
Effectiveness of Virtual Surgical Planning and Three-Dimensional Anatomical Models in Radiological Reconstruction of Center of Rotation and Pelvic Brim in Patients with Anterior Column Defects Requiring Revision Hip Arthroplasty
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
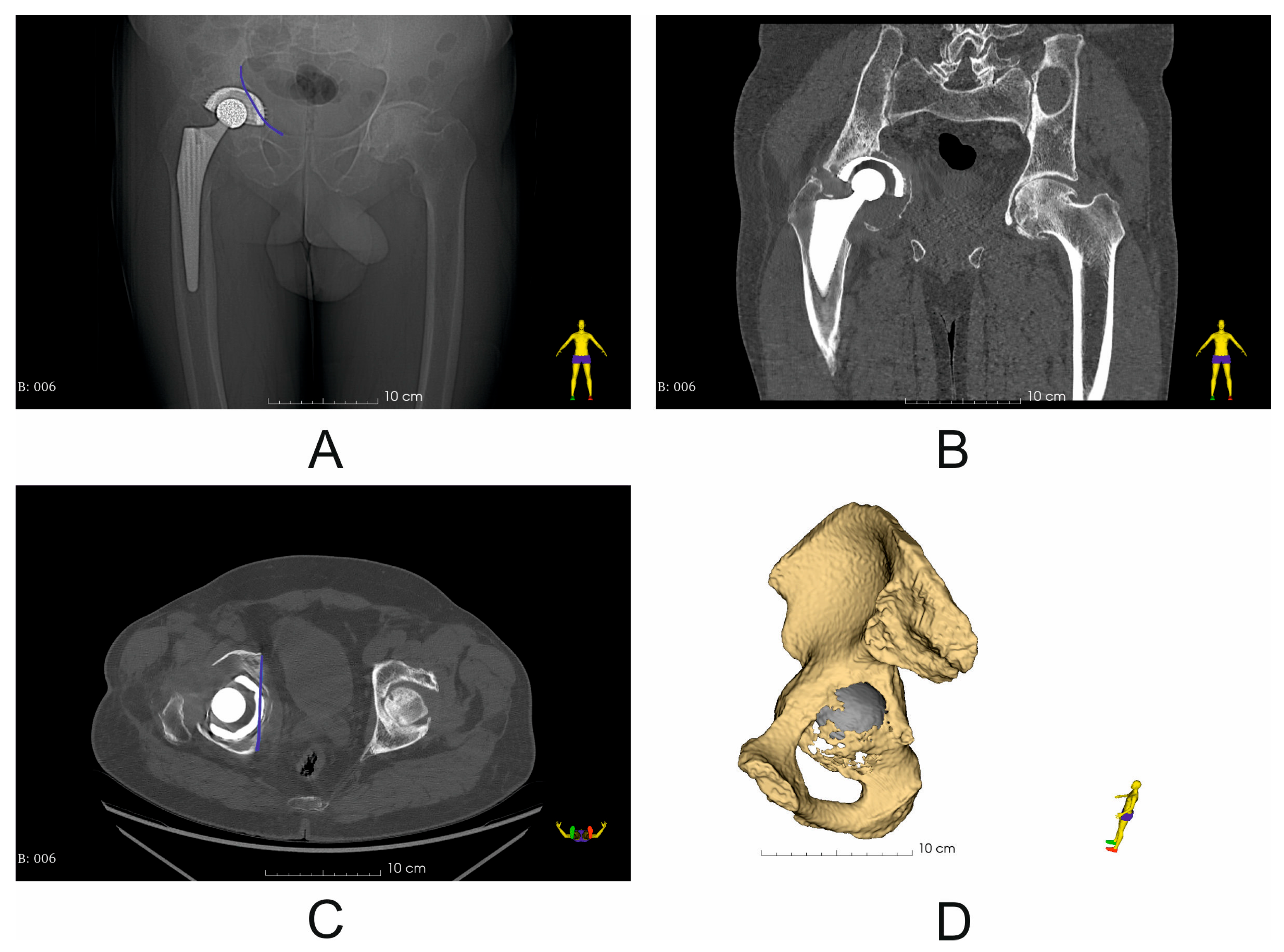
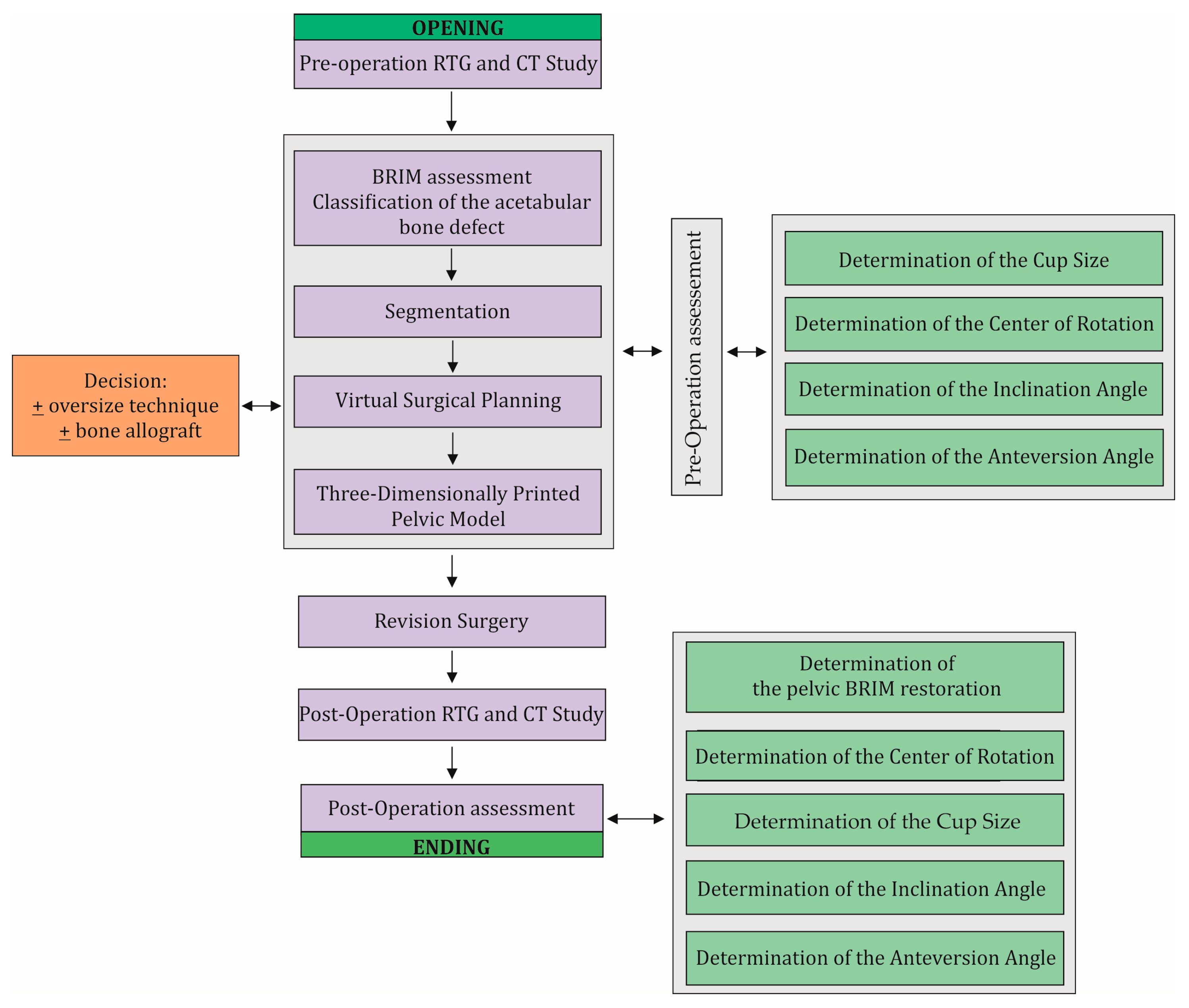
