean VI, mean ± SD | 43.88 ± 19.84 | 9.95 ± 5.44 a | 61.35 ± 10.11 b | 42.57 ± 3.58 c | 26.47 ± 4.24 d | <0.001 |
| FSH (mIU/mL), median (IQR) | 5.21 (4.13–6.45) | 5.37 (4.35–6.02) ab | 4.35 (3.35–5.72) a | 5.65 (5.00–7.70) b | 5.99 (5.54–6.45) b | 0.002 |
| LH (mIU/mL), median (IQR) | 5.1 (4.00–7.98) | 4.7 (4–5.9) | 5.5 (4.33–8.61) | 5.00 (2.95–6.97) | 4.72 (3.79–6.88) | 0.307 |
| LH/FSH Ratio, median (IQR) | 1.03 (0.75–1.57) | 0.93 (0.78–1.13) ab | 1.34 (0.96–2.12) a | 0.88 (0.62–1.10) b | 1.10 (0.6–1.51) ab | 0.002 |
| Estradiol (pg/mL), median (IQR) | 32.75 (25.31–42.38) | 28.22 (21.23–40.03) | 36.01 (28.51–47) | 32.75 (22.30–37.70) | 31.82 (29.07–39.36) | 0.155 |
| Total testosterone (ng/mL), median (IQR) | 1.62 (1.11–2.06) | 1.00 (0.97–1.06) a | 2.14 (1.77–2.34) b | 1.55 (1.41–1.62) c | 1.11 (1.1–1.3) ac | <0.001 |
| Free testosterone (pg/mL), median (IQR) | 3.9 (1.9–5) | 1.61 (1.53–1.64) a | 5.00 (3.9–5.37) b | 3.20 (2.60–3.90) c | 1.61 (1.51–1.9) a | <0.001 |
| DHEAS (μg/dL), median (IQR) | 299 (290–346) | 152 (136–165) | 241 (147–290) a | 299 (263–311) b | 362 (299–429) b | <0.001 |
| Hormones | Correlation Coefficient (R) | p-Value |
|---|---|---|
| FSH | –0.149 | 0.050 |
| LH | 0.130 | 0.090 |
| LH/FSH | 0.225 | 0.003 |
| Estradiol | 0.178 | 0.019 |
| Total Testosterone | 0.797 | <0.001 |
| Free Testosterone | 0.778 | <0.001 |
| DHEAS | –0.483 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baş, H.; Filiz, S. Evaluation of Ovarian Stromal Microvascularity and Clinical-Hormonal Associations in Reproductive-Aged Women with Polycystic Ovary Morphology. Diagnostics 2025, 15, 1376. https://doi.org/10.3390/diagnostics15111376
Baş H, Filiz S. Evaluation of Ovarian Stromal Microvascularity and Clinical-Hormonal Associations in Reproductive-Aged Women with Polycystic Ovary Morphology. Diagnostics. 2025; 15(11):1376. https://doi.org/10.3390/diagnostics15111376
Chicago/Turabian StyleBaş, Hakan, and Süleyman Filiz. 2025. "Evaluation of Ovarian Stromal Microvascularity and Clinical-Hormonal Associations in Reproductive-Aged Women with Polycystic Ovary Morphology" Diagnostics 15, no. 11: 1376. https://doi.org/10.3390/diagnostics15111376
APA StyleBaş, H., & Filiz, S. (2025). Evaluation of Ovarian Stromal Microvascularity and Clinical-Hormonal Associations in Reproductive-Aged Women with Polycystic Ovary Morphology. Diagnostics, 15(11), 1376. https://doi.org/10.3390/diagnostics15111376