2.1. Clinical Information and Surgical Technique: Classification of the Acetabular Bone Defect
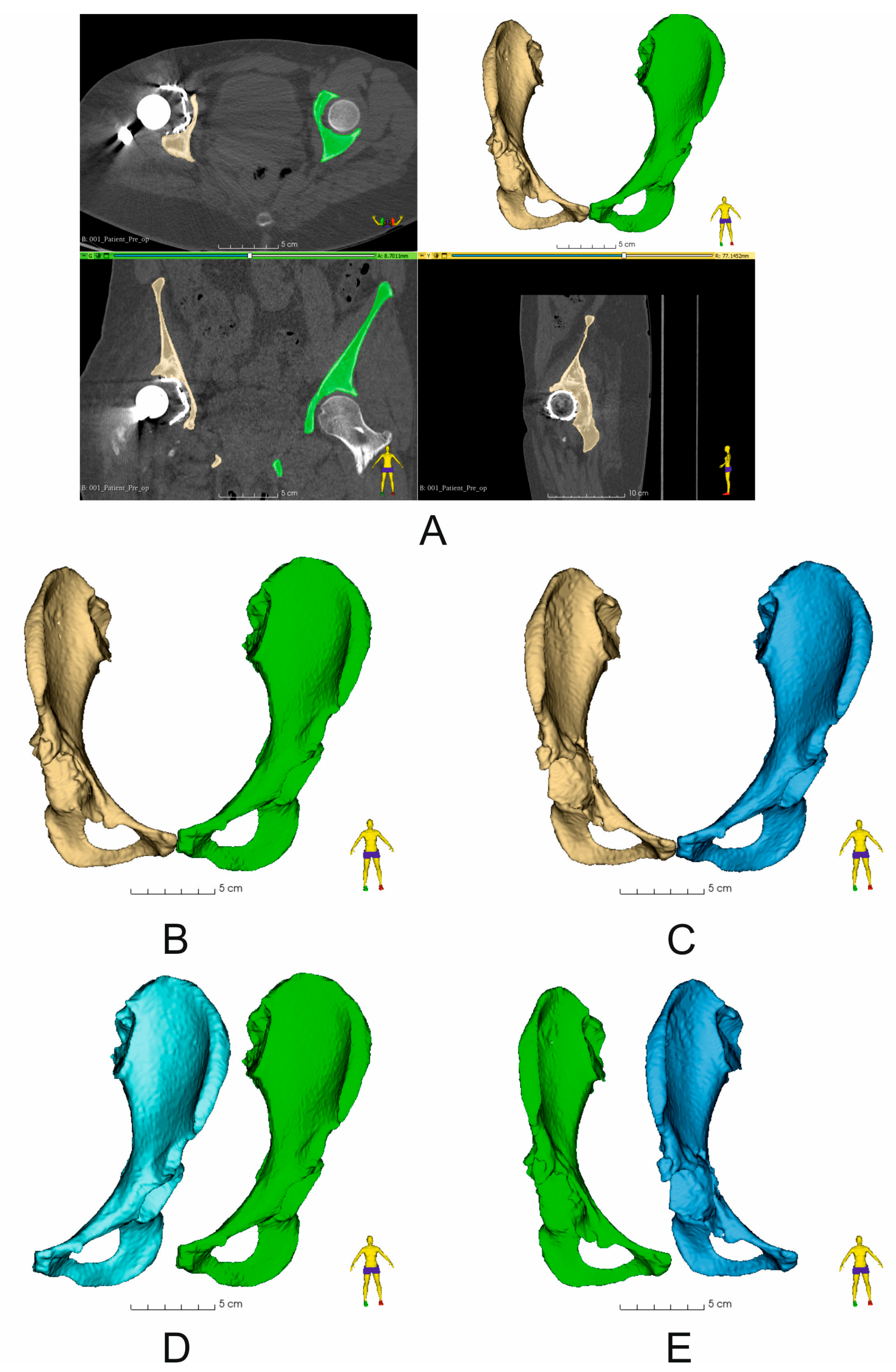
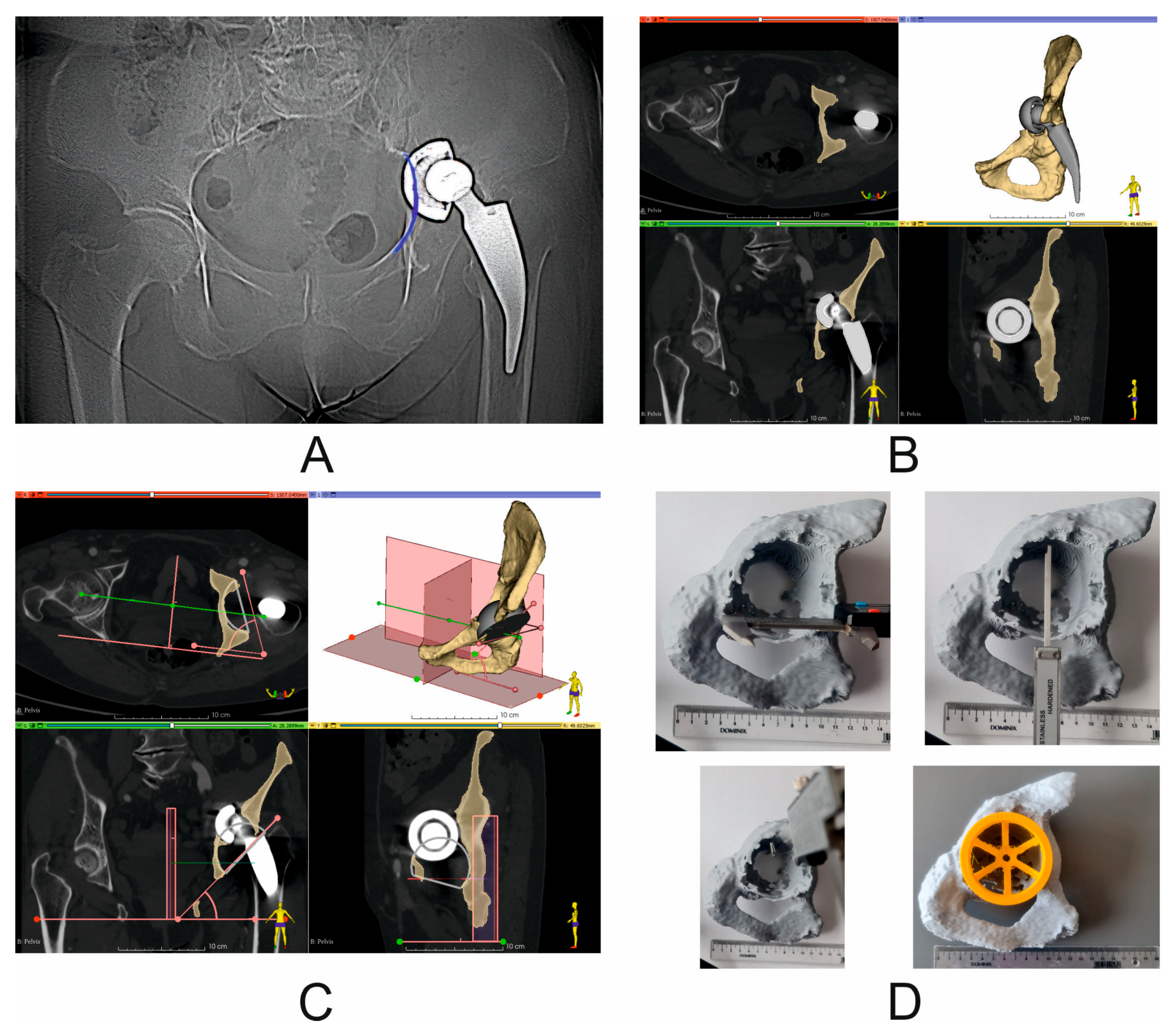
2.2. Virtual Surgical Planning (Pre- and Post-Operation Assessment): Assessment of the Quality of Bone Structure Segmentation and Pelvic BRIM Damage, Determination of the Diameter of the Revision Cup, Determination of the Inclination and Anteversion Angles and the Center of Rotation (COR), and Assessment of the Size of the Acetabular Revision Cup
2.3. Three-Dimensional Printing of Pelvic Models
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beckers, G.; Djebara, A.-E.; Gauthier, M.; Lubbeke, A.; Gamulin, A.; Zingg, M.; Bastian, J.D.; Hannouche, D. Acetabular Peri-Prosthetic Fractures—A Narrative Review. Medicina 2022, 58, 630. [Google Scholar] [CrossRef] [PubMed]
- AO Surgery Reference. Available online: https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/acetabulum/further-reading/radiology-of-the-intact-acetabulum#standard-imaging-views (accessed on 2 October 2024).
- Mancino, F.; Cacciola, G.; De Marco, D.; Greenberg, A.; Perisano, C.; Malahias, M.; Sculco, P.K.; Maccauro, G.; De Martino, I. Reconstruction options and outcomes for acetabular bone loss in revision hip arthroplasty. Orthop. Rev. 2020, 12, 8655. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- D’Antonio, J.A.; Capello, W.N.; Borden, L.S.; Bargar, W.L.; Bierbaum, B.F.; Boettcher, W.G.; Steinberg, M.E.; Stulberg, S.D.; Wedge, J.H. Classification and Management of Acetabular Abnormalities in Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 1989, 243, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Paprosky, W.G.; Perona, P.G.; Lawrence, J.M. Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J. Arthroplast. 1994, 9, 33–44. [Google Scholar] [CrossRef]
- Pandey, A.K.; Zuke, W.A.; Surace, P.; Kamath, A.F. Management of acetabular bone loss in revision total hip replacement: A narrative literature review. Ann. Jt. 2023, 9, 21. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fröschen, F.S.; Randau, T.M.; Walter, S.G.; Dally, F.; Wirtz, D.C.; Gravius, S. Use of custom-made acetabular components (CMAC) as part of a two-stage procedure in patients with severe periacetabular bone loss. Oper. Orthopadie Und Traumatol. 2022, 34, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Dong, P.; Li, Z.; Zhu, F.; Wang, Z.; Cai, X. Biomechanical analysis of the fixation systems for anterior column and posterior hemi-transverse acetabular fractures. Acta Orthop. Traumatol. Turc. 2017, 51, 248–253. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Harnroongroj, T. The role of the anterior column of the acetabulum on pelvic stability: A biomechanical study. Injury 1998, 29, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Wegrzyn, J.; Thoreson, A.R.; Guyen, O.; Lewallen, D.G.; An, K. Cementation of a dual-mobility acetabular component into a well-fixed metal shell during revision total hip arthroplasty: A biomechanical validation. J. Orthop. Res. 2013, 31, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Andrzejewski, K.; Domżalski, M.; Komorowski, P.; Poszepczyński, J.; Rokita, B.; Elgalal, M. Optimization of Revision Hip Arthroplasty Workflow by Means of Detailed Pre-Surgical Planning Using Computed Tomography Data, Open-Source Software and Three-Dimensional-Printed Models. Diagnostics 2023, 13, 2516. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Huang, Y.; Zhou, B.; Zhou, Y. Mid-Term Follow-Up of Acetabular Revision Arthroplasty Using Jumbo Cups. Orthop. Surg. 2019, 11, 811–818. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peng, Y.-W.; Shen, J.-M.; Zhang, Y.-C.; Sun, J.-Y.; Du, Y.-Q.; Zhou, Y.-G. Jumbo cup in hip joint renovation may cause the center of rotation to increase. World J. Clin. Cases 2021, 9, 6300–6307. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rolvien, T.; Friesecke, C.; Butscheidt, S.; Gehrke, T.; Hahn, M.; Püschel, K. A novel, multi-level approach to assess allograft incorporation in revision total hip arthroplasty. Sci. Rep. 2020, 10, 15226. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kamińska, M.; Jastrzębska, A.; Walkowiak-Przybyło, M.; Walczyńska, M.; Komorowski, P.; Walkowiak, B. Adhesion and Activation of Blood Platelets on Laser-Structured Surfaces of Biomedical Metal Alloys. J. Funct. Biomater. 2023, 14, 478. [Google Scholar] [CrossRef] [PubMed]
- Lewinnek, E.G.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after total hip-replacement arthroplasties. J. Bone Jt. Surg. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, Q.; Liu, P.; Ge, J.; Zhang, Q.; Guo, W.; Wang, W. Clinical and radiological outcomes of jumbo cup in revision total hip arthroplasty: A systematic review. Front. Surg. 2022, 9, 929103. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shen, X.; Tian, H.; Li, Y.; Zuo, J.; Gao, Z.; Xiao, J. Acetabular Revision Arthroplasty Based on 3-Dimensional Reconstruction Technology Using Jumbo Cups. Front. Bioeng. Biotechnol. 2022, 10, 799443. [Google Scholar] [CrossRef]
- van Heumen, M.; Heesterbeek, P.J.C.; Swierstra, B.A.; Van Hellemondt, G.G.; Goosen, J.H.M. Dual mobility acetabular component in revision total hip arthroplasty for persistent dislocation: No dislocations in 50 hips after 1–5 years. J. Orthop. Traumatol. 2015, 16, 15–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hartzler, M.A.; Abdel, M.P.; Sculco, P.K.; Taunton, M.J.; Pagnano, M.W.; Hanssen, A.D. Otto Aufranc Award: Dual-mobility Constructs in Revision THA Reduced Dislocation, Rerevision, and Reoperation Compared with Large Femoral Heads. Clin. Orthop. Relat. Res. 2018, 476, 293–301. [Google Scholar] [CrossRef]
- Chalmers, B.P.; Perry, K.I.; Hanssen, A.D.; Pagnano, M.W.; Abdel, M.P. Conversion of Hip Hemiarthroplasty to Total Hip Arthroplasty Utilizing a Dual-Mobility Construct Compared with Large Femoral Heads. J. Arthroplast. 2017, 32, 3071–3075. [Google Scholar] [CrossRef] [PubMed]
- Strahl, A.; Boese, C.K.; Ries, C.; Hubert, J.; Beil, F.T.; Rolvien, T. Outcome of different reconstruction options using allografts in revision total hip arthroplasty for severe acetabular bone loss: A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2023, 143, 6403–6422. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient [Sex] | Acetabular Size According to VSP [mm] | Acetabular Size After Revision Surgery [mm] | Decision to Use Allograft According to VSP | Use of Allograft in Revision Surgery | Prosthesis Head [mm] | Screws |
|---|---|---|---|---|---|---|
| 1 [male] | 66 | 64 | + | + | 28 | Two screws placed in acetabular roof |
| 2 [male] | 68 | 66 | + | + | ||
| 3 [female] | 64 | 66 | + | + | ||
| 4 [male] | 66 | 64 | + | + | ||
| 5 [female] | 62 | 64 | + | + | ||
| 6 [male] | 68 | 68 | + | + | ||
| 7 [female] | 64 | 62 | + | + | ||
| 8 [male] | 66 | 68 | + | + | ||
| mean ± SD | 65.5 ± 2.1 | 65.3 ± 2.1 |
| Parameters | % Difference [Mean ± SD] | Range Min–Max [mm3] | Correlation Coefficient (Pearson r) | p Value |
|---|---|---|---|---|
| Determination of the correctness of pelvic bone segmentation—Comparison of the volume of the undamaged side of the pelvic bone before and after revision surgery (based on two CT scan results) | 0.01 ± 0.005 * | 180,150–360,838 | Perfect line | 0.0078 |
| Determination of anterior column bone loss between the undamaged and the damaged pelvic bone—before revision surgery | 25.2 ± 5.8 * | 124,862–360,824 | 0.9904 | 0.0078 |
| Determination of anterior column bone loss between the undamaged and the damaged pelvic bone—after revision surgery | 30.1 ± 6.7 * | 115,965–360,838 | 0.9857 | 0.0078 |
| Determination of anterior column bone loss between damaged pelvic bones—before and after revision surgery | 5.0 ± 2.0 * | 124,862–284,985 | 0.9980 | 0.0078 |
| Parameters Differences for Operated Side of Pelvis | Difference [mm] (Mean ± SD) | Range Min–Max [mm] | Correlation Coefficient (Pearson r) | p Value | B [°] |
|---|---|---|---|---|---|
| Difference in COR position, vertical axial coronal plane | 7.8 ± 9.3 * | 22.2–49.2 | 0.4383 | 0.0493 | - |
| Difference in COR position, horizontal axial coronal plane | 4.3 ± 5.9 # | 24.5–42.7 | 0.5779 | 0.0787 | - |
| Difference in COR position, axial plane | 1.6 ± 3.3 # | 28.8–68.5 | 0.9659 | 0.2240 | - |
| Difference in inclination angle | 12.4° * | - | −0.3630 | 0.0025 | IaPre-op: 60.9 ± 8.5 IaPost-op: 48.5 ± 5.5 |
| Difference in anteversion angle | 8.7° * | - | 0.1324 | 0.0080 | AaPre-op: 24.9 ± 4.2 AaPost-op: 16.3 ± 2.1 |
| 3D Printing Parameters | |
|---|---|
| Printing temperature | 205 °C |
| Build plate temperature | 60 °C |
| Layer high | 0.2 mm |
| Infill | 60% |
| Support material | Polyvinyl alcohol (PVA) (Ultimaker B.V, Geldermalsen, The Netherlands) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrzejewski, K.; Domzalski, M.; Rokita, B.; Poszepczynski, J.; Komorowski, P. Effectiveness of Virtual Surgical Planning and Three-Dimensional Anatomical Models in Radiological Reconstruction of Center of Rotation and Pelvic Brim in Patients with Anterior Column Defects Requiring Revision Hip Arthroplasty. Diagnostics 2024, 14, 2574. https://doi.org/10.3390/diagnostics14222574
Andrzejewski K, Domzalski M, Rokita B, Poszepczynski J, Komorowski P. Effectiveness of Virtual Surgical Planning and Three-Dimensional Anatomical Models in Radiological Reconstruction of Center of Rotation and Pelvic Brim in Patients with Anterior Column Defects Requiring Revision Hip Arthroplasty. Diagnostics. 2024; 14(22):2574. https://doi.org/10.3390/diagnostics14222574
Chicago/Turabian StyleAndrzejewski, Krzysztof, Marcin Domzalski, Bozena Rokita, Jan Poszepczynski, and Piotr Komorowski. 2024. "Effectiveness of Virtual Surgical Planning and Three-Dimensional Anatomical Models in Radiological Reconstruction of Center of Rotation and Pelvic Brim in Patients with Anterior Column Defects Requiring Revision Hip Arthroplasty" Diagnostics 14, no. 22: 2574. https://doi.org/10.3390/diagnostics14222574
APA StyleAndrzejewski, K., Domzalski, M., Rokita, B., Poszepczynski, J., & Komorowski, P. (2024). Effectiveness of Virtual Surgical Planning and Three-Dimensional Anatomical Models in Radiological Reconstruction of Center of Rotation and Pelvic Brim in Patients with Anterior Column Defects Requiring Revision Hip Arthroplasty. Diagnostics, 14(22), 2574. https://doi.org/10.3390/diagnostics14222574